

Abstract
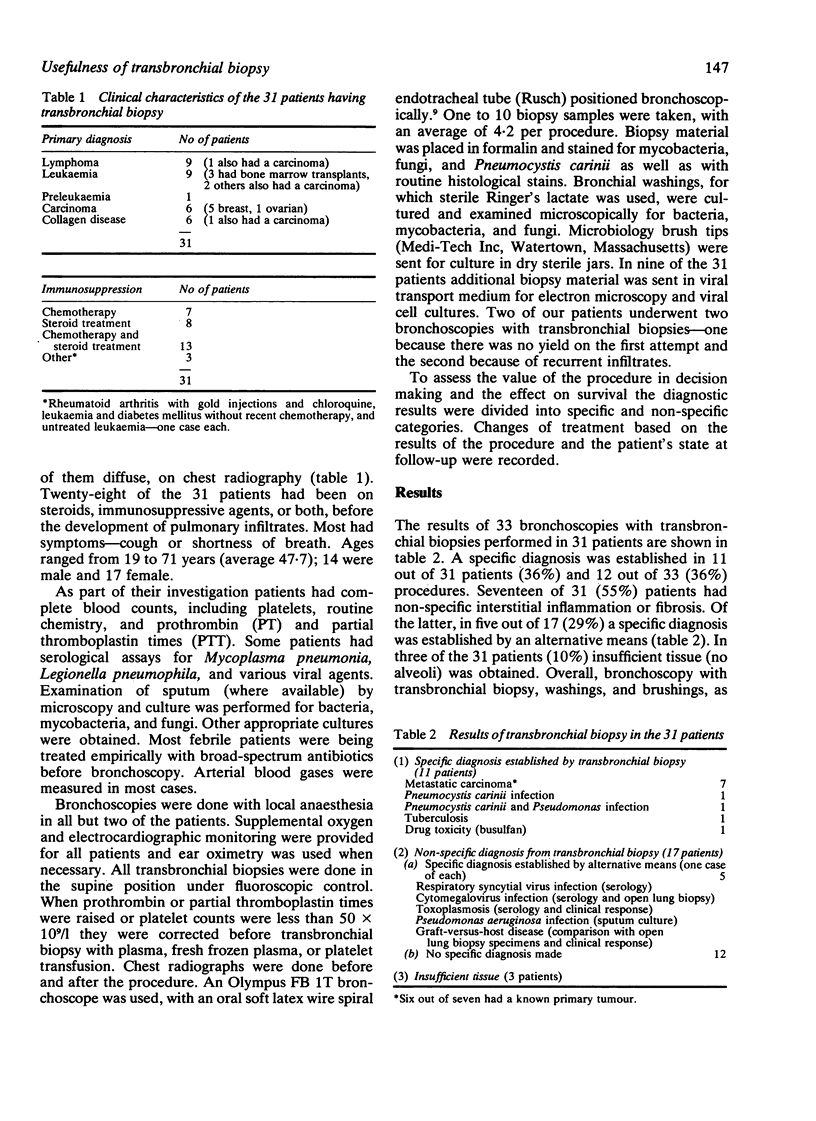
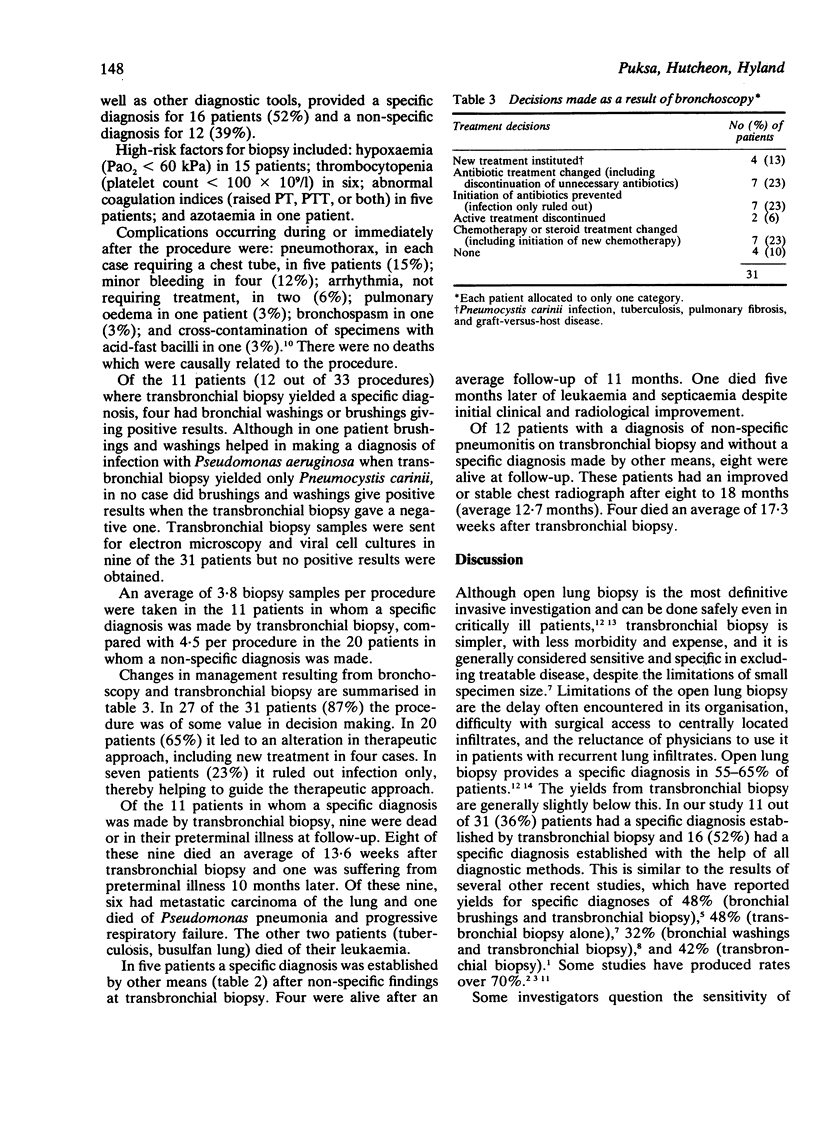
In a retrospective study of thirty-one immunosuppressed patients with new pulmonary infiltrates transbronchial biopsy provided a specific diagnosis in 11 of the 31 (36%) patients. In a further five patients, whose biopsy showed non-specific interstitial pneumonitis, a specific diagnosis was established by other means. Overall a specific diagnosis was obtained in 52% of patients. Twelve patients were left with a diagnosis of non-specific interstitial pneumonitis. In three out of 31 (10%) patients insufficient tissue was obtained. The seven patients who had metastatic carcinoma of the lung did poorly. The nine with other specific diagnoses did better in that five of them were alive after more than 11 months of follow-up. Patients with non-specific pneumonitis did well; eight out of 12 (67%) were alive after an average follow-up of 13.4 months. In 27 of the 31 (87%) patients the procedure was felt to have influenced therapeutic decisions. This was true whether the biopsy yielded a specific or a non-specific diagnosis. In our series making a specific diagnosis did not improve the patients' survival. Those with non-specific pneumonitis who were treated empirically did well, as did patients with specific diagnoses other than metastatic carcinoma of the lung.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bartlett J. G., Alexander J., Mayhew J., Sullivan-Sigler N., Gorbach S. L. Should fiberoptic bronchoscopy aspirates be cultured? Am Rev Respir Dis. 1976 Jul;114(1):73–78. doi: 10.1164/arrd.1976.114.1.73. [DOI] [PubMed] [Google Scholar]
- Chopra S. K., Mohsenifar Z. Fiberoptic bronchoscopy in diagnosis of opportunistic lung infections: assessment of Sputa, Washings, Brushings and biopsy specimens. West J Med. 1979 Jul;131(1):4–7. [PMC free article] [PubMed] [Google Scholar]
- Cunningham J. H., Zavala D. C., Corry R. J., Keim L. W. Trephine air drill, bronchial brush, and fiberoptic transbronchial lung biopsies in immunosuppressed patients. Am Rev Respir Dis. 1977 Feb;115(2):213–220. doi: 10.1164/arrd.1977.115.2.213. [DOI] [PubMed] [Google Scholar]
- Feldman N. T., Penningtonp J. E., Ehrie M. G. Transbronchial lung biopsy in the compromised host. JAMA. 1977 Sep 26;238(13):1377–1379. [PubMed] [Google Scholar]
- Greenman R. L., Goodall P. T., King D. Lung biopsy in immunocompromised hosts. Am J Med. 1975 Oct;59(4):488–496. doi: 10.1016/0002-9343(75)90256-9. [DOI] [PubMed] [Google Scholar]
- Kvale P. A., Bode F. R., Kini S. Diagnostic accuracy in lung cancer; comparison of techniques used in association with flexible fiberoptic bronchoscopy. Chest. 1976 Jun;69(6):752–757. doi: 10.1378/chest.69.6.752. [DOI] [PubMed] [Google Scholar]
- Lauver G. L., Hasan F. M., Morgan R. B., Campbell S. C. The usefulness of fiberoptic bronchoscopy in evaluating new pulmonary lesions in the compromised host. Am J Med. 1979 Apr;66(4):580–585. doi: 10.1016/0002-9343(79)91167-7. [DOI] [PubMed] [Google Scholar]
- Leers W. D. Disinfecting endoscopes: how not to transmit Mycobacterium tuberculosis by bronchoscopy. Can Med Assoc J. 1980 Aug 23;123(4):275-80, 283. [PMC free article] [PubMed] [Google Scholar]
- Leight G. S., Jr, Michaelis L. L. Open lung biopsy for the diagnosis of acute, diffuse pulmonary infiltrates in the immunosuppressed patient. Chest. 1978 Apr;73(4):477–482. doi: 10.1378/chest.73.4.477. [DOI] [PubMed] [Google Scholar]
- Matthay R. A., Farmer W. C., Odero D. Diagnostic fibreoptic bronchoscopy in the immunocompromised host with pulmonary infiltrates. Thorax. 1977 Oct;32(5):539–545. doi: 10.1136/thx.32.5.539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nishio J. N., Lynch J. P., 3rd Fiberoptic bronchoscopy in the immunocompromised host: the significance of a "nonspecific" transbronchial biopsy. Am Rev Respir Dis. 1980 Feb;121(2):307–312. doi: 10.1164/arrd.1980.121.2.307. [DOI] [PubMed] [Google Scholar]
- Pennington J. E., Feldman N. T. Pulmonary infiltrates and fever in patients with hematologic malignancy: assessment of transbronchial biopsy. Am J Med. 1977 Apr;62(4):581–587. doi: 10.1016/0002-9343(77)90421-1. [DOI] [PubMed] [Google Scholar]
- Phillips M. J., Knight R. K., Green M. Fibreoptic bronchoscopy and diagnosis of pulmonary lesions in lymphoma and leukaemia. Thorax. 1980 Jan;35(1):19–25. doi: 10.1136/thx.35.1.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poe R. H., Utell M. J., Israel R. H., Hall W. J., Eshleman J. D. Sensitivity and specificity of the nonspecific transbronchial lung biopsy. Am Rev Respir Dis. 1979 Jan;119(1):25–31. doi: 10.1164/arrd.1979.119.1.25. [DOI] [PubMed] [Google Scholar]
- Rossiter S. J., Miller C., Churg A. M., Carrington C. B., Mark J. B. Open lung biopsy in the immunosuppressed patient. Is it really beneficial? J Thorac Cardiovasc Surg. 1979 Mar;77(3):338–345. [PubMed] [Google Scholar]
- Sanderson D. R., McDougall J. C. Transoral bronchofiberoscopy. Chest. 1978 May;73(5 Suppl):701–703. doi: 10.1378/chest.73.5_supplement.701. [DOI] [PubMed] [Google Scholar]
- Singer C., Armstrong D., Rosen P. P., Walzer P. D., Yu B. Diffuse pulmonary infiltrates in immunosuppressed patients. Prospective study of 80 cases. Am J Med. 1979 Jan;66(1):110–120. doi: 10.1016/0002-9343(79)90490-x. [DOI] [PubMed] [Google Scholar]
- Solomon D. A., Solliday N. H., Gracey D. R. Cytology in fiberoptic bronchoscopy. Comparison of bronchial brushing, washing and post-bronchoscopy sputum. Chest. 1974 Jun;65(6):616–619. doi: 10.1378/chest.65.6.616. [DOI] [PubMed] [Google Scholar]