

Abstract
Background and Purpose
The aim of this study was to determine the usefulness of three-dimensional (3D) scalp EEG source imaging (ESI) in partial epilepsy in comparison with the results of presurgical evaluation, magnetoencephalography (MEG), and electrocorticography (ECoG).
Methods
The epilepsy syndrome of 27 partial epilepsy patients was determined by presurgical evaluations. EEG recordings were made using 70 scalp electrodes, and the 3D coordinates of the electrodes were digitized. ESI images of individual and averaged spikes were analyzed by Curry software with a boundary element method. MEG and ECoG were performed in 23 and 9 patients, respectively.
Results
ESI and MEG source imaging (MSI) results were well concordant with the results of presurgical evaluations (in 96.3% and 100% cases for ESI and MSI, respectively) at the lobar level. However, there were no spikes in the MEG recordings of three patients. The ESI results were well concordant with MSI results in 90.0% of cases. Compared to ECoG, the ESI results tended to be localized deeper than the cortex, whereas the MSI results were generally localized on the cortical surface. ESI was well concordant with ECoG in 8 of 9 (88.9%) cases, and MSI was also well concordant with ECoG in 4 of 5 (80.0%) cases. The EEG single dipoles in one patient with mesial temporal lobe epilepsy were tightly clustered with the averaged dipole when a 3 Hz high-pass filter was used.
Conclusions
The ESI results were well concordant with the results of the presurgical evaluation, MSI, and ECoG. The ESI analysis was found to be useful for localizing the seizure focus and is recommended for the presurgical evaluation of intractable epilepsy patients.
Keywords: partial epilepsy, EEG source imaging, MEG source imaging, source localization, presurgical evaluation, epilepsy surgery
INTRODUCTION
Many modalities can be used to localize an epileptic focus, including neuroimaging techniques such as magnetic resonance imaging (MRI), positron emission tomography (PET), single photon emission computed tomography (SPECT), and subtraction ictal SPECT coregistered to MRI (SISCOM), and electrophysiological signal recording techniques such as scalp electroencephalography (EEG), electrocorticography (ECoG), and magnetoencephalography (MEG). These techniques have been used in the presurgical evaluation of refractory epilepsy patients, and EEG remains crucial in the identification of epileptogenic regions.1,2
Electroencephalography source imaging (ESI), which is a technique involving the coregistration of EEG and MRI and analysis of the EEG source in three dimensions with the assistance of computer techniques, has been used for the last decade to localize epileptogenic zones noninvasively.3,4,5,6,7,8,9,10 Two methods are widely used for EEG source localization: dipole source localization and a distributed source model. Several studies have researched distributed source models because they reflect the electrophysiological reality of the EEG generators.11,12 Meanwhile, many researchers have demonstrated that dipole source models can be successfully employed to detect the epileptogenic foci of interictal epileptiform discharges.13,14,15 The multiple signal classification (MUSIC) method is a useful tool for source localization that scans multiple independent sources with weaker temporal correlations, and it has been widely applied for localizing epileptic foci.
The spherical head model and the boundary element method (BEM) model have been used for modeling the human head when solving the EEG inverse problem.2,15,16 Many investigators have suggested that the use of a BEM model with realistic head geometry provides superior localization accuracy compared to using a three-shell spherical model when analyzing dipole source models.8,17,18 Also, the BEM model was reported to be more reliable than a finite element method forward model in dipole analysis.9 The validity of an ESI result has been assessed by direct comparisons with the intracranially recorded spikes.9,12,19,20,21 These investigations were performed by either comparing intracranially recorded spikes with previously performed noninvasive ESI14,19,20,22 or comparing ESI results with simultaneously recorded intracranial EEG spikes.9,10,23
The aim of the present study was to verify the accuracy of the high-density three-dimensional (3D) ESI analysis method and to analyze epilepsy foci based on the hypothesis that there is a single dipole source. We compared the ESI results with those obtained by presurgical evaluations and MEG source analysis. We also compared ESI and MEG source imaging (MSI) results with the intracranial EEG findings so as to determine their accuracy. Moreover, we evaluated the effects of changing the high-pass filter (HPF) used when producing ESI images.
METHODS
Patients
Standard 10-10 scalp EEG recordings were performed in 27 partial-epilepsy patients; MEG was also recorded in 23 of them. The subjects comprised 11 females and 16 males whose ages ranged from 16 to 55 years (32.4±10.8 years, mean±standard deviation). The age at seizure onset ranged from 1 to 34 years (13.2±10.5 years). The epilepsy syndrome was diagnosed based on the results of a presurgical evaluation including seizure history, video-EEG monitoring, brain MRI, ictal SPECT, SISCOM, and FDG-PET. Thirteen patients underwent epilepsy surgery: nine underwent an invasive EEG study and four had a single-stage anterior temporal lobectomy with amygdalohippocampectomy. Both ESI and MSI were applied to 5 of 9 patients who underwent intracranial EEG recording, while only ESI was applied to the remaining 4 patients.
3D EEG recordings
Standard 10-10 EEG was performed with 70 scalp electrodes and additional EKG1, EKG2, right shoulder, left shoulder, A1, and A2 electrodes in an epilepsy monitoring unit (EMU). Full 10-10 EEG recordings were performed from 1 to 7 days using a NicoletOne LTM system (Natus Medical Incorporated, Pleasanton, CA, USA) at a sampling rate of 512 Hz. The electrode positions were digitized in 3D coordinates using the Brainsight Frameless system (Rogue Research, Montreal, QC, Canada) and an infrared position-sensing camera (Polaris system, Northern Digital Incorporated, Waterloo, ON, Canada). A coil tracker was attached to the patient's head for tracking the head position, and the position-sensing camera captured the light reflected from the tracker in the coordinate space. The 3D coordinates of each of the 70 electrodes were registered manually using a pointing sensor. The coregistration of scalp electrode locations and each brain MR image was achieved by matching the digitized positions of three fiducial points (nasion and left and right preauricular points) with the locations of these points on the MR image.
MEG recording
Magnetoencephalography is a noninvasive neurophysiological technique for detecting the magnetic fields generated by electric currents in the brain that has previously been used to localize the source of epileptic discharges in epilepsy patients.24,25,26,27 MEG was used in the present study to detect spontaneous epileptic discharges. A 152-channel MEG system (KRISS MEG, Daejeon, Korea) covering the whole head was used to make MEG recordings in a magnetically shielded room for 60-90 minutes at a sampling rate of 1,024 Hz. The relative positions of the head and the MEG sensors were determined by attaching four small positioning coils to the head. The positions of the coils were recorded at intervals of 10-15 min by the MEG sensors to allow coregistration with MRI data. The recordings were made with the patients in a sleep-deprived state in order to induce more interictal spikes. The 10-20 EEG system scalp recordings were made simultaneously with the MEG recordings.
Source localization of EEG and MEG
Electroencephalography source localization was performed on EEG recordings acquired during the presurgical investigation. Source localization of individual and averaged spikes was performed using Curry 7 software (Compumedics, Charlotte, NC, USA). ESI and MSI involve EEG- and MEG-based dipole source localizations, respectively, combined with brain MRI.
We used anatomical MRI images to develop each patient's BEM model. To ensure precise boundary modeling, the image's skin, brain, cortex, gray-matter, and white-matter parameters were determined explicitly. For EEG source reconstruction, a realistic three-compartment head model (comprising the skin and the inner and outer skulls) was defined. The BEM conductance was 0.3300 S/m for the skin, 0.0042 S/m for the outer skull, and 0.3300 S/m for the inner skull. MEG source reconstruction was performed using a single-compartment model consisting of only the inner surface of the skull. By selecting exact landmarks on the MRI image, the electrode positions could be accurately adjusted on the BEM.
Electroencephalography and MEG interictal spikes were selected by an experienced epileptologist using visual inspection. The criterion for spike selection was that it had to show a distinct sharp waveform with phase reversal in a bipolar montage followed by a slow wave. Selected spikes were analyzed at the peak point, since previous studies have demonstrated that the use of spike peaks reduces localization errors.8,9 Baseline drift was corrected, and the filtering was set as a low-pass filter (LPF) with a cutoff of 100 Hz and an HPF with a cutoff of 1 or 3 Hz. Spike epochs were generated using a time window from -700 to +300 ms relative to the negative peak. For source analysis we used a single equivalent current dipole model, which is a fixed MUSIC technique. The EEG and MEG dipole source locations were evaluated at the lobar level by presurgical evaluation.
High-pass filter cutoffs
It has been recommended for the HPF cutoff to be set within the range of 2-10 Hz rather than 0.5-1 Hz.28 We therefore analyzed the effects of the following different HPF cutoffs for 64 spikes in one mesial temporal lobe epilepsy (MTLE) patient: 0.5, 1, 2, 3, 4, 5, and 6 Hz. This patient showed frequent scalp EEG spikes, and underwent an intracranial EEG study and both pre- and postoperative brain MRI. The patient had been seizure free for more than 2 years following the surgery. We evaluated the performance with respect to dipole dispersed distances, amplitudes, confidence ellipsoid (CE) volumes, and goodness of fit (GOF) values. The accuracy of a dipole model is commonly assessed by the GOF or residual variance. A smaller CE for the EEG or MEG spike source indicates that the model is more reliable.29 The calculation for CE included the signal-to-noise ratio of the spike, the number of sensors for data recording, and the GOF.30
Presurgical evaluation
The presurgical evaluation included long-term video-EEG monitoring, brain MRI, SPECT, SISCOM, and 18F-fluorodeoxyglucose (FDG)-PET, the Wada test, and neuropsychological tests. Video-EEG monitoring was performed for 4-7 days with full 10-10 EEG electrodes, and interictal spikes and ictal EEG were analyzed. We attempted to identify brain lesions on brain MRI acquired using a 3.0-tesla scanner (Philips Achieva, Philips Medical Systems, Best, The Netherlands) or a 1.5-tesla scanner (Signa, General Electric Medical Systems, Milwaukee, WI, USA). Brain MRI, SPECT, and FDG-PET images were inspected visually. The EEG dipole source location was compared with the visually analyzed EEG interictal spike generation regions, ictal onset zone, and MEG dipole source location, and the neuroimaging test results. The concordance rates between EEG/MEG dipole source location and the result of presurgical evaluation were evaluated at the lobar level and graded by 1, 0.5 or 0. The concordance rate was decided by comparing the results of two different modalities among three modalities (presurgical evaluation, ESI, and MSI). If the results of two modalities indicated the epileptic focus at the same or similar location in the same lobe, the concordance rate was described as "well concordant" and 1. If the locations of two results were far apart in the same lobe, the concordance rate was described as "partially concordant" and 0.5. If two results indicated the epileptic focus in different lobes, the concordance rate was described as "not concordant" and 0.
Intracranial EEG
Thirteen patients underwent resective surgery after presurgical evaluations, and 9 of them underwent intracranial EEG recording. The surgical outcome was followed for 18.2±6.8 months. The gold standard in this study was the comprehensive presurgical evaluations for nonsurgical cases, and the intracranial EEG findings and surgical resection margin for surgical cases. The anatomical concordance rate was evaluated at the sublobar level. Sublobar regions were defined as follows: 1) superior lateral, inferior lateral, medial, and orbitofrontal frontal regions, 2) lateral, mesial, and basal temporal regions, 3) dorsolateral and medial parietal regions, and 4) lateral, medial, and basal occipital regions. Intracranial ECoG recording was performed for 7-10 days prior to the surgical resection, and the interictal spikes and ictal EEG recordings were analyzed.
RESULTS
EEG and MEG source localization
The clinical information, the results of presurgical evaluations, and dipole source localizations of EEG and MEG for 27 patients are summarized in Table 1. There were 21 cases of temporal lobe epilepsy (TLE), 2 of frontotemporal epilepsy, 2 of centroparietal epilepsy, 1 of frontocentral epilepsy, and 1 of temporo-occipital epilepsy. There were 19 lesional patients, of whom 13 had MTLE, and 8 nonlesional patients.
Table 1.
The summary of clinical characteristics, presurgical evaluation results, ESI/MSI results, and concordance rate
| Pt No. | Age (yr) | Sex | Age of onset (yr) | Brain MRI lesion | Interictal spike | Ictal EEG onset | Ictal SPECT | SISCOM | FDG-PET | Epilepsy syndrome | ESI | MSI | ESI and epilepsy syndrome concordance rate | MSI and epilepsy syndrome concordance rate | ESI and MSI concordance rate |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 37 | F | 6 | L P (R/O CD) | L CP | L CP | L P | R P | NP | L CPLE | L post mes & bas T, precuneus, P | L dl P, precuneus | 0.5 | 1 | 0.5 |
| 2 | 24 | F | 9 | L HS | L FT; R FT | Bi FC to FT (L>R) | L F, T; R F | L F, T | L F, T; R T | L MTLE | L ant & mes T | L sup T, insula | 1 | 0.5 | 0.5 |
| 3 | 34 | M | 5 | WNL | L T | Diffuse, L T | L T, F | L F, T | L F, T | L FTLE | L ant mes & bas T | L ant mes & bas T, L OF | 1 | 1 | 1 |
| 4 | 20 | M | 9 | WNL | R FCT | R F; Bi F (R>L) | R F, T, P | R F, T, P | R hemisphere | R FC epilepsy | R ant F | R F, P | 1 | 1 | 1 |
| 5 | 51 | M | 5 | R HS, R inf T (R/O CD) | R FT | R T, FT | R F, T | R F, T | R F, T, Oper, insula | R TLE | R ant & mid T | R ant & mid & post T | 1 | 1 | 1 |
| 6 | 55 | F | 19 | L HS | L FT | L FT | L T | L T | L T | L MTLE | L mid T | L mid T | 1 | 1 | 1 |
| 7 | 21 | F | 15 | L HS | L FT | L FT | L F, BG | L F, T | L F, T | L MTLE | L ant bas T | L ant & mid T, OF | 1 | 1 | 1 |
| 8 | 20 | M | 6 | L HS | L FT | L FT | L T | L T | L T | L MTLE | L ant T | L mid T | 1 | 1 | 1 |
| 9 | 20 | M | 5 | L HS | L FT | L FT | L T; R F, T, P | L T | L T; R F | L MTLE | L ant T | L ant & mid & post T | 1 | 1 | 1 |
| 10 | 20 | M | 3 | L HS | L F | L F, T, P | L F, T | L T | L F, T, insula | L MTLE | L ant T | L ant T | 1 | 1 | 1 |
| 11 | 30 | M | 25 | WNL | L mid post T | L mid post T | L T | L T | NP | L TLE | L ant mes T | L ant & post T | 1 | 1 | 1 |
| 12 | 31 | F | 3 | L HS | L FT | L FT | L F, T | L T, thalamus, insula | L T | L MTLE | L ant bas T | L ant inf & mid sup T | 1 | 1 | 1 |
| 13 | 38 | M | 32 | WNL | L FT; R FT | L T; Bi T | L T | L T, insula | L T | L TLE | L ant T | L ant & mid & post T, insula | 1 | 1 | 1 |
| 14 | 52 | F | 6 | L HS | L FT | Bi FT; L mid post T | L F, T | L T | L T | L MTLE | L ant T | L ant & mid T | 1 | 1 | 1 |
| 15 | 36 | F | 6 | L HS | Bi FT (L>R) | Bi FT (L>R) | L T; R F, T, P | Bi F; L T | NP | Bi TLE (L>R) | L ant & mid bas T | L mid & post T | 1 | 1 | 1 |
| 16 | 29 | F | 16 | L HS, AG high signal, L OF atrophy | L mid post T and FT | L post T | L F, T, P | L T, insula | L F, Oper, T | L MTLE | L ant & mid T | L mid T | 1 | 1 | 1 |
| 17 | 28 | F | 7 | WNL | R FT | R FT; Bi T | L F, T; R F, T | L F, T insula; R T | NP | R FTLE | R ant & mid T | R mid & post T | 1 | 1 | 1 |
| 18 | 24 | M | 16 | R ant sup mid T (R/O ganglioglioma or DNET) | R FT | R FT | NP | NP | R F, T | R TLE | R ant & mid T | R mid & post T | 1 | 1 | 1 |
| 19 | 32 | M | 28 | WNL | R FT | R FT | R T | R T, insula | R T | R TLE | R ant T | R ant T | 1 | 1 | 1 |
| 20 | 16 | M | 8 | L bas O (CD) | L FT | L P, O | L F, T, O | L F, T, insula, O | L T, O | L TOLE | L bas O, ant bas T | L O, post T | 1 | 1 | 1 |
| 21 | 32 | F | 1 | WNL | L C, T, P | Bi CP, FT; R T | R F; L F, T, P | L F, T, P | R F, Oper, P | L CPLE | L CP | No IED* | 1 | - | - |
| 22 | 36 | F | 15 | L HS | L FT | L FT | L T | L T | L T | L MTLE | L ant T | No IED | 1 | - | - |
| 23 | 25 | M | 3 | R HS | R FT | R T | R F, T | R F, T | R F, T; L T | R MTLE | R ant T | No IED | 1 | - | - |
| 24 | 51 | M | 34 | R inf T (R/O CD, R/O DNET) | R FT | R FT | R F, T, P | R F, insula, T | R F, insula, T | R TLE | R bas inf ant T | NP | 1 | - | - |
| 25 | 34 | M | 10 | WNL | R FT | R T | R T | No significant hyper | R T | R TLE | R ant & mid T | NP | 1 | - | - |
| 26 | 39 | M | 33 | L HS (tail), white matter in both P | L FT | L FT | L T | L F, T, AG, HC (head) | Bi T (R>L) | L MTLE | L ant & mid mes T | NP | 1 | - | - |
| 27 | 40 | M | 30 | R bas T | R FT | R FT | R T, insula, P | R T | R T | R TLE | R ant & mid T | NP | 1 | - | - |
*Unable to analyze by artifact.
AG: amygdala, AH: amygdalohippocampectomy, ant: anterior, ATL: anterior temporal lobectomy, bas: basal, Bi: bilateral, C: central, CD: cortical dysplasia, CP: centroparietal, CPLE: centroparietal lobe epilepsy, dl: dorsolateral, DNET: dysembryoplastic neuroepithelial tumor, ESI: EEG source imaging, F: frontal, FC: frontocentral, FCT: frontocentrotemporal, FT: frontotemporal, FTLE: frontotemporal lobe epilepsy, HC: hippocampus, HS: hippocampal sclerosis, hyper: hyperperfusion, IED: interictal epileptiform discharge, inf: inferior, L: left, lat: lateral, med: medial, MEG: magnetoencephalography, mes: mesial, MSI: MEG source imaging, mid: middle, MTLE: mesial TLE, NP: not performed, O: occipital, Oper: operculum, OF: orbitofrontal, P: parietal, post: posterior, R: right, R/O: rule out, SISCOM: Subtraction Ictal SPECT coregistered to MRI, sup: superior, T: temporal, TLE: temporal lobe epilepsy, TOLE: temporo-occipital lobe epilepsy, WNL: within normal limit.
The concordance rate of ESI and MSI was determined based on the presurgical evaluation and ECoG. ESI was well concordant with the results of presurgical evaluation in 26 of the 27 (96.3%) patients, and partially concordant in remaining patient (3.7%). Meanwhile, MSI was well concordant with the results of presurgical evaluation in all but three patients whose MEG spikes were not recorded. The MSI results were well concordant with the ESI results in 18 of 20 (90.0%) patients and partially concordant in 2 (10.0%). The remaining three patients exhibited only EEG spikes (i.e., no MEG spikes).
Fig. 1 shows the ESI (Fig. 1A), MSI (Fig. 1B), and neuroimaging results of patient #14, who had MTLE. Both ESI and MSI were analyzed with left anterior temporal spikes with a BEM volume conductor. The HPF cutoff was 3 Hz, and dipole sources with GOF values above 70% are plotted in the figure.
Fig. 1.
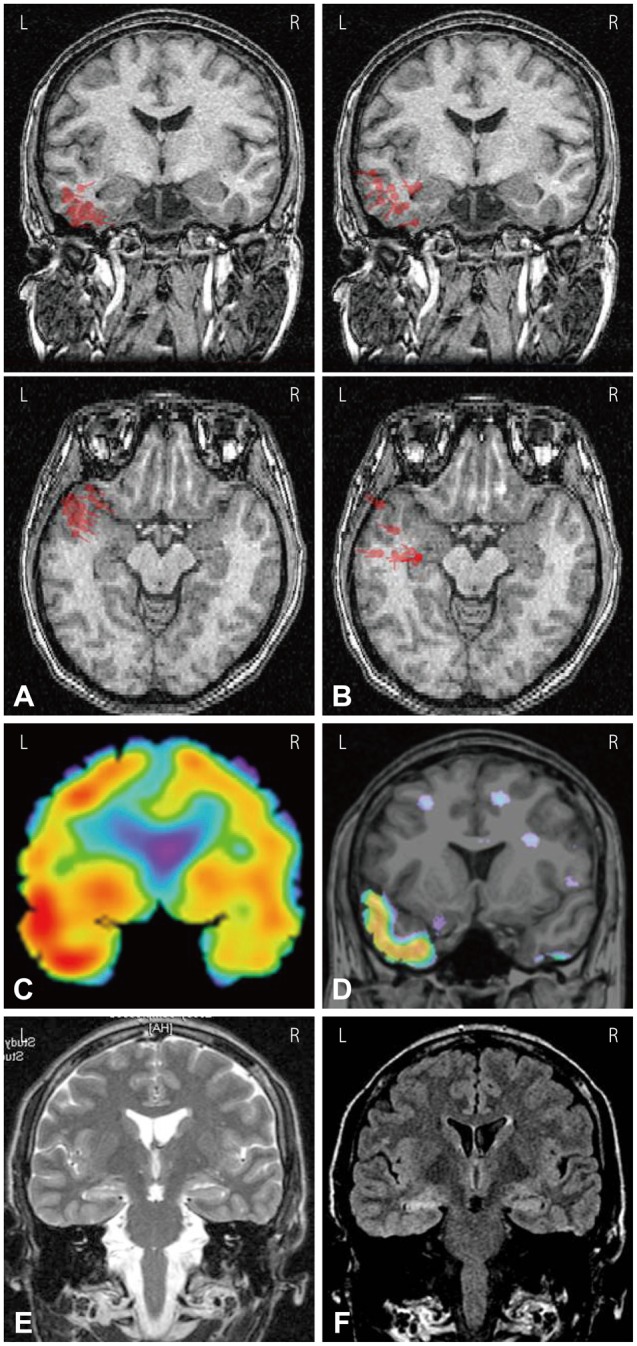
EEG and MEG dipole source analysis of patient #14 who had left temporal lobe epilepsy. A: EEG dipoles [high-pass filter (HPF)=3 Hz, goodness of fit (GOF) levels ≥70%] were localized in left basal and anterior temporal regions. B: MEG dipoles (HPF=3 Hz, GOF levels ≥70%) were localized in left anterior to middle temporal regions. C: Ictal SPECT showed left temporal hyperperfusion. D: SISCOM showed left anterior to mid temporal hyperperfusion. (E) T2-weighted MRI and (F) FLAIR MRI showed left hippocampal sclerosis. L: left, R: right.
Thirteen patients (#2, 5, 6, 7, 8, 9, 10, 12, 14, 16, 22, 23, and 26) were diagnosed as MTLE with hippocampal sclerosis (HS), and most of these patients' EEG dipoles were quite consistently localized in the anterior, basal, or mesial temporal region ipsilateral to the side of HS. The numbers of analyzed EEG dipoles differed markedly between the patients (from 5 to 65 spikes), and several dipoles were located in front of the ipsilateral anterior temporal region, which is outside the temporal cortex. However, MEG dipole sources were not consistently localized in the same region. MEG dipoles were distributed more widely in the anterior, superior, middle, and posterior lateral temporal regions, and occasionally in the insula or frontal region. Most of the MEG dipoles were localized in cortical surface areas.
Six patients (#1, 5, 18, 20, 24, and 27) had a lesion in the cortical surface area. Both ESI and MSI analyses were performed in patient #1, 5, 18, and 20. Patient #1 showed cortical dysplasia in the left parietal lobe extending from the cortical surface to the deep white matter, and was diagnosed as left centroparietal lobe epilepsy. ESI showed dipoles in the deep white matter of the left parietal lobe, with the results being partially concordant with presurgical evaluation, whereas MSI showed dipoles in the left dorsolateral parietal cortex. Patient #5 had right HS and cortical dysplasia in the right inferior temporal region. The EEG dipoles were observed in the right mesial, anterior, and middle temporal regions, whereas MEG dipoles were observed throughout the right whole lateral temporal lobe. The EEG dipoles were more widely distributed in this patient than in the patients who had only HS. In patient #18, a cystic tumor was located in the right anterior-superior temporal region, and a calcification was found in the right perihippocampal region. The EEG dipoles were located on the mesial side of the right temporal lobe, whereas the MEG dipoles were located on the lateral side. In patient #20, who had left basal occipital cortical dysplasia, the EEG dipoles were located in both the left anterior temporal and basal occipital regions. However, the MEG dipoles were located in the left occipital lobe. In patient #24 and 27, a benign tumor and cortical dysplasia were located in the right inferior temporal and basal temporal regions, respectively. The EEG dipoles were localized near those lesions.
Brain MRI revealed no lesion in eight patients (#3, 4, 11, 13, 17, 19, 21, and 25). When the ESI and MSI results were compared with the location of the epileptic focus determined by the presurgical evaluation, the locations of all EEG and MEG dipoles were well concordant with those epileptic foci at the lobar level. The comparison between the ESI and MSI results revealed differences at the sublobar level. In patient #3, the ESI and MSI results were similar at the sublobar level. However, the EEG and MEG dipoles of the other patients differed slightly at the sublobar level. The EEG dipoles were located more anteriorly than the MEG dipoles in patient #4 (Fig. 2). In patient #11 and 13, EEG dipoles were located in the left anterior temporal lobe whereas the MEG dipoles were seen throughout the anterior, middle, and posterior temporal regions.
Fig. 2.
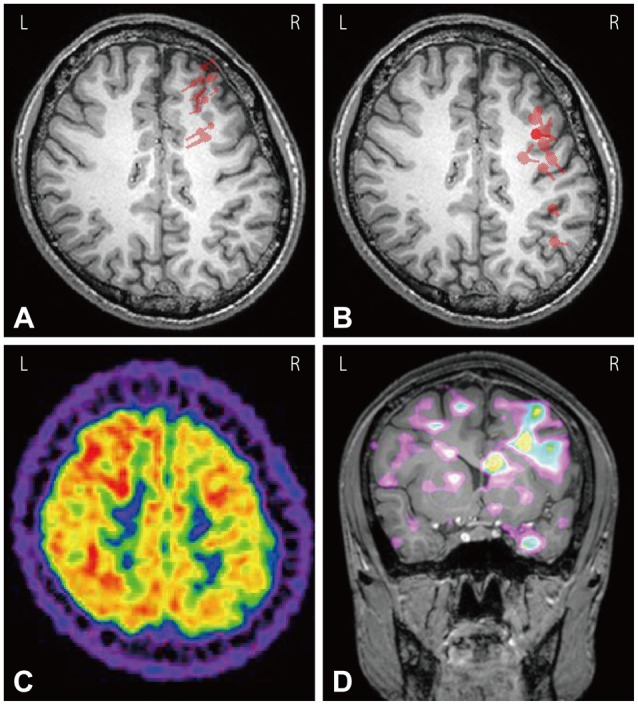
EEG and MEG dipole source analysis of patient #4 who had right frontocentral lobe epilepsy. A: EEG dipoles [high-pass filter (HPF)=3 Hz, goodness of fit (GOF) levels ≥70%] were localized in right frontal lobe. B: MEG dipoles (HPF=3 Hz, GOF levels ≥70%) were localized in right frontal and parietal regions. C: FDG-PET showed hypometabolism in right frontoparietal cortex. D: SISCOM showed ictal hyperperfusion in the right dorsolateral and medial frontal cortices. L: left, R: right.
Concordance of ESI and MSI with intracranial EEG
Table 2 presents the results of epilepsy surgery. Five of 9 patients who underwent invasive EEG recordings demonstrated both high-density EEG and MEG dipole source localization. The concordance rate of the ESI and MSI results with intracranial EEG findings was 88.9% for ESI in 9 patients and 80% for MSI in 5 patients. Among 13 surgery patients, 10 (76.9%), 1 (7.7%), and 2 (15.4%) patients had outcomes of Engel classes IA, IIIA, and IIIB, respectively.
Table 2.
The summary of ECoG, pathology and surgical outcome in 13 patients
| Pt No. | ECoG interictal spikes | ECoG ictal onset zone | ESI-ECoG concordance rate | MSI-ECoG concordance rate | Surgical resection area | Pathology | Postop. F/U duration | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | L inf & ant to mid sup P, post cingulate gyrus | L inf & ant to mid sup P | 1 | 1 | L sup & med P, post cingulate gyrus | FCD IIB in P | 1 yr 1 mo | IIIB |
| 2 | L inf lat & mes & post lat T | L mes & lat bas T | 1 | 1 | L ATL/AH, lat bas T | HS, FCD IIIA in T | 1 yr 1 mo | IA |
| 3 | L OF, mes & inf lat T, HC head | L OF, mes & lat T | 1 | 1 | L ATL/AH & OF | Minimal cortical dyslamination in F, FCD IC in T, Focal infarct in HC | 2 yr 5 mo | IIIA |
| 4 | R med F, OF, lat & bas T, inf P | R med & lat F, OF, lat & bas T, inf P | 1 | 1 | R ant & mid F, inf P | Dense fibrous tissue and floating arachroid cells S/O arachroid cyst in F, P | 1 yr 4 mo | IA |
| 5 | R mes & lat T, AG, HC head | R mes T, AG | 0.5 | 0.5 | R ATL/AH | HS, FCD IIIA in T | 1 yr 7 mo | IA |
| 6 | NP | NP | - | - | L ATL/AH | HS, FCD IIIA in T | 1 yr 1 mo | IA |
| 7 | NP | NP | - | - | L ATL/AH | HS, FCD IIIA in T | 1 yr 2 mo | IA |
| 8 | NP | NP | - | - | L ATL/AH | HS, FCD IIIA in T | 1 yr 2 mo | IA |
| 23 | NP | NP | - | - | R ATL/AH | HS, FCD IIIA in T | 1 yr 4 mo | IA |
| 24 | R mes & bas & lat T, HC body | R mes to bas T, HC body | 1 | - | R ATL/AH & R OF | FCD IC in OF, FCD IC & IB in T | 1 yr 5 mo | IA |
| 25 | R mes & bas & lat T, HC head to body | R post lat & bas & mes & sup lat T, AG to HC body | 1 | - | R extended ATL/AH, lat T | FCD IC in ant T, FCD 1A in sup lat T | 1 yr 1 mo | IIIB |
| 26 | L mes & bas & ant lat T, HC head to tail | L mes T, HC head to tail | 1 | - | L ATL/AH | HS, FCD IIIA in T | 2 yr 5 mo | IA |
| 27 | R bas T (lesion), mes & lat T, HC head to body | R bas T (lesion) | 1 | - | R ATL/AH, R lat & R bas T | FCD IIIC in lat T, cavernous angioma in bas T (lesion) | 2 yr 7 mo | IA |
AG: amygdala, AH: amygdalohippocampectomy, ant: anterior, ATL: anterior temporal lobectomy, bas: basal, Bi: bilateral, ECoG: electrocorticography, ESI: EEG source imaging, F: frontal, FCD: focal cortical dysplasia, HC: hippocampus, HS: hippocampal sclerosis, F/U: follow up, inf: inferior, L: left, lat: lateral, med: medial, mes: mesial, mid: middle, mo: month, MSI: MEG source imaging, NP: not performed, OF: orbitofrontal, P: parietal, post: posterior, R: right, S/O: suggestive of, sup: superior, T: temporal, yr: year.
In patient #1, the EEG dipoles were localized in deeper white matter of the left parietal lobe compared to the ECoG interictal spikes recorded by subdural electrodes, whereas the MEG dipoles were well concordant with the location of the ECoG spikes. However, we did not make EEG recordings in deep white matter where cortical dysplasia was present. In patient #2, ECoG showed frequent spikes in the left inferior and mesial temporal regions and less frequent spikes in the lateral mid-posterior temporal region. The EEG dipoles were located in the mesial and anterior basal temporal regions, whereas the MEG dipoles were located in the superior lateral temporal region. The surgical pathology revealed left HS and cortical dysplasia in the left anterior and basal temporal regions. In patient #3, intracranial electrodes were inserted in the left temporal and frontal regions. ECoG showed interictal spikes in the left basal temporal and orbitofrontal regions. The ESI and MSI results were well concordant with ECoG spikes in the left temporal region. However, only MSI (i.e., not ESI) showed dipoles in the orbitofrontal region too. In patient #4, who had interictal spikes in the right frontal lobe in ECoG, the EEG dipoles were located in more-anterior frontal regions, whereas the MEG dipoles were located in the frontal and parietal regions (Fig. 2A and B). In patient #5, who had right HS and inferior temporal cortical dysplasia, the EEG dipoles were located in the right mesial and basal temporal regions, whereas the MEG dipoles were located more diffusely in the right temporal lobe. ECoG showed interictal spikes most frequently in the mesial temporal region, followed by the anterior, middle, and posterior temporal regions.
Comparison of different HPF cutoffs
The 64 individual EEG dipoles of patient #26, who had left MTLE, are plotted in Fig. 3. Dipoles were analyzed in a preoperative BEM head model for different HPF cutoffs, and are superimposed on postoperative MRI results in the figure. The HPF cutoffs were 0.5, 1, 2, 3, 4, 5, and 6 Hz for A to G in Fig. 3. The LPF cutoff was 100 Hz in all cases. Fig. 3H shows the dipoles of averaged 64 spikes for different HPF cutoffs using the same colors as in A-G. Individual EEG dipoles are dispersed in location and orientation around the averaged dipole.
Fig. 3.

Different high-pass filter (HPF) setting. The 64 individual dipoles of patient #26 who had left mesial temporal lobe epilepsy. EEG dipoles were analyzed in preoperative boundary element method (BEM) head model in different HPF settings and superimposed on the postoperative MRI. HPF settings were as follow: (A) 0.5 Hz, (B) 1Hz, (C) 2 Hz, (D) 3 Hz, (E) 4 Hz, (F) 5 Hz, and (G) 6 Hz. Low pass filter settings were all 100 Hz. The H shows averaged dipoles of A-G with the matched color. Circles surrounding each dipole indicate confidence ellipsoid range. Each color indicates different HPF setting (red: 0.5 Hz, orange: 1 Hz, yellow: 2 Hz, green: 3 Hz, bright blue: 4 Hz, blue: 5 Hz, violet: 6 Hz). L: left, R: right.
Table 3 lists the HPF cutoffs and the mean distance and variance values for the 64 individual EEG dipoles relative to the average EEG dipole obtained by statistical analysis. The results indicate that an HPF cutoff of 3 Hz minimized the distances of the EEG dipoles from the averaged dipole and the CE value. GOF was also maximum for an HPF cutoff of 3 Hz, but the amplitude was not maximum and the mean amplitude of the dipoles became smaller as the HPF cutoff increased.
Table 3.
The effect of high-pass filter change on EEG source imaging
| HPF (Hz) | Mean single dipole distance from the averaged dipole location (mm) | Amp (µAmm) | Confidence ellipsoid (mL) | GOF (%) |
|---|---|---|---|---|
| 0.5 | 20.6±8.1 | 822.7±289.7 | 602.5±816.5 | 82.3±5.4 |
| 1 | 19.1±7.7 | 786.4±297.3 | 554.0±831.9 | 83.4±4.8 |
| 2 | 17.4±7.4 | 781.9±252.3 | 344.1±495.4 | 85.5±3.6 |
| 3 | 15.3±6.1 | 763.4±230.2 | 297.9±394.8 | 85.9±4.0 |
| 4 | 15.6±6.1 | 661.1±204.1 | 389.1±547.3 | 83.8±5.4 |
| 5 | 15.5±5.9 | 500.6±170.1 | 634.1±886.1 | 79.8±7.0 |
| 6 | 18.0±8.0 | 395.5±228.7 | 891.6±1936.1 | 75.7±9.4 |
Values are mean±SD.
Amp: amplitude, GOF: goodness of fit, HPF: high-pass filter.
Fig. 4 compares the ECoG findings and the EEG dipoles of patient #26 with left MTLE. The electrode location of ictal EEG onset in ECoG is indicated by a red circle (Fig. 4A), and the location of interictal spikes frequently recorded in ECoG is indicated by a bright blue circle. The ESI results for the averaged 64 spikes as obtained when using different HPF cutoffs are shown in Fig. 4B in different colors. The circle around each dipole indicates the CE range.
Fig. 4.
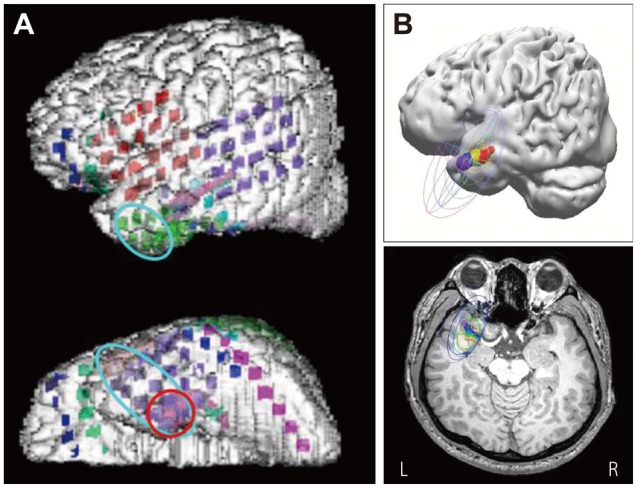
The comparison between ECoG and EEG dipoles of patient #26. The patient had left mesial temporal lobe epilepsy. A: Intracranial EEG electrode locations were plotted on the patient's three dimensional MRI. Red circle indicates the electrode location of ictal ECoG onset, and bright blue circle indicates the location of interictal spikes frequently recorded on ECoG. B: EEG dipoles of averaged 64 spikes with different high-pass filter settings: red: 0.5 Hz, orange: 1 Hz, yellow: 2 Hz, green: 3 Hz, bright blue: 4 Hz, blue: 5 Hz, violet: 6 Hz. The circle around each dipole indicates confidence ellipsoid range. L: left, R: right.
DISCUSSION
Various neuroimaging techniques have been applied for the presurgical evaluation of epilepsy. Brain MRI, FDG-PET, SPECT, and SISCOM are widely used, whereas noninvasive ESI and MSI techniques are utilized in only a small number of centers. The clinical usefulness of MSI has been verified, and while the clinical role and usefulness of ESI have been emphasized, it is still only at the investigation stage.11 The present study analyzed 70-channel ESI prospectively and compared the results with those obtained using MSI and other types of presurgical evaluation. To solve the inverse problem, we applied 70-channel EEG in the EMU and applied an individual patient head model for the ESI analysis, and we digitized each patient's electrode positions on the patient's brain MRI images. We also performed a detailed ESI reliability analysis by applying different HPF cutoffs for detecting the interictal spikes.
We found that the ESI results were well concordant at the lobar level with the presurgical evaluations. While this is similar to the results obtained in previous studies, the present study differs from previous ESI studies in several notable ways. In a study of 128-channel ESI, 5 of 7 patients who underwent intracranial EEG recording in addition to the routine presurgical evaluation had consistent EEG dipoles at the lobar level, but they used a three shell sphere model.6 A previous study found a high level of agreement between intracranial EEG and ESI findings, although the recordings were not made simultaneously.11 However, they used a three-shell sphere forward modeling method with standardized electrode positions. Previous ESI studies have focused on TLE and have usually addressed reliability and validity only indirectly.4,6,11 On the other hand, ESI has rarely been applied to extra-TLE patients. A previous study performed high-density EEG recordings (128-256 channels) and volumetric brain MRI in 27 patients with extra-TLE,4 but 3D digitizing of electrode locations was not conducted. That study analyzed the mid-uprising time point of interictal spikes, and there is still debate about the analysis of spike time points. Analyzing the peak spike point seems to be more appropriate than analyzing the onset point or a point between the onset and peak time of a spike in similar studies that used a single equivalent dipole model,8,9 so we decided to analyze the peak spike point. Other study also investigated ESI with 256-channel EEG recordings in 7 MTLE patients.10 However, they used an Montreal Neurological Institute head model with standard brain electrode positions, whose head geometry is less realistic. In the ESI analysis performed in the present study, we applied a dipole source analyzing technique using individualized realistic forward models based on the patients' 3D digitized electrode positions and a BEM model. A previous study applied ESI with a 76-channel scalp EEG system and digitized the electrode locations,8 but used a modified 10-20 EEG system that differs from the 10-10 system used in the present study. That study compared the effects of the electrode density and the use of different head models on the localization accuracy, but the effects of different HPF cutoffs were not analyzed.
In the present study, we found that EEG dipoles were concordant at the lobar level with the results of presurgical evaluations in 26 of the 27 patients (96.3%) when using 70-channel EEG recording. This is similar to previous studies' findings; 93.7% lobar-level concordance in 32 patients with 128-channel EEG6 and 90% lobar-level concordance in 30 patients with EEG employing fewer than 30 channels.7 It therefore seems that the number of electrodes does not greatly influence the lobar-level concordance rate. In our study, the concordance rate at the sublobar level of EEG dipoles with the intracranial EEG findings was 88.9% (8 of 9 patients), with the remaining patient showing partial concordance.
Previous studies found that using more scalp EEG electrodes improved the spatial resolution.5,11 Although those authors proposed that it is necessary to use more than 63 scalp EEG electrodes in order to reduce the distance from the resection margin to less than 2 cm, the ideal number of scalp electrodes for ESI analysis remains to be determined in future investigations.11 A previous study used an electrode cap to implement 152-channel EEG with high spatial resolution over a 1-hour monitoring period.4 However, the use of an electrode cap has potential limitations of unreliable electrode-scalp contacts and poor long-term EEG recordings,11 which contrasts with EEG generally being known for its advantage of long-term recording and its insensitivity to changes in head position. Therefore, applying the 10-10 EEG system is recommended for optimal EEG dipole source analysis.
Simple equivalent dipole fitting analysis is a good source estimation technique for localizing an epileptic focus.14,31 A distributed source model (e.g., Low Resolution Brain Electromagnetic Tomography, LORETA) yields a distributed electric field density rather than the focal modality, and it may also display widely dispersed unrelated information. A previous study that performed EEG dipole source analysis with a 27-channel scalp EEG system and simultaneous ECoG recording in one patient with MTLE demonstrated the high concordance between these measurements;9 the present study also found a high concordance rate between ESI results and ECoG findings in 9 diverse patients with lesional or nonlesional partial epilepsy.
In single dipole source localization, the EEG dipole source may move when different HPF cutoffs are used. This characteristic has resulted in some confusion among investigators when determining the location of the EEG dipole, indicating the necessity of comparing the effect of different HPF cutoffs. It has been reported that the EEG source activity onset is best demarcated by using a higher HPF cutoff, with one within the range of 2-10 Hz being preferable over one within the range of 0.5-1 Hz.28 We found that the distribution of individual spike dipoles was most consistent with the averaged dipole when a 3 Hz HPF cutoff was applied; HPF cutoffs lower or higher than 3 Hz resulted in dipoles of wider dispersion, and lower signal amplitude and greater CE. These results are consistent with a previous ESI study finding that a 3 Hz HPF cutoff was the most appropriate.9
Our study analyzed both EEG and MEG dipoles in 23 patients. In a single dipole source analysis of EEG, the EEG dipoles tended to be localized in brain regions deeper than the cortex in patients with MTLE. This result is similar to a previous study finding spike dipoles localized in deeper brain regions, such as white matter, than actual cortex.32 It is known that MEG is less sensitive to deep brain sources because the signals decrease in proportion with the square of the distance from the source.33 Our MSI analysis also showed that the distribution was wider over lateral and whole temporal regions. However, MSI in our study showed a high concordance rate of 100% at the lobar level compared with the presurgical evaluation results, and of 80% (4 of 5 patients) at the sublobar level compared with intracranial EEG results.
In MTLE patients, the ESI results were the most correctly localized to the anterior, basal, or mesial region of the temporal lobe. The ESI results obtained in neocortical and nonlesional epilepsy patients were not as accurate as those in MTLE patients, although the EEG dipoles were reasonably well localized at the lobar level compared with presurgical evaluations and intracranial EEG results. EEG recordings of interictal spikes can be made over a longer time period than MEG recordings, which are typically limited to only about 1 hour. Therefore, patients who exhibit rare interictal spikes during EMU period will tend to show no MEG spikes during a 1-hour recording session. Moreover, ESI is more feasible than MSI for patients with mental retardation or young children because many such subjects find it difficult to remain motionless for an hour. Finally, MEG signals are affected by the presence of metal objects, so large artifacts in MEG recordings can be present when patients have metallic dental implants. Such noise contamination of MEG channels may affect the MSI results even when the MEG reader turns off those channels. In contrast, ESI can be applied more generally since it is not affected by the presence of metallic implants.
There are several problems to be solved in ESI. Our study was an individualized investigation that developed an individual's forward model and coregistered the patient's brain MRI with the scalp electrode position. However, the volume conductor can be different in different patients. The same values for three conductor parameters (skin and the inner and outer skulls) were applied to all patients in our study, whereas the conductance of the skin and skull may differ between patients, especially in postsurgical patients, which may exert an inhomogeneous skull conductor effect in the EEG source analysis. Another issue that needs to be addressed is identifying a more accurate method for analyzing ESI in patients with neocortical epilepsy.
Acknowledgements
This study was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (HI10C2020).
Footnotes
Conflicts of Interest: The authors have no financial conflicts of interest.
References
- 1.Diekmann V, Becker W, Jürgens R, Grözinger B, Kleiser B, Richter HP, et al. Localisation of epileptic foci with electric, magnetic and combined electromagnetic models. Electroencephalogr Clin Neurophysiol. 1998;106:297–313. doi: 10.1016/s0013-4694(97)00142-9. [DOI] [PubMed] [Google Scholar]
- 2.Ding L, Worrell GA, Lagerlund TD, He B. Ictal source analysis: localization and imaging of causal interactions in humans. Neuroimage. 2007;34:575–586. doi: 10.1016/j.neuroimage.2006.09.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brodbeck V, Spinelli L, Lascano AM, Pollo C, Schaller K, Vargas MI, et al. Electrical source imaging for presurgical focus localization in epilepsy patients with normal MRI. Epilepsia. 2010;51:583–591. doi: 10.1111/j.1528-1167.2010.02521.x. [DOI] [PubMed] [Google Scholar]
- 4.Brodbeck V, Spinelli L, Lascano AM, Wissmeier M, Vargas MI, Vulliemoz S, et al. Electroencephalographic source imaging: a prospective study of 152 operated epileptic patients. Brain. 2011;134(Pt 10):2887–2897. doi: 10.1093/brain/awr243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lantz G, Grave de Peralta R, Spinelli L, Seeck M, Michel CM. Epileptic source localization with high density EEG: how many electrodes are needed? Clin Neurophysiol. 2003;114:63–69. doi: 10.1016/s1388-2457(02)00337-1. [DOI] [PubMed] [Google Scholar]
- 6.Michel CM, Lantz G, Spinelli L, De Peralta RG, Landis T, Seeck M. 128-channel EEG source imaging in epilepsy: clinical yield and localization precision. J Clin Neurophysiol. 2004;21:71–83. doi: 10.1097/00004691-200403000-00001. [DOI] [PubMed] [Google Scholar]
- 7.Sperli F, Spinelli L, Seeck M, Kurian M, Michel CM, Lantz G. EEG source imaging in pediatric epilepsy surgery: a new perspective in presurgical workup. Epilepsia. 2006;47:981–990. doi: 10.1111/j.1528-1167.2006.00550.x. [DOI] [PubMed] [Google Scholar]
- 8.Wang G, Worrell G, Yang L, Wilke C, He B. Interictal spike analysis of high-density EEG in patients with partial epilepsy. Clin Neurophysiol. 2011;122:1098–1105. doi: 10.1016/j.clinph.2010.10.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wennberg R, Cheyne D. EEG source imaging of anterior temporal lobe spikes: validity and reliability. Clin Neurophysiol. 2014;125:886–902. doi: 10.1016/j.clinph.2013.09.042. [DOI] [PubMed] [Google Scholar]
- 10.Yamazaki M, Terrill M, Fujimoto A, Yamamoto T, Tucker DM. Integrating dense array EEG in the presurgical evaluation of temporal lobe epilepsy. ISRN Neurol. 2012;2012:924081. doi: 10.5402/2012/924081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Plummer C, Harvey AS, Cook M. EEG source localization in focal epilepsy: where are we now? Epilepsia. 2008;49:201–218. doi: 10.1111/j.1528-1167.2007.01381.x. [DOI] [PubMed] [Google Scholar]
- 12.Zumsteg D, Friedman A, Wennberg RA, Wieser HG. Source localization of mesial temporal interictal epileptiform discharges: correlation with intracranial foramen ovale electrode recordings. Clin Neurophysiol. 2005;116:2810–2818. doi: 10.1016/j.clinph.2005.08.009. [DOI] [PubMed] [Google Scholar]
- 13.Ebersole JS, Hawes-Ebersole S. Clinical application of dipole models in the localization of epileptiform activity. J Clin Neurophysiol. 2007;24:120–129. doi: 10.1097/WNP.0b013e31803ece13. [DOI] [PubMed] [Google Scholar]
- 14.Gavaret M, Trébuchon A, Bartolomei F, Marquis P, McGonigal A, Wendling F, et al. Source localization of scalp-EEG interictal spikes in posterior cortex epilepsies investigated by HR-EEG and SEEG. Epilepsia. 2009;50:276–289. doi: 10.1111/j.1528-1167.2008.01742.x. [DOI] [PubMed] [Google Scholar]
- 15.Huppertz HJ, Hoegg S, Sick C, Lücking CH, Zentner J, Schulze-Bonhage A, et al. Cortical current density reconstruction of interictal epileptiform activity in temporal lobe epilepsy. Clin Neurophysiol. 2001;112:1761–1772. doi: 10.1016/s1388-2457(01)00588-0. [DOI] [PubMed] [Google Scholar]
- 16.He B, Musha T, Okamoto Y, Homma S, Nakajima Y, Sato T. Electric dipole tracing in the brain by means of the boundary element method and its accuracy. IEEE Trans Biomed Eng. 1987;34:406–414. doi: 10.1109/tbme.1987.326056. [DOI] [PubMed] [Google Scholar]
- 17.Herrendorf G, Steinhoff BJ, Kolle R, Baudewig J, Waberski TD, Buchner H, et al. Dipole-source analysis in a realistic head model in patients with focal epilepsy. Epilepsia. 2000;41:71–80. doi: 10.1111/j.1528-1157.2000.tb01508.x. [DOI] [PubMed] [Google Scholar]
- 18.Roth BJ, Ko D, von Albertini-Carletti IR, Scaffidi D, Sato S. Dipole localization in patients with epilepsy using the realistically shaped head model. Electroencephalogr Clin Neurophysiol. 1997;102:159–166. doi: 10.1016/s0013-4694(96)95111-5. [DOI] [PubMed] [Google Scholar]
- 19.Gavaret M, Badier JM, Marquis P, Bartolomei F, Chauvel P. Electric source imaging in temporal lobe epilepsy. J Clin Neurophysiol. 2004;21:267–282. doi: 10.1097/01.wnp.0000139929.06455.82. [DOI] [PubMed] [Google Scholar]
- 20.Merlet I, Gotman J. Reliability of dipole models of epileptic spikes. Clin Neurophysiol. 1999;110:1013–1028. doi: 10.1016/s1388-2457(98)00062-5. [DOI] [PubMed] [Google Scholar]
- 21.Plummer C, Litewka L, Farish S, Harvey AS, Cook MJ. Clinical utility of current-generation dipole modelling of scalp EEG. Clin Neurophysiol. 2007;118:2344–2361. doi: 10.1016/j.clinph.2007.08.016. [DOI] [PubMed] [Google Scholar]
- 22.Gavaret M, Badier JM, Marquis P, McGonigal A, Bartolomei F, Regis J, et al. Electric source imaging in frontal lobe epilepsy. J Clin Neurophysiol. 2006;23:358–370. doi: 10.1097/01.wnp.0000214588.94843.c2. [DOI] [PubMed] [Google Scholar]
- 23.Lantz G, Holub M, Ryding E, Rosén I. Simultaneous intracranial and extracranial recording of interictal epileptiform activity in patients with drug resistant partial epilepsy: patterns of conduction and results from dipole reconstructions. Electroencephalogr Clin Neurophysiol. 1996;99:69–78. doi: 10.1016/0921-884x(96)95686-6. [DOI] [PubMed] [Google Scholar]
- 24.Jin K, Nakasato N, Shamoto H, Kanno A, Itoyama Y, Tominaga T. Neuromagnetic localization of spike sources in perilesional, contralateral mirror, and ipsilateral remote areas in patients with cavernoma. Epilepsia. 2007;48:2160–2166. doi: 10.1111/j.1528-1167.2007.01228.x. [DOI] [PubMed] [Google Scholar]
- 25.Knowlton RC, Laxer KD, Aminoff MJ, Roberts TP, Wong ST, Rowley HA. Magnetoencephalography in partial epilepsy: clinical yield and localization accuracy. Ann Neurol. 1997;42:622–631. doi: 10.1002/ana.410420413. [DOI] [PubMed] [Google Scholar]
- 26.Nakasato N, Levesque MF, Barth DS, Baumgartner C, Rogers RL, Sutherling WW. Comparisons of MEG, EEG, and ECoG source localization in neocortical partial epilepsy in humans. Electroencephalogr Clin Neurophysiol. 1994;91:171–178. doi: 10.1016/0013-4694(94)90067-1. [DOI] [PubMed] [Google Scholar]
- 27.Stefan H. Clinical applications of MEG in epilepsy. Brain Topogr. 1993;5:425–427. doi: 10.1007/BF01128701. [DOI] [PubMed] [Google Scholar]
- 28.Scherg M, Bast T, Berg P. Multiple source analysis of interictal spikes: goals, requirements, and clinical value. J Clin Neurophysiol. 1999;16:214–224. doi: 10.1097/00004691-199905000-00003. [DOI] [PubMed] [Google Scholar]
- 29.Ebersole JS, Ebersole SM. Combining MEG and EEG source modeling in epilepsy evaluations. J Clin Neurophysiol. 2010;27:360–371. doi: 10.1097/WNP.0b013e318201ffc4. [DOI] [PubMed] [Google Scholar]
- 30.Fuchs M, Wagner M, Kastner J. Confidence limits of dipole source reconstruction results. Clin Neurophysiol. 2004;115:1442–1451. doi: 10.1016/j.clinph.2004.01.019. [DOI] [PubMed] [Google Scholar]
- 31.Rose S, Ebersole JS. Advances in spike localization with EEG dipole modeling. Clin EEG Neurosci. 2009;40:281–287. doi: 10.1177/155005940904000410. [DOI] [PubMed] [Google Scholar]
- 32.Ebersole JS. EEG dipole modeling in complex partial epilepsy. Brain Topogr. 1991;4:113–123. doi: 10.1007/BF01132768. [DOI] [PubMed] [Google Scholar]
- 33.Rampp S, Stefan H. On the opposition of EEG and MEG. Clin Neurophysiol. 2007;118:1658–1659. doi: 10.1016/j.clinph.2007.04.021. [DOI] [PubMed] [Google Scholar]