

Abstract
Social support and collective efficacy are related to child physical abuse. However, little is known about whether these relationships differ for women and men, although mothers and fathers differ in the quantity and quality of time spent with children. This study examined whether the relationship between social support, collective efficacy, and physical abuse is stronger for mothers than fathers. Telephone interviews were conducted with parent respondents in 50 California cities (n=3,023). Data were analyzed via overdispersed multilevel Poisson models. Results suggest that high levels of emotional support were inversely associated with physical abuse for women and men, although this effect was stronger for women. High levels of companionship support were positively associated with physical abuse for women; however the opposite was true for men. There were no significant interactions between collective efficacy variables and gender. The relationships between some types of social support and physical abuse appear to vary for men and women suggesting possibilities for more targeted intervention.
Keywords: physical abuse, parental risk, gender, social support, collective efficacy
In 2012, Child Protective Services identified 124,544 child victims of physical abuse (i.e. the intentional injury of children), with the vast majority abused by their own parents (US DHHS, 2012). This number is likely an under estimate as many cases of abuse are not reported to Child Protective Services. General population estimates are approximately 4.5 times higher, suggesting that most children being physically abused are in need of intervention and services (Sedlak et al., 2010). Physical abuse is associated with mental, behavioral, or physical health problems throughout the life course such as depression, anxiety, cardiovascular disease, and suicide (Fuller-Thomson et al., 2011; McCauley et al., 1997; Springer et al., 2007). Although the literature examining perpetrators of physical abuse is mixed, recent estimates suggest that men are more likely to commit physical abuse than women, although women are more likely to commit all kinds of child maltreatment (Sedlak et al., 2010; US DHHS, 2012; Way et al., 2001). However, despite these differences, many studies examining physical abuse have focused predominately on mothers to the exclusion of fathers (Shapiro, 2010). In addition, there has been little examination of how relationships between risk factors and physical abuse might differ between mothers and fathers (Daniel et al., 2005). As a result, there is little sense of whether or how child welfare or other social service workers should design prevention or intervention strategies specifically for mothers or fathers. This represents a potential missed opportunity to provide targeted and more effective services to vulnerable families.
Social support and collective efficacy are two well-established risk factors for child maltreatment that could have different effects for mothers and fathers (Coohey, 1995; Coohey, 2000; Coulton, Korbin, & Su, 1999; Freisthler, 2006; Leventhal & Brooks-Gunn, 2000; Li, Godinet, & Arnsberger, 2011; Guterman et al., 2009; Martin, Gardner, & Brooks-Gunn, 2012; Sidebotham et al., 2006). Literature suggests that the associations between different types of social support, collective efficacy, and health outcomes may vary for women and men (Bassett & Moore, 2013; Browning et al., 2013; Dalgard et al., 2006; Kendler, Myers, & Prescott, 2005; Landman-Peeters et al., 2005; Stafford et al., 2005). Little is known, however about how gender may modify the association of these factors with physical abuse. This study expands on previous work by examining whether the relationship between social support, collective efficacy, and physical abuse differ for mothers and fathers in a general population sample, which are less frequently studied and less biased than those drawn from child welfare samples (Hill, 2006; Testa & Smith, 2009).
Gender Roles & Parenting
Gender is distinct from biological sex in that it is a formed identity continuously shaped and re-shaped by both individual experiences and interactions with the larger social environment (West & Zimmerman, 1987). Despite this distinction, in this study self-reported biological sex is used as an imperfect proxy for gender due to the influence of traditional gender roles. Gender stereotypes commonly portrayed in the media generally minimize the roles of fathers and emphasize mothers as the primary parenting relationship (Wall & Arnold, 2007). Gender is related to how parents distribute their domestic work, with women taking on more work than men (Craig & Mullan, 2011; Parker & Wang, 2013). As a result children typically spend more time with mothers than fathers, and fathers are more likely to parent with a partner. Research also suggests that that that quality of time spent with children differs for mothers and fathers, with fathers having more “playtime” with children and spending less time running errands or multi-tasking while with their children than mothers (Craig, 2006; Duocet, 2009). These differences are likely to be related to the quality of a parent’s social relationships and their interactions with the larger social and community environment (Kwan, 2000).
Gender, Social Support, and Physical Abuse
Social support is theorized to enhance well-being (Cohen & Wills, 1985) and is inversely associated with child maltreatment (Coohey, 2000; Li, Godinet, & Arnsberger, 2011; Martin, Gardner, & Brooks-Gunn, 2012; Sidebotham et al., 2006). Social support is composed of three separate domains: 1) emotional support (i.e. having close interpersonal relationships); 2) tangible support (i.e. help with financial or instrumental needs); and 3) companionship support (i.e. the presence of people to “hang out” or engage in activities with) (Cohen, 1983). All three of these domains appear to be important to parents in understanding risk of physical abuse (Coohey, 2000; Freisthler, Holmes, & Price Wolf, 2014).
Research suggests that women report higher levels of social support than men, and that social support may have different associations with outcomes for women and men (Dalgard et al., 2006; Kendler, Myers, & Prescott, 2005; Landman-Peeters et al., 2005). Despite these findings, little is known about whether these variations apply to physical abuse. There are several potential arguments for why social support might have a different relationship with physical abuse for mothers and fathers. First, gender might determine a parent’s perception of need for social support resources. Traditional social roles for women emphasize communal needs and partnership, while those for men emphasize individualism and competition (Eagly, 1987). These differences might make social support more expected and therefore more beneficial to women than men. For example, mothers with low levels of emotional support may feel more emotionally isolated than fathers with comparable levels of support, and be more likely to be abusive to their children. Second, gender might be related to actual need for support for parenting-related problems. Although the present study did not directly measure time spent with children or housekeeping duties, recent evidence suggests that while the gender gap in domestic labor is narrowing, women continue to spend more time caring for children and fulfilling household needs than men (Parker & Wang, 2013). As a result, women may have greater need for tangible support that offers assistance with childcare or child-related needs. If these needs are unmet, frustrated or overwhelmed mothers could be more likely to be physically abusive. Third, gender might be associated with the types of social relationships that parents form. Gender roles shape patterns of everyday activity and exposures to the larger community environment through occupations and opportunities, which continue to be segregated by gender (Gabriel & Schmitz, 2007). Women may have greater opportunities for parent-specific support such as “Mother’s groups”, which are often composed exclusively of mothers and could provide emotional, tangible, and companionship support for parenting-related needs (Duocet, 2009). In contrast, fathers may receive support from non-parenting related sources, which could have a weaker relationship with parenting behaviors such as physical abuse. Accordingly, I predicted that more emotional, tangible, and companionship support would be associated with less physical abuse, and that these relationships would be stronger for mothers than fathers.
Gender, Collective Efficacy, and Physical Abuse
Gender theorists have noted that contextual factors such as place shape the parenting practices of mothers and fathers (Duocet, 2009). Additionally, several studies find that environmental influences are related to higher community rates of child maltreatment (Coulton et al., 1999; Freisthler, 2004; Garbarino & Kostelny, 1992). A person’s perceptions of the quality of neighborhood social relationships also appear to play a role. One example is collective efficacy, which includes both informal social control (belief that neighborhoods will intercede against problems in the community) and social cohesion (the trust and level of social engagement of the community; Sampson et al., 2002). Informal social control and social cohesion are often studied separately as they can have dissimilar relationships to outcomes (Tendulkar et al., 2012), and are both related to child maltreatment (Coulton et al., 1999; Guterman et al., 2009). Research examining health outcomes finds that lower levels of informal social control and social cohesion may be more strongly associated with negative outcomes for women than men (Browning et al., 2013; Stafford et al., 2005).
These gender differences in the relationship between informal social control, social cohesion, and behavioral health could also be present in the case of child physical abuse. First, women and men may have different levels or types of exposure to the neighborhood environment (Bassett & Moore, 2013; Stafford et al., 2005). Initial evidence suggests that women spend more time in their local community and devote more of their time to running local household errands than men (Kwan, 2000). This increased exposure to the neighborhood environment could impact associations between collective efficacy and parenting behaviors. Women in neighborhoods with low informal social control or social cohesion could have greater exposure to negative social norms or abusive parenting behaviors, which could in turn be related to their own behavior (Portes, 1998). Second, gender could be related to the level of alarm experienced as a result of negative neighborhood environments (Ellaway & Macintyre, 2001). Women spending more time with their children in negative neighborhood environments could be more fearful if their children wander away or misbehave, and be more likely to use physically abusive punishments to control their children’s behavior (Shor, 2000). In contrast, fathers living in neighborhoods with low collective efficacy may experience less related alarm and have less exposure to their children. As a result, I predicted that higher informal social control and social cohesion would be more strongly related to less physical abuse for mothers than fathers.
Methods
Study Sample and Data Collection
Data were obtained from a population-based sample of parents or legal guardians aged 18 years or older from 50 midsized (population of 50,000–500,000) California cities. Approximately 60 respondents were sampled from each city (range 47–74). Potential participants were randomly selected from a sample list obtained from various sources (e.g. credit card or baby product companies), sent a promotional letter, and interviewed via computer assisted telephone survey. Listed sampling procedures such as the one used here are more efficient than random digit dialing in specific geographic areas and are relatively unbiased (Brick, Waksber, Kulp, & Starer, 1995; Gruenewald, Remer, & LaScala, 2014; Kempf & Remington, 2007; Tucker, Lepkowski, & Piekarski, 2002). To reduce potential non-response bias, each phone number was called up to 10 times at varying days and times, and two refusal conversions were attempted for those who were deemed eligible. Respondents received an incentive fee of $25 for participation in the approximately 30 minute survey Although the majority of the survey was conducted by a live interviewer, in order to reduce social desirability bias and prevent respondents from being reported to Child Protective Services all questions about abusive behaviors were administered via Interactive Voice Response (IVR) technology. Eligible respondents had 1 or more children aged 12 years or younger who lived with them at least 50% of the time and spoke either English or Spanish. Respondents with more than one child aged 12 or younger were asked to identify the child who had the most recent birthday and answer all questions about him or her (“focal child”). One eligible adult was randomly selected per household for participation (n=3,023). The final study response rate was 47.4%, as calculated by definitions of the American Association for Public Opinion Research (AAPOR, 2002). Previous studies found that this study sample may have a higher average income than the general population, but identified few other differences (Kepple, Freisthler, & Johnson-Motoyama, 2014). Post-stratification weights accounting for gender-specific race/ethnicity were calculated and used for all multivariate analyses.
Measures
Social Support
Social support was measured by the Interpersonal Support Evaluation List (Cohen & Hoberman, 1983), which examines tangible (e.g., If I had to go out of town for a few weeks, it would be difficult to find someone who would look after my house or apartment), emotional (e.g., I feel that there is no one I can share my most private worries and fears with), and companionship (e.g., If I wanted to have lunch with someone, I could easily find someone to join me) support. Domains had 4 items with responses ranging from 1 (Definitely False) to 4 (Definitely True). Higher scores indicate more of each support domain. Cronbach’s alpha scores for the support scales were .66 (companionship) .68 (emotional) and .59 (tangible).
Collective Efficacy
Four items from the Project on Human Development in Chicago Neighborhoods (PHDCN) community survey (Sampson et al., 1999) were used to measure individual perception of informal social control (α=.69). Items ask how likely is it that the respondent’s neighbors would step in if: 1) they knew that some of the neighborhood children were skipping school and hanging out on a street corner; 2) they saw children spray-painting graffiti on a local building; 3) there was a fight in front of their house and someone was being beaten up or threatened; 4) a child was showing disrespect to an adult. Response options were on a 5-point scale ranging from “very likely” to “very unlikely” and were summed, with higher scores indicating less informal social control (possible range 4–20). Social cohesion was measured by three items from the same survey (α=.77), and asked respondents how often people in their neighborhood: 1) did favors for each other; 2) had parties or got together with each other; 3) visit in each other’s homes or on the street. Responses were on a 4-point scale ranging from “often” to “never” and were summed (range 4–12), with higher scores indicating lower social cohesion.
Parental Physical Abuse
The frequency of child physical abuse was measured by the Parent-Child Conflict Tactics Scale (CTS-PC; Straus et al., 1998). Respondents were asked how often they practiced four abusive behaviors (e.g. hitting with a fist or kicking, throwing or knocking the child down) in the past 12 months. An additional abusive behavior (“shaking a child”) was asked when the focal child was under the age of two. Response options were categories ranging from none to more than 10 times in the past year. The internal consistency of the scale (α = .51) was similar to that found in other general population samples, where rates of physical abuse are lower than child welfare samples (Straus et al., 1998). Since the frequency categories are unevenly distributed, the midpoint of each category was summed to create a yearly frequency of physical abuse, as recommended by Straus et al. (1998). Table 1 presents the unweighted and weighted frequency of each physical abuse item for this sample. Approximately 7.6% of the sample had used any physically abusive behavior in the past year. These rates are lower than other general population samples using the CTS-PC (Straus et al., 1998), perhaps due to the over-representation of higher income respondents in the sample (Sedlak, 2010).
Table 1.
Type and Mean Frequency Scores of Physical Abuse Behaviors (N=3,023)
| Item | Unweighted number reporting any use of behavior | Weighted % of any use of behavior | Weighted mean frequency of behavior |
|---|---|---|---|
| In the past year, how often have you shook him/her? (For children younger than 2) | 66 | 2.3 | 0.26 |
| In the past year, how often have you hit him/her with a fist or kicked him/her? | 62 | 2.6 | 0.29 |
| In the past year, how often have you hit him/her on some other part of the body besides the bottom with belt, hairbrush, stick, or other hard object? | 15 | 1.0 | 0.05 |
| In the past year, how often have you slapped him/her on the face, head, or ears? | 106 | 3.4 | 0.14 |
| In the past year, how often have you threw or knocked him/her down? | 29 | 1.5 | 0.05 |
| Total Physical Abuse Scale | 185 | 7.6 | 0.54 |
Control Variables
City-level disadvantage, personality, psychosocial, and demographic variables were included in models as controls. Principal components analysis was used to compute a city-level disadvantage score from the following variables: percent of households with no vehicle, percent of families in poverty, percent of unemployment in the labor force, and percent of population with less than a high school diploma. These variables loaded onto a single factor explaining 81% percent of associated variance. Higher scores indicate greater city-level disadvantage. Parental impulsivity was measured with the Dickman Dysfuntional Impulsivity Scale (Dickman, 1990). The scale is composed of 7 items (α=.723) examining whether respondents respond quickly or inappropriately to situations without forethought (e.g., I often get into trouble because I don’t think before I act). Responses are coded as “yes” or “no”. Items were reverse coded when necessary and summed to create the scale, with higher scores indicating greater impulsivity. Two parenting stress items (α=.688) from the Dimensions of Discipline Inventory were used to assess parental stress in relation to the focal child, with higher scores indicating greater stress (e.g., in the past year, how often have you felt stressed out when your child misbehaved?; Straus & Fauchier, 2011). Characteristics of the parent and child were controlled for, including income, age, race/ethnicity, marital status, and the age and gender of the focal child. Income was categorized into 7 groups ($20,000 or less; $20,001 to $40,000; $40,001 to $60,000; $60,001 to $80,000; $80,001 to $100,000; $101,000 to $150,000; and $150,001 and higher). Categorical variables were dummy coded into African American, Hispanic/Latino, Asian American, Multi-racial or Other Race (vs. White), married or in a marriage-like relationship (vs. single/widowed/divorced), and male focal child (vs. female).
Missing Data
Only two variables (frequency of physical abuse and informal social control) had more than 4% missing values. The frequency of physical abuse had approximately 9% missing values, likely due to the sensitivity of the questions and concerns about responses being reported to child protective services. To assess the effect that these missing data may have had on analyses, a multi-level logistic regression model including all of the study variables was used to calculate the odds of not completing the physical abuse questions. Only two variables were significant: Asians were less likely to complete the physical abuse questions (compared to Whites), while those with lower incomes were more likely to complete the survey than those with higher incomes. Social control had 11% missing values, due to individuals selecting “Don’t know” in response to questions about their neighborhood. Cases with missing data were dropped from analyses.
Analysis Procedures
Post-stratification survey weights based on gender-specific race/ethnicity were created to increase study generalizability to the 50 cities. As respondents (level 1) were nested within cities (level 2), multi-level modeling was used. Additionally, the dependent variable (frequency of physical abuse, M=.54, SD=2.9) was highly skewed (skewness=9.6, SD=.047) and had a larger variance than the mean, due to large number of zeroes in the dataset (Osgood, 2000). As a result, weighted overdispersed Poisson hierarchical models were used. All multivariate analyses were conducted with the use of HLM 7.0 (Raudenbush, Bryk, & Congdon, 2011). In order to ease interpretation, all continuous variables were centered on the grand mean.
To address the hypothesis that gender would modify associations between social support, collective efficacy, and frequency of physical abuse, a sequence of overdispersed multilevel Poisson models were fit. First, an intercept only model including no predictors was created to examine between-city variation in physical abuse rates (Model 1). Second, an intercepts-and-slopes-as outcomes model was used to test associations between social support, collective efficacy (level 1) and physical abuse, while controlling for city-level disadvantage (level 2), and psychosocial and demographic characteristics of the parent and child (Model 2). Finally, multiplicative interaction variables were calculated using the product of variable values (gender grand-mean centered social support variables and gender grand-mean centered collective efficacy variables). Model 3 add red these interaction variables to Model 2. It was not possible to conduct a multivariate test of variance-covariance components using an overdispersed Poisson model, which are based on penalized quasi-likelihood estimation and not maximum-likelihood estimation (Raudenbush et al., 2011). The population average models with robust standard errors were examined and statistical significance was evaluated at the p<=.05 level.
Results
Descriptive and Bivariate Results
Descriptive characteristics of the sample are presented in Table 2. Chi-square and independent samples t-tests were used to identify differences between women and men on key study variables. Men compared to women had an older focal child (t[3022]=−2.131, p=.033), lower parenting stress (t[3022]=3.769, p<.01), lower emotional support (t[2988]=4.246, p<.01), and lower social cohesion scores (t[3006]=2.224, p=.026). Women had higher tangible support scores than men (t[2995]=−2.157, p=.031). These differences were generally very small.
Table 2.
Descriptive Characteristics of the Overall Sample, Women, and Men
| Overall Sample (N=3023) | Women (n=1973) | Men (n=1050) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable Name | N | Unweighted % or M (SD) | Weighted % or M (SD) | N | Unweighted % or M (SD) | Weighted% or M (SD) | N | Unweighted % or M (SD) | Weighted % or M (SD) |
| Focal Child | |||||||||
| Male | 1495 | 49.5 | 48.8 | 981 | 51.8 | 50.6 | 514 | 50.5 | 50.9 |
| Female | 1414 | 46.8 | 47.3 | 911 | 48.2 | 49.4 | 503 | 49.5 | 49.1 |
| Age | 3023 | 6.7 (3.6) | 6.9 | 1973 | 6.6 (3.6) | 6.8 (3.6) | 1050 | 7.0 (3.5) | 7.0 (3.4) |
| Caregiver | |||||||||
| Under 30 | 404 | 13.4 | 14.0 | 332 | 16.8 | 18.3 | 72 | 6.9 | 9.3 |
| 31–45 | 1891 | 62.6 | 60.8 | 1255 | 63.6 | 60.9 | 636 | 60.6 | 60.7 |
| 46+ | 728 | 24.1 | 25.2 | 386 | 19.6 | 20.8 | 342 | 32.6 | 30.0 |
| White | 1753 | 58.0 | 52.4 | 1120 | 56.9 | 45.3 | 633 | 60.3 | 49.3 |
| Asian | 236 | 7.8 | 9.3 | 131 | 6.7 | 8.7 | 105 | 10.1 | 10.1 |
| Black | 111 | 3.7 | 6.1 | 78 | 4.0 | 6.5 | 33 | 3.2 | 5.7 |
| Hispanic | 733 | 24.2 | 32.5 | 528 | 26.8 | 34.2 | 205 | 19.7 | 30.7 |
| Multi-Racial | 92 | 3.0 | 2.7 | 56 | 2.8 | 3.3 | 36 | 3.5 | 2.2 |
| Other | 84 | 2.8 | 1.8 | 56 | 2.8 | 2.1 | 28 | 2.7 | 1.6 |
| Married/Cohabitating | 2673 | 88.4 | 74.3 | 1681 | 85.2 | 67.3 | 992 | 94.5 | 82.0 |
| Single | 350 | 11.6 | 25.7 | 292 | 14.8 | 32.7 | 58 | 5.5 | 18.0 |
| Income | |||||||||
| ≤ $20,000 | 258 | 8.9 | 10.9 | 221 | 11.7 | 15.3 | 37 | 3.6 | 7.0 |
| $20,001 – $40,000 | 358 | 12.3 | 16.7 | 262 | 13.9 | 19.9 | 96 | 9.4 | 14.5 |
| $40,001 – $60,000 | 373 | 12.8 | 14.4 | 251 | 13.3 | 14.8 | 122 | 11.9 | 15.1 |
| $60,001 – $80,000 | 450 | 15.5 | 14.0 | 284 | 15.1 | 12.8 | 166 | 16.3 | 16.2 |
| $80,001 – $100,000 | 412 | 14.2 | 12.6 | 263 | 13.9 | 12.2 | 149 | 14.6 | 14.0 |
| $100,001 – $150,000 | 648 | 22.3 | 16.9 | 391 | 20.7 | 16.0 | 257 | 25.2 | 19.0 |
| $150,001 + | 409 | 14.1 | 11.1 | 215 | 11.4 | 8.9 | 194 | 18.5 | 14.2 |
| Impulsivity | 2975 | 0.7 (1.3) | 0.8 | 1940 | 0.8 (1.3) | 0.8 (1.3) | 1035 | 0.7 (1.4) | 0.7 (1.3) |
| Parenting Stress | 3023 | 4.1 (1.7) | 4.0 | 1973 | 4.2 (1.7) | 4.1 (1.7) | 1050 | 3.9 (1.6) | 3.9 (1.6) |
| Companion Support | 2993 | 14.1 (2.1) | 14.1 | 1952 | 14.1 (2.2) | 14.0 (2.2) | 1041 | 14.2 (2.0) | 14.1 (2.2) |
| Tangible Support | 2995 | 14.5 (2.0) | 14.4 | 1954 | 14.4 (2.1) | 14.3 (2.1) | 1041 | 14.6 (1.8) | 14.5 (2.0) |
| Emotional Support | 2995 | 14.9 (1.9) | 14.7 | 1958 | 14.9 (1.9) | 14.9 (1.9) | 1037 | 14.8 (2.0) | 14.5 (2.2) |
| Social Control | 2753 | 7.7 (3.0) | 7.9 | 1794 | 7.7 (3.0) | 7.9 (3.3) | 959 | 7.7 (3.0) | 8.1 (3.1) |
| Social Cohesion | 3010 | 6.6 (2.4) | 6.8 | 1964 | 6.7 (2.5) | 6.9 (2.5) | 1046 | 6.4 (2.2) | 6.7 (2.3) |
Note. Significant differences between men and women are bolded (p<.05)
Multivariate Results
To ease interpretation of results, Incidence Rate Ratios (IRR), which represent the percentage of increase or decrease in the expected number of incidents of physical abuse in a year due to each independent variable (given the baseline or reference of covariates) were calculated by exponentiating the Poisson coefficients. The null model (Model 1) estimated the variance of physical abuse at the city level (level 2). The city-level variance was 0.84 (p<.001), indicating significant differences in physical abuse between cities. The IRR for the Model 1 intercept represents the mean frequency of physical abuse in the sample (IRR=0.55, 95% CI [0.36, 0.83]).
The results for Models 2 and 3 are presented in Table 3. Model 2 examines main effects of level 1 and 2 variables, without any interaction terms. There was no statistically significant difference in frequency of physical abuse between women and men. Among the key independent variables, more emotional support was associated with lower frequency of physical abuse, indicating that having an emotional support score one unit above the mean was associated with a 20% reduction in predicted instances of physical abuse. While this relationship was as predicted, contrary to expectations, tangible support, companionship support, informal social control and social cohesion were not associated with physical abuse. Among the control variables, an older focal child, being African American (compared to White), having greater levels of parenting stress, more impulsivity, and living in more disadvantaged cities were associated with higher frequency of physical abuse. Being married or cohabitating (versus single) was associated with lower frequency of physical abuse in Model 2.
Table 3.
Incidence Rate Ratios from Multi-level Poisson Regressions for the Independent Effects of Social Support and Collective Efficacy (Model 2) and Social Support, Collective Efficacy and Gender Interactions (Model 3) on Child Physical Abuse
| Model 2 | Model 3 | |||
|---|---|---|---|---|
| Variable Name (reference group) | IRR | CI (p) | IRR | CI (p) |
| Intercept | 0.32 | (0.08,1.17) | 0.24 | (0.04,1.32) |
| Level 1: Parent Level | ||||
| Control Variables | ||||
| Male Focal Child (Female) | 1.19 | (0.58,2.43) | 1.16 | (0.71,1.89) |
| Age, Focal Child | 1.14 | (1.08,1.21) *** | 1.16 | (1.10,1.22) *** |
| Men (Women) | 0.81 | (0.42,1.54) | 1.038 | (0.60,1.77) |
| Parental Age (30 and under) | ||||
| 31–44 | 2.00 | (0.65,6.11) | 2.21 | (0.55,8.87) |
| 45+ | 0.79 | (0.29,2.15) | 0.80 | (0.20,3.14) |
| Married/Cohabitating (Single) | 0.36 | (0.18,0.70) ** | 0.36 | (0.18,0.72) ** |
| Race/Ethnicity | ||||
| Asian American | 1.41 | (0.33,5.91) | 0.92 | (0.18,4.55) |
| African American | 4.37 | (1.62,11.78) ** | 4.51 | (2.60,7.82) *** |
| Hispanic | 0.72 | (0.40,1.29) | 0.75 | (0.43,1.31) |
| Multi-racial | 0.180 | (0.01,2.09) | 0.44 | (0.11,1.77) |
| Other race | 0.90 | (0.31,2.55) | 1.04 | (0.35,3.02) |
| Income | 1.13 | (0.85,1.49) | 1.13 | (0.86,1.47) |
| Impulsivity | 1.33 | (1.12,1.58) *** | 1.29 | (1.12,1.48) *** |
| Parenting Stress | 1.23 | (1.13,1.33) *** | 1.21 | (1.11,1.32) *** |
| Type & Quantity of Social Support | ||||
| Tangible | 0.93 | (0.84,1.04) | 0.99 | (0.88,1.12) |
| Emotional | 0.80 | (0.71,0.91) *** | 0.67 | (0.57,0.79) *** |
| Companionship | 1.10 | (0.89,1.36) | 1.43 | (1.12,1.83) *** |
| Collective Efficacy | ||||
| Informal Social Control | 1.07 | (0.99,1.17) | 1.04 | (0.94,1.15) |
| Social Cohesion | 1.02 | (0.90,1.15) | 0.97 | (0.81,1.15) |
| Interactions | ||||
| Tangible* Gender | 0.95 | (0.72,1.26) | ||
| Emotional* Gender | 1.39 | (1.04,1.85) * | ||
| Companionship* Gender | 0.58 | (0.36,0.92) * | ||
| Informal Social Control* Gender | 1.07 | (0.94,1.23) | ||
| Social Cohesion* Gender | 1.16 | (0.96,1.39) | ||
| Level 2: City Level | ||||
| Disadvantage Score | 1.45 | (1.04,2.01) * | 1.40 | (1.06,1.85) * |
| City-level variance (sd) | 0.45 (0.67) | 0.00 (0.01) | ||
| Wald χ2 (df) | 116.31 (48) *** | 26.09(48) | ||
Note. For social support variables, increasing scores mean higher levels of support. For collective efficacy variables, increasing scores mean lower perceived social control or social cohesion. IRR= Incidence Rate Ratio.
p<.05,
p<.01,
p<.001
Interactions between gender and social support variables and gender and collective efficacy variables were added in Model 3. As predicted there were significant gender by emotional support and gender by companionship support interactions, with the latter interaction being contrary to expectation. As displayed in Figure 1, the absence or presence of emotional support was more highly related to physical abuse (i.e. a steeper slope) for women in comparison to men. As shown in Figure 2, for women, low companionship support was associated with lower frequency of physical abuse than high companionship support. The opposite was true for men, for whom low companionship support was associated with higher frequency of physical abuse than high companionship support. An additional model (Model 4, not shown) was created to examine if these two interactions were still significant after removing non-significant interactions from the model. Both interactions remained significant at the p<.05 level and the direction, size, and interpretation of the interactions were virtually unchanged. Contrary to the study hypotheses, there were no interaction effects between gender and tangible support, and gender and either of the collective efficacy variables.
Figure 1.
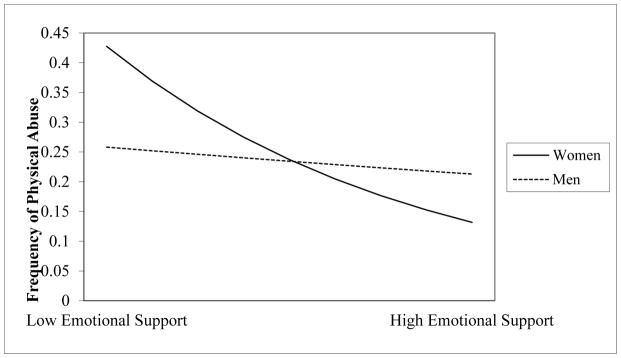
Interaction between emotional support and gender on frequency of physical abuse
Note. Low and high values represent one standard deviation above and below the population mean, respectively.
Figure 2.

Interaction between companionship support and gender on frequency of physical abuse
Note. Low and high values represent one standard deviation above and below the population mean, respectively.
Discussion
Although research suggests that gender moderates the effect of social support and collective efficacy on physical health, mental health, or behavioral outcomes, the current study represents one of the first to directly investigate gender-based moderation of these variables in relation to the physical abuse of children. It was predicted that high levels of social support and collective efficacy would be related to less frequent physical abuse, and that these associations would be stronger for women. These predictions were partially supported by the data. Only emotional support was significantly associated with lower frequency of physical abuse whereas other types of support and efficacy were not. As predicted, high levels of emotional support were more strongly related to less physical abuse for women than men. Unexpectedly, high levels of companionship support were associated with greater frequency of physical abuse for women, while the opposite was true for men.
Somewhat surprisingly, there was no significant difference in frequency of physical abuse between men and women. This is in contrast to data from the Fourth National Incidence Study of Child Abuse and Neglect (NIS-4), which found that children are more likely to be physically abused by men than women. The NIS-4, however, is a sample of children identified as maltreated by social service providers and the child welfare system. This focus on maltreated children could lead to an artificial association between parental gender and physical abuse. For example, it could be that due to greater physical strength and size, cases of physical abuse perpetrated by men compared to women are more likely to produce severe injuries in children (Starling & Holden, 2000), potentially making them more easily identifiable to social services professionals. In contrast, the current study, which relies on parental self-report in a general population sample, may better represent all cases of physical abuse, regardless of the severity of the injury. Alternatively, there may be other gender-based differences in the relationships between individual or neighborhood risk factors and physical abuse that were untested in this study, potentially masking true differences in rates of physical abuse. For example, the association between child age and physical abuse may differ for mothers and fathers (Strauss et al., 1998). Finally, there could be gender-related bias in survey completion or the self-report of physically abusive behaviors. However, a previous analysis using this dataset found no differences between men and women in whether or not a parent completed the child abuse questions (Kepple, Freisthler, & Motoyama-Johnson, 2014)and IVR technology was used to help reduce social desirability bias. Given the mixed findings regarding the gender of those perpetrating physical abuse (Sedlak et al., 2010; Straus et al., 1998) more research from representative population based studies is needed to help assess whether and under what conditions mothers or fathers are more likely to physically abuse their children.
Social Support
There was no main effect association between tangible support and frequency of physical abuse, which is in contrast to other research on child maltreatment (Coohey, 1996, 2000, DePanfilis, 1996; Ortega, 2002; Polansky et al., 1985; Thompson. 1985). This could be potentially due to higher average incomes in the sample, as more wealthy parents may have less tangible needs, thereby weakening or eliminating the relationship between tangible support and physical abuse. In addition, the interaction between tangible support and gender was not significant. The hypothesis that tangible support would be more strongly related to physical abuse for women than men due to increased childcare duties and need for child-related assistance was consequently unfounded. However, the questions used in the current study measure general tangible support and do not take into account parenting-specific tangible assistance. Measures that focus exclusively on types of tangible assistance that benefit parents specifically, such as carpooling, childcare, and assistance with paying for child-related items, could potentially have a stronger relationship with physical abuse for women. It is also possible, however, that tangible support has no added effect on frequency of physical abuse while controlling for emotional support and companionship support, and that this does not vary by gender.
While more emotional support was inversely associated with physical abuse for the overall sample, a significant gender by emotional support interaction suggests that this effect may be stronger for women than men. This finding is similar to literature which found that social support may be more beneficial for women than men for other outcomes (Dalgard et al., 2006; Landman-Peeters et al., 2005). Women report higher levels of emotional support than men and may view social relationships as more important than men (Eagly, 1987; Kendler, Myers, & Prescott, 2005). As a result, emotional support could have weaker beneficial impact for men. Another possibility is that there are differences in the types of emotionally supportive relationships parents engage in. Women may have more access to “mother’s groups” and relationships with other parents due to their increased time spent with children (Duocet, 2009). These relationships might provide emotional support (advice, listening, and empathy about parenting challenges and discipline techniques) that is more strongly related to lower frequency of physical abuse than other types of global emotional support. Given the rich literature suggesting that social support can buffer against the negative effects of stress (see Cohen & Wills, 1985), it may be that women with low levels of emotional support may be more vulnerable to stressors than men with low levels of emotional support, which could in turn raise risk of physical abuse. Due to the lack of an overall stress scale in these data, a stress-buffering hypothesis was not tested. However, future research could help further examine potential mechanisms by investigating whether emotional support moderates the relationship between stress and physical abuse, and if this relationship differs for mothers and fathers.
The relationship between companionship support and physical abuse also appears to be conditional on gender. High companionship support was related to greater frequency of physical abuse for women and lower frequency of physical abuse for men. The opposite was true at levels of low companionship support. Higher companionship support could create stress instead of promoting resilience and well-being for women. While research in this area is limited, examinations of other measures of social relationships have found that larger social networks introduce stressors (Felton & Berry, 1992). More opportunities for socializing may consequently be draining instead of rejuvenating for women, who could already be coping with increased childcare and household duties. Alternatively, women who physically abuse their children more frequently could also be more likely to pursue social activities as a way of finding respite from parenting duties. In contrast, greater companionship support may have positive effects for men. Engaging in leisure activities could provide men with opportunities to relieve stress or enhance well-being. These potential explanations are purely speculative, however, as the current findings are contrary to the study hypothesis and research specifically examining this type of support is limited and mixed (Freisthler et al., 2014; DePanfilis, 1996). While these initial findings suggest that social companionship may have varying effects on child physical abuse for men and women, they should be followed by future research that is better able to parse out positive and negative aspects of social relationships.
Collective Efficacy
It was predicted that two components of collective efficacy, informal social control and social cohesion, would be associated with frequency of physical abuse, as has been the case in other studies of child maltreatment (Coulton, Korbin, & Su, 1999; Guterman et al., 2009). Contrary to this hypothesis, there were no main effects for either dimension of collective efficacy. It could be that due to higher average incomes, fewer individuals in this sample live in neighborhoods with significant socioeconomic disadvantage as compared to studies specifically examining vulnerable or at-risk families (Guterman et al., 2009). As a result, informal social control and social cohesion could have a weaker relationship with physical abuse. However, greater city-level disadvantage was associated with frequency of physical abuse, suggesting that while collective efficacy was not significant, the larger environment is related to physical abuse. Additionally, although previous literature has suggested that the relationship between collective efficacy and physical abuse differs by gender, this was not the case in these data. It is possible that the hypothesized mechanisms that might lead to gender differences (e.g., varying time spent in the neighborhood, different perceptions about neighborhoods and related stress) might either be incorrect or did not apply to this sample.
While studies have found that collective efficacy and neighborhood characteristics are related to maltreatment, these static effects tend to be small (Coulton et al., 1999) and may be predominately filtered through individually measured risk factors like stress (Guterman, 2009). Additionally, parents (particularly those that work full-time) may spend much of their time outside of their own neighborhood (Kwan, 2000), potentially decreasing the strength of relationships between neighborhood effects and child physical abuse. Research suggests that taking into account a person’s individual travel patterns, or “activity spaces”, may allow for differentiated evaluations of risk that more accurately reflect how exposures to negative environments are experienced (Golledge & Stimson, 1997). Future work should take a dynamic perspective of the interaction between individuals and their environments, as well as how these factors relate to child physical abuse.
Limitations
Although one of the strengths of this study is the use of a population-based sample, the study response rate (47.4%) raises questions about the generalizability of results. To help address this concern data were weighted by gender-specific race/ethnicity. However, as noted previously, this sample may have higher average incomes than the general U.S. population. Consequently, these findings may underestimate the prevalence of physical abuse, which is more frequent in lower income populations. As a result, findings should be considered exploratory until they can be replicated with more representative datasets. Another potential concern is the self-reporting of abusive behaviors. To address this, IVR was used to collect data on abusive behaviors. While it is not possible to gauge the presence of deceptive answers or under-reporting in the data, other analyses from this sample found few differences between those who dropped out of the IVR portion of the survey compared to those who completed it (Kepple, Freisthler, & Johnson-Motoyama, 2013). However, under-reporting may also be present due to the selection of one “focal child” for the physical abuse questions, as a parent may abuse one child and not another. While potential mechanisms for relationships have been discussed, causal inferences cannot be made from this study due to a cross-sectional and correlational design. Finally, this study uses self-reported gender as a proxy for many highly related but distinct constructs, including gender roles, gender roles socialization, and parenting duties. As a result, these findings likely simplify a series of complex phenomena and should be supplemented by analyses better able to test specific mechanisms by which gender variables might moderate relationships between social support, collective efficacy and physical abuse.
Implications
These findings have several implications for direct and community-based practice. While interventions boosting emotional support for parents could be helpful, particularly for women, not all social relationships are positive. Interventions that increase companionship support without attention to the quality of relationships may have unintended harms, particularly for mothers. Practitioners working with families at risk of abuse or with a history of abuse might ask families to identify the different supportive relationships in their lives and assess how they might protect against or increase risk of physical abuse.
The finding that only companionship support had opposite associations with child abuse for mothers and fathers is encouraging, as it indicates that most individual or community-based interventions do not need to take into account substantial gender differences. Instead, interventions can focus on including fathers, who are often overlooked by child welfare workers as potential resources for positive change (Daniel & Taylor, 2001), even though the majority of single mothers in the child welfare system have some type of male involvement in their family life (Bellamy, 2009). Although fathers can be difficult to engage in risk reducing programs (Duggan et al., 2004), their inclusion could result in enhanced beneficial outcomes for children and families (Lewis & Lamb, 2003; Lindhahl, 2008).
Acknowledgments
The preparation of this paper was supported by a grant from the National Institute on Alcohol Abuse and Alcoholism (P60-AA006282).
Footnotes
The content is solely the responsibility of the author and does not necessarily represent the official views of the NIAAA or the National Institutes of Health.
References
- American Association for Public Opinion Research. Standard definitions: Final dispositions of case codes & outcome rates for surveys. AAPOR; Ann Arbot, MI: 2002. [Google Scholar]
- Bassett E, Moore S. Gender differences in the social pathways linking neighborhood disadvantage to depressive symptoms in adults. PLOS One. 2013;8(10) doi: 10.1371/journal.pone.0076554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bellamy J. A national study of male involvement among families in contact with the child welfare system. Child Maltreatment. 2009;14(3) doi: 10.1177/1077559508326288. [DOI] [PubMed] [Google Scholar]
- Brick JM, Waksberg J, Kulp D, Starer A. Bias in list-assisted telephone samples. Public Opinion Quarterly. 1995;59:218–235. [Google Scholar]
- Browning CR, Soller B, Gardner M, Brooks-Gunn J. “Feeling disorder” as a comparative and contingent disorder: gender, neighborhood conditions, and adolescent mental health. Journal of Health and Social Behavior. 2013;54(3):296–314. doi: 10.1177/0022146513498510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Hoberman H. Positive events and social supports as buffers of life change stress. Journal of Applied Social Psychology. 1983;13:99–125. [Google Scholar]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98(2):310–357. [PubMed] [Google Scholar]
- Coohey C. Neglectful mothers, their mothers, and partners: The significance of mutual aid. Child Abuse & Neglect. 1995;19:885–889. doi: 10.1016/0145-2134(95)00051-9. [DOI] [PubMed] [Google Scholar]
- Coohey C. Child maltreatment: Testing the social isolation hypothesis. Child Abuse & Neglect. 1996;20:241–254. doi: 10.1016/s0145-2134(95)00143-3. [DOI] [PubMed] [Google Scholar]
- Coohey C. The role of friends, in-laws, and other kin in father-perpetrated child physical abuse. Child Welfare. 2000;79(4):373–402. [PubMed] [Google Scholar]
- Coulton C, Korbin J, Su M. Neighborhoods and child maltreatment: a multi-level study. Child Abuse & Neglect. 1999;23(11):1019–1040. doi: 10.1016/s0145-2134(99)00076-9. [DOI] [PubMed] [Google Scholar]
- Craig L. Does father care mean fathers share?: A comparison of how mothers and fathers spend time with children. Gender & Society. 2006;20(2):259–81. [Google Scholar]
- Craig L, Mullan K. How mothers and fathers share childcare: A cross-national time-use comparison. American Sociological Review. 2011;76(6):834–861. [Google Scholar]
- Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, et al. Negative life events, social support and gender differences in depression. Social Psychiatry & Psychiatric Epidemiology. 2006;41:44–451. doi: 10.1007/s00127-006-0051-5. [DOI] [PubMed] [Google Scholar]
- Daniel B, Featherstone B, Hooper CA, Scourfield J. Why gender matters for Every Child Matters. The British Journal of Social Work. 2005;35(8):1343–1355. [Google Scholar]
- Daniel B, Taylor J. Engaging with fathers: Practice issues for health and social care. London: Jessica Kingsley; 2001. [Google Scholar]
- DePanfilis D. Social isolation of neglectful families: A review of social support assessment and intervention models. Child Maltreatment. 1996;1:37–52. [Google Scholar]
- Dickman SJ. Functional & dysfuntional impulsivity: personality & cognitive correlates. Journal of Perspectives on Social Psychology. 1990;58:95–102. doi: 10.1037//0022-3514.58.1.95. [DOI] [PubMed] [Google Scholar]
- Duggan A, Fuddy L, Burrell L, Higman SM, McFarlane E, Windham A, et al. Randomized trial of a statewide home visiting program: impact in reducing parental risk factors. Child Abuse & Neglect. 2004;28:623–643. doi: 10.1016/j.chiabu.2003.08.008. [DOI] [PubMed] [Google Scholar]
- Duocet A. Gender equality and gender differencecs: Parenting, habitus, and embodiment (The 2008 Porter lecture) Canadian Review of Sociology. 2009;46(2):103. doi: 10.1111/j.1755-618x.2009.01206.x. [DOI] [PubMed] [Google Scholar]
- Eagly A. Sex differences in social behavior: a social-role interpretation. L. Erlbaum Associates; 1987. [Google Scholar]
- Ellaway A, Macintyre S. Women in their place. Gender and perceptions of neighborhoods and health in the West of Scotland. In: Dyck I, Davis Lewis N, McLafferty S, editors. Geographies of women’s health. London: Routledge; 2001. pp. 265–281. [Google Scholar]
- Felton BJ, Berry CA. Do the sources of the urban elderly’s social support determine its psychological consequences? Psychology and Aging. 1992;7:89–97. doi: 10.1037//0882-7974.7.1.89. [DOI] [PubMed] [Google Scholar]
- Freisthler B, Holmes M, Price Wolf J. The dark side of social support: Understanding the role of social support, drinking behaviors and alcohol outlets for child physical abuse. Child Abuse & Neglect. 2014;38:1106–1119. doi: 10.1016/j.chiabu.2014.03.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freisthler B, Merritt DH, LaScala E. Understanding the ecology of child maltreatment: A review of the literature and directions for future research. Child Maltreatment. 2006;11(3):263–280. doi: 10.1177/1077559506289524. [DOI] [PubMed] [Google Scholar]
- Freisthler B, Midanik LT, Gruenewald PJ. Alcohol outlets and child physical abuse and neglect: Applying routine activities theory to the study of child maltreatment. Journal of Studies on Alcohol and Drugs. 2004;65(5) doi: 10.15288/jsa.2004.65.586. [DOI] [PubMed] [Google Scholar]
- Fuller-Thomson E, Brennenstuhl S, Frank J. The association between childhood physical abuse and heart disease in adulthood: Findings from a representative community sample. Child Abuse & Neglect. 2011;34(9):689–698. doi: 10.1016/j.chiabu.2010.02.005. [DOI] [PubMed] [Google Scholar]
- Gabriel P, Schmitz S. Gender differences in occupational distributions among workers. Monthly Labor Review 2007 [Google Scholar]
- Garbarino J, Kostelny K. Child maltreatment as a community problem. Child Abuse and Neglect. 1992;16:455–464. doi: 10.1016/0145-2134(92)90062-v. [DOI] [PubMed] [Google Scholar]
- Golledge RG, Stimson RJ. Spatial behavior: A geographic perspective. New York, NY: Guilford Press; 1997. [Google Scholar]
- Guterman NB, Lee Y, Waldfogel J, Rathouz PJ. Fathers and maternal risk for physical child abuse. Child Maltreatment. 2009;14(3) doi: 10.1177/1077559509337893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gruenewald PJ, Remer L, LaScala EA. Testing a social ecological model of alcohol use: The California 50-city study. Addiction. 2014 doi: 10.1111/add.12438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill RB. Synthesis of research on disproportionality in child welfare: An update: Casey-CSSP Alliance for Racial Equity in the Child Welfare System. 2006. [Google Scholar]
- Kempf AM, Remington PL. New challenges for telephone survey research in the Twenty-First century. Annual Review of Public Health. 2007;28:113–126. doi: 10.1146/annurev.publhealth.28.021406.144059. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Myers J, Prescott CA. Sex differences in the relationships between social support and risk for major depression: A longitudinal study of opposite-sex twin pairs. American Journal of Psychiatry. 2005;162(2):250–256. doi: 10.1176/appi.ajp.162.2.250. [DOI] [PubMed] [Google Scholar]
- Kepple N, Freisthler B, Johnson-Motoyama M. Bia in child maltreatment self-reports using interactive voice response (IVR) Child Abuse & Neglect. 2014 doi: 10.1016/j.chiabu.2014.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwan MP. Gender differences in space-time constraints. Area. 2000;32(2):145–156. [Google Scholar]
- Landman-Peeters KMC, Hartman CA, van der Pompe G, den Boer JA, Minderaa RB, Ormel J. Gender differences in the relation between social support, problems in parent-offspring communication, and depression and anxiety. Social Science & Medicine. 2005;60(11):2549–2559. doi: 10.1016/j.socscimed.2004.10.024. [DOI] [PubMed] [Google Scholar]
- Leventhal T, Brooks-Gunn J. The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychological Bulletin. 2000;126(2):309–337. doi: 10.1037/0033-2909.126.2.309. [DOI] [PubMed] [Google Scholar]
- Lewis C, Lamb ME. Fathers’ influences on children’s development: The evidence from two-parent families. European Journal of Psychology of Education. 2003;18(2):211–228. [Google Scholar]
- Li F, Godinet MT, Arnsberger P. Protective factors among families with children at risk of maltreatment. Child and Youth Services Review. 2011;33:139–148. [Google Scholar]
- Lindahl BW, Tollefson D, Risser H, Lovejoy MC. A meta-analysis of father involvement in parent training. Research in Social Work Practice. 2008;18:2. [Google Scholar]
- Martin A, Gardner M, Brooks-Gunn J. The mediated and moderated effects of family support on child maltreatment. Journal of Family Issues. 2012;33(7):920–941. doi: 10.1177/0192513X11431683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCauley J, Kern DE, Kolodner K, Dill L, Schroeder AF, DeChant HK, et al. Clinical characteristics of women with a history of childhood abuse: Unhealed wounds. JAMA. 1997;277(17):1362–1368. [PubMed] [Google Scholar]
- Ortega DM. How much support is too much? Parenting efficacy and social support. Children and Youth Services Review. 2002;24(11):853–876. [Google Scholar]
- Osgood DW. Poisson-based regression analysis of aggregate crime rates. Journal of Quantitative Criminology. 2000;16(1) [Google Scholar]
- Parker K, Wang W. Modern parenthood: Roles of moms and dads converge as they balance work and family. Washington, D.C: Pew Research Center; 2013. [Google Scholar]
- Polansky NA, Ammons PW, Gaudin JM. Loneliness and isolation in child neglect. Social Casework: The Journal of Contemporary Social Work. 1985;6:38–47. [Google Scholar]
- Portes A. Social capital: Its origins and applications in modern sociology. Annual Review of Sociology. 1998;24:1–24. [Google Scholar]
- Raudenbush SW, Bryk AS, Cheong YF, Congdon RT, du Toit M. HLM 7: Hierarchical linear & nonlinear modeling. LIncolnwood, IL: Scientific Software International, Inc; 2011. [Google Scholar]
- Raudenbush SW, Bryk AS, Congdon R. HLM 7 for Windows [Computer software] Skokie, IL: Scientific Software International, Inc; 2011. [Google Scholar]
- Sampson RJ, Morenoff JD, Earls F. Beyond social capital: Spatial dynamics of collective efficacy for children. American Sociological Review. 1999;64:633–660. [Google Scholar]
- Sampson RJ, Morenoff JD, Gannon-Rowley T. Assessing “neighborhood effects”: social processes and new directions in research. Annual Review of Sociology. 2002;28:443–478. [Google Scholar]
- Shor R. Child maltreatment: differences in perceptions between parents in low income and middle income neighborhoods. The British Journal of Social Work. 2000;30(2):165–178. [Google Scholar]
- Sedlak AJ, Metternburg J, Besena M, Petta I, McPherson K, Greene A, et al. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to Congress. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families; 2010. [Google Scholar]
- Shapiro A, Krysik J. Finding fathers in social work research and practice. Journal of Social Work Values and Ethics. 2010;20(1) [Google Scholar]
- Sidebotham P, Heron J, Team AS. Child maltreatment in the “children of the nineties”: a cohort study of risk factors. Child Abuse & Neglect. 2006;30(5):497–522. doi: 10.1016/j.chiabu.2005.11.005. [DOI] [PubMed] [Google Scholar]
- Sperry DM, Widom CS. Child abuse and neglect, social support, and psychopathology in adulthood: A prospective investigation. Child Abuse & Neglect. 2013;37(6):415–425. doi: 10.1016/j.chiabu.2013.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Springer KW, Sheridan J, Kuo D, Carnes M. Long-term physical and mental health consequences of childhood physical abuse: Results from a large population-based sample of men and women. Child Abuse & Neglect. 2007;31(5):517–530. doi: 10.1016/j.chiabu.2007.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stafford M, Cummins S, Macintyre S, Ellaway A, Marmot M. Gender differences in the associations between health and neighborhood environment. Social Science & Medicine. 2005;60(8):1681–1692. doi: 10.1016/j.socscimed.2004.08.028. [DOI] [PubMed] [Google Scholar]
- Starling SP, Holden JR. Perpetrators of abusive head trauma: a comparison of two geographic populations. Southern Medical Journal. 2000;93(5):463–465. [PubMed] [Google Scholar]
- Straus MA, Fauchier A. Manual for the Dimensions of Disciple Inventory (DDI) Durham, NH: Family Research Laboratory, University of New Hampshire; 2011. [Google Scholar]
- Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D. Identification of child maltreatment with the Parent-Child Conflict Tactics Scales: Development & psychometric data for a national sample of American parents. Child Abuse & Neglect. 1998;22(4):249–270. doi: 10.1016/s0145-2134(97)00174-9. [DOI] [PubMed] [Google Scholar]
- Tendulkar SA, Koenan KC, Dunn EC, Buka S, Subramanian SV. Neighborhood influences on perceived social support among parents: Findings from the project on Human Development in Chicago Neighborhoods. PLOS One. 2012;7(4) doi: 10.1371/journal.pone.0034235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, Smith B. Prevention and drug treatment. The Future of Children. 2009;19:147–168. doi: 10.1353/foc.0.0033. [DOI] [PubMed] [Google Scholar]
- Thompson RA. Preventing Child Maltreatment through Social Support. Thousand Oaks, CA: Sage; 1985. [Google Scholar]
- Tucker C, Lepkowski JM, Piekarski L. The current efficiency of list-assisted telephone sampling designs. Public Opinion Quarterly. 2002;66:321–338. [Google Scholar]
- U.S. Department of Health and Human Services, A. f. C. a. F., Administration on Children, Youth, and Families, Children’s Bureau. Child Maltreatment 2011. 2012. [Google Scholar]
- Wall G, Arnold S. How involved is involved fathering?: An exploration of the contemporary culture of fatherhood. Gender & Society. 2007;21:508–527. [Google Scholar]
- Way I, Chung S, Jonson-Reid M, Drake B. Maltreatment perpetrators: A 54-month analysis of recidivism. Child Abuse & Neglect. 2001;25:1093–1108. doi: 10.1016/s0145-2134(01)00258-7. [DOI] [PubMed] [Google Scholar]
- West C, Zimmerman DH. Doing gender. Gender & Society. 1987;1(2):125–151. [Google Scholar]
- Williamson JM, Borduin CM, Howe BA. The ecology of adolescent maltreatment: A multilevel examination of adolescent physical abuse, sexual abuse, and neglect. Journal of Consulting and Clinical Psychology. 1991;59(3):449–457. doi: 10.1037//0022-006x.59.3.449. [DOI] [PubMed] [Google Scholar]