

Abstract
Background:
Chronic renal disease and hemodialysis cause numerous psychological, social, cultural, and spiritual challenges for both patients and their families. Overcoming these challenges is possible only through providing holistic support for the patients. Today, despite the support provided by family and professional caregivers for the patients, patients still express dissatisfaction with the support provided and believe it to be inadequate. In fact, patients and family caregivers and healthcare practitioners seem to have different understandings of the notion of support. Thus, the researcher decided to examine the concept of support from the viewpoint of hemodialysis patients.
Materials and Methods:
This descriptive phenomenological research was conducted on 17 patients with end-stage renal disease (ESRD) who were undergoing hemodialysis. Purposive sampling was performed and continued until data saturation. Data were collected through 30–60 min unstructured interviews and analyzed using Colaizzi's method.
Results:
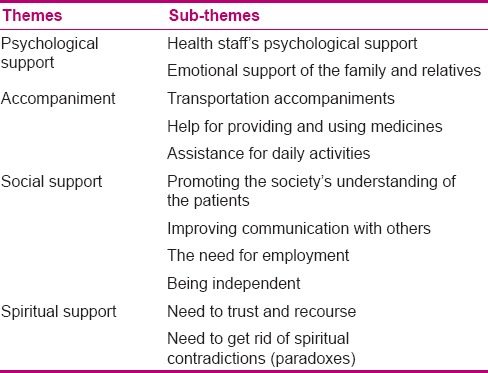
From the analysis of data, 4 themes (psychological support, accompaniment, social support, and spiritual support) and 11 sub-themes were obtained. Psychological support consisted of two sub-themes of psychological support by healthcare practitioners and emotional support by family and relatives. Accompaniment included three sub-themes of assistance in transportation, providing and using medicine, and daily activities. Social support was identified with four sub-themes of promotion of the society's understanding of the patients’ condition, improvement of communication with others, the need for employment, and independence. Spiritual support was identified with two sub-themes of the need for faith and trust in God or Imams and the need to resolve spiritual contradictions.
Conclusion:
The results showed that from the viewpoint of the participants, the concept of support consisted of psychological support, social support, accompanying the patient, and spiritual support. Hence, it can be concluded that this concept should be considered in healthcare planning, in order to improve the health and quality of life of these patients and their adaptation to the disease and its treatment process.
Keywords: Hemodialysis, Iran, phenomenology, support
INTRODUCTION
The burden of chronic diseases, such as chronic renal disease, is considered to be one of the greatest challenges of the health systems of the 21st century. It is anticipated that by 2020, there will be 1200 cases of end-stage renal disease (ESRD) per million population.[1] In ESRD, the irreversible damage caused to the kidneys renders alternative treatments necessary for the sustenance and continuation of life. Hemodialysis is the most common alternative treatment method in Iran and other parts of the world.[2] In 2013, 1,500,000 people in the world, 25,000 people in Iran,[3] and 1500 people in Isfahan Province were reported to have undergone hemodialysis.[4]
Although hemodialysis prolongs the life of patients, it also imposes many restrictions on them that may lead to physical, psychological, social, and economic complications.[5] It can also be the leading cause of depression, anxiety, low self-esteem, impaired mental impression, and hopelessness for the patients. Many patients experience a state of conflict between dependency on others and the hemodialysis machine and a desire to be independent, and this affects their relationship with the people who are most important in their lives.[6] Economic, employment-related, and social communication issues are among the social impacts of this disease and hemodialysis. Moreover, problems such as fatigue, infertility, sexual dysfunction, bone abnormalities, anemia, cardiovascular problems, and gastrointestinal disorders cause frequent hospitalizations that, in turn, may lead to mental disorders and increased mortality rate.[7] Chronic renal disease and hemodialysis cause numerous psychological, social, cultural, and spiritual challenges for patients and their families. Overcoming these challenges is possible only through providing holistic support for the patient. It is worth emphasizing, however, that despite the support provided by family and professional caregivers for the patients, these patients still express dissatisfaction with this support and believe it to be inadequate.[8] In fact, patients, family caregivers, and healthcare practitioners seem to have different understandings of the notion of support.[9,10]
Sadala (2006) argues that nurses plan their treatment process without taking into account the experiences of patients undergoing hemodialysis and this is the cause of patients’ dissatisfaction despite the great care and support they receive. Therefore, given the different aspects of support, it is impossible to develop an appropriate program for these patients without understanding their perception of the concept of support.[11]
Hitherto, many quantitative studies have been conducted in Iran with an emphasis on perceived social support and the status of patient support. For example, Rambod and Rafii (2009) have examined patients’ perception of social support,[9] Haririan et al. (2011) have evaluated information and instrumental support in these patients,[12] and Rambod et al. (2012) have examined the quality of life of these patients and its relationship with social support.[9] However, it is noteworthy that in most of these studies, the attitudes of respondents have been limited to a predetermined framework and only the social aspects of support have been addressed. In a qualitative study, the patients’ perception of support resources in coping with hemodialysis has been evaluated.[13] Understanding the concept of support, as a general and comprehensive concept, from the viewpoint of the patients helps professional healthcare practitioners, including nurses and domiciliary caregivers, to develop a realistic care-support program.[14] To provide an explanation of the concept of support from the perspective of hemodialysis patients, a deep understanding of the meaning of support is necessary. Moreover, the descriptive phenomenological method is the most suitable method to obtain a deep understanding of experiences and the complex phenomena.[15] Hence, in this study, the researcher decided to explain the concept of support from the patients’ perspective using the descriptive phenomenological method.
MATERIALS AND METHODS
This study was conducted using the descriptive phenomenological method. The study population consisted of patients with ESRD who were undergoing hemodialysis. Purposive sampling was performed and continued until data saturation, meaning no new topic or code appeared in the subsequent interviews and all information was repeated. The study subjects consisted of 17 patients who were willing to participate in the study, had no speech or hearing problems, could speak fluent Persian, and had undergone their first hemodialysis therapy session at least 3 months in advance. Patients with any factor that, during the interview, prevented them from continuing their cooperation or those who were unwilling to continue their participation were excluded from the study.
After obtaining the required license from Isfahan University of Medical Sciences, Isfahan, Iran, the researcher referred to Al-Zahra Hospital, Isfahan and presented her introduction letter to the authorities and obtained their approval. Then, after selecting a suitable environment for the interviews, the researcher selected the participants from among the hemodialysis patients using purposive sampling method. Next, the researcher introduced herself, offered the required information, explained the objectives of the study, and informed the participants that they could leave the study whenever they wanted to. In addition, the patients were assured that the information would be confidential and the name of the patients would not be expressed anywhere. Finally, after obtaining their willingness to participate and they signed written consent forms, the time of the interviews was scheduled.
On the day of the interview, the researcher held a face-to-face interview with each patient in a suitable room in Al-Zahra Hospital. The interviews began as unstructured interviews and were continued using exploratory questions. Each interview lasted for 30–60 min. With the consent of the participants, the interviews were recorded using an MP3 player (Creative model). At the end of each interview, the participants were informed about the likelihood of another meeting to complete and clarify the interviews. Although the participants agreed to this, a second interview was necessary in only one case.
After the interviews, each recorded interview was listened to several times and, using ONE NOTE software, they were transcribed verbatim and numbered by the researcher. Data saturation was reached after 17 interviews. Sampling lasted about 2 months, from the beginning of January 2015 until the end of February 2015.
Data analysis was performed using Colaizzi's method. First, in order to understand how the participants felt, their statements were read (step 1). Then, the key phrases were extracted (step 2) and were written in scientific language (step 3). The regulated concepts were organized into thematic categories (step 4). Then, the findings were integrated into a comprehensive description of the desired phenomenon (step 5), and this description of the investigated phenomenon was presented in the form of an explicit and clear statement (step 6). Finally, the findings were returned to the participants and were evaluated (step 7).[16]
In this study, for the validity and reliability of the data, Gaba and Lincoln criteria were used. The believability of the study was ensured through the researcher's long-term engagement in collecting and analyzing the data, and use of the revisions and reviews conducted by the research associates and participants. To achieve data reliability, after being heard, implemented, and analyzed, the interviews were peer-reviewed. In addition, auditing was used to achieve data neutrality and objectivity. Furthermore, given the previous experiences of the researcher in the hemodialysis ward, she tried not to let her views and beliefs affect the study's implementation process, tried to avoid prejudices, and did not study any similar research until the end of the analysis process.
In order to achieve reliability of findings, after the hearing, implementation, and analysis of the interviews, another person, who had mastered the qualitative studies, but was not involved in the study's process, was asked to help in the evaluation process. Thus, one or two of the recorded interviews together with the written form of the interviews were assigned to him to be evaluated. To provide the transferability of the study, the research was fully explained and the context and stages of the study were fully described to the subjects by the researcher. Furthermore, it was attempted to select subjects who were different in terms of demographic characteristics.[17] Since the interviews were in Persian, the spoken words of the participants were quoted indirectly.
RESULTS
In the present study, 17 patients (9 women and 8 men) with age ranging from 24 to 83 years and a minimum of 10 months and a maximum of 168 months of treatment length participated. In terms of education, the patients’ education level ranged from being illiterate to having master's degree. Moreover, seven patients were married and their wives took care of them, seven patients lived either with their parents or their children, and two patients lived alone. Diabetes was the most common underlying cause of chronic kidney disease [Table 1]. The analysis of the data resulted in 4 themes (psychological support, accompaniment, social support, and spiritual support) and 11 sub-themes. Psychological support consisted of two sub-themes of psychological support by healthcare practitioners and emotional support by family and relatives. Accompaniment included three sub-themes of assistance in transportation, providing and using medicine, and daily activities. Social support was identified with four sub-themes of promotion of the society's understanding of the patients’ condition, improvement of communication with others, the need for employment, and independence. Spiritual support was identified with the two sub-themes of the need for faith and trust in God and the need to resolve spiritual contradictions (paradoxes) [Table 2].
Table 1.
Participants’ demographic characteristics
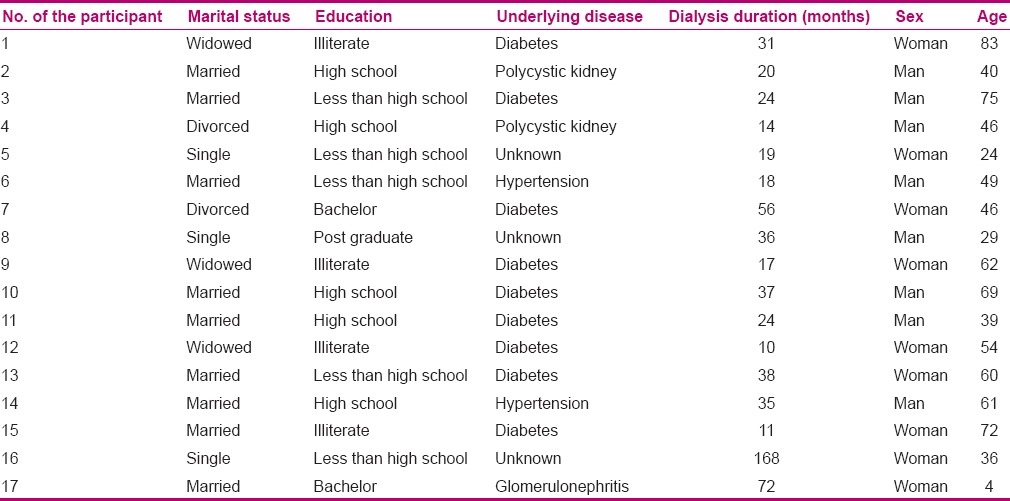
Table 2.
Themes and sub-themes
Psychological support
The participants emphasized two aspects of support: support by healthcare practitioners and support by family and relatives. Patients undergoing hemodialysis generally undergo three sessions of dialysis a week, each session lasting 4 h, and spend a great deal of time with healthcare practitioners. However, they are mostly cared for physically, and in addition to physical care, they stress their need for emotional and psychological support from healthcare practitioners and communication with them.
Participant 7 declared that s/he had been emotionally supported by the personnel and had not felt alone and, thus, was thankful.
Emotional support from family and relatives, including spouse and children, has a significant impact on the morale of the patients and is considered as an integral part of the care process. According to many participants, it is even more important than physical care. Understanding the situation and mood-swings of the patients enables their family to provide them with a better condition and devote more time to them.
Participant 4, who lived alone, expressed a greater need for emotional support from others than physical support.
From the participants’ statements, it can be understood that receiving psychological support from health practitioners, especially nurses and doctors, together with emotional support from their family can help the patients to tolerate the disease, and its treatment and complications. It can also make them feel that they are supported by others.
Accompaniment
Due to the accumulation of waste and water in the body tissues, such as brain cells, when the patients refer to the dialysis ward, they do not have a desirable general condition. Similarly, when they return home, because of low blood pressure caused by dialysis, the patients do not have a good condition and need to be accompanied by someone.
Participant 9 said that although s/he did not like to be a burden on his/her children, because of his/her poor condition and having vertigo, s/he needed to be accompanied by them.
To treat complications of kidney disease and hemodialysis, and to treat other underlying diseases and their complications, the patients need to use different medicines. In addition, because of visual impairments and old age in some patients, as well as illiteracy, they need the support of their family for the provision, and correct and timely use of their medicines.
Participant 5 pointed out that his/her drugs were purchased by his/her mother because s/he was unable to do so.
Participant 10 stated that because of suffering from diabetes and poor eyesight, his wife had accepted the responsibility to inject his insulin.
Most hemodialysis patients, often because of old age, underlying diseases and visual problems caused by these diseases, fatigue, and boredom, need to be accompanied in their daily activities.
Participant 3 said that owing to his poor eyesight, his wife took the responsibility for shaving his face and cutting his nails.
The participants’ statements illustrated that most dialysis patients do not have adequate physical power and good mental condition to perform their daily activities such as transportation, correct use of drugs, personal hygiene, and self-care. Therefore, the accompaniment of their families will guarantee the continuation of their lives and provide them with a high-quality life.
Social support
The participants demanded to be understood by the society. Instead of being pitied, which offends them, they would like to be understood and supported by others.
According to participant 11, no one cares about them and people help them out of pity, and this kind of behavior upsets them.
Sometimes, concealment or fear of social stigma reduces the relationship of the patients and their families with other people. In fact, families, regardless of the communication needs of the patient, try to maintain the position of other family members through hiding the disease.
Participant 16 declared that within the last 14 years that he has been undergoing dialysis, his mother has hidden his disease as she does not want to jeopardize his sisters’ chances of marrying. Therefore, they have refrained from any contact with most of their relatives.
These patients have to follow a specific schedule and spend much of their time in the dialysis ward. This often interferes with their work and leads to the loss of their jobs.
Participant 2, who was a truck driver, said that as he is often traveling, he cannot refer to the hospital according to the scheduled sessions. He stated that if he refers to the hospital three times a week for dialysis, he will get fired from his job.
Two or three dialysis sessions per week, morbidity in the case of inadequate dialysis, and frequent referral to the hospital lead to the dependency of the patients on the dialysis machine and healthcare practitioners. On the other hand, lethargy, fatigue, impaired vision, and other such problems result in the patients’ dependence on their families. This kind of dependency is more common in the weaker and older people. To be independent is one of the psychological needs of human beings and dependency on the dialysis machine, dialysis personnel, and family members is the problem these patients are faced with. Thus, helping them to maintain their independence is considered as an important component of support.
Participant 1 stated that she had asked her daughter to let her take care of her personal affairs or help her daughter with her work, but her daughter did not allow her.
The participants’ statements imply that increasing the society's understanding will have a significant impact on the people's support for these patients. Hence, using these patients in jobs commensurate with their capabilities and limitations and helping them to maintain their independence is essential and will enhance their social relationships.
Spiritual support
Participants declared that they needed to enhance their faith and trust in God or spiritual forces, and some of them sought support to resolve their religious contradictions.
Participant 16 said that s/he has only asked God for the healing of his/her disease. S/he requested help in maintaining his/her faith in spite of the disease.
Some participants, because of numerous problems and prolonged duration of the disease, had experienced spiritual and religious contradictions. This was more prevalent in younger people.
Participant 8 said that s/he has always been thinking about his/her relationship with God. S/he believed that because of the illness, s/he has lost all his/her opportunities. S/he asked why God does not heal him/her if He can, and wanted an explanation in this regard.
According to the participants, being hopeful of the grace of God and reliance on him, and asking Imams for help together with prayer brings them peace and helps them to cope with their disease-related problems much better and easier. Hence, they demanded spiritual support and believed that strengthening their spirituality is the only way to resolve their spiritual and religious contradictions.
DISCUSSION
The present study aimed to examine the concept of support from the viewpoint of hemodialysis patients. Consequently, emotional or psychological support, accompaniment, social support, and spiritual support were introduced by the participants as the concepts of support. Psychological or emotional support was one of the concepts, and the participants declared that they need to be supported emotionally by healthcare practitioners. Similarly, in a study conducted by Sanson Fisher et al. (2009), most patients stated that they needed to be supported by their doctors, nurses, family, and relatives.[18]
Asgari et al. (2010) conducted a qualitative research on the perception of chronic renal disease patients of support resources in coping with hemodialysis.[13] They extracted six themes that included being unified with the family, informed confidence in doctors, empathy and responsibility of nurses, gaining spirit from adapted patients, feeling valuable when accompanied by relatives, and satisfaction with supporting organizations. Most of these themes are in line with those of the current study.
The participants also expressed that they need to be supported emotionally by their families. In Iran, family members are emotionally dependent on each other and when one member becomes ill, s/he is supported by the family more than ever. However, sometimes, families are under pressure because of a family member's chronic disease, and therefore, that family member feels that s/he is not supported by his/her family.
According to many studies, family is the most important and primary source of support for patients, and the highest level of social support is received from the family.[12,19,20,21,22,23,24] Although all participants of this study (save two) were living with and supported by their families, they felt that they needed more support. The results obtained in the study of Juergensen et al. (2006) are also in line with those of the present study.[25] Their results showed that the patients were living with and supported by their families, but considered these supports inadequate.[25]
The participants declared that for transportation, they needed to be accompanied by someone. In this regard, Braz et al. (2005) wrote that uremia brings about concentration problems, memory loss, and impaired judgment.[22] Thus, most patients required to be accompanied in going out of their home.[22]
Continued hemodialysis results in different problems caused by frequent hospitalizations for the patients. Moreover, owing to the poor condition of the patients both before and after dialysis, they need to be accompanied by someone.
Providing medicines and helping the patients to take their drugs correctly and on time was another case of support considered by the patients. These patients have to take multiple kinds of medicines and, as statistics show, taking them based on the prescription is an important challenge for the patients. Therefore, for an accurate and timely use of medicines, the patients need to be helped by others and, in this regard, having the support of the family is very important.[23]
Assistance in daily activities, such as personal hygiene and home-care needs, was also stressed by the participants. Continued symptoms of the disease result in physical weakness, lack of energy, and fatigue in the patients, to the extent that these patients sometimes need help to carry out even their simplest daily activities.[24]
The results also showed that the participants hated to be pitied and instead needed to be understood by others as they considered this as a form of support. In the study by Melissa et al. (2007), social support improved the physical and mental conditions, quality of life, and survival rate of these patients.[25] Similarly, the results obtained by Skar and Folkestad (2013) showed that not only in our country, but also in all Western societies, patients, instead of being socially supported, are pitied by their relatives and friends and suffer from this issue.[26]
Moreover, the participants were upset about reducing their social relationships and believed that providing conditions to promote relationships with others would be supportive. The results of the study conducted by Rezai et al. (2009) showed that most patients undergoing hemodialysis had a completely negative image of their responses to social stimuli, communication with others, and presence in society, and had experienced changes in their social interactions.[27]
The participants considered employment as a kind of social support. Since these patients spend much of their time on dialysis and medical care and often have poor health conditions, they are faced with limitations in terms of employment and usually lose their jobs.[28,29,30,31] On the other hand, the participants emphasized their independence. In this regard, Al-Nazli (2013) noted that the patients’ dependency on the dialysis machine, diet-related limitations, the time spent for hemodialysis, and frequent hospitalizations lead to the patients’ dependence that troubles them. Dependency on treatment and inability to perform daily activities lead to patients’ social isolation and diffidence, which in turn make them more dependent and affect their psychological and social performance and quality of life.[23] Therefore, nurses and domiciliary caregivers should allow patients to perform their daily activities alone, as far as the activity does not jeopardize the patients’ safety and health. In Iran, because of strong emotional connections, domiciliary caregivers and even nurses do not allow the patients to carry out their personal activities. This behavior may cause the patients to lose their self-confidence and have a sense of powerlessness. Thus, according to the participants, social support constitutes another aspect of support.
The participants also believed that faith and trust in God would help them tolerate their problems better. Furthermore, they considered the strengthening of their spiritual dimensions as an important aspect of support. The fact that human beings need to have faith and trust in God is explicitly mentioned in Quran. It is said in Quran, “O mankinds, you all need the needless God.” Studies have also shown that often during illness, religious beliefs and tendency toward spirituality increase and affect the acceptance of hemodialysis by the patients. In this regard, religious belief, as a lifestyle, is a good source of support for the patients and equips them with efficient types of coping skills.[13] Tanyi and Werner (2007) have shown that women, who have strong religious orientations, undergoing hemodialysis use positive spiritual themes in their lives to deal with problems.[10]
In addition, statements of the participants showed that through recourse to Imams, they try to get closer to God. The Holy Quran says, “O believers! Be virtuous and choose a way to get closer to God.” This way is definitely “recourse” and includes any action that brings one closer to God.[32]
On the other hand, some participants considered their disease as a disaster. They believed that they did not deserve the disease and noted that they were angry with God; however, they were upset about this issue and said that they would like to be supported to resolve this contradiction. Kazemi et al. (2011) found that at the very outset of the treatment process, the patients experience a kind of shock and crisis and are angry with God, but as their general condition begins to improve, they succeed to overcome this paradoxical situation.[33] Therefore, these patients need to be supported spiritually or morally by the healthcare personnel, and it is necessary for the personnel to expand their knowledge and understanding of spirituality and include it in their caring programs.[34]
CONCLUSION
According to the participants of this study, different aspects of support included mental or psychological support, social support, accompaniment, and spiritual support. However, it seems that accompaniment and spiritual support are unique concepts obtained in this study. Since this study was conducted in Iran and people in Iran have strong emotional connections with their relatives such as spouses and children, it seems that this issue has to be considered in healthcare planning and training domiciliary caregivers. Furthermore, strengthening the spiritual dimension of these patients can improve their quality of life and help them adapt to the treatment process.
ACKNOWLEDGMENT
This study is the result of a research project approved by the Isfahan Kidney Research Center, Iran. Thus, we would like to express our endless gratitude to the head and members of this center and all those who helped us conduct this study, particularly the participants.
Footnotes
Source of Support: Isfahan University of Medical Sciences.
Conflict of Interest: Nil.
REFERENCES
- 1.Zheng J, You LM, Lou TQ, Chen NC, Lai DY, Liang YY, et al. Development and psychometric evalution of the Dialysis patient-perceived Exercise Benefits and Barriers Scales. Int J Nurs Stud. 2010;47:166–80. doi: 10.1016/j.ijnurstu.2009.05.023. [DOI] [PubMed] [Google Scholar]
- 2.Hemati Z, Alidosti M, Sharifirad G, Kargar M. The relationship between depression and quality of life among hemodialysis patients in Chaharmahal and Bakhtiary province in the year 2011. J Educ Health Promot. 2012;2:6. doi: 10.4103/2277-9531.106645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Iranian Consortium of Dialysis. Calendar of Dialysis by the End of 2014. [Last accessed on 2015 Mar 9]. Available from: http://www.iranesrd.com/
- 4.Mojdeh S, Karimi S, Mehrabi A, Bakhtiari S. Etiology of renal failure and peritoneal dialysis complications in Isfahan. Health. 2013;5:1702–5. [Google Scholar]
- 5.Khan MA. Frequency of symptomatology in patients on hemodialysis. RMJ. 2012;37:24–6. [Google Scholar]
- 6.Shasty C, Haj Babaei M. Examine the adequacy of dialysis in patients undergoing hemodialysis in Tehran Hospitals. Ebnesina J. 2012;40:24–9. [Google Scholar]
- 7.Bryan NS, Torregrossa AC, Mian AI, Berkson DL, Westby CM, Moncrief JW. Acute effects of hemodialysis on nitrite and nitrate: Potential cardiovascular implications in dialysis patients. Free Radic Biol Med. 2013;58:46–51. doi: 10.1016/j.freeradbiomed.2013.01.020. [DOI] [PubMed] [Google Scholar]
- 8.Dabirian A, Zolfaghari H, Abed Saidi H, Alavi-Majd H. Views of AIDS patients regarding nursing care quality in healthcare centers affiliated to Shaheed Beheshti and Tehran Universities of Medical Sciences. JNM SBMU. 2008;18:40–5. [Google Scholar]
- 9.Rambod M, Rafii F. Perceived social support and quality of life in Iranian hemodialysis patients. J Nurs Scholarsh. 2010;42:242–9. doi: 10.1111/j.1547-5069.2010.01353.x. [DOI] [PubMed] [Google Scholar]
- 10.Tanyi RA, Werner JS. Spirituality in African American and Caucasian women with end-stage renal disease on hemodialysis treatment. Health Care Women Int. 2007;28:141–54. doi: 10.1080/07399330601128486. [DOI] [PubMed] [Google Scholar]
- 11.Sadala ML, Lorençon M. Life with a hemodialysis machine. J Ren Care. 2006;32:147–52. doi: 10.1111/j.1755-6686.2006.tb00006.x. [DOI] [PubMed] [Google Scholar]
- 12.Haririan HR, Aghajanloo A, Fard MG. Assessment of Informational and instrumental support in hemodialysis patients in the hospitals of Zanjan University of Medical Sciences. NMCJ. 2011;1:25–30. [Google Scholar]
- 13.Asgari MR, Mohammadi E, Fallahi Khoshknab M, Tamadon MR. The perception of chronic renal failure patients from advocacy resources in adjustment with hemodialysis: A qualitative study. IJCCN. 2011;3:133–44. [Google Scholar]
- 14.Salsal M, Parvizi S, Adib Hajbagheri M. Vol. 2. Tehran: Boshra Publication; 2004. Qualitative Research Methods; pp. 2–7. [Google Scholar]
- 15.Streubert SH, Carpenter D. Philadelphia: Lippincott Williams and Wiking; 2003. Qualitative Research in Nursing; p. 67. [Google Scholar]
- 16.Burns N, Grove SK. St Louis: Saunders; 2009. The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence; pp. 24–30. [Google Scholar]
- 17.Polit DF, Beck CT. Philadelphia: Lippincott, Williams and Wilkins; 2014. Essentials of Nursing Research; p. 333. [Google Scholar]
- 18.Sanson-Fisher R, Girgis A, Boyes A, Bonevski B, Burton L, Cook P. The unmet supportive care needs of patients with cancer. Supportive Care Review Group. Cancer. 2000;88:226–37. doi: 10.1002/(sici)1097-0142(20000101)88:1<226::aid-cncr30>3.3.co;2-g. [DOI] [PubMed] [Google Scholar]
- 19.Vázquez I, Valderrábano F, Fort J, Jofré R, López-Gómez JM, Moreno F, et al. Spanish Cooperative Renal Patients Quality of Life Study Group. Psychosocial factors and health-related quality of life in hemodialysis patients. Qual Life Res. 2005;14:179–90. doi: 10.1007/s11136-004-3919-4. [DOI] [PubMed] [Google Scholar]
- 20.Zamanzadeh V, Heidarzadeh M, Oshvandi K, Lakdizaji S. Relationship between quality of life and social support in hemodialysis patients in Imam Khomeini and Sina Educational Hospitals of Tabriz University of Medical Sciences. Medical Journal of Tabriz University of Medical Sciences. 2007;29:49–5. [Google Scholar]
- 21.Juergensen E, Wuerth D, Finkelstein SH, Juergensen PH, Bekui A, Finkelstein FO. Hemodialysis and peritoneal dialysis: Patients’ Assessment of their satisfaction with therapy and the impact of the therapy on their lives. Clin J Am Soc Nephrol. 2006;1:1191–6. doi: 10.2215/CJN.01220406. [DOI] [PubMed] [Google Scholar]
- 22.Braz Pardijani S, Mohammadi I, Bromand B. The effect of self care education on quality of life and physical problems in hemodialysis patients. Journal of Kordistan University Medical Science. 2005;10:69–79. [Google Scholar]
- 23.Al Nazly E, Ahmad M, Musil C, Nabolsi M. Hemodialysis stressors and coping strategies among Jordanian patients on hemodialysis: A qualitative study. Nephrol Nurs J. 2013;40:321–8. [PubMed] [Google Scholar]
- 24.Letchmi S, Das S, Halim H, Zakariah FA, Hassan H, Mat S, et al. Fatigue experienced by patients receiving maintenance dialysis in hemodialysis units. Nurs Health Sci. 2011;13:60–4. doi: 10.1111/j.1442-2018.2011.00579.x. [DOI] [PubMed] [Google Scholar]
- 25.Thong MS, Kaptein AA, Krediet RT, Boeschoten EW, Dekker FW. Social support predicts survival in dialysis patients. Nephrol Dial Transplant. 2007;22:845–50. doi: 10.1093/ndt/gfl700. [DOI] [PubMed] [Google Scholar]
- 26.Skår AB, Folkestad H, Smedal T, Grytten N. “I refer to them as my colleagues”: The experience of mutual recognition of self, identity and empowerment in multiple sclerosis. Disabil Rehabil. 2013;36:672–7. doi: 10.3109/09638288.2013.808273. [DOI] [PubMed] [Google Scholar]
- 27.Rezai R, Hejazi SH, Shahnazari J, Mahmoudi M, Siedi Andy S, Payesh J. Comparison of body image in patients treated with hemodialysis and kidney transplant. Psyesh Journal. 2010;8:279–87. [Google Scholar]
- 28.Greeff M, Uys LR, Wantland D, Makoae L, Chirwa M, Dlamini P, et al. Perceived HIV stigma and life satisfaction among persons living with HIV infection in five African countries: A longitudinal study. Int J Nurs Stud. 2010;47:475–86. doi: 10.1016/j.ijnurstu.2009.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wu AW, Fink NE, Marsh-Manzi JV, Meyer KB, Finkelstein FO, Chapman MM, et al. Changes in quality of life during hemodialysis and peritoneal dialysis treatment: Generic and disease specific measures. J Am Soc Nephrol. 2004;15:743–53. doi: 10.1097/01.asn.0000113315.81448.ca. [DOI] [PubMed] [Google Scholar]
- 30.Singh AK, Farag YM, Mittal BV, Subramanian KK, Reddy SR, Acharya VN, et al. Epidemiology and risk factors of chronic kidney disease in India - results from the SEEK (Screening and Early Evaluation of Kidney Disease) study. BMC Nephrol. 2013;14:114. doi: 10.1186/1471-2369-14-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. 11th ed. Philadelphia: Lippincott Williams and Wilkins; 2010. Brunner and Suddarth's Text Book of Medical-Surgical Nursing; pp. 820–30. [Google Scholar]
- 32.Ameli H. 17th ed. Qom: Eslami Publications; 2010. Vasael Shia; pp. 340–2. [Google Scholar]
- 33.Kazemi M, Nasrabadi AN, Hasanpour M, Hassankhani H, Mills J. Experience of Iranian persons receiving hemodialysis: A descriptive, exploratory study. Nurs Health Sci. 2011;13:88–93. doi: 10.1111/j.1442-2018.2011.00586.x. [DOI] [PubMed] [Google Scholar]
- 34.Nia SH, Hojjati H, Nazari R, Qorbani M, Akhoondzade G. The effect of prayer on mental health of hemodialysis patients referring to Imam Reza Hospital in Amol City. IJCCN. 2012;5:29–34. [Google Scholar]