

Abstract
Mutations of the dystrophin DMD gene, essentially deletions of one or several exons, are the cause of two devastating and to date incurable diseases, Duchenne (DMD) and Becker (BMD) muscular dystrophies. Depending upon the preservation or not of the reading frame, dystrophin is completely absent in DMD, or present in either a mutated or a truncated form in BMD. DMD is a severe disease which leads to a premature death of the patients. Therapy approaches are evolving with the aim to transform the severe DMD in the BMD form of the disease by restoring the expression of a mutated or truncated dystrophin. These therapies are based on the assumption that BMD is a mild disease. However, this is not completely true as BMD patients are more or less severely affected and no molecular basis of this heterogeneity of the BMD form of the disease is yet understood. The aim of this review is to report for the correlation between dystrophin structures in BMD deletions in view of this heterogeneity and to emphasize that examining BMD patients in details is highly relevant to anticipate for DMD therapy effects.
KEYWORDS: Dystrophin, Becker muscular dystrophy, Duchenne muscular dystrophy, exon skipping, micro-dystrophin
INTRODUCTION
Mutations of the dystrophin DMD gene are the cause of two devastating and to date incurable diseases, Duchenne (DMD) and Becker (BMD) muscular dystrophies [1]. DMD gene is the longest human gene with 2.4 Megabases of DNA representing ~1% of the chromosome X DNA [2, 3]. It is localized on the locus p21 of chromosome X and codes for the protein dystrophin. This large gene comprises 79 exons separated by very large introns which explain the giant size of the gene; the mRNA of the largest isoform of dystrophin is 14 kb which is only 0.6% of the total weight of the gene. The intron 44 is 170 kb on its own. Several promoters are active in a tissue-specificity manner and lead to the expression of full length or shorter dystrophins. The full length dystrophin is expressed in all striated skeletal, smooth and cardiac muscles. Shorter isoforms are expressed in brain cells and in retina.
MUTATIONS OF THE DMD GENE
A high number of mutations of the DMD gene has been reported with ~65% being deletions of one or several exons, ~10% of duplications of exons and ~15% of single point mutations [4, 5]. Depending on the fact that mutations maintain or not of the reading frame, dystrophin will or not be present according to the Monaco rule [6]. In case of out-of-frame mutations, dystrophin is mostly deficient and this leads to the severe DMD disease. In case of in-frame mutations, dystrophin will be expressed as a mutated protein either with missense substitution or deletions or duplications of an internal part of the protein (Figure 1). These in-frame mutations mostly lead to the less severe BMD disease in accord with the Monaco rule but in certain cases, exceptions to the Monaco rule appear where a DMD phenotype with an in-frame mutation is observed. This is particularly prominent when mutations involve the N-terminal actin-binding-domain or the Cys-rich domain affecting the binding of dystrophin to F-actin or β-dystroglycan, respectively.
FIGURE 1.

Examples of mutations of the DMD gene and their consequences on the production of dystrophin and the corresponding phenotypes. The boxes represent exons. Right faces of boxes indicate that the exon codes for an entire protein sequence based on 3-bases codons (examples: exons 47, 48, 49). Curved faces indicate that the exon does not code for an entire protein sequence but that either the first or the last bases need the preceding or following exon to code a full 3-bases codon (examples: exons 50, 51, 52). BMD for Becker muscular dystrophy; DMD for Duchenne muscular dystrophy.
CLINICS, HISTOPATHOLOGY AND DYSTROPHIN IN DMD AND BMD
The first clinical signs of DMD are difficulties for young boys to walk and to climb stairs as early as 2-3 years of age. These boys never run and become wheelchair confined before their 12 years. Respiratory and cardiac impairments appear progressively and in most cases, patients do not survive after their 30 years (for a review focusing on clinics, see [7]). These clinical signs are due to a progressive muscle weakness involving all striated skeletal and cardiac muscles and are accompanied by highly elevated creatine kinase blood levels [8-10]. Similar clinical signs are observed for BMD patients but with very variable time course and severity. Some BMD patients are highly asymptomatic while some become wheelchair confined around 16 years of age. They could survive until very old ages or some of them die from an early heart failure [11, 12]. On the histological point of view, the DMD muscles show cycles of fiber necrosis and regeneration. However, regeneration is overtaken by fiber loss mechanisms and fibrosis and adipose tissue replacement are increased. Nuclei are in the normal muscle at the cell periphery and with the ongoing regeneration in DMD muscles, nuclei become centrally localized. All these features vary depending on the age of the DMD patients with fibrosis and fatty infiltration increasing with age and being highly variable in BMD. In DMD, electron microscopy reveals lesions of the plasma membrane [13] which indicates that the primary role of dystrophin is to maintain plasma membrane integrity.
Immunoblotting of dystrophin in DMD muscles reveals the total absence of dystrophin except in some revertant fibers. In BMD muscles, the expression of mutated dystrophin is observed but with highly variable extents from less than 10 % to as high as 75% of the full length expression of normal muscles [14, 15]. The direct correlation between dystrophin amount in BMD and clinical severity is not proven. However, it is recognized that measuring accurately the dystrophin level is highly challenging [16] partly explaining the lack of clear correlation between phenotype severity and dystrophin level. Other parameters could also be involved as there exist certain unexplained results which appear in contrast with the accepted rules [17].
DYSTROPHIN
Dystrophin consists of four major structural domains (Figure 2) [18, 19]. The N-terminal domain coded by exons 1 to 8 is mostly an actin-binding domain with two calponin-homology domains CH1 and CH2 [20-22]. The central part of dystrophin coded by exons 8 to 61 is made of 24 spectrin-like repeats interspaced by four hinges H1 to H4 and at the origin of the rod-shaped filament nature of dystrophin [23]. This long domain interacts with a high number of proteins among which they are the filamentous actin [24], intermediate filaments [25, 26] and microtubules [27, 28] and finally the muscular isoform of nitric oxide synthase (nNOS)[29-31] and PAR1-b [32]. In addition, this domain interacts with membrane phospholipids[33-35]. The third domain coded by exons 62 to 69 is the Cys-rich domain composed of a WW domain, two EF hands and a ZZ domain[36, 37]. This domain binds to the most important partner of dystrophin i.e. the membrane protein β-dystroglycan [38, 39] and to several other proteins such as plectin[40], ankyrin [41] and the intermediate filament protein synemin[25]. The C-terminal domain of dystrophin coded by exons 69 to 79 binds to the two cytoplasmic proteins syntrophin and dystrobrevin[42, 43].
FIGURE 2.
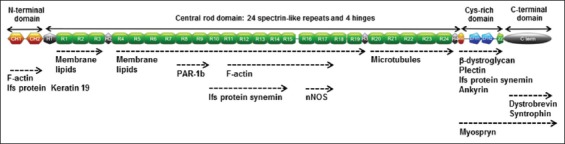
Dystrophin domains and partners. CH1 and CH2: calponin homology domains 1 and 2; H: unstructured regions called hinge; R: spectrin like repeat; WW: Tryptophan-rich domain; Z: ZZ domain; EFH: EF hand domains; PAR-1b: polarity regulating kinase 1b; nNOS: n-nitrous oxide synthase; Ifs: intermediate filaments.
Dystrophin is anchored to plasma membrane by phospholipids and β-dystroglycan which in turn interacts with extracellular matrix proteins (Figure 2). As such, dystrophin constitutes a major scaffolding protein of normal muscle which links cytoskeletal actin, microtubules and intermediate filaments to the extracellular matrix. This dystrophin scaffolding network is present at specific structures of the skeletal and heart muscle named costameres situated at the periphery of the fibers along with the transverse M- and Z-lines [44, 45]. Costameres are specifically involved in the lateral transmission of forces from the cytosol to the extracellular matrix by which they prevent plasma membrane ruptures during muscle contractions [41, 46-49].
DYSTROPHIN AND DMD AND BMD
The primary defects in both DMD and BMD are disruptions of this dystrophin scaffolding network by the absence of dystrophin in DMD or due to mutations that ablate part of the protein as in BMD. The transmission of forces from the cytosol to the extracellular matrix at the costamere is impaired, leading to frequent ruptures of plasma membrane during contractions [13, 50]. This leads to leakage of cellular components such as creatine kinase from the interior of the muscle cells which explains the high plasma membrane creatine kinase levels in blood of children suffering from DMD. In addition, these ruptures of plasma membrane increase inside fluxes of calcium which subsequently activate calcium-dependent proteases [51].
It is remarkable that a primary defect i.e. the dystrophin deficit or mutation induces a progressive muscle impairment demonstrating that muscle is able to function without dystrophin but is not able to resist forces in the long time. That signifies that the therapy strategies could be very large from inducing dystrophin expression to compensatory therapies such as increasing blood flow with NO mimetic, increasing regeneration potential, surrogate protein expression… As well, the observation of the progression of the disease in BMD patients indicates that dystrophin could sustain partly its function even with mutations that ablate part of its central domain. In the reverse, missense mutations in the N-terminal ABD or in the Cys-rich domain could be accompanied by the DMD severe phenotype [4, 5]. Therefore, it is clear that certain parts of the molecule are more indispensable than others and this led to the idea that a therapy strategy could be to transform the severe DMD phenotype into a mild BMD phenotype, expressing mutation in the less indispensable part of dystrophin (Figure 3).
FIGURE 3.
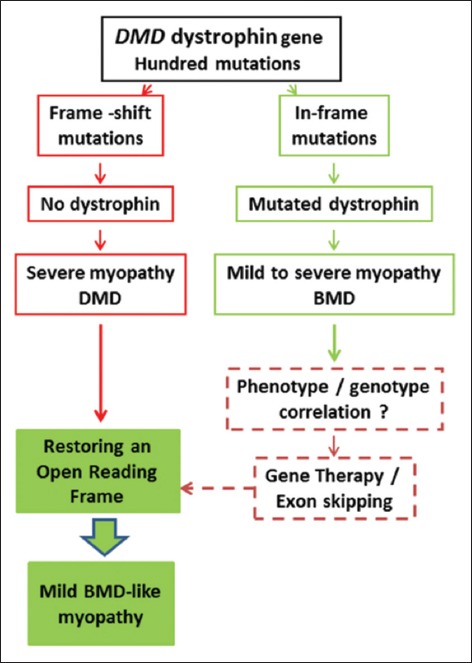
The Monaco rule and how it is used to generate therapy patterns.
DYSTROPHIN AND DMD THERAPY
Indeed, the injection of naked whole cDNA has been proven to be inefficient to produce significant dystrophin levels in diseased muscles and the cDNA has to be vectorised to specifically reach muscles. For this purposes, different serotypes of adeno-associated viruses (AAV) have been used. However, the whole DMD cDNA is too large to be inserted in the AAVs. Therefore, the concept of micro-dystrophin has emerged [52]. Truncated gene coding sequences (micro-dystrophins) inspired from the truncated dystrophin coding sequences observed in mild BMD patients [53](Figure 3) were designed [54-57]. One of these has been well used in animal models such as the mdx mouse and the grmd dog. This highly simplified micro-dystrophin only consists of the N- and Cys-rich domains with two hinges and four repeats (Figure 4)[58, 59]. However, this micro-dystrophin does not recapitulate all the functions of dystrophin [54] and further improvements are needed essentially by addition of other binding domains of dystrophin such as for example, the nNOS and microtubule binding sites (Figure 2) [56].
FIGURE 4.

Two examples of micro-dystrophins.
The exon skipping therapy aims at recover an in-frame mutation equivalent to a BMD mutation. In case of the frame-shifting deletion of exon, modifying the splicing of mRNA allows the exclusion of one or several additional exons and the restoration of a reading frame (Figure 5). To this end, small antisense oligonucleotides (AONs) sequences are designed to bind to exon splice junctions, masking them from the spliceosome. This modifies the splicing and skips the exon (s) focused on from the mRNA. Two types of AONs have been designed, 2’O-methyl phosphorothioate (2’O-Me) or phosphorodiamidate morpholino (PMO) oligomers.
FIGURE 5.
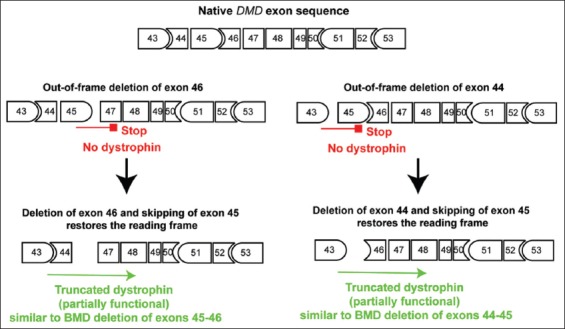
Exon skipping for restoration of the reading frame. Same legend as in Figure 1.
The proof of concept has been largely demonstrated [60-66] [67] and there are now human trials in progress using oligonucleotides injection using AAV [68-72](see the excellent reviews about therapy [56, 73-74]). For example, the deletions of exon 46 or 44 both shift the reading frame and result in no dystrophin production. The two deletions can be enlarged by skipping exon 45 resulting in the two in-frame deletions 45-46 and 44-45, respectively (Figure 5). Theoretically, the two enlarged deletions should lead to the production of a BMD-like truncated and partially functional dystrophin.
However, these schemes are more complex than at first glance since a lot of BMD patients have a more severe disease than others. This high variability of phenotypes has long been recognized but rather recently examining BMD patients in details has emerged to be relevant to anticipate for DMD therapy effects. In the two examples here in Figure 5, two BMD-like deletions may be produced using the same drug in different patients. However, the deletion 45-46 has been recently reported to be accompanied by a DMD phenotype [75] and to produce no dystrophin (personal communication). On contrast, there are no patients reported for the deletion of exons 44-45, signifying that the deletion may be asymptomatic. Therefore, the therapy of these two DMD deletions may not result in the same cure effect even though we anticipate that patients will all be transformed in BMD-like patients.
In that field, we recently studied the clinical status of BMD patients with deletions starting by exon 45 deletion e.g. deletions of exons 45-47, 45-48, 45-49 and 45-51 and the in vitro biochemical status of the proteins [76]. We showed that the structure of the new dystrophins as produced in these BMD patients could partly explain the differences in the clinical severity of the patients. The patients with deletions 45-47 and 45-49 were confined to wheelchair or were diagnosed with a cardiomyopathy about 10 years earlier than patients with deletions 45-48 and 45-51. The new junction at the deletion site of these two last deletions reconstitutes a spectrin-like structure while it is not the case of the two first deletions. Therefore, the choice for skipping one exon or the other for restoring the reading frame to a DMD deletion means that the genotype - phenotype correlation data in BMD patients is well established. In addition, this proves that examining the status of large cohorts of BMD patients together with the status of dystrophin is of high interest for the therapy design. For the clinicians, this also signifies that it is essential to diagnose all the BMD patients by genetics and to follow the time course of the disease by regularly evaluating respiratory and cardiac muscle status and walking ability of the BMD patients.
CONCLUSION
Finally, it appears that therapies in progress will not cure the DMD disease but slow down its progression. The purpose now is to focus therapy on the BMD-like dystrophin sequences with the less severe disease either for gene or exon skipping therapy. We have now to increase our knowledge about BMD disease genetics and time course and dystrophin structure consequences after BMD deletions. The effects of genetics modifiers have also to be studied in details such as non-synonymous polymorphism (SNPs) [4], noncoding RNAs [77, 78] or other genetic modifiers [79-83] as they all may modulate the expression of dystrophin or the severity of the disease. The diagnosis of BMD is highly relevant to anticipate and to understand data resulting from human clinical trials. It is also likely that certain severe BMD patients should benefit from therapy strategies or from compensatory strategies elaborated for DMD patients.
ACKNOWLEDGEMENTS
The author thanks all the colleagues and collaborators who participated in France and worldwide to her work about dystrophin structure and function and the AFM-Téléthon for its constant support.
REFERENCES
- [1].Koenig M, Beggs A, Moyer M, Scherpf S, Heindrich K, Bettecken T, et al. The molecular basis for Duchenne versus Becker muscular dystrophy: correlation of severity with type of deletion. Am J Hum Genet. 1989;45:498–506. [PMC free article] [PubMed] [Google Scholar]
- [2].Koenig M, Hoffman EP, Bertelson CJ, Monaco AP, Feener C, Kunkel LM. Complete cloning of the Duchenne muscular dystrophy (DMD) cDNA and preliminary genomic organization of the DMD gene in normal and affected individuals. Cell. 1987 Jul 31;50:509–17. doi: 10.1016/0092-8674(87)90504-6. http://dx.doi.org/10.1016/0092-8674(87)90504-6 . [DOI] [PubMed] [Google Scholar]
- [3].Kenwrick S, Patterson M, Speer A, Fischbeck K, Davies K. Molecular analysis of the Duchenne muscular dystrophy region using pulsed field gel electrophoresis. Cell. 1987 Jan 30;48:351–7. doi: 10.1016/0092-8674(87)90438-7. http://dx.doi.org/10.1016/0092-8674(87)90438-7 . [DOI] [PubMed] [Google Scholar]
- [4].Flanigan KM, Dunn DM, von Niederhausern A, Soltanzadeh P, Gappmaier E, Howard MT, et al. Mutational spectrum of DMD mutations in dystrophinopathy patients: application of modern diagnostic techniques to a large cohort. Hum Mutat. 2009 Dec;30:1657–66. doi: 10.1002/humu.21114. http://dx.doi.org/10.1002/humu.21114 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Tuffery-Giraud S, Beroud C, Leturcq F, Yaou RB, Hamroun D, Michel-Calemard L, et al. Genotype-phenotype analysis in 2,405 patients with a dystrophinopathy using the UMD-DMD database: a model of nationwide knowledgebase. Hum Mutat. 2009 Jun;30:934–45. doi: 10.1002/humu.20976. http://dx.doi.org/10.1002/humu.20976 . [DOI] [PubMed] [Google Scholar]
- [6].Monaco A, Bertelson C, Liechti-Gallati S, Moser H, Kunkel L. An explanation for the phenotypic differences between patients bearing partial deletions of the DMD locus. Genomics. 1988;2:90–5. doi: 10.1016/0888-7543(88)90113-9. http://dx.doi.org/10.1016/0888-7543(88)90113-9 . [DOI] [PubMed] [Google Scholar]
- [7].Wein N, Alfano L, Flanigan KM. Genetics and Emerging Treatments for Duchenne and Becker Muscular Dystrophy. Pediatr Clin N Am. 2015;62(3):723–42. doi: 10.1016/j.pcl.2015.03.008. http://dx.doi.org/10.1016/j.pcl.2015.03.008 . [DOI] [PubMed] [Google Scholar]
- [8].Kohler M, Clarenbach CF, Boni L, Brack T, Russi EW, Bloch KE. Quality of life, physical disability, and respiratory impairment in Duchenne muscular dystrophy. Am J Respir Crit Care Med. 2005 Oct 15;172:1032–6. doi: 10.1164/rccm.200503-322OC. http://dx.doi.org/10.1164/rccm.200503-322OC . [DOI] [PubMed] [Google Scholar]
- [9].Davies KE, Nowak KJ. Molecular mechanisms of muscular dystrophies: old and new players. Nat Rev Mol Cell Biol. 2006 Oct;7:762–73. doi: 10.1038/nrm2024. http://dx.doi.org/10.1038/nrm2024 . [DOI] [PubMed] [Google Scholar]
- [10].Rahimov F, Kunkel LM. The cell biology of disease: cellular and molecular mechanisms underlying muscular dystrophy. J Cell Biol. 2013 May 13;201:499–510. doi: 10.1083/jcb.201212142. http://dx.doi.org/10.1083/jcb.201212142 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Bushby KM, Gardner-Medwin D. The clinical, genetic and dystrophin characteristics of Becker muscular dystrophy I. Natural history. J Neurol. 1993 Feb;240:98–104. doi: 10.1007/BF00858725. http://dx.doi.org/10.1007/BF00858725 . [DOI] [PubMed] [Google Scholar]
- [12].Bushby KM, Gardner-Medwin D, Nicholson LV, Johnson MA, Haggerty ID, Cleghorn NJ, et al. The clinical, genetic and dystrophin characteristics of Becker muscular dystrophy II. Correlation of phenotype with genetic and protein abnormalities. J Neurol. 1993 Feb;240:105–12. doi: 10.1007/BF00858726. http://dx.doi.org/10.1007/BF00858726 . [DOI] [PubMed] [Google Scholar]
- [13].Petrof BJ, Shrager JB, Stedmann HH, Kelly AM, Sweeney HL. Dystrophin protects the sarcolemma from stresses developed during muscle contraction. Proceedings of the National Academy of Sciences, USA. 1993;90:3710–4. doi: 10.1073/pnas.90.8.3710. http://dx.doi.org/10.1073/pnas.90.8.3710 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Neri M, Torelli S, Brown S, Ugo I, Sabatelli P, Merlini L, et al. Dystrophin levels as low as 30% are sufficient to avoid muscular dystrophy in the human. Neuromuscul Disord. 2007 Dec;17:913–8. doi: 10.1016/j.nmd.2007.07.005. http://dx.doi.org/10.1016/j.nmd.2007.07.005 . [DOI] [PubMed] [Google Scholar]
- [15].Anthony K, Cirak S, Torelli S, Tasca G, Feng L, Arechavala-Gomeza V, et al. Dystrophin quantification and clinical correlations in Becker muscular dystrophy: implications for clinical trials. Brain. 2011 Dec;134:3544–56. doi: 10.1093/brain/awr291. http://dx.doi.org/10.1093/brain/awr291 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Aartsma-Rus A. Dystrophin analysis in clinical trials. Journal of Neuromuscular diseases. 2014;1:41–53. [PubMed] [Google Scholar]
- [17].Dubowitz V, Cohn RD. Dystrophin and Duchenne dystrophy. Neuromuscul Disord. 2015 May;25:361–2. doi: 10.1016/j.nmd.2015.03.013. http://dx.doi.org/10.1016/j.nmd.2015.03.013 . [DOI] [PubMed] [Google Scholar]
- [18].Ervasti J, Campbell K. Dystrophin and the membrane skeleton. Curr Op Cell Biol. 1993;5:82–7. doi: 10.1016/s0955-0674(05)80012-2. http://dx.doi.org/10.1016/S0955-0674(05)80012-2 . [DOI] [PubMed] [Google Scholar]
- [19].Le Rumeur E, Winder SJ, Hubert JF. Dystrophin: More than just the sum of its parts. Biochim Biophys Acta. 2010 Sep;1804:1713–22. doi: 10.1016/j.bbapap.2010.05.001. [DOI] [PubMed] [Google Scholar]
- [20].Levine BA, Moir AJG, Patchell VB, Perry SV. Binding sites involved in the interaction of actin with the N-terminal region of dystrophin. FEBS Letters. 1992;298:44–8. doi: 10.1016/0014-5793(92)80019-d. http://dx.doi.org/10.1016/0014-5793(92)80019-D . [DOI] [PubMed] [Google Scholar]
- [21].Keep NH, Norwood FLM, Moores CA, Winder SJ, Kendrick-Jones J. The 2.0 A Structure of the Second Calponin Homology Domain from the Actin-binding Region of the Dystrophin Homologue Utrophin. J Mol Biol. 1999;285:1257–64. doi: 10.1006/jmbi.1998.2406. http://dx.doi.org/10.1006/jmbi.1998.2406 . [DOI] [PubMed] [Google Scholar]
- [22].Norwood F, Sutherland-Smith A, Keep N, Kendrick-Jones J. The structure of the N-terminal actin-binding domain of human dystrophin and how mutations in this domain may cause Duchenne or Becker muscular dystrophy. Structure. 2000;8:481–91. doi: 10.1016/s0969-2126(00)00132-5. http://dx.doi.org/10.1016/S0969-2126(00)00132-5 . [DOI] [PubMed] [Google Scholar]
- [23].Koenig M, Kunkel LM. Detailed analysis of the repeat domain of dystrophin reveals four potential hinge segments that may confer flexibility. J Biol Chem. 1990;265:4560–6. [PubMed] [Google Scholar]
- [24].Amann KJ, Renley BA, Ervasti JM. A Cluster of Basic Repeats in the Dystrophin Rod Domain Binds F-actin through an Electrostatic Interaction. J Biol Chem. 1998;273:28419–23. doi: 10.1074/jbc.273.43.28419. http://dx.doi.org/10.1074/jbc.273.43.28419 . [DOI] [PubMed] [Google Scholar]
- [25].Bhosle RC, Michele DE, Campbell KP, Li Z, Robson RM. Interactions of intermediate filament protein synemin with dystrophin and utrophin. Biochem Biophys Res Commun. 2006 Aug 4;346:768–77. doi: 10.1016/j.bbrc.2006.05.192. http://dx.doi.org/10.1016/j.bbrc.2006.05.192 . [DOI] [PubMed] [Google Scholar]
- [26].Stone MR, O’Neill A, Catino D, Bloch RJ. Specific interaction of the actin-binding domain of dystrophin with intermediate filaments containing keratin 19. Mol Biol Cell. 2005 Sep;16:4280–93. doi: 10.1091/mbc.E05-02-0112. http://dx.doi.org/10.1091/mbc.E05-02-0112 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Prins KW, Humston JL, Mehta A, Tate V, Ralston E, Ervasti JM. Dystrophin is a microtubule-associated protein. J Cell Biol. 2009 Aug 10;186:363–9. doi: 10.1083/jcb.200905048. http://dx.doi.org/10.1083/jcb.200905048 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Belanto JJ, Mader TL, Eckhoff MD, Strandjord DM, Banks GB, Gardner MK, et al. Microtubule binding distinguishes dystrophin from utrophin. Proc Natl Acad Sci U S A. 2014 Apr 15;111:5723–8. doi: 10.1073/pnas.1323842111. http://dx.doi.org/10.1073/pnas.1323842111 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Lai Y, Thomas GD, Yue Y, Yang HT, Li D, Long C, et al. Dystrophins carrying spectrin-like repeats 16 and 17 anchor nNOS to the sarcolemma and enhance exercise performance in a mouse model of muscular dystrophy. J Clin Invest. 2009 Mar;119:624–35. doi: 10.1172/JCI36612. http://dx.doi.org/10.1172/JCI36612 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Lai Y, Zhao J, Yue Y, Duan D. alpha2 and alpha3 helices of dystrophin R16 and R17 frame a microdomain in the alpha1 helix of dystrophin R17 for neuronal NOS binding. Proc Natl Acad Sci U S A. 2013 Nov 26;110:525–30. doi: 10.1073/pnas.1211431109. http://dx.doi.org/10.1073/pnas.1211431109 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Giudice E, Molza A-E, Laurin Y, Nicolas A, Le Rumeur E, Delalande O. Molecular clues to the dystrophin–nNOS interaction: a theoretical approach. Biochemistry. 2013;52:7777–84. doi: 10.1021/bi400794p. http://dx.doi.org/10.1021/bi400794p . [DOI] [PubMed] [Google Scholar]
- [32].Yamashita K, Suzuki A, Satoh Y, Ide M, Amano Y, Masuda-Hirata M, et al. The 8th and 9th tandem spectrin-like repeats of utrophin cooperatively form a functional unit to interact with polarity-regulating kinase PAR-1b. Biochem Biophys Res Commun. 2010 Nov;26(391):812–7. doi: 10.1016/j.bbrc.2009.11.144. http://dx.doi.org/10.1016/j.bbrc.2009.11.144 . [DOI] [PubMed] [Google Scholar]
- [33].Le Rumeur E, Fichou Y, Pottier S, Gaboriau F, Rondeau-Mouro C, Vincent M, et al. Interaction of dystrophin rod domain with membrane phospholipids: evidence of a close proximity between tryptophan residues and lipids. J Biol Chem. 2003;278:5993–6001. doi: 10.1074/jbc.M207321200. http://dx.doi.org/10.1074/jbc.M207321200 . [DOI] [PubMed] [Google Scholar]
- [34].Legardinier S, Hubert J-F, Le Bihan O, Tascon C, Rocher C, Raguénès-Nicol C, et al. Sub-domains of the dystrophin rod domain display contrasting lipid-binding and stability properties. Biochim Biophys Acta. 2008;1784:672–82. doi: 10.1016/j.bbapap.2007.12.014. http://dx.doi.org/10.1016/j.bbapap.2007.12.014 . [DOI] [PubMed] [Google Scholar]
- [35].Legardinier S, Raguénès-Nicol C, Tascon C, Rocher C, Hardy S, Hubert JF, et al. Mapping of the lipid-binding and stability properties of the central rod domain of human dystrophin. J Mol Biol. 2009;389:546–58. doi: 10.1016/j.jmb.2009.04.025. http://dx.doi.org/10.1016/j.jmb.2009.04.025 . [DOI] [PubMed] [Google Scholar]
- [36].Campbell K, Kahl S. Association of dystrophin and an integral membrane glycoprotein. Nature. 1989;338:259–62. doi: 10.1038/338259a0. http://dx.doi.org/10.1038/338259a0 . [DOI] [PubMed] [Google Scholar]
- [37].Ervasti J, Campbell K. A Role for the Dystrophin-Glycoprotein Complex as aTransmembrane Linker between Laminin and Actin. J Cell Biol. 1993;122:809–23. doi: 10.1083/jcb.122.4.809. http://dx.doi.org/10.1083/jcb.122.4.809 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Huang X, Poy F, Zhang R, Joachimiak A, Sudol M, Eck MJ. Structure of a WW domain containing fragment of dystrophin in complex with beta-dystroglycan. Nat Struct Biol. 2000 Aug;7:634–8. doi: 10.1038/77923. http://dx.doi.org/10.1038/77923 . [DOI] [PubMed] [Google Scholar]
- [39].Hnia K, Zouiten D, Cantel S, Chazalette D, Hugon G, Fehrentz JA, et al. ZZ domain of dystrophin and utrophin: topology and mapping of a beta-dystroglycan interaction site. Biochem J. 2007 Feb 1;401:667–77. doi: 10.1042/BJ20061051. http://dx.doi.org/10.1042/BJ20061051 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Rezniczek GA, Konieczny P, Nikolic B, Reipert S, Schneller D, Abrahamsberg C, et al. Plectin 1f scaffolding at the sarcolemma of dystrophic (mdx) muscle fibers through multiple interactions with beta-dystroglycan. J Cell Biol. 2007 Mar 26;176:965–77. doi: 10.1083/jcb.200604179. http://dx.doi.org/10.1083/jcb.200604179 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Ayalon G, Davis JQ, Scotland PB, Bennett V. An ankyrin-based mechanism for functional organization of dystrophin and dystroglycan. Cell. 2008 Dec 26;135:1189–200. doi: 10.1016/j.cell.2008.10.018. http://dx.doi.org/10.1016/j.cell.2008.10.018 . [DOI] [PubMed] [Google Scholar]
- [42].Sadoulet-Puccio H, Rajala M, Kunkel L. Dystrobrevin and dystrophin: An interaction through coiled-coil motifs. Proc Natl Acad Sci USA. 1997;94:12413–8. doi: 10.1073/pnas.94.23.12413. http://dx.doi.org/10.1073/pnas.94.23.12413 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Newey SE, Benson MA, Ponting CP, Davies KE, Blake DJ. Alternative splicing of dystrobrevin regulates the stoichiometry of syntrophin binding to the dystrophin protein complex. Curr Biol. 2000 Oct 19;10:1295–8. doi: 10.1016/s0960-9822(00)00760-0. http://dx.doi.org/10.1016/S0960-9822(00)00760-0 . [DOI] [PubMed] [Google Scholar]
- [44].Zubrzycka-Gaarn EE, Bulman DE, Karpati G, Burghes AH, Belfall B, Klamut HJ, et al. The Duchenne muscular dystrophy gene product is localized in sarcolemma of human skeletal muscle. Nature. 1988 Jun 2;333:466–9. doi: 10.1038/333466a0. http://dx.doi.org/10.1038/333466a0 . [DOI] [PubMed] [Google Scholar]
- [45].Jaka O, Casas-Fraile L, Lopez de Munain A, Saenz A. Costamere proteins and their involvement in myopathic processes. Expert Rev Mol Med. 2015;17:e12. doi: 10.1017/erm.2015.9. http://dx.doi.org/10.1017/erm.2015.9 . [DOI] [PubMed] [Google Scholar]
- [46].Ervasti JM. Costameres: the Achilles’ heel of Herculean muscle. J Biol Chem. 2003 Apr 18;278:13591–4. doi: 10.1074/jbc.R200021200. http://dx.doi.org/10.1074/jbc.R200021200 . [DOI] [PubMed] [Google Scholar]
- [47].Bloch RJ, Capetanaki Y, O’Neill A, Reed P, Williams MW, Resneck WG, et al. Costameres: repeating structures at the sarcolemma of skeletal muscle. Clin Orthop Relat Res. 2002. Oct, pp. S203–10. http://dx.doi.org/10.1097/00003086-200210001-00024 . [DOI] [PubMed]
- [48].Bloch RJ, Gonzalez-Serratos H. Lateral force transmission across costameres in skeletal muscle. Exerc Sport Sci Rev. 2003 Apr;31:73–8. doi: 10.1097/00003677-200304000-00004. http://dx.doi.org/10.1097/00003677-200304000-00004 . [DOI] [PubMed] [Google Scholar]
- [49].Kumar A, Khandelwal N, Malya R, Reid MB, Boriek AM. Loss of dystrophin causes aberrant mechanotransduction in skeletal muscle fibers. Faseb J. 2004 Jan;18:102–13. doi: 10.1096/fj.03-0453com. http://dx.doi.org/10.1096/fj.03-0453com . [DOI] [PubMed] [Google Scholar]
- [50].Bloch RJ, Reed P, O’Neill A, Strong J, Williams M, Porter N, et al. Costameres mediate force transduction in healthy skeletal muscle and are altered in muscular dystrophies. J Muscle Res Cell Motil. 2004;25:590–2. [PubMed] [Google Scholar]
- [51].Bloch RJ, Reed P, O’Neill A, Strong J, Williams M, Porter N, et al. Costameres mediate force transduction in healthy skeletal muscle and are altered in muscular dystrophies. J Muscle Res Cell Motil. 2004;25:590–2. [PubMed] [Google Scholar]
- [52].Mariol MC, Segalat L. Muscular degeneration in the absence of dystrophin is a calcium-dependent process. Curr Biol. 2001 Oct 30;11:1691–4. doi: 10.1016/s0960-9822(01)00528-0. http://dx.doi.org/10.1016/S0960-9822(01)00528-0 . [DOI] [PubMed] [Google Scholar]
- [53].Harper SQ, Hauser MA, DelloRusso C, Duan D, Crawford RW, Phelps SF, et al. Modular flexibility of dystrophin: implications for gene therapy of Duchenne muscular dystrophy. Nature Med. 2002;8:253–61. doi: 10.1038/nm0302-253. http://dx.doi.org/10.1038/nm0302-253 . [DOI] [PubMed] [Google Scholar]
- [54].England S, Nicholson L, Johnson M, Forrest S, Love D, Zubrzycka-Gaarn E, et al. Very mild muscular dystrophy associated with the deletion of 46% of the dystrophin. Nature. 1990;343:180–2. doi: 10.1038/343180a0. http://dx.doi.org/10.1038/343180a0 . [DOI] [PubMed] [Google Scholar]
- [55].Seto JT, Ramos JN, Muir L, Chamberlain JS, Odom GL. Gene replacement therapies for duchenne muscular dystrophy using adeno-associated viral vectors. Curr Gene Ther. 2012 Jun;12:139–51. doi: 10.2174/156652312800840603. http://dx.doi.org/10.2174/156652312800840603 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].Fairclough RJ, Wood MJ, Davies KE. Therapy for Duchenne muscular dystrophy: renewed optimism from genetic approaches. Nat Rev Genet. 2013 Jun;14:373–8. doi: 10.1038/nrg3460. http://dx.doi.org/10.1038/nrg3460 . [DOI] [PubMed] [Google Scholar]
- [57].Jarmin S, Kymalainen H, Popplewell L, Dickson G. New developments in the use of gene therapy to treat Duchenne muscular dystrophy. Expert Opin Biol Ther. 2014 Feb;14:209–30. doi: 10.1517/14712598.2014.866087. http://dx.doi.org/10.1517/14712598.2014.866087 . [DOI] [PubMed] [Google Scholar]
- [58].McGreevy JW, Hakim CH, McIntosh MA, Duan D. Animal models of Duchenne muscular dystrophy: from basic mechanisms to gene therapy. Dis Model Mech. 2015 Mar;8:195–213. doi: 10.1242/dmm.018424. http://dx.doi.org/10.1242/dmm.018424 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Gregorevic P, Blankinship MJ, Allen JM, Chamberlain JS. Systemic microdystrophin gene delivery improves skeletal muscle structure and function in old dystrophic mdx mice. Mol Ther. 2008 Apr;16:657–64. doi: 10.1038/mt.2008.28. http://dx.doi.org/10.1038/mt.2008.28 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Foster H, Sharp PS, Athanasopoulos T, Trollet C, Graham IR, Foster K, et al. Codon and mRNA sequence optimization of microdystrophin transgenes improves expression and physiological outcome in dystrophic mdx mice following AAV2/8 gene transfer. Mol Ther. 2008 Nov;16:1825–32. doi: 10.1038/mt.2008.186. http://dx.doi.org/10.1038/mt.2008.186 . [DOI] [PubMed] [Google Scholar]
- [61].Goyenvalle A, Vulin A, Fougerousse F, Leturcq F, Kaplan J, Garcia L, et al. Rescue of dystrophic muscle through U7 snRNA-mediated exon skipping. Science. 2004. p. 306. http://dx.doi.org/10.1126/science.1104297 . [DOI] [PubMed]
- [62].Aartsma-Rus A, Janson AA, Heemskerk JA, De Winter CL, Van Ommen GJ, Van Deutekom JC. Therapeutic modulation of DMD splicing by blocking exonic splicing enhancer sites with antisense oligonucleotides. Ann N Y Acad Sci. 2006 Oct;1082:74–6. doi: 10.1196/annals.1348.058. http://dx.doi.org/10.1196/annals.1348.058 . [DOI] [PubMed] [Google Scholar]
- [63].Aartsma-Rus A, Janson AA, Kaman WE, Bremmer-Bout M, van Ommen GJ, den Dunnen JT, et al. Antisense-induced multiexon skipping for Duchenne muscular dystrophy makes more sense. Am J Hum Genet. 2004 Jan;74:83–92. doi: 10.1086/381039. http://dx.doi.org/10.1086/381039 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [64].Takeshima Y, Yagi M, Wada H, Ishibashi K, Nishiyama A, Kakumoto M, et al. Intravenous infusion of an antisense oligonucleotide results in exon skipping in muscle dystrophin mRNA of Duchenne muscular dystrophy. Pediatr Res. 2006 May;59:690–4. doi: 10.1203/01.pdr.0000215047.51278.7c. http://dx.doi.org/10.1203/01.pdr.0000215047.51278.7c . [DOI] [PubMed] [Google Scholar]
- [65].McClorey G, Moulton HM, Iversen PL, Fletcher S, Wilton SD. Antisense oligonucleotide-induced exon skipping restores dystrophin expression in vitro in a canine model of DMD. Gene Ther. 2006 Oct;13:1373–81. doi: 10.1038/sj.gt.3302800. http://dx.doi.org/10.1038/sj.gt.3302800 . [DOI] [PubMed] [Google Scholar]
- [66].Vulin A, Barthelemy I, Goyenvalle A, Thibaud JL, Beley C, Griffith G, et al. Muscle function recovery in golden retriever muscular dystrophy after AAV1-U7 exon skipping. Mol Ther. 2012 Nov;20:2120–33. doi: 10.1038/mt.2012.181. http://dx.doi.org/10.1038/mt.2012.181 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Aartsma-Rus A, Muntoni F. 194th ENMC international workshop 3rd ENMC workshop on exon skipping: towards clinical application of antisense-mediated exon skipping for Duchenne muscular dystrophy 8-10 December 2012, Naarden, The Netherlands. Neuromuscul Disord. 2013 Nov;23:934–44. doi: 10.1016/j.nmd.2013.06.369. http://dx.doi.org/10.1016/j.nmd.2013.06.369 . [DOI] [PubMed] [Google Scholar]
- [68].Le Guiner C, Montus M, Servais L, Cherel Y, Francois V, Thibaud JL, et al. Forelimb treatment in a large cohort of dystrophic dogs supports delivery of a recombinant AAV for exon skipping in Duchenne patients. Mol Ther. 2014 Nov;22:1923–35. doi: 10.1038/mt.2014.151. http://dx.doi.org/10.1038/mt.2014.151 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].van Deutekom JC, Janson AA, Ginjaar IB, Frankhuizen WS, Aartsma-Rus A, Bremmer-Bout M, et al. Local dystrophin restoration with antisense oligonucleotide PRO051. N Engl J Med. 2007 Dec 27;357:2677–86. doi: 10.1056/NEJMoa073108. http://dx.doi.org/10.1056/NEJMoa073108 . [DOI] [PubMed] [Google Scholar]
- [70].Kinali M, Arechavala-Gomeza V, Feng L, Cirak S, Hunt D, Adkin C, et al. Local restoration of dystrophin expression with the morpholino oligomer AVI-4658 in Duchenne muscular dystrophy: a single-blind, placebo-controlled, dose-escalation, proof-of-concept study. Lancet Neurol. 2009 Oct;8:918–28. doi: 10.1016/S1474-4422(09)70211-X. http://dx.doi.org/10.1016/S1474-4422(09)70211-X . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [71].Goemans NM, Tulinius M, van den Akker JT, Burm BE, Ekhart PF, Heuvelmans N, et al. Systemic administration of PRO051 in Duchenne’s muscular dystrophy. N Engl J Med. 2011 Apr 21;364:1513–22. doi: 10.1056/NEJMoa1011367. http://dx.doi.org/10.1056/NEJMoa1011367 . [DOI] [PubMed] [Google Scholar]
- [72].Cirak S, Arechavala-Gomeza V, Guglieri M, Feng L, Torelli S, Anthony K, et al. Exon skipping and dystrophin restoration in patients with Duchenne muscular dystrophy after systemic phosphorodiamidate morpholino oligomer treatment: an open-label, phase 2, dose-escalation study. Lancet. 2011 Aug 13;378:595–605. doi: 10.1016/S0140-6736(11)60756-3. http://dx.doi.org/10.1016/S0140-6736(11)60756-3 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Cirak S, Feng L, Anthony K, Arechavala-Gomeza V, Torelli S, Sewry C, et al. Restoration of the Dystrophin-associated Glycoprotein Complex After Exon Skipping Therapy in Duchenne Muscular Dystrophy. Mol Ther. 2011 Nov;:15. doi: 10.1038/mt.2011.248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [74].Guiraud S, Aartsma-Rus A, Vieira NM, Davies KE, van Ommen GJ, Kunkel LM. The Pathogenesis and Therapy of Muscular Dystrophies. Annu Rev Genomics Hum Genet. 2015. Jun, p. 4. http://dx.doi.org/10.1146/annurev-genom-090314-025003 . [DOI] [PubMed]
- [75].Wilton SD, Veedu RN, Fletcher S. The emperor’ s new dystrophin: finding sense in the noise. Trends Mol Med. 2015. May, p. 23. http://dx.doi.org/10.1016/j.molmed.2015.04.006 . [DOI] [PubMed]
- [76].Findlay AR, Wein N, Kaminoh Y, Taylor LE, Dunn DM, Mendell JR, et al. Clinical phenotypes as predictors of the outcome of skipping around DMD exon 45. Ann Neurol. 2015 Jan 21;77:668–74. doi: 10.1002/ana.24365. http://dx.doi.org/10.1002/ana.24365 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [77].Nicolas A, Raguenes-Nicol C, Ben Yaou R, Ameziane-Le Hir S, Cheron A, Vie V, et al. Becker muscular dystrophy severity is linked to the structure of dystrophin. Hum Mol Genet. 2015 Oct 27;24:1267–79. doi: 10.1093/hmg/ddu537. http://dx.doi.org/10.1093/hmg/ddu537 . [DOI] [PubMed] [Google Scholar]
- [78].Cacchiarelli D, Martone J, Girardi E, Cesana M, Incitti T, Morlando M, et al. MicroRNAs involved in molecular circuitries relevant for the Duchenne muscular dystrophy pathogenesis are controlled by the dystrophin/nNOS pathway. Cell Metab. 2010 Oct 6;12:341–51. doi: 10.1016/j.cmet.2010.07.008. http://dx.doi.org/10.1016/j.cmet.2010.07.008 . [DOI] [PubMed] [Google Scholar]
- [79].Cacchiarelli D, Incitti T, Martone J, Cesana M, Cazzella V, Santini T, et al. miR-31 modulates dystrophin expression: new implications for Duchenne muscular dystrophy therapy. EMBO Rep. 2011 Feb;12:136–41. doi: 10.1038/embor.2010.208. http://dx.doi.org/10.1038/embor.2010.208 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [80].Kerst B, Mennerich D, Schuelke M, Stoltenburg-Didinger G, von Moers A, Gossrau R, et al. Heterozygous myogenic factor 6 mutation associated with myopathy and severe course of Becker muscular dystrophy. Neuromuscul Disord. 2000;10:572–7. doi: 10.1016/s0960-8966(00)00150-4. http://dx.doi.org/10.1016/S0960-8966(00)00150-4 . [DOI] [PubMed] [Google Scholar]
- [81].Davis DB, Delmonte AJ, Ly CT, McNally EM. Myoferlin, a candidate gene and potential modifier of muscular dystrophy. Hum Mol Genet. 2000 Jan 22;9:217–26. doi: 10.1093/hmg/9.2.217. http://dx.doi.org/10.1093/hmg/9.2.217 . [DOI] [PubMed] [Google Scholar]
- [82].Pegoraro E, Hoffman EP, Piva L, Gavassini BF, Cagnin S, Ermani M, et al. SPP1 genotype is a determinant of disease severity in Duchenne muscular dystrophy. Neurology. 2011 Jan 18;76:219–26. doi: 10.1212/WNL.0b013e318207afeb. http://dx.doi.org/10.1212/WNL.0b013e318207afeb . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [83].Bello L, Piva L, Barp A, Taglia A, Picillo E, Vasco G, et al. Importance of SPP1 genotype as a covariate in clinical trials in Duchenne muscular dystrophy. Neurology. 2012 Jul 10;79:159–62. doi: 10.1212/WNL.0b013e31825f04ea. http://dx.doi.org/10.1212/WNL.0b013e31825f04ea . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [84].Flanigan KM, Ceco E, Lamar KM, Kaminoh Y, Dunn DM, Mendell JR, et al. LTBP4 genotype predicts age of ambulatory loss in Duchenne muscular dystrophy. Ann Neurol. 2013 Apr;73:481–8. doi: 10.1002/ana.23819. http://dx.doi.org/10.1002/ana.23819 . [DOI] [PMC free article] [PubMed] [Google Scholar]