

Abstract
Objective
Treatment of severe ulcerative colitis (UC) is challenging. Although the efficacy of tacrolimus (TAC) and infliximab (IFX) have been evaluated in patients with severe UC, the safety and efficacy levels of sequential therapies (TAC→IFX/IFX→TAC) in these patients remain unclear. The aim of this study was to assess short-term and long-term outcomes in patients with severe UC treated with TAC and IFX.
Methods
From October 2001 to February 2014, 29 patients with consecutive severe UC treated with TAC or IFX were retrospectively evaluated. Median follow-up duration was 27 months (range 0.5–118 months). The primary end point was short-term outcomes at 8 weeks after induction of TAC (TAC group, n=22) or IFX (IFX group, n=7). The secondary end point included long-term outcomes and colectomy-free survival. The clinical response was evaluated based on a partial Mayo score.
Results
The clinical remission (CR) rate at 8 weeks in the TAC and IFX groups was 63.6% and 71.4%, respectively. In 13 of the 29 patients (10 in the TAC group, 3 in the IFX group), sequential therapies were used in their clinical courses. In 9 of these 13 patients (6 in the TAC group, 3 in the IFX group), CR was achieved and maintained by sequential therapies. Overall cumulative colectomy-free survival was 79.3% at 118 months.
Conclusions
TAC and IFX had similar effects on remission induction in patients with severely active UC. Sequential therapies could rescue patients with UC who failed initial treatment with TAC or IFX. In clinical practice, sequential therapies might be deliberately performed.
Keywords: INFLAMMATORY BOWEL DISEASE, IBD CLINICAL, ULCERATIVE COLITIS
Summary box.
What is already known about this subject?
-
▸
Corticosteroid (CS) is a first-line therapy for patients with severe ulcerative colitis (UC).
-
▸
Second-line rescue therapy using tacrolimus (TAC) or infliximab (IFX) is considered for severe UC cases refractory to CS.
-
▸
Data on the short-term and long-term outcomes of patients with severe UC treated with TAC and IFX are limited.
-
▸
The efficacy and safety levels of sequential therapies (TAC→IFX or IFX→TAC) remain unclear.
What are the new findings?
-
▸
TAC and IFX had similar effects on remission induction in patients with severe UC.
-
▸
Sequential therapies could avoid colectomy in patients with severe UC refractory to initial treatment with TAC or IFX.
-
▸
In our study, there were no serious adverse events in the treatment with sequential therapies.
How might it impact on clinical practice in the foreseeable future?
-
▸
Our data demonstrated that sequential therapies could be considered for patients with severe UC who failed to respond to initial treatment with TAC or IFX.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory disorder of the colon characterised by diarrhoea, bloody stool, abdominal pain, fever, anaemia and weight loss.1
A recent study showed that 25% of patients with UC experienced episodes of severe colitis.2 Although introduction of intravenous corticosteroids (CS) has modified the natural history of severe acute relapse, approximately 30–40% of patients with UC are refractory to steroid therapy, and without further medical management these patients will require emergency colectomy.3 Therefore, the development of a second-line rescue therapy for steroid-resistant cases remains an important challenge. The calcineurin-inhibitor cyclosporine (CsA) is an immunosuppressant that inhibits T-cell-mediated production of interleukin-2 (IL-2). CsA was first shown to be an effective rescue therapy for acute severe steroid-refractory UC in 1994.4 Recent studies showed response rates to CsA ranging from 64% to 82%.4 5 Despite the benefits of CsA treatment, it is associated with significant toxicity and adverse reactions, and thus alternative agents are required.
Tacrolimus (TAC) is an immunosuppressive macrolide isolated from Streptomyces tsukubaensis.6 TAC inhibits the complexation of calcineurin with its respective cytoplasmic receptors, cyclophilin and FK-binding protein 12, both of which regulate calmodulin-dependent phosphatase activity, thereby interrupting the signal transduction pathway in T cells.7 Although TAC and CsA have similar modes of action, TAC has a 30-fold to 100-fold greater immunosuppressive effect in vitro and a 10-fold to 20-fold greater effect in vivo than CsA, as well as more reliable intestinal absorption, even in the presence of gastrointestinal disease.8 A randomised controlled trial and several case studies have demonstrated that TAC is effective for inducing and maintaining remission in patients with refractory UC.8–11 TAC is thus considered to be a promising therapeutic option for refractory UC.
In the past 10 years, infliximab (IFX), a monoclonal antibody that binds free and membrane-bound tumour necrosis factor α, has demonstrated efficacy for UC. Its superior efficacy compared to placebo in moderate-to-severe non-acute UC is well established based on UC trials (ACT1 and ACT2), with a response rate between 61% and 69%.12
While the use of both TAC and IFX has been shown to be effective and safe as rescue therapy, data directly comparing the effects of these two agents on severe UC are limited.13 14 In the present study, we reviewed a series of patients with severe UC admitted consecutively to our hospital from 2001 up to the present, who had been treated with TAC or IFX.
Methods
Patients
This was a retrospective single centre study in Kyoto University Hospital. We reviewed the medical records of all patients who received at least one IFX infusion or TAC treatment for treatment of severe active UC.
The diagnosis of UC was confirmed according to standardised criteria by prior clinical assessment, radiology, endoscopy and histology. We used the same definitions of steroid dependency and refractoriness as the European Crohn's and Colitis Organization consensus.15 According to the Montreal classification, a disease event was categorised as proctitis if present up to 15 cm from the anal verge, as left-sided colitis if present up to but not beyond the splenic flexure, or as extensive colitis if present beyond the splenic flexure.16
From October 2001 to February 2014, all patients with severe UC were treated with TAC or IFX at Kyoto University Hospital. All patients with UC in this study had severe disease activity with a Mayo score greater than 10 and moderate-to-severe inflammation on sigmoidoscopy, despite concurrent treatment with CS and/or immunomodulators (IM).
Treatment regimens were as follows: TAC was administered orally at an initial dose of 0.1 mg/kg/day or was administered intravenously at an initial dose of 0.01 mg/kg/day, and the dose was adjusted to produce whole blood trough levels of 10–15 ng/mL to induce remission. IFX episodic therapy was defined as a single infusion of 5 mg/kg of IFX at induction, followed by further infusion if necessary. Scheduled therapy was defined as intravenous infusions of IFX at a dose of 5 mg/kg at weeks 0, 2 and 6, followed by regular infusions every 8 weeks thereafter. For patients who did not respond to initial treatments either with TAC or IFX, and those who had relapsed despite their response to initial treatment, sequential therapies (TAC→IFX or IFX→TAC) were performed under the global assessment of physicians.17 We collected data on the demographics, baseline characteristics of severe UC, previous and concomitant medications, clinical outcome and adverse events of both treatments.
Informed consent for participation in this study, which was approved by the institutional ethics committee, was provided by all patients.
Clinical outcomes
To evaluate disease activity and response to both treatments, a partial Mayo score18–20 was retrospectively determined both before treatment and after 8 weeks of treatment, as well as at the last follow-up visit. In Kyoto University Hospital, we evaluate disease activity of all patients with UC, at least on every 4-week visit after starting their induction therapy, by the partial Mayo score. Clinical remission (CR) was defined as a partial Mayo score of less than 3. Relapse was defined as an increase in the partial Mayo score to 3 or higher with additional therapies required. Mucosal healing was defined as endoscopic Mayo score of 0. Short-term outcomes were evaluated at 8 weeks after initiating TAC or IFX treatment. Long-term outcomes were evaluated using data from patients who were followed up for more than 6 months after TAC or IFX treatment. Moreover, colectomy-free survival was evaluated in all 29 patients with severe UC during the period from the time of their initial treatments to the last follow-up visit.
Definition of cytomegalovirus reactivation
All patients were tested for colonic cytomegalovirus (CMV) reactivation by immunohistochemistry and quantitative real-time PCR using colonic biopsy specimens (mucosal PCR). Colonic biopsy specimens were obtained from inflamed colonic mucosa, fixed in formalin, embedded in paraffin and stained with H&E, and immunohistochemistry was performed using anti-CMV monoclonal antibodies (Dako Cytomation, Kyoto, Japan).21 Cases in which the CMV-DNA copy number was over 10 copies/μg DNA were defined as positive for CMV reactivation. Cases in which CMV was detected by either one of these methods were diagnosed with positive colonic CMV reactivation.22
Assessment and statistics
The primary end point of this study was short-term outcome at 8 weeks after induction of TAC or IFX. Secondary end points included long-term outcome and colectomy-free survival at 2014 after the initiation of treatment. Moreover, we assessed the efficacy and safety of the sequential therapies (TAC→IFX or IFX→TAC) in patients with UC refractory to the initial treatment. Cumulative colectomy-free survival was assessed using the Kaplan-Meir method. Comparisons of differences within groups were performed using the Mann-Whitney U test or Student t test, depending on the distribution. Categorical data were compared by χ2 analysis. A p value of less than 0.05 was considered to be statistically significant.
Results
Patient characteristics
Clinical characteristics of all patients with severe UC are shown in table 1. Median age at diagnosis of severe UC was 34 years (range 19–69 years). Median disease duration before the induction therapy was 43 months (range 2–348 months). Median follow-up period was 27 months (range 0.5–118 months). Of the 29 patients, 18 were men and 11 were women. Of the 29 patients, 24 were hospitalised at the induction therapy. Median partial Mayo score was 9 (range 8–9) and the endoscopic Mayo score was 3 (range 2–3). Of the 29 patients, 23 had extensive disease type and the other 6 patients had left-sided disease. C reactive protein level was 7.0 (0.1–27.1) mg/dL, haemoglobin level was 10.3 (7.1–13.4) g/dL and serum albumin level was 2.9 (1.7–4.9) g/dL. Regarding previous response to CS, 14 of the 29 patients (48.3%) were refractory to CS, 11 (37.9%) were dependent on CS and the remaining 4 patients (13.8%) were naïve to CS. As concomitant therapy with the induction therapy, except for one patient who was allergic to 5-aminosalicylate (5-ASA), the patients were all treated with 5-ASA. Prior to initiating treatment with TAC or IFX, 16 of the 29 patients were treated with CS (9 with intravenous CS and 7 with oral CS). Median duration of treatment with systemic CS before initiating TAC or IFX was 36 days (range 14–4200 days). At initiating treatment with TAC or IFX, CS had already tapered off in 9 of the 29 patients. CS was not used for these patients’ induction therapies because they had previous histories of long-term use of CS. Despite being naïve to CS in the remaining four patients, they were not treated with CS because they refused it. Nine of the 29 patients were treated with concomitant thiopurine and 15 were treated with concomitant cytapheresis.
Table 1.
Clinical characteristics of 29 patients with severe UC
| All patients | Tacrolimus group | Infliximab group | p Value* | |
|---|---|---|---|---|
| (n=29) | (n=22) | (n=7) | ||
| Age at diagnosis of severe UC (median (range)) (years) | 34 (19–69) | 34.5 (19–69) | 33 (22–58) | 0.799 |
| Disease duration prior to the induction therapy (median (range)) (months) | 43 (2–348) | 45 (2–348) | 32 (6–157) | 0.760 |
| Follow-up period (median (range)) (months) | 27 (0.5–118) | 21 (2–118) | 30 (0.5–79) | 0.541 |
| Gender | 0.758 | |||
| Male | 18 | 14 | 4 | |
| Female | 11 | 8 | 3 | |
| Hospitalised patients at the induction therapy | 24 | 19 | 5 | 0.569 |
| Partial Mayo score (median (range)) | 9 (8–9) | 8.5 (8–9) | 9 (8–9) | 0.779 |
| Endoscopic Mayo score (median (range)) | 3 (2–3) | 3 (3–3) | 3 (2–3) | 0.476 |
| Disease extent | 0.555 | |||
| Extensive | 23 | 18 | 5 | |
| Left sided | 6 | 4 | 2 | |
| Laboratory examination (mean±SD (range)) (mg/dL) | ||||
| C reactive protein | 7.0±7.1 (0.1–27.1) | 5.7±5.5 (0.1–19) | 11.2±10.3 (1.3–27.1) | 0.270 |
| Haemoglobin | 10.3±1.8 (7.1–13.4) | 10.4±2.0 (7.1–13.4) | 10.0±1.1 (9.3–12.5) | 0.858 |
| Albumin | 2.9±0.6 (1.7–4.0) | 2.9±0.6 (1.8–4.0) | 2.8±0.7 (1.7–3.7) | 0.939 |
| Previous response to corticosteroid | ||||
| Corticosteroid refractory | 14 | 12 | 2 | 0.436 |
| Corticosteroid dependent | 11 | 6 | 5 | 0.096 |
| Corticosteroid naïve | 4 | 4 | 0 | 0.544 |
| Concomitant therapy at the induction therapy† | ||||
| 5-aminosalitirate | 28 | 21 | 7 | 1.000 |
| Corticosteroid | 16 | 12 | 4 | 1.000 |
| Thiopurine | 9 | 6 | 3 | 0.746 |
| Cytapheresis | 15 | 13 | 2 | 0.323 |
| Positive rate of CMV reactivation (percentage (positive/all)) (%) | 44.8 (13/29) | 40.9 (9/22) | 57.1 (4/7) | 0.452 |
Numbers of patients are shown unless specified.
*Comparison of differences between tacrolimus group and infliximab group was evaluated.
†Some patients were treated in conjunction with other therapies.
CMV, cytomegalovirus; UC, ulcerative colitis.
For the induction therapy, 22 of the 29 patients were treated with TAC (TAC group) and the remaining 7 patients were treated with IFX (IFX group). The choice of TAC or IFX treatment for the induction therapy was conducted according to the primary physician's decision at that time. There were no significant differences in the clinical characteristics between the TAC and IFX groups.
Short-term outcomes
The clinical course of short-term outcomes of the 29 patients with severe UC is shown in figure 1. Of 22 patients in the TAC group, 14 achieved a CR at 8 weeks after initiating TAC and 6 of the remaining 8 patients could not achieve a CR, although they responded to TAC. The remaining two patients did not respond to TAC and required sequential therapy (switched to IFX) within 8 weeks after initiating TAC. Of seven patients in the IFX group, five achieved a CR at 8 weeks after initiating IFX, while one required sequential therapy (switched to TAC). One patient who did not respond to IFX resulted in a colectomy without sequential therapy. The CR rate at 8 weeks from initiating TAC or IFX including sequential therapy in the 29 patients with severe UC was 65.5% (19/29). The colectomy rate at 8 weeks was 3.4% (1/29).
Figure 1.

Short-term and long-term outcomes of the 29 patients with severe ulcerative colitis (UC). Short-term outcomes: 14 of 22 patients in the tacrolimus (TAC) group and 5 of 7 patients in the infliximab (IFX) group achieved a clinical remission (CR) at 8 weeks after initiating TAC or IFX. Two patients in the TAC group were refractory to TAC and required sequential therapy. Two patients in the IFX group were refractory to IFX and one could achieve a CR after switching to TAC. The remaining one resulted in colectomy without switching to TAC. The CR rate at 8 weeks in the TAC and IFX groups was 63.6% and 71.4%, respectively. Long-term outcomes: In the TAC group, of 14 patients who achieved a CR at 8 weeks after initiating TAC, 11 patients could maintain a CR and 3 flared-up. A total of nine patients could not achieve and maintain a CR with TAC. Six of the nine patients could achieve a CR by sequential therapy, and the remaining three resulted in colectomy (one patient within 6 months). Two patients who required sequential therapy within 8 weeks after initiating TAC resulted in colectomy within 6 months after initiating TAC. In the IFX group, of four patients who achieved a CR at 8 weeks after initiating IFX, three could maintain a CR and one flared-up. A total of two patients could not achieve and maintain a CR with IFX and they could achieve a CR by sequential therapy. One patient who achieved a CR by sequential therapy within 8 weeks after initiating IFX could maintain a CR. *Reveals the patient who resulted in colectomy within 6 months after initiating TAC or IFX.
Long-term outcomes
Of the 29 patients with severe UC, 25 were followed up for more than 6 months after initiating treatment with TAC or IFX. The median follow-up period of the 25 patients (TAC group: n=19, IFX group: n=6) was 29 months (range 7–118 months). The clinical course of long-term outcomes of the 25 patients with severe UC is shown in figure 1. Of 14 patients who achieved a CR at 8 weeks after initiating TAC, 11 could maintain a CR continuing TAC. The remaining three had a flare-up of UC, of whom one resulted in colectomy without sequential therapy within 6 months after initiating TAC. The remaining two patients who had a flare-up of UC despite achieving a CR and six patients who could not achieve a CR at 8 weeks after initiating TAC required sequential therapy (switched to IFX). After induction of sequential therapy, six of the eight patients could achieve and maintain a CR, and the remaining two required colectomy. Moreover, two patients who required the sequential therapy (switched to IFX) within 8 weeks after initiating TAC could not achieve a CR and required colectomy. However, in the IFX group, three of the four patients who achieved a CR at 8 weeks after initiating IFX could maintain a CR. The remaining one patient who had a flare-up of UC and the one patient who could not achieve a CR at 8 weeks after initiating IFX required sequential therapy (switched to TAC), and they could achieve and maintain a CR. The patient who required sequential therapy (switched to TAC) within 8 weeks after initiating IFX could achieve and maintain a CR. Overall, total 23 patients (TAC group: n=17, IFX group: n=6) could maintain a CR at the end of follow-up. The medications in these patients are summarised in table 2. Regarding their maintenance therapy at the end of follow-up, five patients in the TAC group and one patient in the IFX group were treated with IFX in conjunction with IM and 5-ASA. One patient in the TAC group and two patients in the IFX group were treated with IFX in conjunction with 5-ASA. Three patients in the TAC group were treated with TAC in conjunction with IM and 5-ASA. Four patients in the TAC group and two patients in the IFX group were treated with IM and 5-ASA. One patient in the TAC group was treated with IM alone due to intolerance of 5-ASA. Three patients in the TAC group and one patient in the IFX group were treated with 5-ASA. Regarding cumulative dosage of each drug during the observational period, the mean cumulative dosage of IM in the TAC group was more than twice that in the IFX group.
Table 2.
Medications in patients who achieved a CR at the end of follow-up
| TAC group | IFX group | |
|---|---|---|
| (n=17) | (n=6) | |
| Observational period (median (range)) (months) | 29 (14–118) | 32 (22–79) |
| Maintenance therapy at the end of follow-up | ||
| IFX+IM+5-ASA | 5 | 1 |
| IFX+5-ASA | 1 | 2 |
| TAC+IM+5-ASA | 3 | 0 |
| IM+5-ASA | 4 | 2 |
| IM | 1 | 0 |
| 5-ASA | 3 | 1 |
| Cumulative dosage of each drug during observational period | ||
| TAC (mean (range)) (mg) | 2852 (389–5937) | 1016 (0–2861) |
| IFX (mean (range)) (mg) | 3866 (1500–19 260) | 5843 (225–20 520) |
| IM (mean (range)) (mg) | 38 910 (7800–110 550) | 16 122 (0–42 700) |
| 5-ASA (mean (range)) (g) | 4537 (0–10 138) | 3609 (828–6994) |
Numbers of patients are shown unless specified.
5-ASA, 5-aminosalicylate; CR, clinical remission; IFX, infliximab; IM, immunomodulators; TAC, tacrolimus.
Comparison of maintenance therapy between the patients who achieved a CR with TAC and those who relapsed with TAC
Of the 29 patients with severe UC, 25 (22 in the TAC group and 3 in the IFX group) were treated with TAC in their clinical course. We analysed the differences in the maintenance therapy between those who achieved a CR with TAC (CR group, n=14) and those who relapsed with TAC (Relapse group, n=11), as shown in table 3. In the 18 patients (10 in the CR group and 8 in the Relapse group), long-term use of TAC (more than 6 months) was performed. As a result, 10 of 18 patients (55.6%) could achieve a CR. Regarding the maintenance therapy with TAC, the median treatment duration with TAC was 471 days (range 325–995 days) in the 10 patients who were finally switched to IM or treated with the combination of TAC and IM.
Table 3.
Comparison of maintenance therapy between the patients who achieved a CR with TAC and those who relapsed with TAC
| CR | Relapse | |
|---|---|---|
| (n=14) | (n=11) | |
| Duration of TAC use (median (range)) (days) | 411 (121–995) | 405 (63–962) |
| Cessation of TAC within 6 months | 4 | 3 |
| Maintenance therapy with TAC | ||
| IM+5-ASA | 13 | 7 |
| IM | 1 | 0 |
| 5-ASA | 0 | 4 |
Numbers of patients are shown unless specified.
5-ASA, 5-aminosalicylate; CR, clinical remission; IM, immunomodulators; TAC, tacrolimus.
Intensification of IFX treatment
Of the 29 patients with severe UC, 17 patients (10 in the TAC group and 7 in the IFX group) were treated with at least more than one infusion of IFX. Nine (6 in the TAC group and 3 in the IFX group) of the 17 patients could achieve a CR after the treatment with IFX. Six (4 in the TAC group and 2 in the IFX group) of the nine patients needed the intensification of IFX treatment such as dose escalation and shortening of interval in order to maintain a CR. All the eight patients (4 in the TAC group and 4 in the IFX group) who could not achieve a CR from the treatment with IFX resulted in colectomy or were switched to TAC without intensifying IFX treatment.
Mucosal healing
During our observational periods, 27 of the 29 patients were evaluated by colonoscopy after their treatments, although the timing and frequency of colonoscopy varied among the patients. At the first endoscopic analysis after the initial treatment (median: 31 days, range: 9–1782 days), four patients in the TAC group could achieve mucosal healing. Two of the four patients had been continued with TAC treatment at the first endoscopic examination and the remaining two patients had not. At the latest endoscopic analysis after the initial treatment (median: 851 days, range: 248–2091 days), seven patients could achieve mucosal healing. One of the seven patients could achieve a CR after switching IFX to TAC and the remaining six patients could achieve a CR after treatment with TAC.
Colectomy-free survival
Of the 29 patients with severe UC, 6 patients required colectomy. One resulted in colectomy within 8 weeks after initiating IFX and 3 resulted in colectomy within 6 months after initiating TAC. The remaining two resulted in colectomy later than 6 months after initiating TAC. Based on Kaplan-Meier survival analysis, the overall cumulative colectomy-free survival was estimated to be 79.3% at 118 months (figure 2A). Moreover, the cumulative colectomy-free survival was 77.3% at 118 months (range 2–118 months) in the TAC group and 85.7% at 79 months (range 0.5–79 months) in the IFX group (p=0.704; figure 2B). Regarding the effect of the sequential therapies, 9 of 13 patients who were refractory to the initial treatments (TAC group: n=10, IFX group: n=3) responded to the sequential therapies and avoided colectomy.
Figure 2.
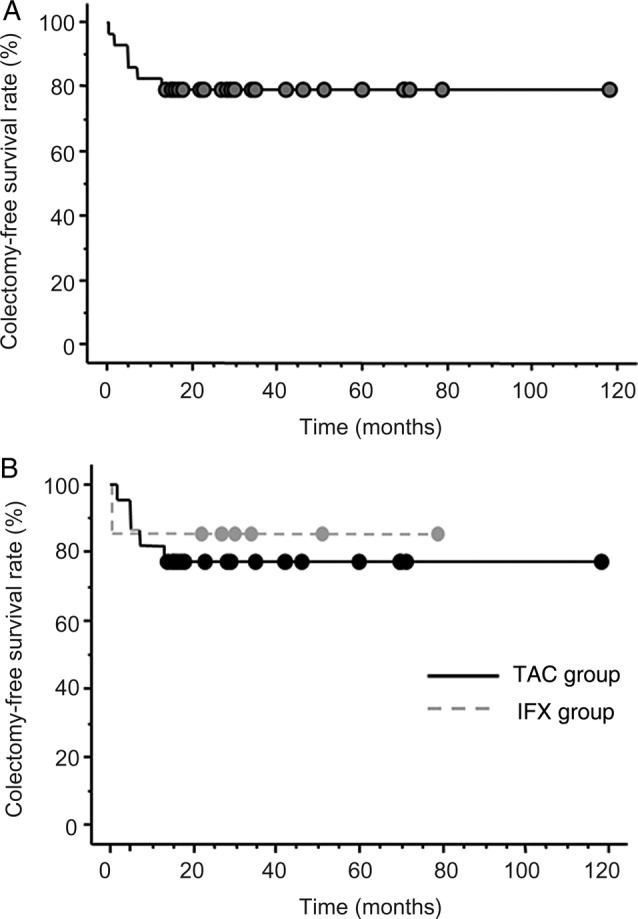
(A) Proportion of patients who avoided colectomy (n=23). The overall cumulative colectomy-free survival was estimated to be 79.3% at 118 months, based on Kaplan-Meier survival analysis. (B) Proportion of patients who avoided colectomy (n=17 in the tacrolimus (TAC) group and n=6 in the infliximab (IFX) group). The cumulative colectomy-free survival was estimated to be 77.3% at 118 months in the TAC group (solid line) and 85.7% at 79 months in the IFX group (dashed line) (p=0.704).
Predictors of colectomy
To evaluate the predictive factors for colectomy in patients with severe UC, we analysed the differences in the patient characteristics between patients with severe UC who required a colectomy (colectomy group) and those who did not (non-colectomy group; table 4). The positive rate of CMV reactivation in the colectomy group was significantly higher than that in the non-colectomy group (p=0.033). There were no significant differences between the colectomy group and non-colectomy group with regard to age, disease duration, sex, partial Mayo score, endoscopic Mayo score, disease extent, laboratory examination, daily dosage of CS and copy number of CMV-DNA. Therefore, our data suggest that positivity of colonic CMV reactivation is a predictive factor for colectomy, regardless of the copy number of CMV-DNA in the colonic mucosa.
Table 4.
Predictors in colectomy
| Colectomy | Non-colectomy | p Value | |
|---|---|---|---|
| (n=6) | (n=23) | ||
| Age at diagnosis of severe UC (median (range)) (years) | 49.5 (20–64) | 33 (19–69) | 0.153 |
| Disease duration prior to the induction therapy (median (range)) (months) | 50 (4–348) | 34 (2–157) | 0.590 |
| Gender | 0.494 | ||
| Male | 3 | 15 | |
| Female | 3 | 8 | |
| Partial Mayo score (median (range)) | 8.5 (8–9) | 9 (8–9) | 0.936 |
| Endoscopic Mayo score (median (range)) | 3 (2–3) | 3 (3–3) | 0.893 |
| Disease extent | 0.160 | ||
| Extensive | 6 | 17 | |
| Left sided | 0 | 6 | |
| Laboratory examination (mean±SD (range)) (mg/dL) | |||
| C reactive protein | 8.1±9.8 (1.2–27.1) | 6.8±6.5 (0.1–18.7) | 0.893 |
| Haemoglobin | 9.7±1.5 (7.5–11.8) | 10.4±1.8 (7.9–13.1) | 0.518 |
| Albumin | 2.7±0.6 (1.7±3.4) | 3.0±0.6 (1.8–4.0) | 0.318 |
| Daily dosage of corticosteroid prior to TAC or IFX (median (range)) (mg/day) | 17.5 (0–60) | 7.5 (0–60) | 0.647 |
| Positive rate of CMV reactivation (percentage (positive/all)) (%) | 83.3 (5/6) | 34.8 (8/23) | 0.033 |
| Copy number of CMV-DNA in patients with CMV reactivation (median (range)) (copies/μg) | 975 (320–1400) | 1300 (390–12 000) | 0.445 |
Numbers of patients are shown unless specified.
CMV, cytomegalovirus; IFX, infliximab; TAC, tacrolimus; UC, ulcerative colitis.
Adverse events
During our observational periods, no patients died and no life-threatening events occurred. In addition, opportunistic infections and reactivation of tuberculosis or hepatitis B virus were not observed in any of the 29 patients with severe UC.
Discussion
The purpose of this retrospective study was to evaluate the short-term and long-term clinical outcome of Japanese patients with severe UC treated with TAC, IFX and sequential therapies. The rate of induction of remission at 8 weeks in the TAC and IFX groups was similar. In addition, 69.2% (9/13) of patients required alternative induction regimens (so-called sequential therapies) to avoid colectomy. During this observational study, no serious complications related to these medical therapies were observed. The present data first suggest that sequential therapies could avoid colectomy in cases of severe UC failing to respond to TAC or IFX.
Patients with severe UC require a pro-active approach with either effective medical treatment or a timely surgical approach. To avoid the increasing mortality of these patients, physicians should carefully determine the therapeutic strategy depending on the patient's condition. Intravenous CS remains the first-line treatment.23 24 High-dose and prolonged exposure to CS, however, predisposes patients to increased infections and peri-operative complications such as thrombosis and anastomotic leakage.25 Thus, in patients with severe UC who did not respond to CS therapies, rescue medical therapies with either a calcineurin inhibitor or antitumour necrosis factor α antibodies are necessary.
First, we assessed the rate of induction of remission in patients with severe UC treated with TAC or IFX. Regarding the effect of IFX in hospitalised patients with severely active UC, two randomised control trials (RCTs) evaluated 56 patients and compared biological therapy with placebo. According to these RCTs, IFX tended to be superior to placebo.26 27 As for the efficacy of TAC in severely active UC, previous reports showed that CR rates in patients with severe UC at 1 and 3 months after administering TAC were 45% and 72%, respectively.9 28 Our study demonstrated that there were no differences in the CR rates in patients with severe UC at 8 weeks between the TAC and IFX groups, suggesting that the effects of TAC, a calcineurin inhibitor, are potentially similar to those of IFX on severe UC. Actually, recent RCTs revealed that the efficacies of CsA, another calcineurin inhibitor, were equivalent to those of IFX for acute patients with severe UC refractory to intravenous CS.29
Second, we assessed the efficacy and safety of sequential therapies in this study. Several studies have examined the effect of sequential therapy with alternative drugs in patients with refractory UC.13 14 30–32 Maser et al reported the efficacy of the sequential therapies in patients with UC refractory to CsA or IFX. The CR rate of the IFX-salvage group (CsA-patients with refractory UC treated with IFX) and the CsA-salvage group (IFX-refractory those with CsA) was 40% and 33%, respectively.32 In the present study, the CR rate of the IFX-salvage group (TAC-refractory, receiving IFX) and the TAC-salvage group (IFX-refractory, receiving TAC) was 60% (6/10) and 100% (3/3), respectively. Of note, all patients requiring sequential therapies had no serious adverse events. Maser's data,32 however, showed a high incidence (16%, 3/19) of serious adverse events, including one death related to infection. The different frequency of serious side effects between our study and Maser's might be due to different doses of CS with which patients in each study had been treated before starting calcineurin inhibitor or biologicals.33 However, gastroenterologists must deliberately follow-up patients with UC treated with sequential therapies to avoid adverse events as much as possible. Several studies have reported the long-term outcomes of patients with severe CS-refractory UC treated with CsA or IFX. Croft et al34 reported that the colectomy-free rate at 12 months was 42% in the CsA group and 65% in the IFX group. The 3-year colectomy-free rates ranged from 43% to 55% in the CsA group, and from 70% to 73% in the IFX group.35–37 In our study, the cumulative colectomy-free survival was 77.3% at 118 months in the TAC group and 85.7% at 79 months in the IFX group (figure 2B). Thus, sequential therapies appeared to contribute to extending the colectomy-free survival term. Moreover, the maintenance therapy, particularly after the induction therapy with TAC in severe UC, is an important issue to prevent colectomy. According to our study, long-term treatment with TAC could induce a clinically better outcome in patients with severe UC. However, further studies will be required to ascertain the efficacy and safety levels of long-term treatment with TAC in patients with refractory UC.
Next, we analysed the predictors of colectomy in this study. Our data demonstrated that positivity of CMV-DNA in the colonic mucosa was a significant predictor of colectomy. In general, CMV can lead to worsening colitis in patients with moderate-to-severe UC.38 39 Therefore, we always consider the involvement of CMV infection in patients with UC refractory to immunosuppressive therapies. We assessed the CMV-DNA in the colonic mucosa of all enrolled patients before starting TAC or IFX therapy. In the present study, however, there was no significant difference in the copy number of CMV-DNA between the two groups. Heterogeneity of patients’ characteristics might affect these discrepancies. Therefore, the relevance of the copy number of CMV-DNA is an issue to be addressed in the future. Of 13 patients who were positive for colonic CMV-DNA, 7 patients were treated with ganciclovir on the basis of physician's decision. The use of ganciclovir did not affect colectomy rate in this retrospective observational study (p=0.12, data by χ2 analysis). Because there was no difference in the CR ratio at 8 weeks between the two groups, our data suggest that optimal control of colonic inflammation could lead to UC remission despite the lack of antiviral therapy.
There are some limitations to our study, including the small sample size, heterogeneity of patients’ prior treatment history and therapeutic protocol. Despite the small number of patients, our data suggested the efficacy of sequential therapies for avoiding colectomy in patients with severe UC. However, the difference in the history of patients’ prior treatments might have affected subsequent treatment outcome. Moreover, because this study was a retrospective uncontrolled study, our current data should be assessed carefully.
Conclusions
In conclusion, our data indicate that TAC, IFX and their sequential therapies could allow some patients with severe UC to avoid colectomy, although further investigation with larger cases is necessary.
Footnotes
Contributors: NM, TY, MM and HN designed the study. NM wrote the manuscript and performed a major role in collecting patients’ data. YK, SY, TT, AM, YH, TY, MM and HN collected patients’ data and were involved in editing the manuscript. All authors read and approved the final manuscript.
Funding: This work was supported by the Japan Society for the Promotion of Science “KAKENHI” Grants-in-aid for Scientific Research (24590941, 25860532, 26460967 and 26893122), and Health and Labour Sciences Research Grants for Research on Rare and Intractable Disease from the Ministry of Health, Labour and Welfare, Japan.
Competing interests: None.
Patient consent: Obtained.
Ethics approval: Ethics committee of Kyoto University Hospital.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1.Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet 2007;369:1641–57. doi:10.1016/S0140-6736(07)60751-X [DOI] [PubMed] [Google Scholar]
- 2.Dnesen LC, Walsh AJ, Protic MN, et al. The pattern and outcome of acute severe colitis. J Crohns Colitis 2010;4:431–7. doi:10.1016/j.crohns.2010.02.001 [DOI] [PubMed] [Google Scholar]
- 3.Turner D, Walsh CM, Steinhart AH, et al. Response to corticosteroids in severe ulcerative colitis: a systematic review of the literature and a meta-regression. Clin Gastroenterol Hepatol 2007;5:103–10. doi:10.1016/j.cgh.2006.09.033 [DOI] [PubMed] [Google Scholar]
- 4.Lichtiger S, Present DH, Kornbluth A, et al. Cyclosporine in severe ulcerative colitis refractory to steroid therapy. N Engl J Med 1994;330:1841–5. doi:10.1056/NEJM199406303302601 [DOI] [PubMed] [Google Scholar]
- 5.D'Haens G, Lemmens L, Geboes K, et al. Intravenous cyclosporine versus intravenous corticosteroids as single therapy for severe attacks of ulcerative colitis. Gastroenterology 2001;120:1323–9. doi:10.1053/gast.2001.23983 [DOI] [PubMed] [Google Scholar]
- 6.Kino T, Hatanaka H, Hashimoto M, et al. FK-506, a novel immunosuppressant isolated from a Streptomyces. I. Fermentation, isolation, and physico-chemical and biological characteristics. J Antibiot (Tokyo) 1987;40:1249–55. doi:10.7164/antibiotics.40.1249 [DOI] [PubMed] [Google Scholar]
- 7.Schreiber SL, Crabtree GR. The mechanism of action of cyclosporin A and FK506. Immunol Today 1992;13:136–42. doi:10.1016/0167-5699(92)90111-J [DOI] [PubMed] [Google Scholar]
- 8.Ogata H, Matsui T, Nakamura M, et al. A randomised dose finding study of oral tacrolimus (FK506) therapy in refractory ulcerative colitis. Gut 2006;55:1255–62. doi:10.1136/gut.2005.081794 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baumgart DC, Pintoffl JP, Sturm A, et al. Tacrolimus is safe and effective in patients with severe steroid-refractory or steroid-dependent inflammatory bowel disease—a long-term follow-up. Am J Gastroenterol 2006;101:1048–56. doi:10.1111/j.1572-0241.2006.00524.x [DOI] [PubMed] [Google Scholar]
- 10.Fellermann K, Tanko Z, Herrlinger KR, et al. Response of refractory colitis to intravenous or oral tacrolimu (FK506). Inflamm Bowel Dis 2002;9:317–24. doi:10.1097/00054725-200209000-00002 [DOI] [PubMed] [Google Scholar]
- 11.Yamamoto S, Nakase H, Mikami S, et al. Long-term effect of tacrolimus therapy in patients with refractory ulcerative colitis. Aliment Pharmacol Ther 2008;28:589–97. doi:10.1111/j.1365-2036.2008.03764.x [DOI] [PubMed] [Google Scholar]
- 12.Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med 2005;353:2462–76. doi:10.1056/NEJMoa050516 [DOI] [PubMed] [Google Scholar]
- 13.Yamamoto S, Nakase H, Matsuura M, et al. Efficacy and safety of infliximab as rescue therapy for ulcerative colitis refractory to tacrolimus. J Gastroenterol Hepatol 2010;25:886–91. doi:10.1111/j.1440-1746.2009.06206.x [DOI] [PubMed] [Google Scholar]
- 14.Tsukamoto H, Tanida S, Mizoshita T, et al. Infliximab salvage therapy for patients with ulcerative colitis who failed to respond to tacrolimus. Eur J Gastroenterol Hepatol 2013;25:714–18. doi:10.1097/MEG.0b013e32835eb999 [DOI] [PubMed] [Google Scholar]
- 15.Dignass A, Eliakim R, Magro F, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 1: definitions and diagnosis. J Crohns Colitis 2012;6:965–90. doi:10.1016/j.crohns.2012.09.003 [DOI] [PubMed] [Google Scholar]
- 16.Satsangi J, Silverberg MS, Vermeire S, et al. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut 2006;55:749–53. doi:10.1136/gut.2005.082909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hanauer S, Schwartz J, Robinson M, et al. Mesalamine capsules for treatment of active ulcerative colitis: results of a controlled trial. Pentasa Study Group. Am J Gastroenterol 1993;88:1188–97. [PubMed] [Google Scholar]
- 18.Lewis JD, Chuai S, Nessel L, et al. Use of the non-invasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm Bowel Dis 2008;14:1660–6. doi:10.1002/ibd.20520 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shiga H, Miyazawa T, Kinouchi Y, et al. Life-event stress induced by the Great East Japan Earthquake was associated with relapse in ulcerative colitis but not Crohn's disease: a retrospective cohort study. BMJ Open 2013;3:e002294 doi:10.1136/bmjopen-2012-002294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jones A, McCurdy JD, Loftus EV Jr, et al. Effects of antiviral therapy for patients with inflammatory bowel disease and a positive intestinal biopsy for cytomegalovirus. Clin Gastroenterol Hepatol 2014:pii: S1542-3565(14)01391-3 Published Online First: 2 Oct 2014 doi:10.1016/j.cgh.2014.09.042 [DOI] [PubMed] [Google Scholar]
- 21.Kou T, Nakase H, Tamaki H, et al. Cytomegalovirus infection in patients with ulcerative colitis diagnosed by quantitative real-time PCR analysis. Dig Dis Sci 2006;51:1052–5. doi:10.1007/s10620-006-8006-y [DOI] [PubMed] [Google Scholar]
- 22.Yoshino T, Nakase H, Ueno S, et al. Usefulness of quantitative real-time PCR assay for early detection of cytomegalovirus infection in patients with ulcerative colitis refractory to immunosuppressive therapies. Inflamm Bowel Dis 2007;13:1516–21. doi:10.1002/ibd.20253 [DOI] [PubMed] [Google Scholar]
- 23.Jakobovits SL, Travis SP. Management of acute severe colitis. Br Med Bull 2006;75–76:131–44. doi:10.1093/bmb/ldl001 [DOI] [PubMed] [Google Scholar]
- 24.Van Assche G, Vermeire S, Rutgeerts P. Management of acute severe ulcerative colitis. Gut 2011;60:130–3. doi:10.1136/gut.2009.192765 [DOI] [PubMed] [Google Scholar]
- 25.Zitomersky NL, Verhave M, Trenor CC III. Thrombosis and inflammatory bowel disease: a call for improved awareness and prevention. Inflamm Bowel Dis 2011;17:458–70. doi:10.1002/ibd.21334 [DOI] [PubMed] [Google Scholar]
- 26.Sands BE, Tremaine WJ, Sandborn WJ, et al. Infliximab in the treatment of severe, steroid-refractory ulcerative colitis: a pilot study. Inflamm Bowel Dis 2001;7:83–8. doi:10.1097/00054725-200105000-00001 [DOI] [PubMed] [Google Scholar]
- 27.Järnerot G, Hertervig E, Friis-Liby I, et al. Infliximab as rescue therapy in severe to moderately severe ulcerative colitis: a randomized, placebo-controlled study. Gastroenterology 2005;128:1805–11. doi:10.1053/j.gastro.2005.03.003 [DOI] [PubMed] [Google Scholar]
- 28.Schmidt KJ, Herrlinger KR, Emmrich J, et al. Short-term efficacy of tacrolimus in steroid-refractory ulcerative colitis—experience in 130 patients. Aliment Pharmacol Ther 2013;37:129–36. doi:10.1111/apt.12118 [DOI] [PubMed] [Google Scholar]
- 29.Laharie D, Bourreille A, Branche J, et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: a parallel, open-label randomized controlled trial. Lancet 2012;380:1909–15. doi:10.1016/S0140-6736(12)61084-8 [DOI] [PubMed] [Google Scholar]
- 30.Chaparro M, Burgueño P, Iglesias E, et al. Infliximab salvage therapy after failure of ciclosporin in corticosteroid-refractory ulcerative colitis: a multicentre study. Aliment Pharmacol Ther 2012;35:275–83. doi:10.1111/j.1365-2036.2011.04934.x [DOI] [PubMed] [Google Scholar]
- 31.Thin LW, Murray K, Lawrance IC. Oral tacrolimus for the treatmen of refractory inflammatory bowel disease in the biologic era. Inflamm Bowel Dis 2013;19:1490–8. doi:10.1097/MIB.0b013e318281f362 [DOI] [PubMed] [Google Scholar]
- 32.Maser EA, Deconda D, Lichtiger S, et al. Cyclosporine and infliximab as rescue therapy for each other in patients with steroid-refractory ulcerative colitis. Clin Gastroenterol Hepatol 2008;6:1112–16. doi:10.1016/j.cgh.2008.04.035 [DOI] [PubMed] [Google Scholar]
- 33.Nakase H, Yoshino T, Matsuura M. Role in calcineurin inhibitors for inflammatory bowel disease in the biologics era: when and how to use. Inflamm Bowel Dis 2014;20:2151–6. doi:10.1097/MIB.0000000000000130 [DOI] [PubMed] [Google Scholar]
- 34.Croft A, Walsh A, Doecke J, et al. Outcomes of salvage therapy for steroid-refractory acute severe ulcerative colitis: ciclosporin vs. infliximab. Aliment Pharmacol Ther 2013;38:294–302. doi:10.1111/apt.12375 [DOI] [PubMed] [Google Scholar]
- 35.Mocciaro F, Renna S, Orlando A, et al. Cyclosporine or infliximab as rescue therapy in severe refractory ulcerative colitis: early and long-term data from a retrospective observational study. J Crohns Colitis 2012;6:681–6. doi:10.1016/j.crohns.2011.11.021 [DOI] [PubMed] [Google Scholar]
- 36.Arts J, D'Haens G, Zeegers M, et al. Long-term outcome of treatment with intravenous cyclosporin in patients with severe ulcerative colitis. Inflamm Bowel Dis 2004;10:73–8. doi:10.1097/00054725-200403000-00002 [DOI] [PubMed] [Google Scholar]
- 37.Moskovitz DN, Van Assche G, Maenhout B, et al. Incidence of colectomy during long-term follow-up after cyclosporine-induced remission of severe ulcerative colitis. Clin Gastroenterol Hepatol 2006;4:760–5. doi:10.1016/j.cgh.2006.04.001 [DOI] [PubMed] [Google Scholar]
- 38.Kandiel A, Lashner B. Cytomegalovirus colitis complicating inflammatory bowel disease. Am J Gastroenterol 2006;101:2857–65. doi:10.1111/j.1572-0241.2006.00869.x [DOI] [PubMed] [Google Scholar]
- 39.Roblin X, Pillet S, Oussalah A, et al. Cytomegalovirus load in inflamed intestinal tissue is predictive of resistance to immunosuppressive therapy in ulcerative colitis. Am J Gastroenterol 2011;106:2001–8. doi:10.1038/ajg.2011.202 [DOI] [PubMed] [Google Scholar]