

Abstract
Objective
The purpose of this retrospective study was to investigate short-term and long-term skeletodental outcomes of Class III activator treatment.
Methods
A Class III activator treatment group (AG) comprised of 22 patients (9 boys, 13 girls) was compared with a Class III control group (CG) comprised of 17 patients (6 boys, 11 girls). The total treatment period was divided into three stages; the initial stage (T1), the post-activator treatment or post-mandibular growth peak stage (T2), and the long-term follow-up stage (T3). Cephalometric changes were evaluated statistically via the Mann-Whitney U-test and the Friedman test.
Results
The AG exhibited significant increases in the SNA angle, ANB angle, Wits appraisal, A point-N perpendicular, Convexity of A point, and proclination of the maxillary incisors, from T1 to T2. In the long-term follow-up (T1-T3), the AG exhibited significantly greater increases in the ANB angle, Wits appraisal, and Convexity of A point than the CG.
Conclusions
Favorable skeletal outcomes induced during the Class III activator treatment period were generally maintained until the long-term follow-up period of the post-mandibular growth peak stage.
Keywords: Class III activator, Skeletodental changes
INTRODUCTION
Class III malocclusion is a more common clinical problem in Mongolian populations than in Caucasian populations.1 The prevalence of Class III malocclusion ranges from 2.3% to 16.7% in Asia,2,3,4 and in a series of studies undertaken in Korea 38.1% to 48.3% of the patients who visited a clinic seeking orthodontic treatment had Class III malocclusion.5,6,7 Similarly, survey results pertaining to the distribution of orthodontic patients in Wonkwang University Dental Hospital revealed that Class III patients comprised 34.2% of them, and of these, 33.6% were growing patients.
Treatment of Class III malocclusions in growing patients is generally considered one of the most complex challenges in orthodontics.8,9,10,11 Early intervention treatment in patients with Class III malocclusion is controversial, for reasons relating to unpredictable prognoses, reduced efficiency arising from the associated long treatment times, and patient compliance problems. 1,12,13 In view of these potential problems, the success or otherwise of several orthopedic treatments including chin caps, facemasks, and functional appliances have been studied.14,15,16,17 However, early intervention treatment of growing patients with skeletal Class III malocclusion via orthodontic or orthopedic modalities has become a common practice, favored for reasons relating to effectiveness, functional rehabilitation, and patients' quality of life; including their emotional development.18,19
Successful clinical results of functional appliance therapy have been reported by several authors.14,20,21 Examples of functional orthopedic appliances for Class III treatment are the Fränkel function regulator III, Bionator III, and Class III activator.
Many previous studies have investigated the effects of Class III activator therapy.20,22,23,24,25 Several of these have reported short-term treatment effects, including improvement of patient profile with significant clockwise rotation of the mandible and proclination of the maxillary incisors.22,23,24,25 However, few studies have investigated the long-term effects of this treatment modality.20
In the current study, we investigated the short-term and long-term skeletodental changes associated with Class III activator treatment in growing patients.
MATERIALS AND METHODS
Patient selection
Patients in the study groups were selected from the growing Korean patients diagnosed by the Department of Orthodontics, Wonkwang University Dental Hospital from July 2000 to June 2011. This retrospective study was approved by the institutional review board of the Dental Hospital of Wonkwang University (approval number WKDIRB201408-01).
Patients were classified into either a Class III activator treatment group (AG) or a Class III control group (CG). The AG was comprised of 22 patients (9 boys, 13 girls) treated with Class III activator over the mandibular growth peak without combination or alteration with other growth modification appliances. The CG was comprised of 17 patients (6 boys, 11 girls) who were not treated with removable appliances that could modify growth or mandibular position (Table 1).
Table 1. Demographics of the study groups.
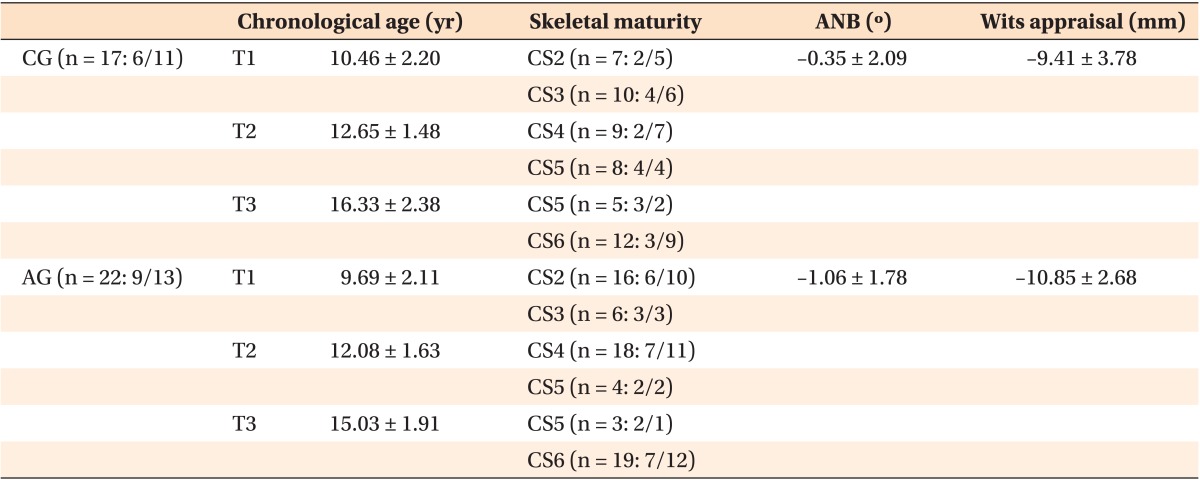
Values are presented as mean ± standard deviation or total number: number of boys/girls.
AG, Class III activator treatment group; CG, Class III control group; T1, initial stage; T2, post-activator treatment or post-mandibular growth peak stage; T3, long-term follow-up stage.
Inclusion criteria included skeletal Class III discrepancy beyond the normal range (normal mean ± 1 standard deviation) based on the ANB angle and Wits appraisal measurements according to individual growth state; premandibular growth peak stage at the time of diagnosis; no previous orthodontic treatment; no craniofacial anomalies including cleft lip and palate; and availability of adequate specific supplementary data including diagnostic records, treatment progress notes, and lateral cephalometric radiographs.
Skeletal maturity
The total treatment period was divided into three stages; the initial stage (T1), the post-activator treatment or post-mandibular growth peak stage (T2), and the long-term follow-up stage (T3). Skeletal maturation was determined by lateral cephalometric radiographs using a modified version of the cervical vertebral maturation method26 (modified CVM method), independently of chronologic age. The stages of cervical vertebral maturation were all classified by the same investigator (HKR).
All patients were in pre-mandibular growth peak stage (CS1-CS3) at T1, post-mandibular growth peak stage (CS4-CS5) at T2, and more than a year after mandibular growth peak stage (CS5-CS6) at T3.
Treatment protocols
In the AG, the construction bite of the activator was taken in the most posterior mandibular position with various heights, according to the patients' individual conditions. The appliances fitted well in the patients' mouths. Clinicians instructed the patients to wear the appliances for at least 14 hours per day. All AG patients were treated via the same protocol by the residents, under the supervision of faculty supervisors. AG patients wore the activator consistently until post-mandibular growth peak stage (T2), at which time the second phase of fixed appliance treatment was recommended. After activator treatment, comprehensive orthodontic treatment was initiated in 18 patients (8 boys, 10 girls). Orthodontic treatment combined with orthognathic surgery was recommended to 4 other patients (1 boy, 3 girls).
CG patients were treated via various means depending on their individual conditions. Four girls were observed for habit control, 5 patients (3 boys, 2 girls) were treated with removable appliances for dental alignment, and 8 patients (3 boys, 5 girls) initially underwent fixed appliance treatment on only their maxillary dentition. After T2, 13 patients (5 boys, 8 girls) received comprehensive orthodontic treatment and 4 patients (1 boy, 3 girls) were observed regularly for possible further growth of the jaws. Orthodontic treatment combined with orthognathic surgery was recommended to 3 patients (1 boy, 2 girls) at T3.
Cephalometric analysis
Lateral cephalometric radiographs were acquired via a Planmeca PM 2002 cc Proline Ceph (Planmeca, Helsinki, Finland) until October 31st 2002, then via a Planmeca Promax Dimax3 Ceph (Planmeca) thereafter, with the patients in natural head position. Lateral cephalometric radiographs were taken at T1, T2, and T3 in each patient. Original films taken with the Planmeca PM 2002 cc Proline Ceph were scanned and converted into a digital format via a Vidar Diagnostic Pro Plus Film Digitizer (Vidar Systems Corporation, Herndon, VA, USA).
All lateral cephalometric radiographs were digitized and calculated using V-ceph 6.0 software (Osstem Implant Co., Ltd., Seoul, Korea) by the same investigator (HKR). Magnification was corrected for all the lateral cephalometric radiographs. Cephalometric analysis was conducted to identify the changes in 20 measurements (Figures 1 and 2, and Table 2).
Figure 1. Landmarks and reference planes. S, Sella; N, Nasion; Po, Porion; Or, Orbitale; Co, Condylion; Ar, Articulare; ANS, anterior nasal spine; PNS, posterior nasal spine; A, Point A; B, Point B; U1E, incisal edge of maxillary central incisor (U1); U1A, root apex of U1; L1E, incisal edge of mandibular incisor (L1); L1A, root apex of L1; Pog, Pogonion; Gn, Gnathion; Me, Menton; Go, Gonion; Sella-Nasion plane (SN plane), line from S to N; Frankfort horizontal plane (FH plane), line from Po to Or; Palatal plane, line from PNS to ANS; Functional occlusal plane, line drawn along the maximum intercuspation of the posterior teeth; N-perpendicular plane (N-perp plane), perpendicular line to FH plane passing through Nasion; Facial plane, line from N to Pog; Mandibular plane, line from Go to Me.

Figure 2. Cephalometric measurements. 1, SNA; 2, SNB; 3, ANB; 4, Palatal plane angle; 5, Mn. plane angle; 6, Gonial angle; 7, lower gonial angle; 8, AB to Mn. plane angle; 9, Y-axis angle; 10, ODI; 11, APDI; 12, U1 to SN; 13, U1 to FH; 14, IMPA; 15, Wits appraisal; 16, Mx. length; 17, Mn. length; 18, A-N perpend; 19, Pog-N perpend; 20, Convexity of A.

Table 2. Definitions of cephalometric measurements.
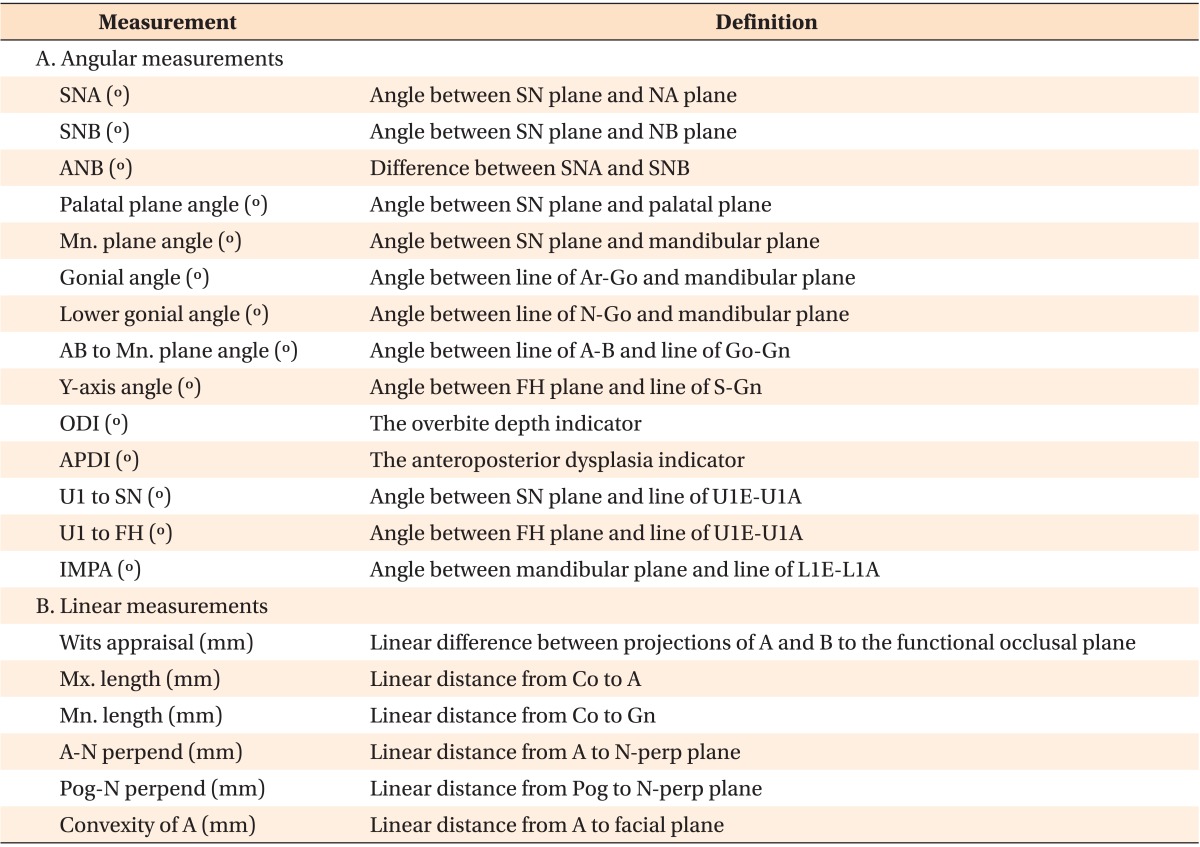
Mx., Maxillary; Mn., mandibular.
Refer to Figure 1 for the location of each landmarks.
Statistical analysis
Prior to statistical analysis, intra-examiner variation was evaluated. Evaluations of stages of the cervical vertebrae were performed twice, 2 weeks apart, and there was no difference. Also, 10 randomly selected radiographs were retraced and remeasured by the same investigator (HKR) 2 weeks after the initial analysis, the paired t-test was used to compare the two data-sets of registrations, and there was no significant difference between the data-sets (p > 0.05). All of the intraclass correlational coefficients were above 0.904, suggesting that intra-examiner agreement was excellent.
Descriptive statistics were calculated for all cephalometric measurements at T1, T2, and T3 in the AG and CG. Statistical analyses were performed using the Statistical Package for Social Sciences software (version 12.0; SPSS, Chicago, IL, USA). Shapiro-Wilks test revealed that the calculated measurements were not normally distributed, thus, the nonparametric Mann-Whitney U-test, Friedman test, and Wilcoxon signed rank test with Bonferroni correction for post-hoc comparisons were used.
RESULTS
No statistically significant differences were found between the skeletodental measurements of the AG and CG at T1 (Table 3).
Table 3. Statistical comparison of initial cephalometric measurements (T1) between Class III activator treatment group (AG) and Class III control group (CG).
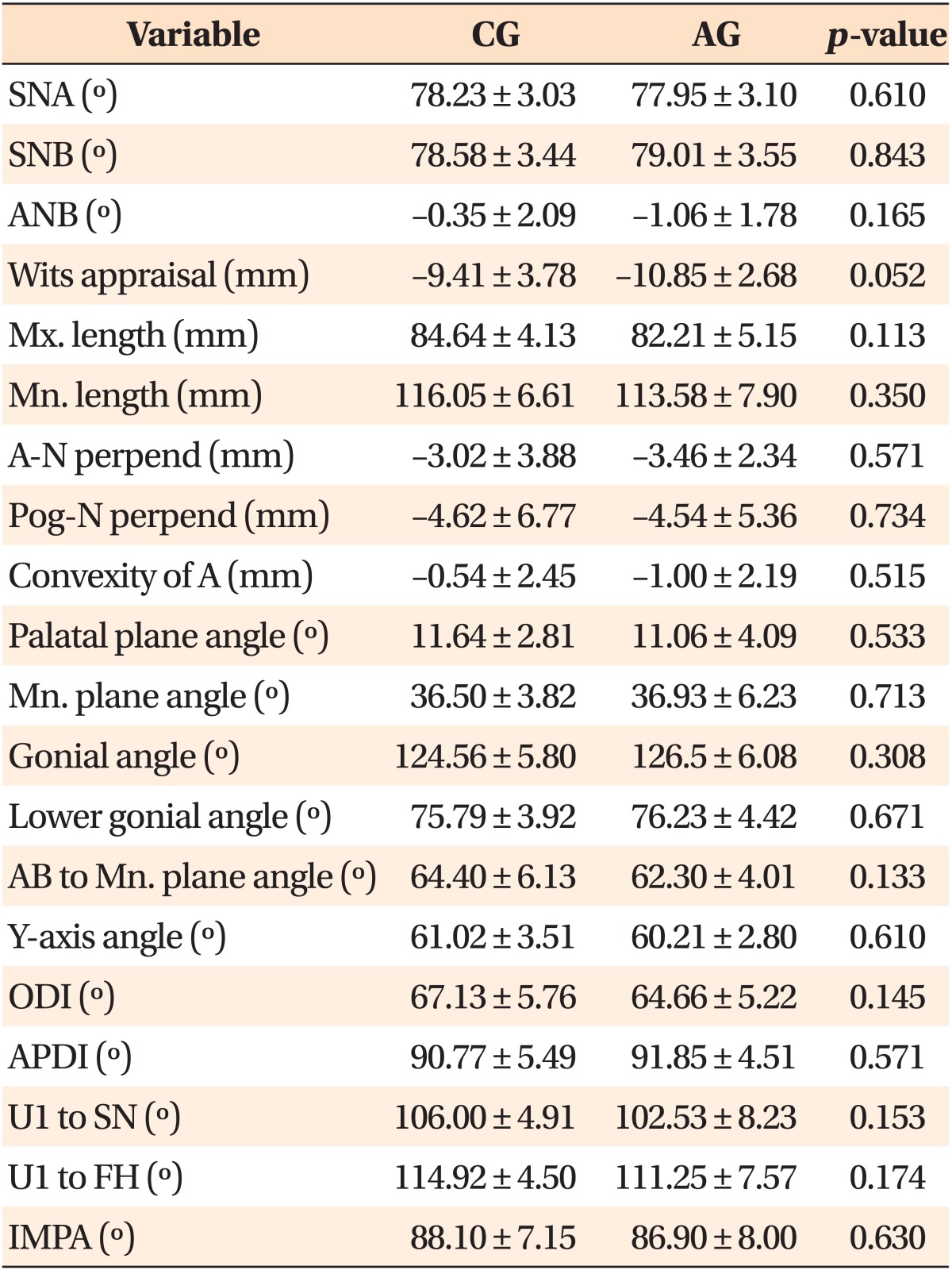
Values are presented as mean ± standard deviation.
Mx., Maxillary; Mn., mandibular.
Mann-Whitney U-test was used.
Refer to Table 2 for the definition of each measurements.
Comparison of measurements within each group
Descriptive data and statistical comparisons for cephalometric measurements at T1, T2, and T3 are presented in Table 4. In the AG, the following measurements changed statistically significantly during the periods: SNA, ANB, Wits appraisal, Mx. length, Mn. length, A-N perpend, Pog-N perpend, Convexity of A, Gonial angle, U1 to SN, and U1 to FH. Of these measurements, SNA, ANB, Convexity of A, U1 to SN, and U1 to FH increased significantly between T1 and T2. Wits appraisal, Mx. length, Mn. length, and A-N perpendicular gradually increased throughout the T1, T2, and T3 periods.
Table 4. Cephalometric measurements of Class III activator treatment group (AG) and Class III control group (CG).
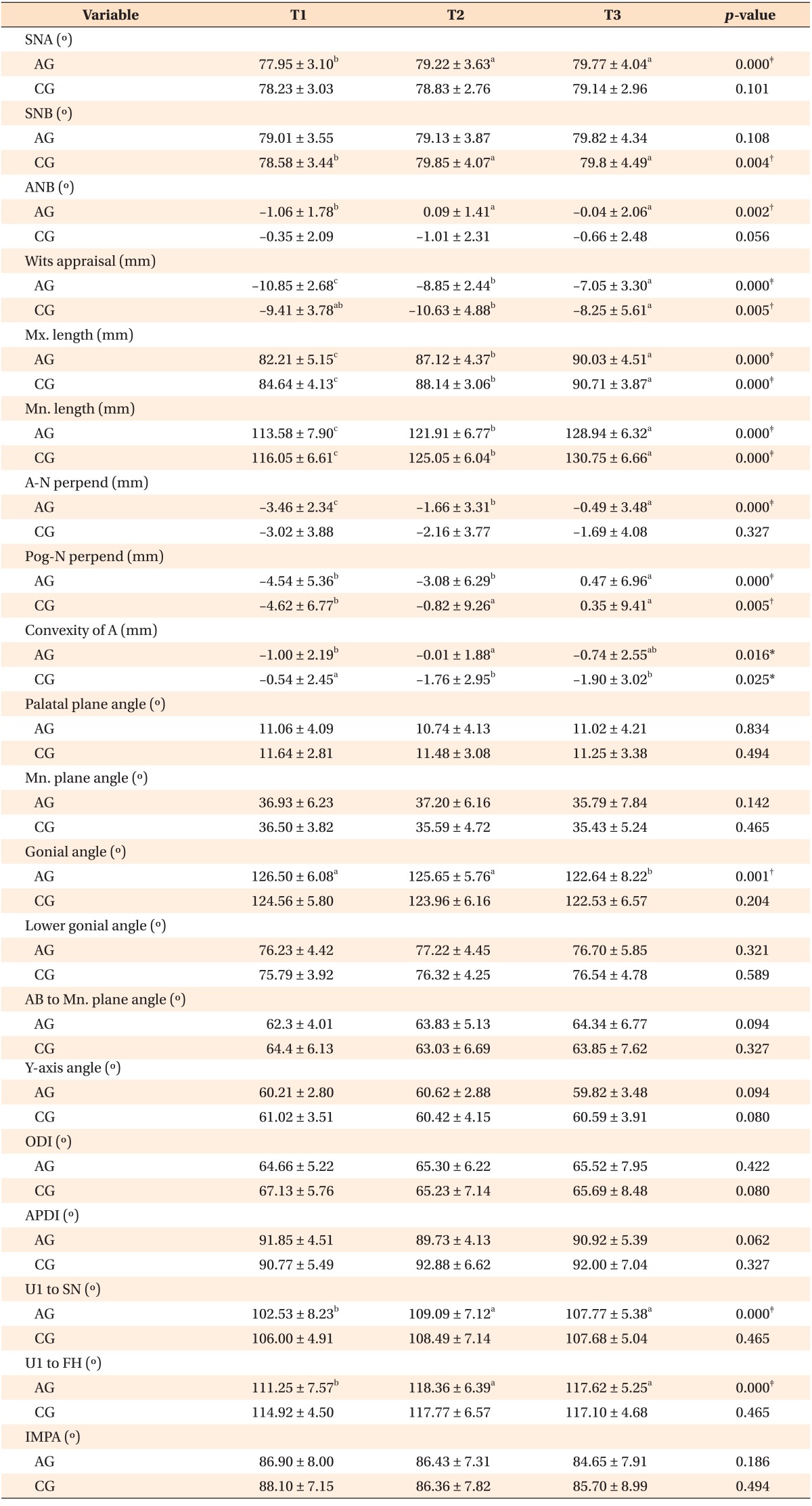
Values are presented as mean ± standard deviation.
T1, Initial stage; T2, post-activator treatment or post-mandibular growth peak stage; T3, long-term follow-up stage.
Friedman test and Wilcoxon signed rank test (Bonferroni correction) for post-hoc comparisons were used. Means with different letters are significantly different according to the Wilcoxon signed rank test (Bonferroni correction): a>b>c.
*p<0.05; †p<0.01; ‡p<0.001.
Refer to Table 2 for the definition of each measurements.
In the CG, the following measurements changed statistically significantly during the periods: SNB, Wits appraisal, Mx. length, Mn. length, Pog-N perpend, and Convexity of A. Of these measurements, SNB, and Pog-N perpend significantly increased between T1 to T2, while Convexity of A significantly decreased. Wits appraisal significantly increased between T2 and T3. Mx. length and Mn. length gradually increased throughout the T1, T2, and T3 periods.
Comparisons of changes between the groups
Descriptive data and statistical comparisons of the cephalometric changes in both groups in each period are presented in Table 5. From T1 to T2, SNB of the AG increased significantly less than that of the CG, resulting in an increase in ANB in the AG that was greater than that of the CG. Wits appraisal, Convexity of A, AB to Mn. plane angle, Y-axis angle, and ODI also increased significantly more in the AG than in the CG. There was a significantly larger decrease in APDI in the AG than in the CG. U1 to SN, and U1 to FH increased significantly more in the AG than in the CG. There were no significant differences in the changes from T2 to T3. From T1 to T3, ANB, Wits appraisal, and Convexity of A increased significantly more in the AG than in the CG. Compared with the CG, a significantly larger change in U1 to FH was observed in the AG.
Table 5. Statistical comparison of cephalometric measurements changes between Class III activator treatment group (AG) and Class III control group (CG) during the periods.
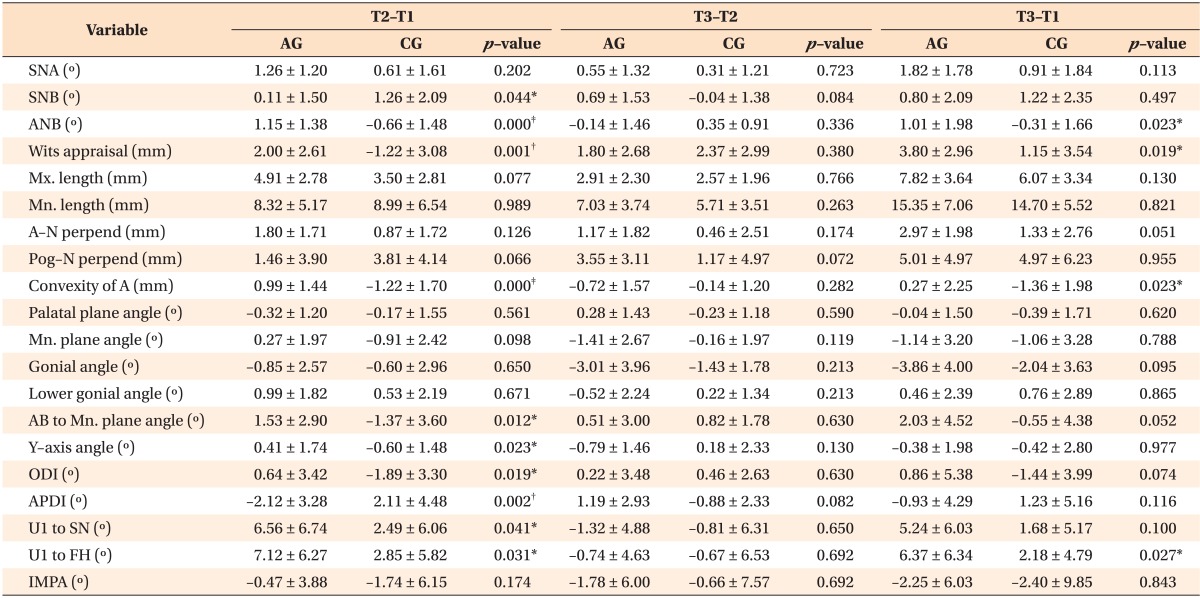
Values are presented as mean ± standard deviation.
Mann-Whitney U-test was used.
T1, Initial stage; T2, post-activator treatment or post-mandibular growth peak stage; T3, long-term follow-up stage.
*p<0.05; †p<0.01; ‡p<0.001
Refer to Table 2 for the definition of each measurements.
DISCUSSION
The objective of this study was to determine short-term and long-term skeletodental changes in growing patients in a Class III AG and a Class III CG. This study revealed that Class III activator therapy resulted in an improved jaw relationship and proclinated maxillary incisors (Table 4). Compared with the CG, skeletodental changes in the AG occurred during the activator treatment period, and remained without substantial changes during the long-term follow-up period (Table 5).
The study has some limitations, most of which stem from the small sample size and retrospective study design. It was difficult to obtain control data from completely untreated patients with equivalent skeletodental conditions, due to ethical considerations. Accordingly, patients treated with habit control and/or dental alignment excluding orthopedic treatment were included in the CG. Furthermore, radiographic images were obtained by two methods, from original films and digital images, increasing the possibility of discrepancies in the cephalometric analysis. In a previous study comparing scanned lateral cephalograms with corresponding original radiographs, some distortions were found.27 However, the authors considered that the use of scanned cephalograms was valid, because the relatively small discrepancies were deemed clinically insignificant.
The appraisal of skeletal maturity in both groups was performed by evaluating stages of the cervical vertebrae, using a modified CVM method.26 In this study, the modified CVM method was applied to assess whether the pubertal spurt in mandibular growth had started or finished. The appraisal of skeletal maturity based on cervical vertebral maturation can be helpful for determining the completion of active growth in studies dealing with the long-term effects of orthopedic treatment strategies.26
Previous studies have shown that the greatest increase in mandibular length occurs during the pubertal growth spurt, which happens during the interval between CS3 and CS4.28,29 The pubertal peak of patients with skeletal Class III malocclusion reportedly lasts longer than that of patients with skeletal Class I malocclusion.30 Therefore, growth modification treatment should be maintained during this growth period, and a long period of observation of patients should be undertaken, until the active growth period is over. Accordingly, patients undergoing maintained activator treatment over the mandibular growth peak were included in this study (Table 1).
The significant changes in SNA, and A-N perpend were associated with forward displacement of the maxilla in the AG (Table 4). Nonetheless, these treatment changes in the AG did not result in significant differences between the AG and CG (Table 5). The insignificant mean change in the measurements related to maxillary growth also suggests that maxillary growth could be caused by both natural factors and activator treatment. This point of view corresponds with previous studies.20,24
Based on assessment of the effect of Class III activator treatment on mandible changes, undertaken by comparing the skeletal changes within each group, we could assume that it prevents the anteroposterior relationship of the mandible from getting worse (Table 4). In particular, the measurements that differed significantly between both groups, such as SNB, ANB, Wits appraisal, Convexity of A, and AB to Mn. plane angle were associated with significantly greater improvement of the jaw relationship in the AG (Table 5). Similar findings relating to Class III activator treatment have been described in other studies.22,23,25 The clockwise rotation of the mandible in the AG had the additional effect of repositioning of the chin downward and backward, and developed facial convexity that contributed to improvement of profile.
Dental changes in the maxilla such as U1 to SN, and U1 to FH were evident in the AG (Table 4). The proclination of the maxillary incisors caused by Class III activator treatment was similar to the dental compensation seen in Class III malocclusion. Furthermore, in terms of dental compensation, proclination of the maxillary incisors contributed to a positive overjet in untreated skeletal Class III patients.31
The observed changes associated with Class III activator therapy, particularly clockwise rotation of the mandible and proclination of maxillary incisors, facilitate the formation of a positive overjet by the Class III camouflage treatment. Moreover, some authors believe that early correction of an anterior crossbite has a positive effect on the sagittal development of the maxilla, developing the bone according to its endogenous growth potential.20 In this respect, correction of the jaw relationship by Class III activator therapy induces harmonious skeletal and dental changes.
From T1 to T3, measurement differences between the AG and CG reflecting skeletal changes, such as ANB, Wits appraisal, and Convexity of A showed that the treatment effects were maintained during the second phase of treatment (Table 5). This showed that helpful skeletal outcomes induced by Class III activator during the activator treatment period were generally maintained until the long-term follow-up period of the post-mandibular growth peak stage.
CONCLUSION
Favorable skeletal changes were achieved by Class III activator therapy that started before the mandibular growth peak and continued over the mandibular growth peak. These treatment effects of Class III activator therapy were generally maintained during the long-term follow-up period of the post-mandibular growth peak stage.
Footnotes
The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
References
- 1.Graber TM, Rakosi T, Petrovic AG. Dentofacial orthopedics with functional appliances. 2nd ed. St. Louis: Mosby; 1997. [Google Scholar]
- 2.Suhr CH, Nahm DS, Chang YI. Epidemiologic study of the prevalence of malocclusion in Korean. Korean J Orthod. 1984;14:33–37. [Google Scholar]
- 3.Kang HK, Ryu YK. A study on the prevalence of malocclusion of Yonsei University students in 1991. Korean J Orthod. 1992;22:691–701. [Google Scholar]
- 4.Miyajima K, McNamara JA, Jr, Sana M, Murata S. An estimation of craniofacial growth in the untreated Class III female with anterior crossbite. Am J Orthod Dentofacial Orthop. 1997;112:425–434. doi: 10.1016/s0889-5406(97)70051-9. [DOI] [PubMed] [Google Scholar]
- 5.Yang WS. The study on the orthodontic patients who visited Department of Orthodontics, Seoul National University Hospital during last 10 years (1985-1994) Korean J Orthod. 1995;25:497–509. [Google Scholar]
- 6.Yu HS, Ryu YK, Lee JY. A study on the distributions and trends in malocclusion patients from department of orthodontics, college of dentistry, Yonsei university. Korean J Orthod. 1999;29:267–276. [Google Scholar]
- 7.Hwang MS, Yoon YJ, Kim KW. An epidemiologic study on the orthodontic patients who visited Department of Orthodontics, Chosun University Dental Hospital last 10 years (1990-1999) Korean J Orthod. 2001;31:283–300. [Google Scholar]
- 8.Son MH, Chang YI. Evaluation of various cephalometric measurements to predict the prognosis of early Class III malocclusion treatment. Korean J Orthod. 2004;34:205–218. [Google Scholar]
- 9.Seehra J, Fleming PS, Mandall N, Dibiase AT. A comparison of two different techniques for early correction of Class III malocclusion. Angle Orthod. 2012;82:96–101. doi: 10.2319/032011-197.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chen L, Chen R, Yang Y, Ji G, Shen G. The effects of maxillary protraction and its long-term stability--a clinical trial in Chinese adolescents. Eur J Orthod. 2012;34:88–95. doi: 10.1093/ejo/cjq185. [DOI] [PubMed] [Google Scholar]
- 11.Morales-Fernández M, Iglesias-Linares A, Yañez-Vico RM, Mendoza-Mendoza A, Solano-Reina E. Boneand dentoalveolar-anchored dentofacial orthopedics for Class III malocclusion: new approaches, similar objectives?: a systematic review. Angle Orthod. 2013;83:540–552. doi: 10.2319/051312-392.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Proffit WR, Fields HW, Sarver DM. Contemporary orthodontics. 5th ed. St. Louis: Mosby; 2013. [Google Scholar]
- 13.Esenlik E, Cahide A, Gayem EA, Yavuz F. Maxillary protraction using skeletal anchorage and intermaxillary elastics in Skeletal Class III patients. Korean J Orthod. 2015;45:95–101. doi: 10.4041/kjod.2015.45.2.95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Garattini G, Levrini L, Crozzoli P, Levrini A. Skeletal and dental modifications produced by the Bionator III appliance. Am J Orthod Dentofacial Orthop. 1998;114:40–44. doi: 10.1016/s0889-5406(98)70235-5. [DOI] [PubMed] [Google Scholar]
- 15.Arman A, Toygar TU, Abuhijleh E. Profile changes associated with different orthopedic treatment approaches in Class III malocclusions. Angle Orthod. 2004;74:733–740. doi: 10.1043/0003-3219(2004)074<0733:PCAWDO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Abdelnaby YL, Nassar EA. Chin cup effects using two different force magnitudes in the management of Class III malocclusions. Angle Orthod. 2010;80:957–962. doi: 10.2319/022210-110.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu ZP, Li CJ, Hu HK, Chen JW, Li F, Zou SJ. Efficacy of short-term chincup therapy for mandibular growth retardation in Class III malocclusion. Angle Orthod. 2011;81:162–168. doi: 10.2319/050510-244.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sugawara J, Aymach Z, Hin H, Nanda R. One-phase vs 2-phase treatment for developing Class III malocclusion: a comparison of identical twins. Am J Orthod Dentofacial Orthop. 2012;141:e11–e22. doi: 10.1016/j.ajodo.2011.05.023. [DOI] [PubMed] [Google Scholar]
- 19.Souki BQ, Figueiredo DS, Lima IL, Oliveira DD, Miguel JA. Two-phase orthodontic treatment of a complex malocclusion: giving up efficiency in favor of effectiveness, quality of life, and functional rehabilitation. Am J Orthod Dentofacial Orthop. 2013;143:547–558. doi: 10.1016/j.ajodo.2012.02.027. [DOI] [PubMed] [Google Scholar]
- 20.Satravaha S, Taweesedt N. Stability of skeletal changes after activator treatment of patients with class III malocclusions. Am J Orthod Dentofacial Orthop. 1999;116:196–206. doi: 10.1016/s0889-5406(99)70218-0. [DOI] [PubMed] [Google Scholar]
- 21.Levin AS, McNamara JA, Jr, Franchi L, Baccetti T, Fränkel C. Short-term and long-term treatment outcomes with the FR-3 appliance of Fränkel. Am J Orthod Dentofacial Orthop. 2008;134:513–524. doi: 10.1016/j.ajodo.2006.10.036. [DOI] [PubMed] [Google Scholar]
- 22.Lim JH, Nahm DS, Yang WS, Suh CH. A case report of mandibular prognathism treated with activatior. Korean J Orthod. 1976;6:79–82. [Google Scholar]
- 23.Chun YS. Clinical considerations on the effect of the Wunderer activator for correction of anterior cross bite. Taehan Chikkwa Uisa Hyophoe Chi. 1986;24:1049–1060. [PubMed] [Google Scholar]
- 24.Pak HS, Jung HS, Jung HM. Treatment of mandibular prognathism with activator; case report. J Korean Acad Pediatr Dent. 1989;16:125–131. [Google Scholar]
- 25.Pak CJ, Kim HJ, Nam SH. A comparison of the functional orthopedic appliances in the treatment of functonal anterior crossbite. J Korean Acad Pediatr Dent. 1995;22:111–127. [Google Scholar]
- 26.Baccetti T, Franchi L, McNamara JA., Jr The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;11:119–129. [Google Scholar]
- 27.Bruntz LQ, Palomo JM, Baden S, Hans MG. A comparison of scanned lateral cephalograms with corresponding original radiographs. Am J Orthod Dentofacial Orthop. 2006;130:340–348. doi: 10.1016/j.ajodo.2004.12.029. [DOI] [PubMed] [Google Scholar]
- 28.O'Reilly MT, Yanniello GJ. Mandibular growth changes and maturation of cervical vertebrae--a longitudinal cephalometric study. Angle Orthod. 1988;58:179–184. doi: 10.1043/0003-3219(1988)058<0179:MGCAMO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 29.Franchi L, Baccetti T, McNamara JA., Jr Mandibular growth as related to cervical vertebral maturation and body height. Am J Orthod Dentofacial Orthop. 2000;118:335–340. doi: 10.1067/mod.2000.107009. [DOI] [PubMed] [Google Scholar]
- 30.Kuc-Michalska M, Baccetti T. Duration of the pubertal peak in skeletal Class I and Class III subjects. Angle Orthod. 2010;80:54–57. doi: 10.2319/020309-69.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kim SJ, Kim KH, Yu HS, Baik HS. Dentoalveolar compensation according to skeletal discrepancy and overjet in skeletal Class III patients. Am J Orthod Dentofacial Orthop. 2014;145:317–324. doi: 10.1016/j.ajodo.2013.11.014. [DOI] [PubMed] [Google Scholar]