

Abstract
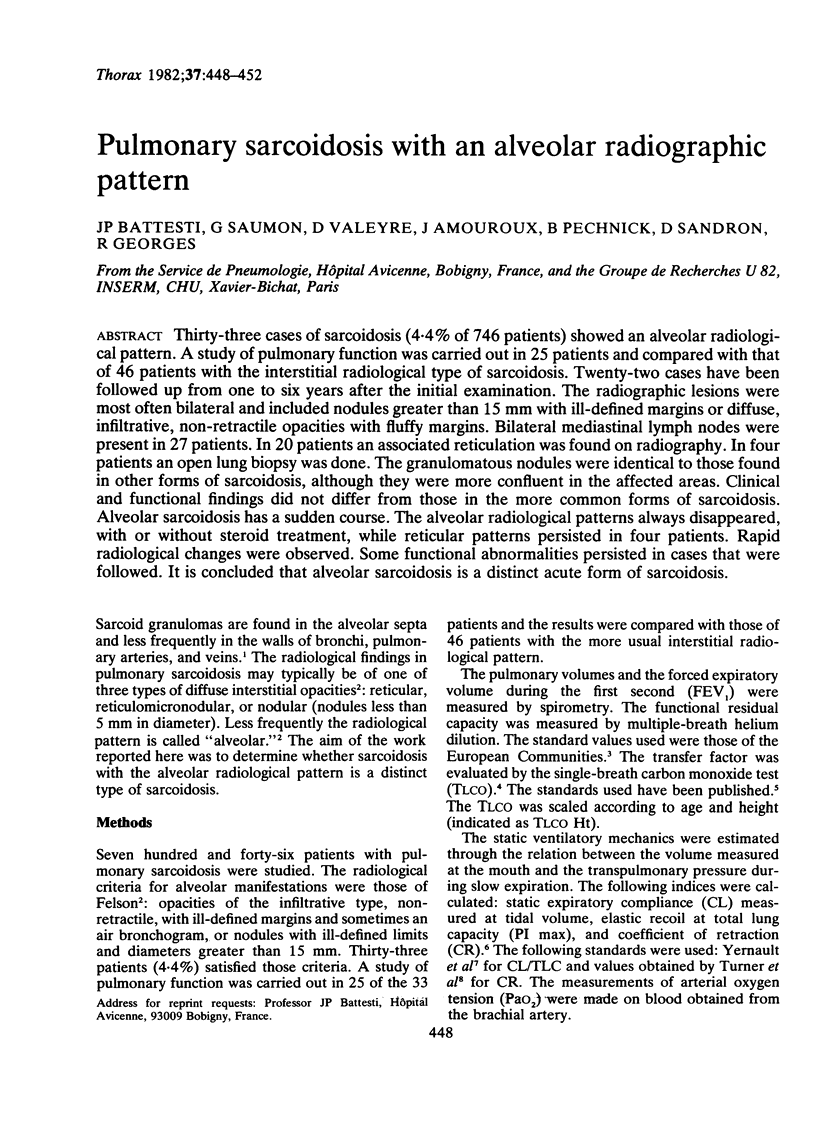
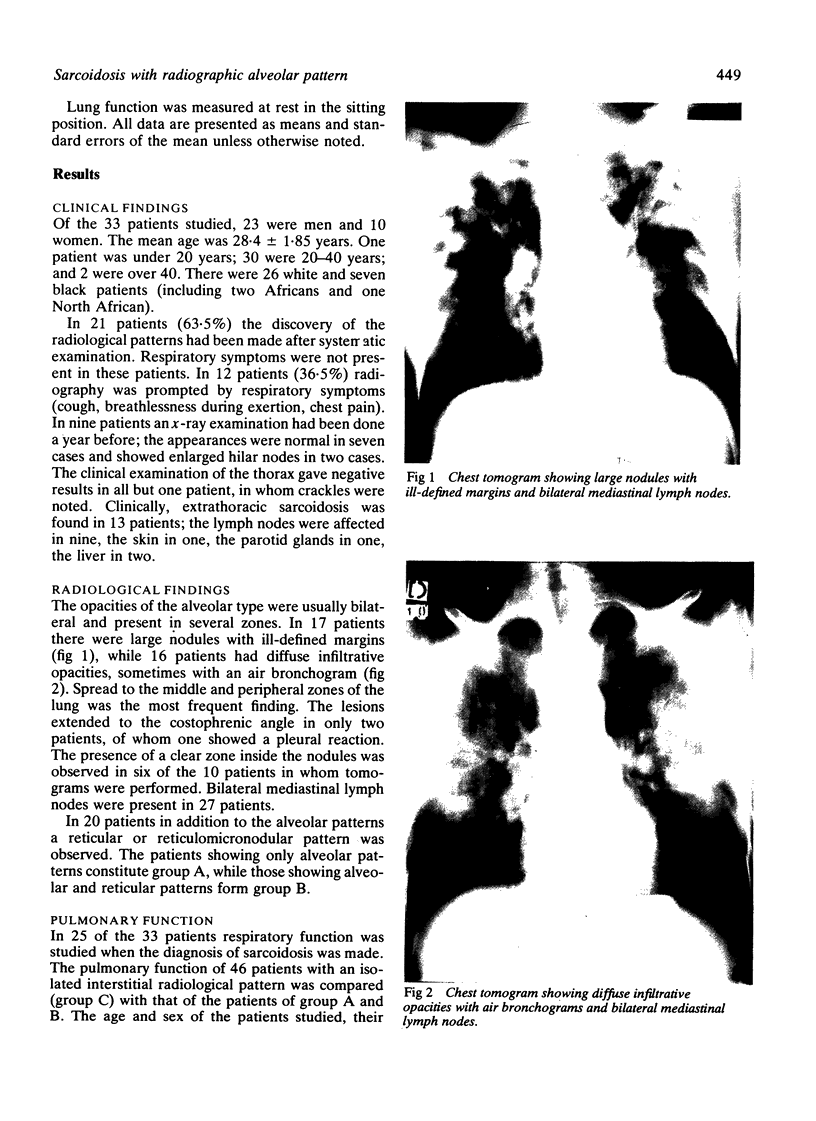
Thirty-three cases of sarcoidosis (4.4% of 746 patients) showed an alveolar radiological pattern. A study of pulmonary function was carried out in 25 patients and compared with that of 46 patients with the interstitial radiological type of sarcoidosis. Twenty-two cases have been followed up from one to six years after the initial examination. The radiographic lesions were most often bilateral and included nodules greater than 15 mm with ill-defined margins or diffuse, infiltrative, non-retractile opacities with fluffy margins. Bilateral mediastinal lymph nodes were present in 27 patients. In 20 patients an associated reticulation was found on radiography. In four patients an open lung biopsy was done. The granulomatous nodules were identical to those found in other forms of sarcoidosis, although they were more confluent in the affected areas. Clinical and functional findings did not differ from those in the more common forms of sarcoidosis. Alveolar sarcoidosis has a sudden course. The alveolar radiological patterns always disappeared, with or without steroid treatment, while reticular patterns persisted in four patients. Rapid radiological changes were observed. Some functional abnormalities persisted in cases that were followed. It is concluded that alveolar sarcoidosis is a distinct acute form of sarcoidosis.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BLAKEMORE W. S., FORSTER R. E., MORTON J. W., OGILVIE C. M. A standardized breath holding technique for the clinical measurement of the diffusing capacity of the lung for carbon monoxide. J Clin Invest. 1957 Jan;36(1 Pt 1):1–17. doi: 10.1172/JCI103402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FELSON B. Uncommon roentgen patterns of pulmonary sarcoidosis. Dis Chest. 1958 Oct;34(4):357–367. doi: 10.1378/chest.34.4.357. [DOI] [PubMed] [Google Scholar]
- Georges R., Saumon G., Loiseau A. The relationship of age to pulmonary membrane conductance and capillary blood volume. Am Rev Respir Dis. 1978 Jun;117(6):1069–1078. doi: 10.1164/arrd.1978.117.6.1069. [DOI] [PubMed] [Google Scholar]
- Gibson G. J., Pride N. B. Pulmonary mechanics in fibrosing alveolitis: the effects of lung shrinkage. Am Rev Respir Dis. 1977 Oct;116(4):637–647. doi: 10.1164/arrd.1977.116.4.637. [DOI] [PubMed] [Google Scholar]
- Kirks D. R., McCormick V. D., Greenspan R. H. Pulmonary sarcoidosis. Roentgenologic analysis of 150 patients. Am J Roentgenol Radium Ther Nucl Med. 1973 Apr;117(4):777–786. doi: 10.2214/ajr.117.4.777. [DOI] [PubMed] [Google Scholar]
- NIH conference. Pulmonary sarcoidosis: a disease characterized and perpetuated by activated lung T-lymphocytes. Ann Intern Med. 1981 Jan;94(1):73–94. doi: 10.7326/0003-4819-94-1-73. [DOI] [PubMed] [Google Scholar]
- Onal E., Lopata M., Lourenço R. V. Nodular pulmonary sarcoidosis. Clinical, roentgenographic, and physiologic course in five patients. Chest. 1977 Sep;72(3):296–300. doi: 10.1378/chest.72.3.296. [DOI] [PubMed] [Google Scholar]
- Rohatgi P. K., Schwab L. E. Primary acute pulmonary cavitation in sarcoidosis. AJR Am J Roentgenol. 1980 Jun;134(6):1199–1203. doi: 10.2214/ajr.134.6.1199. [DOI] [PubMed] [Google Scholar]
- Romer F. K. Sarcoidosis with large nodular lesions simulating pulmonary metastases. An analysis of 126 cases of intrathoracic sarcoidosis. Scand J Respir Dis. 1977;58(1):11–16. [PubMed] [Google Scholar]
- Sahn S. A., Schwarz M. I., Lakshminarayan S. Sarcoidosis: the significance of an acinar pattern on chest roentgenogram. Chest. 1974 Jun;65(6):684–687. doi: 10.1378/chest.65.6.684. [DOI] [PubMed] [Google Scholar]
- Saumon G., Georges R., Loiseau A., Turiaf J. Membrane diffusing capacity and pulmonary capillary blood volume in pulmonary sarcoidosis. Ann N Y Acad Sci. 1976;278:284–291. doi: 10.1111/j.1749-6632.1976.tb47039.x. [DOI] [PubMed] [Google Scholar]
- Schlueter D. P., Immekus J., Stead W. W. Relationship between maximal inspiratory pressure and total lung capacity (coefficient of retraction) in normal subjects and in patients with emphysema, asthma, and diffuse pulmonary infiltration. Am Rev Respir Dis. 1967 Oct;96(4):656–665. doi: 10.1164/arrd.1967.96.4.656. [DOI] [PubMed] [Google Scholar]
- Sharma O. P., Hewlett R., Gordonson J. Nodular sarcoidosis: an unusual radiographic appearance. Chest. 1973 Aug;64(2):189–192. doi: 10.1378/chest.64.2.189. [DOI] [PubMed] [Google Scholar]
- Shigematsu N., Emori K., Matsuba K., Harada S., Takahashi T. Clinicopathologic characteristics of pulmonary acinar sarcoidosis. Chest. 1978 Feb;73(2):186–188. doi: 10.1378/chest.73.2.186. [DOI] [PubMed] [Google Scholar]
- Tellis C. J., Putnam J. S. Cavitation in large multinodular pulmonary disease a rare manifestation of sarcoidosis. Chest. 1977 Jun;71(6):792–793. doi: 10.1378/chest.71.6.792. [DOI] [PubMed] [Google Scholar]
- Turiaf J., Johns C. J., Terstein A. S., Tsuji S., Wurm K. The problem of the treatment of sarcoidosis: Report of the Subcommittee on Therapy. Ann N Y Acad Sci. 1976;278:743–751. doi: 10.1111/j.1749-6632.1976.tb47091.x. [DOI] [PubMed] [Google Scholar]
- Turner J. M., Mead J., Wohl M. E. Elasticity of human lungs in relation to age. J Appl Physiol. 1968 Dec;25(6):664–671. doi: 10.1152/jappl.1968.25.6.664. [DOI] [PubMed] [Google Scholar]
- Yernault J. C., Baran D., Englert M. Effect of growth and aging on the static mechanical lung properties. Bull Eur Physiopathol Respir. 1977 Nov-Dec;13(6):777–788. [PubMed] [Google Scholar]