

Abstract
Background:
Fatigue is the most common side effect of chemotherapy in children with acute lymphoblastic leukemia (ALL). Acupressure is one of the most popular non-pharmacologic methods used to reduce fatigue in other settings. The aim of the study was to evaluate the effect of acupressure on reducing fatigue among children with ALL compared with a placebo treatment.
Materials and Methods:
In a single-blind, randomized, placebo-controlled clinical trial of 120 hospitalized school-aged children with ALL, 24 h after chemotherapy, they were randomly divided into experimental (n = 60) and placebo groups (n = 60). Intensity of fatigue was rated using the Visual Analog Scale. The intervention (finger acupressure) was applied on ST36 (true points) in the experimental group and on LI12 (sham points) in the placebo group. We evaluated the symptoms of fatigue intensity immediately and 1 h after intervention. Fatigue was also measured 24 h after intervention by Fatigue Scale-Child (FS-C). Data were analyzed by SPSS version 16.0 using descriptive statistics, independent t-test, and Chi-square and Fisher exact tests.
Results:
Significant differences were observed between the two groups in the intensity of fatigue 1 h after intervention (P < 0.001). But there was no significant difference between them regarding fatigue 24 h after intervention.
Conclusions:
Applying one time acupressure may reduce the intensity of fatigue at 1 h post-treatment. Therefore, acupressure could be recommended as an effective, non-pharmacologic method for some CRF control. Applying one time acupressure did not have a long-term effect.
Keywords: Acupressure, acute lymphoblastic leukemia, chemotherapy, fatigue
INTRODUCTION
Acute lymphoblastic leukemia (ALL) is one of the most common cancers in children and adolescents and accounts for 75–80% of childhood leukemia.[1] According to a research done in 2011, there were 1.9 billion children forming 27% of the world population,[2] and about 20–50 million children and adolescents are diagnosed with leukemia every year.[3] With the improvement in cancer treatment, children with leukemia have an enhanced survival rate nowadays. However, this has increased the number and severity of side effects and unpleasant symptoms, for instance, fatigue, pain, mucositis, nutritional concerns, nausea, and vomiting.[4] Fatigue is a pervasive, distressing, and weakening symptom that has an extreme negative impact on daily activity, involvement in social activities, maintenance of interpersonal relationships, quality of life, and personal well-being.[5,6,7] Unlike other cancer symptoms that may disappear when the treatment is completed, fatigue has a persistent and lasting effect on children and adolescents undergoing cancer treatment.[8]
Pediatric patients with ALL who require chemotherapy often report the symptom of fatigue as one of the most prevalent illness-related effects that they experience during treatment.[9] Fatigue is a side effect of chemotherapy and is experienced by the affected children, so it has to be managed by pharmacologic and non-pharmacologic approaches.[10]
In studies on adults, fatigue has been reported as a multidimensional symptom including physical, psychological, and emotional aspects.[11] In two longitudinal studies in which pediatric oncology patients rated 10 treatment-related symptoms for symptom distress, fatigue was rated as the most distressing and a common clinical problem during cancer treatment.[12] Fatigue is reported to be more upsetting and troublesome for performing daily activities than, for example, cancer-related pain.[13,14]
About 40% of cancer patients may experience fatigue even years after they complete treatment.[15,16] Various complementary and alternative therapies are often used to manage the side effects and symptoms from cancer treatments, including fatigue.[17] Some preliminary evidence indicates that acupressure (the non-invasive form of acupuncture) was helpful in relieving fatigue in chronic obstructive pulmonary disease (COPD) patients attending a pulmonary rehabilitation program.[18] Moreover, acupressure and transcutaneous electrical acupoint stimulation were found effective in relieving fatigue, sleep problems, and depression in a sample of 106 patients undergoing hemodialysis.[19,20] However, a strong placebo effect was noted in the study, as the sham acupressure group also improved significantly. Recently, a Phase II uncontrolled trial (N = 37) of acupuncture treatment in cancer patients at least 3 weeks after chemotherapy found that acupuncture improved fatigue by 31.1%.[14] In another study, one cohort received twice-weekly acupuncture treatment for 4 weeks (n = 25) and another cohort received treatment once a week for 6 weeks (n = 12), but the difference in the two schedules of treatment was minimal.[21] However, the non-invasive form of acupuncture, acupressure, has received little attention in oncology, although it has been in use in some places for more than 2000 years. Acupressure involves using pressure instead of needles applied to the same points, but is safer, less expensive, and patients can easily learn to apply pressure on their own. Acupressure is a technique derived from acupuncture, a component of Traditional Chinese Medicine (TCM). Acupressure involves pressure with fingers or bands on the body's acupoints and is simple to perform, painless, inexpensive, and effective.[22] The practice of acupressure is derived from a philosophy of balance and unity between the universe, living beings, and energy flow. Chernyak and Sessler reported that any imbalance, disruption, or energy flow blockage within the body can cause disease or pain. The aim of acupoint stimulation is to return the body to a harmonized, balanced condition.[23] During acupressure, physical force is applied to acupuncture points by hand, elbow, or with various devices, in an attempt to treat disease and reduce symptoms. Acupressure has demonstrated optimistic effects on sleep quality,[24,25] sleep quantity,[26,27] and depression[28] in cancer patients and other chronically ill populations. Pilot clinical trials have also demonstrated that acupressure and acupuncture can significantly reduce persistent cancer fatigue by as much as 38%.[29] The Joksamly or ST36 located at 4-finger breadths below the knee depression lateral to the tibia [Figure 1].
Figure 1.

ST36 (Joksamly)
Although in many Western countries cancer-related fatigue in both adults and children has received attention as an important issue and has been studied widely, unfortunately, it has not received enough attention in comparison with pain, nausea, and vomiting management by healthcare professionals and researchers in Iran. No studies could be identified on whether cancer-related fatigue is a common tolerable or distressing symptom among Iranian pediatric oncology patients nor have the coping mechanisms for dealing with the unique fatigue syndrome among these children been methodically studied.
Patients with cancer and their families may not report fatigue to clinicians because they might think fatigue or being “tired” is a predictable cancer-related symptom, and that they must tolerate and deal with fatigue and reduce their expectations for symptom relief. Consequently, cancer-related fatigue is persistently ignored, under-diagnosed, and not treated in Iran.
The aim of the study was to examine the effectiveness of acupressure in the relief of cancer related fatigue (CRF) in pediatric cancer patients after they undergo chemotherapy. Therefore, this study was carried out to investigate the effect of acupressure on CRF in school-aged children being treated for ALL.
MATERIALS AND METHODS
This is a single-blind, randomized controlled clinical trial, wherein 120 children with ALL between the ages of 8 and 12 were recruited, and they were randomly divided into experimental and placebo groups. After completing a demographic form, baseline intensity of fatigue was measured using the Visual Analog Scale (VAS) before the intervention. Ethical considerations, such as informed consent and confidentiality, were adequately addressed, and approval of a Research and Ethics Committee was obtained. Also, providing the research results for both experimental and placebo groups was considered and the researcher's email address was available for both groups to be informed of the results.
On the second day of chemotherapy, the intervention (finger acupressure) was applied for 3 min on ST36 (true points) in the experimental group and on LI12 (sham points) in the placebo group.
Given that in the present study patients with leukemia undergoing chemotherapy were selected, who also suffered from cancer-related fatigue, applying acupressure on various acupoints could be frustrating for the patients. Regarding ethical considerations in this research and according to the results of a previous study that was performed to relieve cancer-related fatigue, ST36 was chosen as the acupressure point and LI12 as the sham point. LI12 is not associated with energy in the TCM and was also used as the sham point in a previous study.[13] In addition, applying acupressure on one point is easy to learn for patients and their family members. Thus, patients and their family members can do this intervention at home to get relieved of cancer-related fatigue.
We evaluated fatigue intensity using VAS immediately and 1 h after the intervention. Fatigue was again measured 24 h after the intervention by the instrument of Fatigue Scale-Child (FS-C). Routine care was administered to both the groups.
Patients were recruited from an oncology unit of two pediatric educational hospitals in Tehran. Inclusion criteria were ALL diagnosis, willing to participate in the study and to be randomized in one of the two groups, age 8–12 years, no prior experience of chemotherapy, no prior experience of acupressure, and anticipated survival more than 3 months.
Patients were excluded if they had low platelet count (<50,000), suffered from a bleeding disorder (e.g. hemophilia), had hemoglobin levels less than 9 g/dl and hematocrit less than 30, or were on active treatment for anemia (i.e., Erythropoietin (EPO) or blood transfusions).
Patients were matched by age and sex and then randomized to the experimental and placebo groups.
Fatigue assessments were designed to measure fatigue along multiple dimensions.
The VAS uses a 100-mm device (0–10) with the extreme left side indicating zero fatigue and the extreme right side indicating maximal fatigue (“worst imaginable fatigue”). The patient indicates fatigue intensity by moving a pointer on the device, yielding a score measured by the pointer location. Patients were familiarized with the VAS device on the first day of hospitalization. The FS-C is a 10-item, self-report instrument that measures cancer-related fatigue and provides a fatigue intensity score. Each item has a 5-point Likert-type format; total scale intensity ratings range from 0 (no fatigue symptoms) to 50 (highest possible fatigue score). The 10-item version of the FS-C achieved a Cronbach alpha of 0.76, whereas the standard FS-C achieved a Cronbach alpha of 0.81. The 10-item FS-C consists of items that discriminate between children who have high cancer-related fatigue and those who do not.[9]
On the second day of chemotherapy, patients in the experimental group received 3 min finger acupressure on point ST36, a point traditionally used for “energy,”[14] located below the knee in the anterior border of tibia. The control group instead received pressure on a point not associated with “energy” in TCM, i.e. LI12 located on the lateral side of the upper arm, with the elbow flexed, on the tile border of humerus [Figure 2].[15] Patients in both acupressure groups were told that the effects of two sets of points were tested, but they were not aware that one set was a sham technique.
Figure 2.
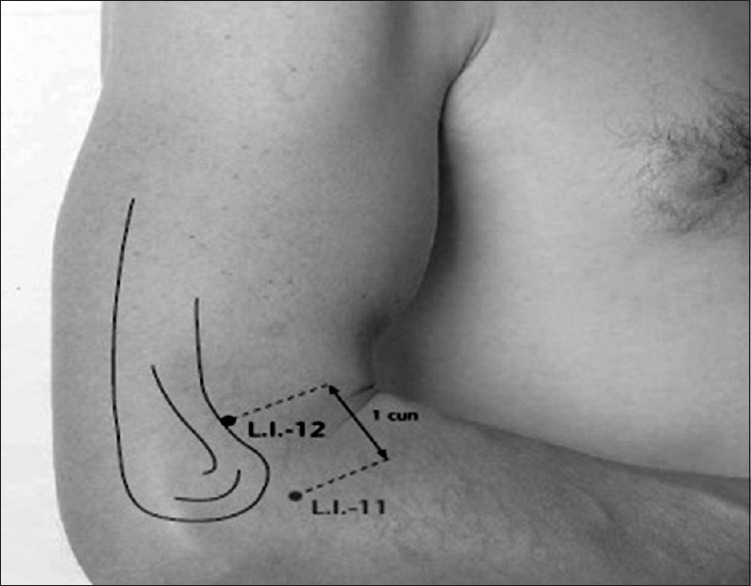
LI12 (Zohoulia)
The study was reviewed and approved by the Research and Ethics Committee of Tehran University of Medical Sciences and Health Services (code: 1744263). Participants and their parents were given verbal and written information about the aim and procedure of the study, the right to withdraw at any time, and the promise to maintain confidentiality by the researchers. They also promised to keep the confidentiality for other participants. Verbal assent from children and adolescents was required for study participation, while the consent forms were signed by their parents. At the end of the study and for ethical reasons, all patients in the sham acupressure group were contacted, presented with the findings of the study, and taught how to locate and press the more effective points. All the patients in the study were receiving routine care. But they did not receive any intervention to reduce cancer-related fatigue.
Data were coded and entered into SPSS (version 16) for statistical analysis. Descriptive statistics were calculated with all demographic and clinical data and fatigue subscale scores. Chi-square and Fisher exact tests were also used to test any differences in demographic data between the two groups. Repeated measures analysis of variance (R-ANOVA) was used to identify any differences in fatigue intensity between the three different time periods (before, immediately, and 1 h after intervention). Ninety-five percent confidence intervals were obtained from t-tests between the two groups.
RESULTS
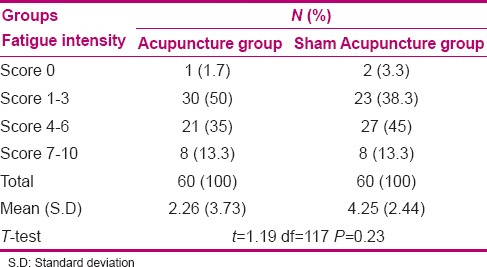
One hundred and twenty children were enrolled in this randomized, controlled trail. No differences between the two groups were found in any of the demographic or other baseline variables. Mean age of the children in both experimental and placebo groups was 9.98 ± 1.55 years. The mean and Standard Deviation of the ages of both groups was identical. To ensure homogeneity between the groups, subjects in the experimental and placebo groups were matched for age. Girls accounted for 31.7% and boys formed 68.3% of the subjects. The children's companion in the hospital was their mother in 63.3% of the experimental group and 65% of the placebo group; there was no significant difference between the two groups in this regard (P = 0.27). Parents’ education and job was not significantly different between the two groups (P < 0.05). Fatigue intensity before intervention was measured in both groups (3.73 ± 2.26 in the experimental group and 4.25 ± 2.44 in the placebo group); the results showed that they were not significantly different (P = 0.23).
Fatigue intensity of the two groups was compared immediately after intervention, but indicated no significant difference between them (P = 0.07) [Table 1]. Most subjects in both groups experienced mild fatigue (score 1–3); so, it would be expected that applying one time acupressure would not reduce fatigue intensity immediately after intervention. There was also significant difference regarding fatigue between the two groups 1 h after intervention (P ≤ 0.001) [Table 2], but not after 24 h (P = 0.82) [Table 3]. Fatigue intensity before intervention was measured in both groups; the results showed that they were not significantly different (P = 0.23) [Table 4]. Regarding fatigue intensity, there was significant difference between before and immediately after intervention and also between before and 1 h after intervention in the experimental group (P < 0.001). In the placebo group, there were significant differences of fatigue intensity between before and immediately after intervention and also between immediately and 1 h after intervention (P < 0.001). Finally, no significant differences were found between the two groups regarding the variables of fatigue 24 h post-intervention. So, in the present study, applying one time acupressure through one point was not found to be effective after 24 h.
Table 1.
Comparison of fatigue intensity in ALL children of the two groups immediately after intervention
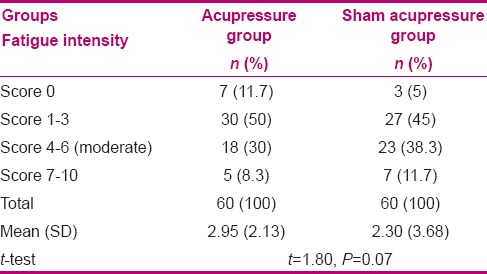
Table 2.
Comparison of fatigue intensity in ALL children of the two groups 1 h after intervention
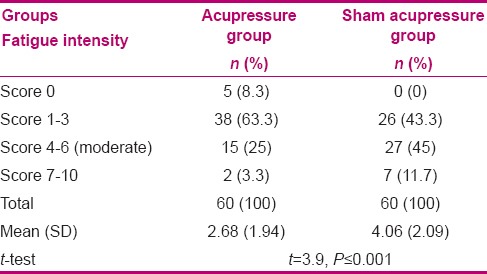
Table 3.
Comparison of fatigue in ALL children of the two groups 24 h after intervention
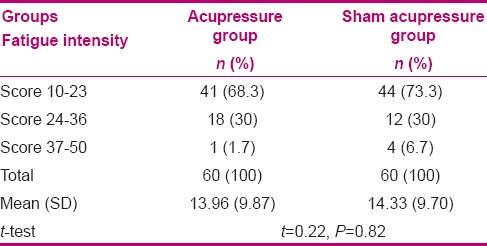
Table 4.
The compression of fatigue intensity in ALL children before intervention in tow groups
DISCUSSION
Acupressure caused greater reduction in fatigue when compared to the placebo group. Regarding the severity of fatigue in subjects 1 h after intervention [Table 3], the independent t-test indicated that it was significantly different between the experimental and placebo groups (P ≤ 0.0001). Therefore, it may be inferred that applying pressure on the right points at the right time can determine the efficacy of acupressure.[27] Stimulation of ST36 may improve the flow of Chi[29] or increase the release of neurotransmitters and neurohormone,[13] and thus reduces the perception of fatigue.
Zick et al. reported that acupressure can manage fatigue. Acupressure has a positive effect of sleep quality, sleep quantity, and depression in cancer patients and those with other chronic diseases. Studies show that acupressure and acupuncture reduce up to 38% of cancer-related fatigue.[13]
Acupressure techniques are non-invasive, safe, and effective. They can be easily taught to patients so that they themselves can manage fatigue and reduce the adverse health outcome to improve their quality of life.[29,30] This study suggests that acupressure could improve fatigue 1 h after intervention. Molassiotis et al. studied the effect of acupressure on alleviating cancer-related fatigue. Forty-seven adults with cancer who experienced moderate to severe fatigue were selected. They underwent acupressure on ST36 for 2 weeks. At the end of intervention, the case group had 19% improvement in fatigue while the control group had 0.6% improvement.[13] The present study used point ST36 to apply acupressure, similar to that in the study of Molassiotis.
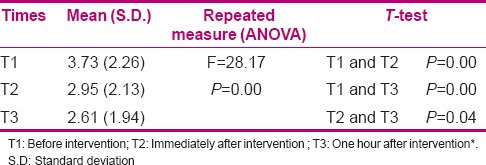
On comparing the severity of fatigue in subjects before, immediately after, and 1 h after acupressure, paired t-tests showed significant differences in the experimental group before and immediately after, and before and 1 h after intervention (P < 0.001). The mean severity of fatigue in the experimental group before intervention was 3.73, but dropped to 2.95 and 2.61 immediately after and 1 h after intervention, respectively. This reduction in severity of fatigue before and immediately after the intervention, and before and 1 h after intervention was significantly different in the experimental group (P ≤ 0.001) [Table 5].
Table 5.
Fatigue intensity over time in Acupuncture group
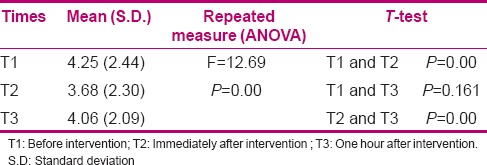
However, as can be seen in Table 6, 1 h after intervention, mean severity of fatigue increased in the placebo group, which shows that the placebo effect did not work and patients’ perception of fatigue increased. The results show that children's severity of fatigue was 4.25 before intervention, but decreased to 3.68 immediately after intervention and increased to 4.06 at 1 h after intervention. A repeated measure ANOVA for the placebo group shows that there was significant difference between before and immediately after intervention and also between immediately after and 1 h after intervention (P ≥ 0.001); although there was some improvement in the sham acupressure group, the improvement was greater in the acupressure group. Acupressure on non-acupoints may produce some effects on fatigue. This may be the result of physiological and psychological effects of the massage itself.[13] Apparently, patients are aware that they are receiving treatment on acupoints or non-acupoint and are more likely to experience positive outcomes because of their expectations.
Table 6.
Fatigue intensity over time in Sham Acupuncture group
Subjects in the sham acupressure group and acupressure group showed improvement in the VAS fatigue score immediately after intervention. Massaging the acupoint or non-acupoint itself may produce various levels of relaxation on the body and, thus, produce different effects on fatigue.[13]
No evidence has been published regarding the effect of acupressure on fatigue caused due to treatment of cancer patients at time intervals before, immediately after, and 1 h after intervention, to be compared with our findings. However, Tsay evaluated the efficacy of acupressure on fatigue among end-stage renal disease patients in which 3-min treatments, real and sham acupressure, were applied to the case and control groups, and they found that fatigue significantly improved in those receiving the real treatment.[20]
Considering these results, we can infer that the effect of acupressure in reducing fatigue immediately after intervention can be attributed to the placebo effect in this group. It is reported that sometimes placebo groups show the efficacy of acupressure. For instance, Agarwel et al. (2005) reported that anxiety before surgery reduced significantly immediately after applying acupressure on a sham point in the placebo group (P <0.001). They mentioned the effect of massaging, and that the feeling of patients that some special intervention is being used to their benefit is the reason for this effect.[31] Two theories about the effect of acupressure on sham points may be relevant here. First, acupressure on sham points is sometimes genuinely effective. Second, subjects’ expectation about the efficacy of intervention may be affected simply by the presence of the researcher as a member of therapy team (Hawthorn effect).[32,33]
On comparing the severity of fatigue in subjects 24 h post-intervention, most subjects in both the experimental group (68.3%) and the placebo group (73.3%) had fatigue scores of 10–23, making it difficult to evaluate the residual effects after 24 h. To determine whether acupressure at shorter intervals and more frequently would reduce fatigue, more extensive study needs to be performed. Although Vickers et al. reported the efficiency of acupuncture on chemotherapy-related fatigue, the study design and treatment type (acupuncture vs. acupressure) may explain the differences in results.[27]
ACKNOWLEDGMENT
The participants of the study are gratefully acknowledged. This research was supported by funds from Tehran University of Medical Sciences and Health Services. This article was derived from a master thesis of Maryam Khosravi with project number (IRCT138807152556N1) Isfahan University of Medical Sciences, Isfahan, Iran.
Footnotes
Source of Support: Tehran University of Medical Sciences and Health Services
Conflict of Interest: None declared.
REFERENCES
- 1.Redaelli A, Laskin BL, Stephens JM, Botteman MF, Pashos CL. A systematic literature review of the clinical and epidemiological burden of acute lymphoblastic leukaemia (ALL) Eur J Cancer Care (Engl) 2005;14:53–62. doi: 10.1111/j.1365-2354.2005.00513.x. [DOI] [PubMed] [Google Scholar]
- 2.United Nations, Department of Economic and Social Affairs, Population Division. 2011. [Last accessed on 2011 May 4]. Available from: http://www.esaun.org/unpd/wpp/unpp/p2k0data.asp/
- 3.He JR, Ye TZ, Ma JX. Current status of research on the epidemiology of children with leukemia. IJ BTI. 2005;3:61–4. [Google Scholar]
- 4.Hockenberry M. Symptom management research in children with cancer. J Pediatr Oncol Nurs. 2004;21:132–6. doi: 10.1177/1043454204264387. [DOI] [PubMed] [Google Scholar]
- 5.Gedaly-Duff V, Lee KA, Nail L, Nicholson HS, Johnson KP. Pain, sleep disturbance, and fatigue in children with leukemia and their parents: A pilot study. Oncol Nurs Forum. 2006;33:641–6. doi: 10.1188/06.ONF.641-646. [DOI] [PubMed] [Google Scholar]
- 6.Langeveld N, Ubbink M, Smets E. ‘I don’t have any energy’: The experience of fatigue in young adult survivors of childhood cancer. Eur J Oncol Nurs. 2000;4:20–8. doi: 10.1054/ejon.1999.0063. [DOI] [PubMed] [Google Scholar]
- 7.Meeske K, Katz ER, Palmer SN, Burwinkle T, Varni JW. Parent proxy-reported health-related quality of life and fatigue in pediatric patients diagnosed with brain tumors and acute lymphoblastic leukemia. Cancer. 2004;101:2116–25. doi: 10.1002/cncr.20609. [DOI] [PubMed] [Google Scholar]
- 8.Wu M, Hsu L, Zhang B, Shen N, Lu H, Li S. The experiences of cancer-related fatigue among Chinese children with leukaemia: A phenomenological study. Int J Nurs Stud. 2010;47:49–59. doi: 10.1016/j.ijnurstu.2009.05.026. [DOI] [PubMed] [Google Scholar]
- 9.Hinds PS, Yang J, Gattuso JS, Hockenberry M, Jones H, Zupanec S, et al. Psychometric and clinical assessment of the 10-item reduced version of the Fatigue Scale-Child instrument. J Pain Symptom Manage. 2010;39:572–8. doi: 10.1016/j.jpainsymman.2009.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hockenberry MJ, Hinds PS, Barrera P, Bryant R, Adams-McNeill J, Hooke C, et al. Three instruments to assess fatigue in children with cancer: The child, parent and staff perspectives. J Pain Symptom Manage. 2003;25:319–28. doi: 10.1016/s0885-3924(02)00680-2. [DOI] [PubMed] [Google Scholar]
- 11.Holley SK. Evaluating patient distress from cancer-related fatigue: An instrument development study. Oncol Nurs Forum. 2000;27:1425–31. [PubMed] [Google Scholar]
- 12.Hinds P, Scholes S, Gattuso J, Riggins M, Heffner B. Adaptation to illness in adolescents with cancer. J Pediatr Oncol Nurs. 1990;7:64–5. doi: 10.1177/104345429000700214. [DOI] [PubMed] [Google Scholar]
- 13.Molassiotis A, Sylt P, Diggins H. The management of cancer-related fatigue after chemotherapy with acupuncture and acupressure: A randomised controlled trial. Complement Ther Med. 2007;15:228–37. doi: 10.1016/j.ctim.2006.09.009. [DOI] [PubMed] [Google Scholar]
- 14.Molassiotis A, Chan CW. Fatigue patterns in Chinese patients receiving radiotherapy. Eur J Oncol Nurs. 2004;8:334–40. doi: 10.1016/j.ejon.2003.12.009. [DOI] [PubMed] [Google Scholar]
- 15.Aird M, Cobbin DM, Rogers C. A study of the relative precision of acupoint location methods. J Altern Complement Med. 2002;8:635–42. doi: 10.1089/107555302320825156. [DOI] [PubMed] [Google Scholar]
- 16.Servaes P, Verhagen S, Bleijenberg G. Determinants of chronic fatigue in disease-free breast cancer patients: A cross-sectional study. Ann Oncol. 2002;13:589–98. doi: 10.1093/annonc/mdf082. [DOI] [PubMed] [Google Scholar]
- 17.Bower JE, Ganz PA, Desmond KA, Bernaards C, Rowland JH, Meyerowitz BE, et al. Fatigue in long-term breast carcinoma survivors: A longitudinal investigation. Cancer. 2006;106:751–8. doi: 10.1002/cncr.21671. [DOI] [PubMed] [Google Scholar]
- 18.Molassiotis A, Fernadez-Ortega P, Pud D, Ozden G, Scott JA, Panteli V, et al. Use of complementary and alternative medicine in cancer patients: A European survey. Ann Oncol. 2005;16:655–63. doi: 10.1093/annonc/mdi110. [DOI] [PubMed] [Google Scholar]
- 19.Maa SH, Gauthier D, Turner M. Acupressure as an adjunct to a pulmonary rehabilitation program. J Cardiopulm Rehabil. 1997;17:268–76. doi: 10.1097/00008483-199707000-00008. [DOI] [PubMed] [Google Scholar]
- 20.Tsay SL. Acupressure and fatigue in patients with end-stage renal disease-a randomized controlled trial. Int J Nurs Stud. 2004;41:99–106. doi: 10.1016/s0020-7489(03)00079-8. [DOI] [PubMed] [Google Scholar]
- 21.Montazeri A. Health-related quality of life in breast cancer patients: A bibliographic review of the literature from 1974 to 2007. J Exp Clin Cancer Res. 2008;27:32. doi: 10.1186/1756-9966-27-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sheahan P, O’leary G, Lee G, Fitzgibbon J. Cystic cervical metastases: Incidence and diagnosis using fine needle aspiration biopsy. Otolaryngol Head Neck Surg. 2002;127:294–8. doi: 10.1067/mhn.2002.128600. [DOI] [PubMed] [Google Scholar]
- 23.Shin YH, Kim TI, Shin MS, Juon HS. Effect of acupressure on nausea and vomiting during chemotherapy cycle for Korean postoperative stomach cancer patients. Cancer Nurs. 2004;27:267–74. doi: 10.1097/00002820-200407000-00002. [DOI] [PubMed] [Google Scholar]
- 24.Chernyak GV, Sessler DI. Perioperative acupuncture and related techniques. Anesthesiology. 2005;102:1031. doi: 10.1097/00000542-200505000-00024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cerrone R, Giani L, Galbiati B, Messina G, Casiraghi M, Proserpio E, et al. Efficacy of HT 7 point acupressure stimulation in the treatment of insomnia in cancer patients and in patients suffering from disorders other than cancer. Minerva Medica. 2008;99:535–7. [PubMed] [Google Scholar]
- 26.Tsay SL, Chen ML. Acupressure and quality of sleep in patients with end-stage renal disease-a randomized controlled trial. Int J Nurs Stud. 2003;40:1–7. doi: 10.1016/s0020-7489(02)00019-6. [DOI] [PubMed] [Google Scholar]
- 27.Vickers AJ, Straus DJ, Fearon B, Cassileth BR. Acupuncture for postchemotherapy fatigue: A phase II study. J Clin Oncol. 2004;22:1731–5. doi: 10.1200/JCO.2004.04.102. [DOI] [PubMed] [Google Scholar]
- 28.Dundee JW, Ghaly RG. Dose the timing of P6 acupuncture influence its efficacy as a postoperative anti-emetic. Br J Anaestha. 1989;63:630. [Google Scholar]
- 29.Zick SM, Alrawi S, Merel G, Burris B, Sen A, Litzinger A, et al. Relaxation acupressure reduces persistent cancer-related fatigue. Evid Based Complement Alternat Med 2011. 2011 doi: 10.1155/2011/142913. pii: 142913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Birch SJ, Felt RL. Brookline, MA: Publication; 1999. Understanding Acupressure Paradigm. [Google Scholar]
- 31.Agarwal A, Ranjan R, Dhiraaj S, Lakra A, Kumar M, Singh U. Acupressure for prevention of pre-operative anxiety: A prospective, randomised, placebo controlled study. Anaesthesia. 2005;60(10):978–81. doi: 10.1111/j.1365-2044.2005.04332.x. [DOI] [PubMed] [Google Scholar]
- 32.Wu B, Zhou RX, Zhou MS. Effect of acupuncture on interleukin-2 level and NK cell immunoactivity of peripheral blood of malignant tumor patients. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1994;14:537–9. [PubMed] [Google Scholar]
- 33.Goats GC. Massage-the scientific basis of an ancient art: Part 2. Physiological and therapeutic effects. Br J Sports Med. 1994;28:153–6. doi: 10.1136/bjsm.28.3.153. [DOI] [PMC free article] [PubMed] [Google Scholar]