

Abstract
Background
Obesity and being overweight are both significant risk factors for multiple chronic conditions. Primary care physicians are in a position to provide health behavior counseling to the majority of US adults, yet most report insufficient training to deliver effective counseling for obesity.
Objective
To assess the degree to which residents training in adult primary care programs are prepared to provide obesity, nutrition, and physical activity (ONPA) counseling.
Methods
Senior residents (postgraduate year [PGY]-3 and PGY-4) from 25 Ohio family medicine, internal medicine, and obstetrics and gynecology programs were surveyed regarding their knowledge about obesity risks and effective counseling, as well as their attitudes, self-efficacy, and perceived professional norms toward ONPA counseling. We examined summary scores, and used regression analyses to assess associations with resident demographics and training program characteristics.
Results
A total of 219 residents participated (62% response rate). Mean ONPA counseling knowledge score was 50.8 (± 15.6) on a 0 to 100 scale. Specialty was associated with counseling self-efficacy (P < .001) and perceived norms (P = .002). Residents who reported having engaged in an elective rotation emphasizing ONPA counseling had significantly higher self-efficacy and more positive attitudes and professional norms scores.
Conclusions
Our findings suggest that primary care residents' knowledge of ONPA assessment and management strategies has room for improvement. Attitudes, self-efficacy, and perceived norms also are low and vary by training program characteristics. A deeper understanding of curricula associated with improved performance in these domains could inform interventions to enhance residents' ONPA counseling skills and prevent chronic disease.
Editor's Note: The online version of this article contains the obesity, nutrition, and physical activity counseling preparedness assessment measures.
Introduction
Being overweight or obese is a risk factor for cardiovascular disease, type 2 diabetes mellitus, dyslipidemia, hypertension, osteoarthritis, and several cancers1–3 and remains common in the United States. Today, more than two-thirds of American adults are overweight, with approximately 35% considered obese (body mass index ≥ 30).4,5 Primary care providers have been called on to help address this epidemic by screening for obesity during ambulatory visits and providing weight reduction, nutrition, and physical activity counseling to their overweight and obese patients.6–11 Although several guidelines exist for this counseling,8,9,12–14 and mounting evidence shows physician advice can encourage weight loss among patients,15–17 weight-related counseling during ambulatory visits occurs at modest rates and is infrequently aligned with recommended methods shown to support behavior change.18–23 Studies examining barriers to weight counseling in primary care practice suggest physicians feel inadequately trained, and report a lack of time and poor self-efficacy to counsel on weight management.24–28 Additionally, physicians may hold negative attitudes toward overweight and obese patients and their ability to sustain change, which may inhibit counseling.29–31 Given this context, research assessing the extent to which residency training prepares primary care physicians to address patient obesity is warranted.
Previous reports show that only half of graduating primary care residents rate themselves as “very prepared” to counsel patients about diet and exercise.32,33 Few studies have looked into explaining this issue or identifying specific areas of need, such as knowledge deficit, poor attitudes, or low confidence.25,34–37 In addition, the literature is predominately focused on internal medicine,34–37 and most studies include only a small number of programs,25,34–37 raising concern about the ability to generalize from the findings. The purpose of this study is to assess the degree to which a statewide sample of senior family medicine (FM), internal medicine (IM), and obstetrics and gynecology (ob-gyn) residents are prepared to provide counseling on the topics of obesity, nutrition, and physical activity (ONPA). We assessed resident knowledge, attitudes, self-efficacy, and perceived professional role. We also examined demographic and training program characteristics potentially associated with variation in levels of preparedness.
Methods
Design
This study represents a cross-sectional survey of senior primary care residents across Ohio, encompassing FM and IM postgraduate year (PGY)-3 and ob-gyn PGY-3 and PGY-4 residents.
Sites and Recruitment
Using maximum variation sampling, 30 of the 54 FM, IM, and ob-gyn programs in Ohio were selected for recruitment based on diversity of specialty, program size, location (north coast, northeast, northwest, and central/southwest), and hospital affiliation. Programs were invited to participate via a letter mailed to the program director describing the purpose and scope of the study. Program enrollment and subsequent data collection scheduling were completed by the study coordinator through follow-up contacts by phone and/or e-mail. Program participation was incentivized by offering an educational presentation about evidence-based strategies for ONPA counseling.
Data Collection
Surveys were collected in person as part of the educational presentation, which was scheduled during a didactic session for residents at each residency site. Resident attendance was incentivized by offering a light lunch or snack during the session. The first 15 to 20 minutes of each session were allotted for survey completion. The study and participation were described, and an information sheet and a paper survey were distributed to each resident in attendance. Surveys were collected as completed, and the 45-minute presentation followed.
Resident participation was voluntary, and no identifying data were collected on the survey. However, a sign-in sheet was used so that senior residents unable to attend the session could be identified and offered the opportunity to participate. For these individuals, survey administration was completed by e-mailing a link to an electronic version of the survey. Residents who completed the electronic survey received a $5 Starbucks e-gift card. Additional recruitment strategies were used when resident participation rates were below 70%, including a $100 Visa gift card raffle, and the mailing of a paper survey with a postage-paid return envelope.
Measures
Demographic characteristics on the survey included sex, age, ethnicity, race, US citizenship, medical school location, and chief resident status. Residency program characteristics that were assessed included specialty, self-reported time spent in ambulatory practice, and exposure to an elective rotation emphasizing ONPA counseling. Program location and number of first-year positions available (used as an indicator of program size) were both obtained from an online directory.38
The indicators of counseling preparedness assessed included ONPA counseling knowledge and attitudes, self-efficacy, and perceived professional norms toward ONPA counseling. ONPA counseling knowledge was assessed by presenting 2 case studies with associated questions (15 items total), which is similar to the format of the United States Medical Licensing Examination and board examinations.39 Items focused on obesity risks and recommended assessment and treatment.12 A knowledge summary score was computed for each respondent by assigning a value of 1 to each correct response, totaling, and transforming to a 0 to 100 scale. Resident attitudes, self-efficacy, and perceived professional norms regarding ONPA counseling were assessed using 12-item, 9-item, and 10-item measures, respectively. Items for the attitudes and self-efficacy measures were adapted from scales identified in the literature.25,30,40 The professional norms measure was developed by the study team, guided by relevant theory and research.41–43 All items used a 5-point Likert response format (1, strongly disagree, to 5, strongly agree). Summary scores were created by totaling responses and dividing by the number of items completed, then transforming into 0 to 100 scales. Higher scores represented greater or more positive responses. All survey items were pilot tested with a sample of 25 FM, IM, and ob-gyn fellows. The final measures are provided as online supplemental material.
The University Hospitals Case Medical Center Institutional Review Board approved the study protocol.
Analyses
Data were stored using REDCap44 and analyzed using SPSS Statistics for Windows 2013 (IBM Corp). Descriptive statistics were used to summarize resident demographic and training program characteristics and ONPA summary scores; associations were examined using bivariate linear regressions. Generalized linear mixed models were used to compute adjusted P values for resident respondents clustered within programs. The study was powered with a target sample size of 24 programs, with an average of 8 residents per program, providing adequate power to detect differences between groups in the magnitude of 0.35 of a standard deviation. Statistical significance was evaluated at P < .05.
Results
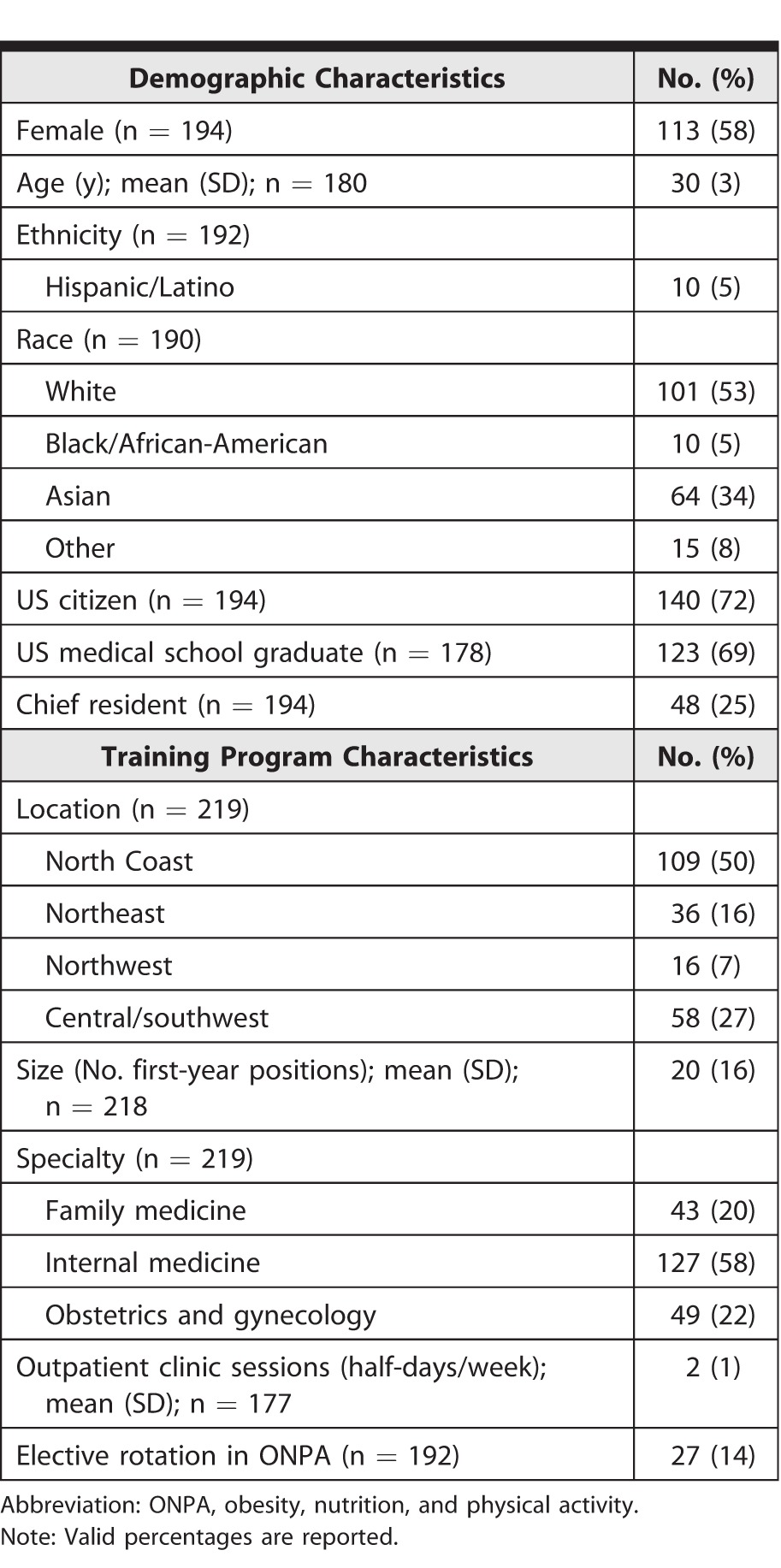
Of the 30 residency programs invited to participate, 25 (83%) completed data collection. A total of 219 senior residents completed the survey, representing a response rate of 62%. TABLE 1 shows the demographic and program characteristics of participating residents. Just over half of respondents were female (58%, 113 of 194), white (53%, 101 of 190), and training in IM (58%, 127 of 219). Few (14%, 27 of 192) reported completing an elective rotation involving significant instruction in ONPA counseling. As some participants did not complete every item, valid percentages are reported for all frequencies.
TABLE 1.
Characteristics of Participating Residents (N = 219)
Statistics for each ONPA counseling domain, including mean, minimum, and maximum scores and person and item reliability,45 are shown in TABLE 2. Mean ONPA counseling knowledge scores were low (50.8, SD = 15.6), with senior residents answering just over half of the items correctly. Scores for attitudes, self-efficacy, and professional norms toward ONPA counseling also were low, on average, with a wide range of scores observed across the sample.
TABLE 2.
Obesity, Nutrition, and Physical Activity (ONPA) Counseling Summary Scores (N = 219)
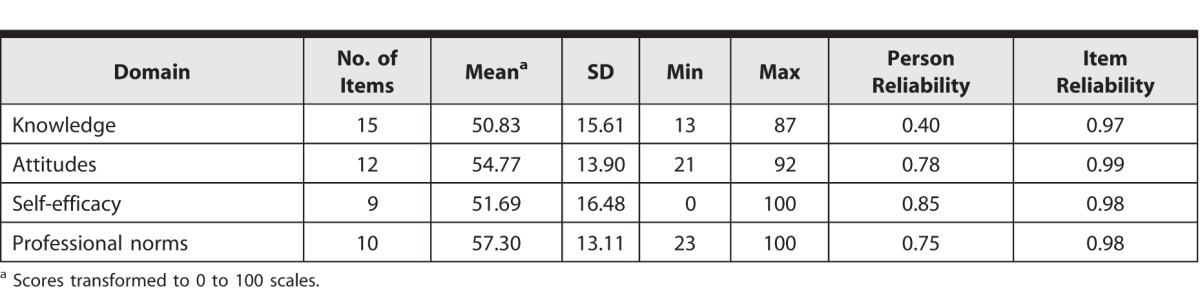
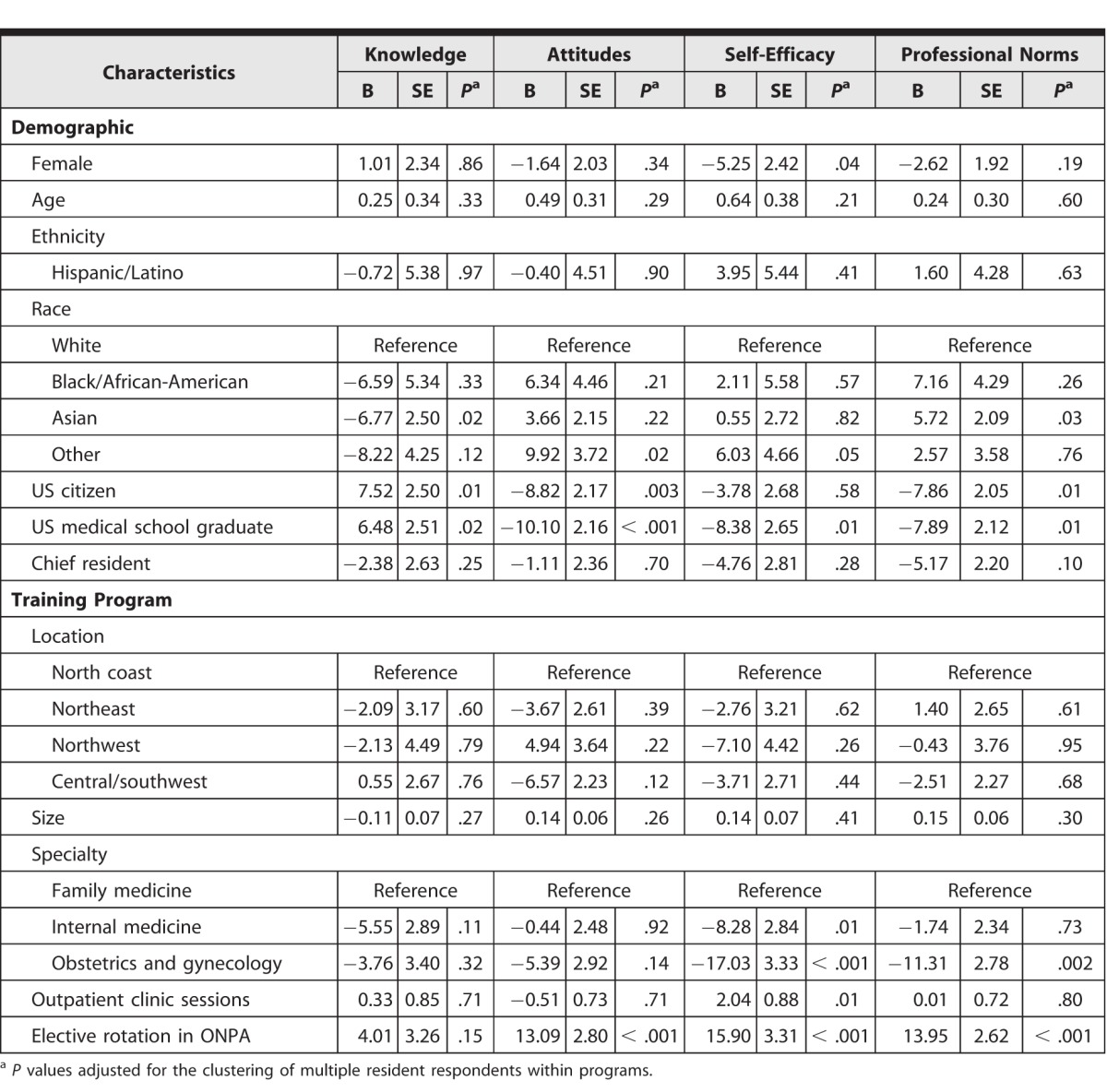
TABLE 3 shows associations between residents' ONPA scores and demographic and training program characteristics. ONPA counseling knowledge significantly varied by resident characteristics, with US citizens (B = 7.52, P = .01) and US medical school graduates (B = 6.48, P = .02) having higher scores with a magnitude of plus one-half standard deviation. However, these same characteristics were associated with significantly less positive attitudes and professional norms toward ONPA counseling. ONPA counseling self-efficacy varied by sex and location of medical school training, with female and US-trained residents reporting significantly lower self-efficacy. Scores for the 4 ONPA domains varied by race, but with no consistent trend. For program characteristics, specialty was associated with self-efficacy to provide counseling, with IM and ob-gyn residents significantly less confident providing ONPA counseling (B = −8.28 and B = −17.03, respectively) compared to FM residents. Residents training in ob-gyn also reported lower professional norms toward ONPA counseling compared to FM residents (B = −11.31, P = .002). Spending more time in an ambulatory practice location was associated with higher self-efficacy (B = 2.04, P = .01), but not knowledge, attitudes, or perceived norms toward counseling. Finally, residents reporting participation in an elective rotation that focused on ONPA had higher self-efficacy and more positive attitudes and professional norms scores (P < .001) with a magnitude of plus 1 standard deviation.
TABLE 3.
Associations Among Residents' Obesity, Nutrition, and Physical Activity (ONPA) Counseling Scores and Demographic and Training Program Characteristics (N = 219)
Discussion
Our results show that senior FM, IM, and ob-gyn residents in Ohio currently are ill-equipped to provide ONPA counseling. On average, residents answered half of the knowledge items incorrectly, indicating that knowledge of recommended obesity counseling guidelines and techniques is limited. Likewise, mean counseling self-efficacy was modest (52 out of 100), suggesting that residents do not feel confident in their ability to perform basic ONPA counseling tasks. These findings are consistent with previous studies showing low self-perceived ONPA counseling proficiency and a poor grasp of strategies to address obesity among IM residents.25,34–37 Studies examining barriers to weight management counseling in primary care practice also report inadequate training as a common barrier.24,26,28
We also assessed attitudes and professional norms toward ONPA counseling to explore the importance residents place on ONPA counseling and their perceptions regarding expectations and the importance placed on this area by their peers, preceptors, and professional societies. While no differences were observed in attitudes toward ONPA counseling across FM, IM, and ob-gyn, perception of professional norms were significantly lower in ob-gyn. This suggests that perceived barriers and challenges to addressing ONPA are similar across subspecialties; however, the perception of professional roles differ.
If primary care physicians are expected to address ONPA with their patients, training programs need to change. Examination of current curricula and critical reflection on the culture and attitudes maintained by program faculty and preceptors both are warranted. Efforts to increase instruction and experiential learning opportunities around ONPA and/or embed novelties of non-US predoctoral programs into US training should be explored to improve resident preparedness regarding ONPA counseling. This is considering the fact that international medical school graduates and residents who reported engagement in an elective rotation emphasizing ONPA showed greater counseling preparedness across domains.
Several study limitations deserve to be noted. First, we surveyed residents in a single state, and the generalizability of these findings may be limited to states and programs with similar characteristics. Second, despite multiple recruitment strategies and additional incentives, the response rate was modest. Residents with a greater interest in obesity care might have been more likely to participate, introducing the potential for participation bias and inflated scores. Third, the measures used in this study are new and have limited validity evidence. However, they were developed by drawing from the literature and were pilot tested. Finally, pediatrics residency programs were excluded from this study because we decided to focus on adult primary care trainees.
Conclusion
Primary care physicians see the majority of the population annually,5 and therefore have the opportunity to play a key role in addressing the American obesity epidemic by routinely counseling about obesity, nutrition, and physical activity during visits. Our findings show that significant gaps exist in primary care residents' preparedness to provide such counseling. Added training or an increased emphasis on ONPA is needed to enhance primary care physicians' skills to provide effective ONPA counseling and to prevent the health risks associated with obesity.
Supplementary Material
Footnotes
All authors are at Case Western Reserve University (CWRU). Samantha Smith, MA, is Data Manager, Department of Family Medicine & Community Health; Eileen L. Seeholzer, MD, MS, is Associate Professor, CWRU School of Medicine, and Department of Internal Medicine, MetroHealth Medical Center; Heidi Gullett, MD, MPH, is Assistant Professor, Department of Family Medicine & Community Health; Brigid Jackson, MA, is Project Coordinator, Department of Family Medicine & Community Health; Elizabeth Antognoli, PhD, MPH, is Research Associate, Department of Family Medicine & Community Health; Susan A. Krejci, MBA, is previous Project Coordinator, Department of Family Medicine & Community Health; and Susan A. Flocke, PhD, is Associate Professor, Department of Family Medicine & Community Health, Associate Director, Prevention Research Center for Healthy Neighborhoods, CWRU, and Director, Behavioral Measurement Core, Case Comprehensive Cancer Center.
Funding: This project was supported by a grant from the Centers for Disease Control and Prevention (grant No. CDC U48DP001930-SIP-12-053).
Conflict of interest: The authors declare they have no competing interests.
A preliminary version of these findings was presented as a poster at the 38th Annual Meeting of the American Society of Preventive Oncology in Arlington, Virginia, March 8–11, 2014.
The authors would like to thank the residency program faculty and resident physicians, who participated and made this study possible, and Drs Brandy Peaker, Eric Tai, and Jennifer Foltz from the US Centers for Disease Control and Prevention for their feedback on the survey and their comments on this manuscript.
This publication was supported by Cooperative Agreement Number 1-U48-DP-001930 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
References
- 1.Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health. 2009;9:88. doi: 10.1186/1471-2458-9-88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.US Department of Health and Human Services. The Surgeon General's Call to Action to Prevent and Decrease Overweight and Obesity. Rockville, MD: US Department of Health and Human Services, Public Health Service, Office of the Surgeon General; 2001. pp. 1–60. [PubMed] [Google Scholar]
- 3.National Task Force on the Prevention and Treatment of Obesity. Overweight, obesity, and health risk. Arch Intern Med. 2000;160(7):898–904. doi: 10.1001/archinte.160.7.898. [DOI] [PubMed] [Google Scholar]
- 4.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Center for Health Statistics. Health, United States, 2013: With Special Feature on Prescription Drugs. Hyattsville, MD: Centers for Disease Control and Prevention, Library of Congress Catalog No. 76-641496; 2014. [PubMed] [Google Scholar]
- 6.US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy people 2020: nutrition and weight status. 2015 https://www.healthypeople.gov/2020/topics-objectives/topic/nutrition-and-weight-status/objectives. Accessed April 13. [Google Scholar]
- 7.US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy people 2020: physical activity. 2015 https://www.healthypeople.gov/2020/topics-objectives/topic/physical-activity/objectives. Accessed April 13. [PubMed] [Google Scholar]
- 8.US Preventive Services Task Force. Screening for obesity in adults: recommendations and rationale. Ann Intern Med. 2003;139(11):930–932. doi: 10.7326/0003-4819-139-11-200312020-00012. [DOI] [PubMed] [Google Scholar]
- 9.Moyer VA. US Preventive Services Task Force. Screening for and management of obesity in adults: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(5):373–378. doi: 10.7326/0003-4819-157-5-201209040-00475. [DOI] [PubMed] [Google Scholar]
- 10.Nawaz H, Katz DL. American College of Preventive Medicine practice policy statement: weight management counseling of overweight adults. Am J Prev Med. 2001;21(1):73–78. doi: 10.1016/s0749-3797(01)00317-8. [DOI] [PubMed] [Google Scholar]
- 11.Jacobson DM, Strohecker L, Compton MT, Katz DL. Physical activity counseling in the adult primary care setting: position statement of the American College of Preventive Medicine. Am J Prev Med. 2005;29(2):158–162. doi: 10.1016/j.amepre.2005.04.009. [DOI] [PubMed] [Google Scholar]
- 12.National Institutes of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults—The Evidence Report. Bethesda, MD: National Heart, Lung, and Blood Institute; 1998. [Google Scholar]
- 13.Jensen MD, Ryan DH, Donato KA, Apovian CM, Ard JD, Comuzzie AG, et al. Special issue: guidelines (2013) for managing overweight and obesity in adults. Obesity. 2014;22(suppl 2):1–410. http://onlinelibrary.wiley.com/doi/10.1002/oby.v22.S2/issuetoc. Accessed May 17, 2015. [Google Scholar]
- 14.Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Obesity Society 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and The Obesity Society. J Am Coll Cardiol. J Am Coll Cardiol. 2014;2014;6363(25, pt B)(25, pt B):3029–3030. 2985–3023. doi: 10.1016/j.jacc.2013.11.004. [published correction appeared in. [DOI] [PubMed] [Google Scholar]
- 15.Rose SA, Poynter PS, Anderson JW, Noar SM, Conigliaro J. Physician weight loss advice and patient weight loss behavior change: a literature review and meta-analysis of survey data. Int J Obes (Lond) 2013;37(1):118–128. doi: 10.1038/ijo.2012.24. [DOI] [PubMed] [Google Scholar]
- 16.Leblanc ES, O'Conner E, Whitlock EP, Patnode CD, Kapka T. Effectiveness of primary care—relevant treatments for obesity in adults: a systematic evidence review for the US Preventive Services Task Force. Ann Intern Med. 2011;155(7):434–447. doi: 10.7326/0003-4819-155-7-201110040-00006. [DOI] [PubMed] [Google Scholar]
- 17.Dansinger ML, Tatsioni A, Wong JB, Chung M, Balk EM. Meta-analysis: the effect of dietary counseling for weight loss. Ann Intern Med. 2007;147(1):41–50. doi: 10.7326/0003-4819-147-1-200707030-00007. [DOI] [PubMed] [Google Scholar]
- 18.Scott JG, Cohen D, DiCicco-Bloom B, Orzano AJ, Gregory P, Flocke SA, et al. Speaking of weight: how patients and primary care clinicians initiate weight loss counseling. Prev Med. 2004;38(6):819–827. doi: 10.1016/j.ypmed.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 19.Kraschnewski JL, Sciamanna CN, Stuckey HL, Chuang CH, Lehman EB, Hwang KO, et al. A silent response to the obesity epidemic: decline in US physician weight counseling. Med Care. 2013;51(2):186–192. doi: 10.1097/MLR.0b013e3182726c33. [DOI] [PubMed] [Google Scholar]
- 20.Antognoli EL, Smith KJ, Mason MJ, Milliner BR, Davis EM, Harris-Haywood S, et al. Direct observation of weight counselling in primary care: alignment with clinical guidelines. Clin Obes. 2014;4(2):69–76. doi: 10.1111/cob.12050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Carroll JK, Antognoli E, Flocke SA. Evaluation of physical activity counseling in primary care using direct observation of the 5As. Ann Fam Med. 2011;9(5):416–422. doi: 10.1370/afm.1299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Flocke SA, Clark A, Schlessman K, Pomiecko G. Exercise, diet, and weight loss advice in the family medicine outpatient setting. Fam Med. 2005;37(6):415–421. [PubMed] [Google Scholar]
- 23.Smith AW, Borowski LA, Liu B, Galuska DA, Signore C, Klabunde C, et al. US primary care physicians' diet-, physical activity-, and weight-related care of adult patients. Am J Prev Med. 2011;41(1):33–42. doi: 10.1016/j.amepre.2011.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Huang J, Yu H, Marin E, Brock S, Carden D, Davis T. Physicians' weight loss counseling in two public hospital primary care clinics. Acad Med. 2004;79(2):156–161. doi: 10.1097/00001888-200402000-00012. [DOI] [PubMed] [Google Scholar]
- 25.Jay M, Gillespie C, Ark T, Richter R, McMacken M, Zabar S, et al. Do internists, pediatricians, and psychiatrists feel competent in obesity care?: using a needs assessment to drive curriculum design. J Gen Intern Med. 2008;23(7):1066–1070. doi: 10.1007/s11606-008-0519-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kolasa KM, Rickett K. Barriers to providing nutrition counseling cited by physicians: a survey of primary care practitioners. Nutr Clin Pract. 2010;25(5):502–509. doi: 10.1177/0884533610380057. [DOI] [PubMed] [Google Scholar]
- 27.Hébert ET, Caughy MO, Shuval K. Primary care providers' perceptions of physical activity counselling in a clinical setting: a systematic review. Br J Sports Med. 2012;46(9):625–631. doi: 10.1136/bjsports-2011-090734. [DOI] [PubMed] [Google Scholar]
- 28.Kushner RF. Barriers to providing nutrition counseling by physicians: a survey of primary care practitioners. Prev Med. 1995;24(6):546–552. doi: 10.1006/pmed.1995.1087. [DOI] [PubMed] [Google Scholar]
- 29.Puhl RM, Heuer CA. The stigma of obesity: a review and update. Obesity. 2009;17(5):941–964. doi: 10.1038/oby.2008.636. [DOI] [PubMed] [Google Scholar]
- 30.Foster GD, Wadden TA, Makris AP, Davidson D, Davidson D, Sanderson RS, et al. Primary care physicians' attitudes about obesity and its treatment. Obes Res. 2003;11(10):1168–1177. doi: 10.1038/oby.2003.161. [DOI] [PubMed] [Google Scholar]
- 31.Jay M, Kalet A, Ark T, McMacken M, Messito MJ, Richter R, et al. Physicians' attitudes about obesity and their associations with competency and specialty: a cross-sectional study. BMC Health Serv Res. 2009;9:106. doi: 10.1186/1472-6963-9-106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Blumenthal D, Gokhale M, Campbell EG, Weissman JS. Preparedness for clinical practice: reports of graduating residents at academic health centers. JAMA. 2001;286(9):1027–1034. doi: 10.1001/jama.286.9.1027. [DOI] [PubMed] [Google Scholar]
- 33.Park ER, Wolfe TJ, Gokhale M, Winickoff JP, Rigotti NA. Perceived preparedness to provide preventive counseling: reports of graduating primary care residents at academic health centers. J Gen Intern Med. 2005;20(5):386–391. doi: 10.1111/j.1525-1497.2005.0024.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tsui JI, Dodson K, Jacobson TA. Cardiovascular disease prevention counseling in residency: resident and attending physician attitudes and practices. J Natl Med Assoc. 2004;96(8):1080–1083. [PMC free article] [PubMed] [Google Scholar]
- 35.Vetter ML, Herring SJ, Sood M, Shah NR, Kalet AL. What do resident physicians know about nutrition? An evaluation of attitudes, self-perceived proficiency and knowledge. J Am Coll Nutr. 2008;27(2):287–298. doi: 10.1080/07315724.2008.10719702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Block JP, DeSalvo KB, Fisher WP. Are physicians equipped to address the obesity epidemic? Knowledge and attitudes of internal medicine residents. Prev Med. 2003;36(6):669–675. doi: 10.1016/s0091-7435(03)00055-0. [DOI] [PubMed] [Google Scholar]
- 37.Davis NJ, Shishodia H, Taqui B, Dumfeh C, Wylie-Rosett J. Resident physician attitudes and competence about obesity treatment: need for improved education. Med Educ Online. 2008;13:5. doi: 10.3885/meo.2008.Res00257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.American Medical Association. Fellowship and Residency Electronic Interactive Database (FREIDA Online) 2015 http://www.ama-assn.org/ama/pub/education-careers/graduate-medical-education/freida-online.page. Accessed April 13. [Google Scholar]
- 39.Tallia AF, Scherger JE, Dickey NW. Swanson's Family Medicine Review: A Problem-Oriented Approach. 7th ed. Philadelphia, PA: Elsevier Inc; 2013. Diet, exercise, and obesity; pp. 38–43. In. [Google Scholar]
- 40.Epling JW, Morley CP, Ploutz-Snyder R. Family physician attitudes in managing obesity: a cross-sectional survey study. BMC Res Notes. 2011;4(1):473. doi: 10.1186/1756-0500-4-473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ajzen I, Fishbein M. Understanding Attitudes and Predicting Social Behavior. Englewood Cliffs, NJ: Prentice-Hall; 1980. [Google Scholar]
- 42.Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. [Google Scholar]
- 43.Surdyk PM, Lynch DC, Leach DC. Professionalism: identifying current themes. Curr Opin Anaesthesiol. 2003;16(6):597–602. doi: 10.1097/00001503-200312000-00005. [DOI] [PubMed] [Google Scholar]
- 44.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bond TG, Fox CM. Applying the Rasch Model: Fundamental Measurement in the Human Sciences. 1st ed. Mahwah, NJ: Lawrence Erlbaum Associates Inc; 2001. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.