

Abstract
Unruptured right sinus of Valsalva aneurysm that causes severe obstruction of the right ventricular outflow tract is extremely rare. We describe the case of a 47-year-old woman who presented with exertional dyspnea. Upon investigation, we discovered an unruptured right sinus of Valsalva aneurysm with associated right ventricular outflow tract obstruction and a supracristal ventricular septal defect. To our knowledge, only 2 such cases have previously been reported in the medical literature.
Although treatment of unruptured sinus of Valsalva aneurysm remains debatable, surgery should be considered for extremely large aneurysms or for progressive enlargement of the aneurysm on serial evaluation. Surgery was undertaken in our patient because there was clear evidence of right ventricular outflow tract obstruction, right-sided heart dilation, and associated exertional dyspnea.
Keywords: Aortic aneurysm; sinus of Valsalva, right/unruptured/surgery; ventricular outflow tract, right/obstruction; ventricular septal defect, supracristal/surgery
First recognized in 1840,1 sinus of Valsalva aneurysm (SVA) is an uncommon cardiac anomaly that is either congenital or acquired. The former is more prevalent: its incidence ranges from 0.1% to 3.5% of all congenital heart diseases.2 The male-to-female ratio is 4:1, with a higher incidence among Asian populations. Sinus of Valsalva aneurysms most often originate from the right or noncoronary sinus, and only rarely from the left coronary sinus.3
These lesions usually remain silent and undetected unless rupture occurs. However, even unruptured SVAs can cause important structural and electrophysiologic abnormalities that in turn lead to arrhythmia, heart block, myocardial ischemia, and (rarely) right ventricular outflow tract (RVOT) obstruction.4,5 There is also an association between SVA and supracristal ventricular septal defect (VSD).6,7
The published literature on SVA is relatively sparse and consists largely of case reports and subsequent series. Unruptured SVA with RVOT obstruction has been reported only rarely, and the triad of unruptured SVA with RVOT obstruction and associated supracristal VSD has been reported only twice previously.8,9 We report a further case of this triad and discuss treatment.
Case Report
In December 2013, a 47-year-old woman with no noteworthy medical record presented to us with a 6-month history of worsening exertional dyspnea. She reported no angina pectoris and had never experienced presyncope, syncope, or arrhythmia. On clinical examination, she was afebrile and hemodynamically stable, with mild pedal edema. Her respiratory examination yielded nothing unusual; auscultation revealed a grade 3/6 pansystolic murmur.
Transthoracic echocardiography (TTE) showed a large aneurysm of the right coronary sinus of Valsalva in association with a presumed perimembranous VSD and moderate tricuspid regurgitation, with a right ventricular (RV) systolic pressure of 126 mmHg. On transesophageal echocardiography (TEE), aneurysmal dilation of the right coronary sinus of Valsalva was evident. This unruptured aneurysm was prolapsing into the RV (Fig. 1) and was causing severe dynamic RVOT obstruction, with a maximal velocity of 4.9 m/s and a peak gradient of 100 mmHg (Fig. 2). The 1.2-cm VSD was supracristal in origin, with a left-to-right shunt (Fig. 3). We also observed moderate central aortic regurgitation (Fig. 4).
Fig. 1.
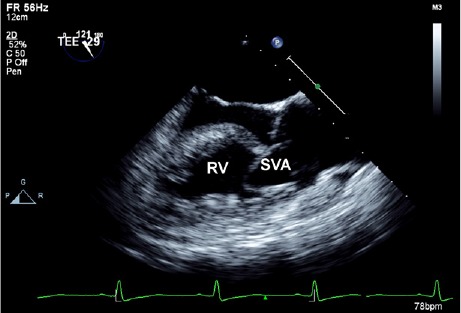
Transesophageal echocardiogram (long-axis view) shows a sinus of Valsalva aneurysm (SVA) prolapsing into the right ventricle (RV).
Fig. 2.
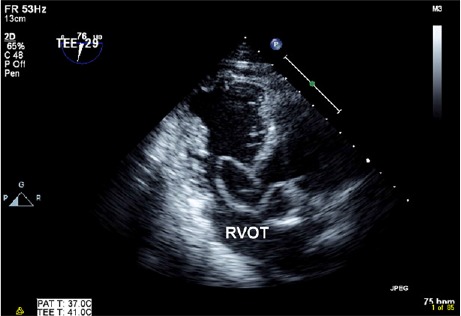
Transesophageal echocardiogram (transgastric view) shows a sinus of Valsalva aneurysm prolapsing through a ventricular septal defect, thereby obstructing the right ventricular outflow tract (RVOT).
Fig. 3.
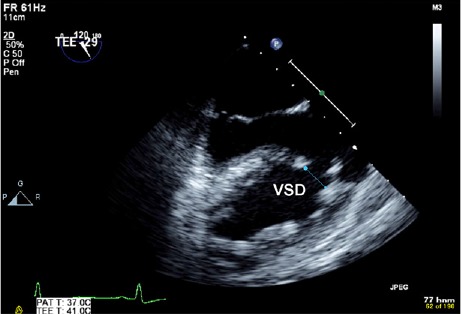
Transesophageal echocardiogram (long-axis view) shows a ventricular septal defect (VSD).
Fig. 4.
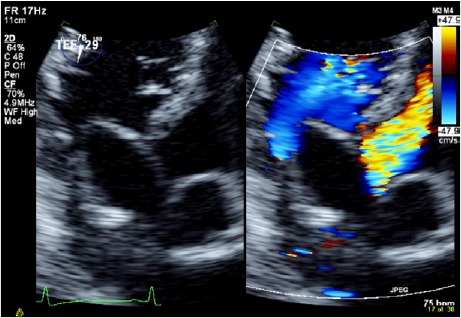
Transesophageal echocardiograms (transgastric view with color-flow Doppler comparison) show right ventricular outflow tract obstruction and aortic regurgitation.
In view of the patient's symptoms and important RVOT hemodynamic obstruction, we sent her for surgical correction. At surgery, both the aorta and the pulmonary artery were opened, which confirmed the above findings and assisted the surgery. The right coronary cusp was aneurysmal and prolapsed through the VSD, causing RVOT obstruction. The SVA and the VSD were repaired with a Gore-Tex® polytetrafluoroethylene patch (W.L. Gore & Associates, Inc.; Flagstaff, Ariz). The aortic valve was replaced with a 23-mm Masters Series mechanical valve (St. Jude Medical, Inc.; St. Paul, Minn). Intraoperative TEE confirmed the successful repair of the VSD, with no residual shunt and a normally functioning aortic valve prosthesis.
Our patient's postoperative recovery was uneventful. At the 6-month follow-up evaluation, she was asymptomatic. Transthoracic echocardiography showed no residual VSD, trivial aortic regurgitation, and mild tricuspid regurgitation, with an RV systolic pressure of 25 mmHg.
Discussion
Sinus of Valsalva aneurysm is defined as an aneurysmal dilation of one or more aortic sinuses between the aortic valve annulus and sinotubular junction. Most of these aneurysms are congenital in origin because of deficiency in the elastic and muscular tissue at the base of the aorta; less often, they are acquired as a consequence of infection (infective endocarditis, syphilis, or tuberculosis), degenerative disease (atherosclerosis, connective-tissue disease, or cystic medial necrosis), or aortic dissection.10
Sinus of Valsalva aneurysms usually remain silent and are detected only as incidental findings in the event of acute rupture or upon echocardiography performed for other indications. The typical site of origin for SVA is the right coronary cusp, but prolapse of this into the RVOT and consequent dynamic obstruction is a rare observation. Within the published literature, unruptured SVAs have also been reported to cause myocardial ischemia (due to obstruction of the coronary ostia), pulmonary insufficiency, tricuspid incompetence, and conduction disturbance.11 A coexisting VSD immediately below the aneurysm, due to distal bulbar septal abnormality, has also been reported, although this is sometimes not evident when imaging is suboptimal, because the prolapsing cusp can occlude the shunt.12 Such patients typically present with exertional dyspnea, palpitations, angina, and acute right-sided heart failure.9,12
Management of unruptured SVA remains controversial, partly because dilation of the aorta at this point (in the absence of underlying connective-tissue disease) seems to have a less malignant prognosis than does dilation of other segments of aorta.13 However, current guidelines advise surgical correction if the transverse diameter of sinuses exceeds 5.5 cm (1C evidence) or if significant valvular dysfunction is noted.14 Surgery should also be considered for extremely large SVAs or for progressive enlargement of the aneurysm on serial evaluation.15 Surgery was undertaken in our patient because there was clear evidence of RVOT obstruction, right-sided heart dilation, and associated exertional dyspnea.
Footnotes
From: Division of Cardiology, Department of Medicine, University Malaya Medical Centre, 50603 Kuala Lumpur, Malaysia
References
- 1.Cripps T, Pumphrey CW, Parker DJ. Rupture of the sinus of Valsalva during pregnancy. Br Heart J. 1987;57(5):490–1. doi: 10.1136/hrt.57.5.490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Takach TJ, Reul GJ, Duncan JM, Cooley DA, Livesay JJ, Ott DA, Frazier OH. Sinus of Valsalva aneurysm or fistula: management and outcome. Ann Thorac Surg. 1999;68(5):1573–7. doi: 10.1016/s0003-4975(99)01045-0. [DOI] [PubMed] [Google Scholar]
- 3.Fishbein MC, Obma R, Roberts WC. Unruptured sinus of Valsalva aneurysm. Am J Cardiol. 1975;35(6):918–22. doi: 10.1016/0002-9149(75)90129-0. [DOI] [PubMed] [Google Scholar]
- 4.Channer KS, Hutter JA, George M. Unruptured aneurysm of the sinus of Valsalva presenting with ventricular tachycardia. Eur Heart J. 1988;9(2):186–90. doi: 10.1093/oxfordjournals.eurheartj.a062473. [DOI] [PubMed] [Google Scholar]
- 5.Walters MI, Ettles D, Guvendik L, Kaye GC. Interventricular septal expansion of a sinus of Valsalva aneurysm: a rare cause of complete heart block. Heart. 1998;80(2):202–3. doi: 10.1136/hrt.80.2.202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chu SH, Hung CR, How SS, Chang H, Wang SS, Tsai CH et al. Ruptured aneurysms of the sinus of Valsalva in Oriental patients. J Thorac Cardiovasc Surg. 1990;99(2):288–98. [PubMed] [Google Scholar]
- 7.Adams JE, Sawyers JL, Scott HW., Jr. Surgical treatment of aneurysms of the aortic sinuses with aorticoatrial fistula; experimental and clinical study. Surgery. 1957;41(1):26–42. [PubMed] [Google Scholar]
- 8.Ionescu CN, Khachane V, Earle M, Marcu CB, Ghantous A, Chrissoheris M. A rare cause of systolic murmur: unruptured right sinus of Valsalva aneurysm with right ventricular outflow tract obstruction and supracristal ventricular septal defect. Conn Med. 2010;74(4):211–3. [PubMed] [Google Scholar]
- 9.Liang CD, Chang JP, Kao CL. Unruptured sinus of Valsalva aneurysm with right ventricular outflow tract obstruction associated with ventricular septal defect. Cathet Cardiovasc Diagn. 1996;37(2):158–61. doi: 10.1002/(SICI)1097-0304(199602)37:2<158::AID-CCD11>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- 10.Marques KM, De Cock CC, Visser CA. Isolated unruptured aneurysm of the right sinus of Valsalva causing right ventricular outflow obstruction. Heart. 1999;81(4):447–8. doi: 10.1136/hrt.81.4.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bulkley BH, Hutchins GM, Ross RS. Aortic sinus of Valsalva aneurysms simulating primary right-sided valvular heart disease. Circulation. 1975;52(4):696–9. doi: 10.1161/01.cir.52.4.696. [DOI] [PubMed] [Google Scholar]
- 12.Thankachen R, Gnanamuthu R, Doshi H, Shukla V, Korula RJ. Unruptured aneurysm of the sinus of Valsalva presenting with right ventricular outflow obstruction. Tex Heart Inst J. 2003;30(2):152–4. [PMC free article] [PubMed] [Google Scholar]
- 13.Roman MJ, Rosen SE, Kramer-Fox R, Devereaux RB. Prognostic significance of the pattern of aortic root dilation in the Marfan syndrome. J Am Coll Cardiol. 1993;22(5):1470–6. doi: 10.1016/0735-1097(93)90559-j. [DOI] [PubMed] [Google Scholar]
- 14.Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE, Jr et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27–e129. doi: 10.1016/j.jacc.2010.02.015. [DOI] [PubMed] [Google Scholar]
- 15.Feldman DN, Roman MJ. Aneurysms of the sinuses of Valsalva. Cardiology. 2006;106(2):73–81. doi: 10.1159/000092635. [DOI] [PubMed] [Google Scholar]