

White matter hyperintensities (WMH) of presumed vascular origin, also referred to as leukoaraiosis, are a very common finding on brain magnetic resonance imaging (MRI) or computed tomography (CT) in older subjects and in patients with stroke and dementia. They are associated with cognitive impairment, triple the risk of stroke and double the risk of dementia. Knowledge of their pathology derives mostly from post mortem studies, many from some years ago. These, by their nature, were generally small, sampled from selected brain regions and probably reflect late-stage disease. They focus on features of demyelination and axonal degeneration, which may be easier to detect histopathologically than changes in extracellular fluid. Here we review advances in brain magnetic resonance imaging (MRI) that are revealing white matter hyperintensities at earlier stages, and changes in normal-appearing white matter that indicate tissue pathology, less marked than those found in WMH. These “pre-visible” changes show that altered interstitial fluid mobility and water content, which may be reversible, probably predate demyelination and axonal damage, which are less likely to be reversible and are probably a late-stage phenomenon. Neuroimaging is also revealing the dynamic nature of WMH, their interactions with other pathological features such as secondary cortical and long tract damage, and contribution to accumulating brain damage. These insights provide opportunities to improve understanding the etiology and pathogenesis of small vessel disease, and represents an enormous unfinished agenda for preventing accumulation of brain damage, and its associated cognitive and physical problems, from mid to later life. Recognizing the earliest stages leading to WMH development will provide important opportunities to prevent (or even reverse) brain damage due to small vessel disease at the earliest stages, and ameliorate its cognitive, physical, stroke and dementia consequences.
Historical Perspective
Worldwide, about 15 million people have a stroke, from which 6 million die and 5 million are left permanently disabled each year1; 35.6 million people worldwide are estimated to be living with dementia, and this is expected to triple by 2050. Although Alzheimer’s disease is the most commonly diagnosed form of cognitive impairment in older people,2 cognitive impairment due to vascular disease alone, or in addition to Alzheimer’s disease, is very common and contributes to substantial worsening of cognitive function for a given burden of Alzheimer’s disease pathology.3 The most common form of vascular cognitive impairment typically results in lesions visible on brain scanning known collectively as small vessel disease (SVD) and described in more detail below. Although stroke and dementia are priorities for many governments, the cause of the 20% of strokes and about 40% of dementias attributed to SVD4 remains unclear, with limited options for prevention and treatment.
The finding of altered areas of white matter attenuation on computed tomography (CT) was first brought to prominence in the late 1980s by Hachinski and colleagues. They described patchy low attenuation in the periventricular and deep white matter, which they referred to as leukoaraiosis (Figure 1).5 These patchy white matter changes are more obvious as abnormal areas of signal intensity on magnetic resonance imaging (MRI) due to the latter’s better sensitivity to soft tissue changes than CT, particularly for subtle alterations in water content. The signal changes predominate in the periventricular and deep white matter, so were commonly referred to originally as “white matter lesions” although they are also recognized to occur in the deep gray matter.6 These areas are hyperintense on T2-weighted (T2), proton density-weighted (PD), and fluid attenuated inversion recovery (FLAIR) MRI sequences, so are now by consensus referred to as “white matter hyperintensities” (WMH), or “subcortical hyperintensities” where deep gray matter is also involved.6 They are also hypointense on T1-weighted and hyperintense on T2*-weighted sequences, but the most sensitive structural sequence for visualizing WMH on MRI is generally the FLAIR sequence (Figure 1).
Figure 1.
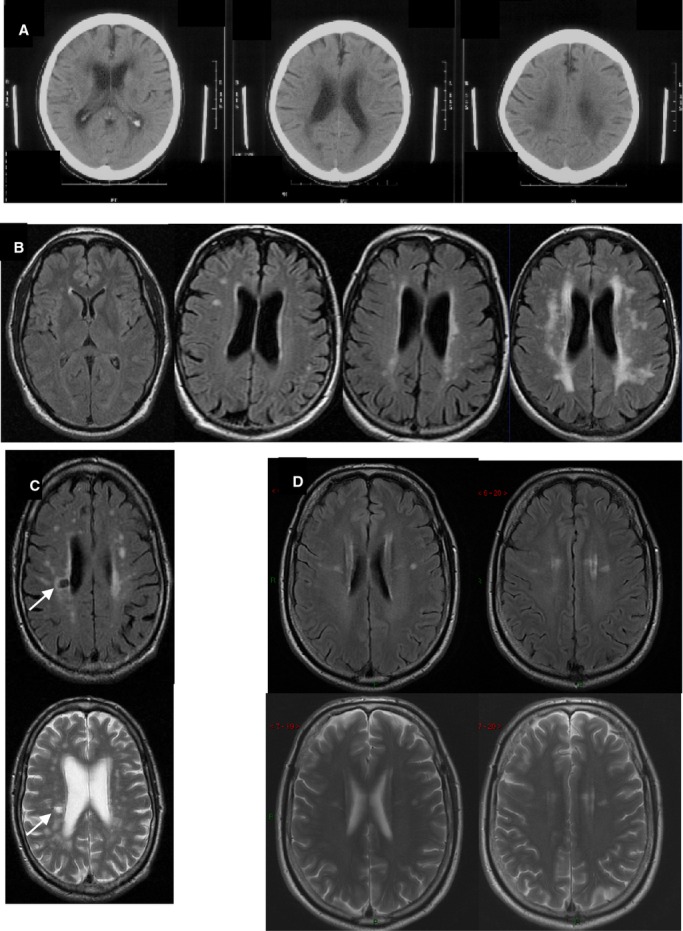
Examples of WMH on (A) CT, (B) MR FLAIR, (C and D) MR FLAIR and T2-weighted imaging. A, Three adjacent CT images from 1 patient with severe WMH. B, Four different subjects showing, L to R, normal to severe WMH. C, FLAIR and T2-w, same subject, show WMH and a lacune (arrow). D, top FLAIR, bottom T2-w images showing that when subtle, WMH are more easily seen on FLAIR. CT indicates computed tomography; FLAIR, fluid attenuated inversion recovery; MR, magnetic resonance; WMH, white matter hyperintensities.
MRI came into wider use in clinical practice and for research in the late 1980s and early 1990s. Early MRI scanners of the 1980s–1990s were generally of lower field strength than are available routinely today. This affected their sensitivity. For example, the earliest scanners in clinical use were 0.2 or 0.5 Tesla field strength, and inevitably were less sensitive to subtle tissue changes than are the 1.5 or 3 T MR scanners that are in widespread use today. The early studies also had fewer sequences available and these were less sensitive to brain soft tissue changes than those available now. For example, it was common to use T1-weighted (T1) or T2 sequences, T1 being of similar sensitivity to subcortical changes as is modern CT scanning, while T2 is relatively insensitive to subtle white matter abnormalities and is less good at identifying changes adjacent to a cerebrospinal fluid (CSF)-containing space than is FLAIR (eg, in the immediate periventricular tissues). Hence, when considering imaging-pathological correlations, imaging-clinical, or imaging-cognitive correlations, it is important to bear in mind that early studies of MRI-pathology correlations may have lacked sensitivity to detect the more subtle changes that are visible today, and thus may have influenced our understanding of the pathophysiology towards what are probably more established, permanent changes.
WMH had been overlooked somewhat by pathologists up until CT and MRI became available,7,8 much of the focus of pathology examinations in the last century being on lacunes (small CSF-containing cavities)9,10 that are easier to detect pathologically than subtle WMH.11,12 The diffuse and often subtle changes of WMH may be hard to see macroscopically on brain sections until they are advanced13; when subtle, the full extent of WMH may be difficult to appreciate histologically unless specifically sought in aging-related changes14 or in other white matter diseases such as multiple sclerosis.15 In contrast, lacunes, ie, small CSF-containing cavities, are more obvious pathologically and had been described in numerous detailed pathology studies (summarized in Bailey et al16) although there were not many imaging-pathology correlations for lacunes either.
Clinical Importance
Until relatively recently, WMH were generally dismissed as inevitable consequences of “normal” advancing age. This is clearly not true. Although WMH do become more common with advancing age,17 their prevalence is highly variable. Furthermore, numerous studies indicate that they have important clinical and risk factor associations, emphasizing that they should not simply be overlooked as inevitable “silent” consequences of the aging brain.
In a meta-analysis of 22 longitudinal studies, WMH were clearly associated with progressive cognitive impairment, a 2-fold increase in the risk of dementia and a 3-fold increase in risk of stroke.18 WMH also affect physical function, resulting in abnormal gait19 and disturbed balance.20 WMH increase the risk of late onset depression.21 Furthermore, WMH are highly heritable,22 and they vary with familial longevity being less frequent in subjects with long-lived parents.23 WMH are inversely associated with intelligence in youth,24 and with educational attainment.25 Whether these latter associations indicate relationships between intelligence and risk factor exposure or reflect brain resilience to damage,26 are as yet unknown.
The prevalence of WMH increases with increasing vascular risk factors, including hypertension,27–29 diabetes,30 smoking,31,32 as well as with many other as yet undetermined risk factors.33 Risk factor exposure seems to be particularly important if it occurs in middle age,29,34 but the relative importance of different risk factors may also vary in different age groups. A large multicenter study of WMH in 2699 stroke patients in 11 stroke centers in China suggested that raised cholesterol was a more important risk factor for WMH in older hypertensive patients whereas age alone was the major risk factor in older non-hypertensive patients. Diabetes mellitus was an important risk factor in younger non-hypertensives.35 It is unclear as yet if hypertension has most of its effect directly on the brain, or if it results in systemic vascular stiffening, which in turn affects the brain white matter36,37 and cognition.38 Accumulating evidence, including associations with left ventricular hypertrophy, tend to point to the former explanation,35,37 but more longitudinal studies to determine the sequence of development of WMH in relation to risk factors are required. Additionally, there are as yet mixed results from randomized trials on whether risk factor reduction can prevent WMH progression or cognitive decline in older subjects,39–41 and some evidence that too aggressive blood pressure reduction in old age could actually worsen white matter damage42 and cognitive decline, perhaps if autoregulation is impaired through vessel stiffening and loss of vasoreactivity. Further trials of risk factor management are needed and specifically at different ages because different vascular risk factors may have more impact at different ages (eg, hypertension in middle age, cholesterol at older ages35). Physical activity is suggested to protect against WMH in cross-sectional studies,43–45 but whether exercise can prevent progression or development of WMH remains to be tested in randomized clinical trials.
WMH are part of the spectrum of small vessel disease (SVD) which includes lacunar (or small subcortical) ischemic and hemorrhagic stroke, lacunes, microbleeds, perivascular spaces and brain atrophy (Figure 2).6,46 All of these features, individually, are associated with cognitive impairment,47–51 even when subtle.
Figure 2.

STRIVE examples of different features of small vessel disease, including white matter hyperintensities. Reproduced with permission from Wardlaw et al.6 DWI indicates diffusion-weighted imaging; FLAIR, fluid attenuated inversion recovery; GRE, gradient recalled echo; STRIVE, standards for reporting vascular changes on neuroimaging; SWI, susceptibility-weighted imaging.
The dynamic nature of these inter-related lesions is illustrated by studying patterns of lesion evolution (Figure 3): acute small subcortical infarcts can disappear (10%), remain looking like a WMH (60% to 70%), or cavitate to form a lacune (20% to 30%)52–54; lacunes may form at the edge55 or (in our experience) in the middle of a WMH; WMH can “grow” at the edges of small subcortical infarcts56; incident lacunes57 and WMH58 are associated with cortical thinning and cerebral atrophy59; all of which indicate progressive and accumulating brain damage. Furthermore, WMH increase risk of brain damage in the presence of other pathologies, for example, they associate with infarct growth and worse outcome after large artery stroke,60,61 and they predict poor functional stroke outcome.62–64
Figure 3.
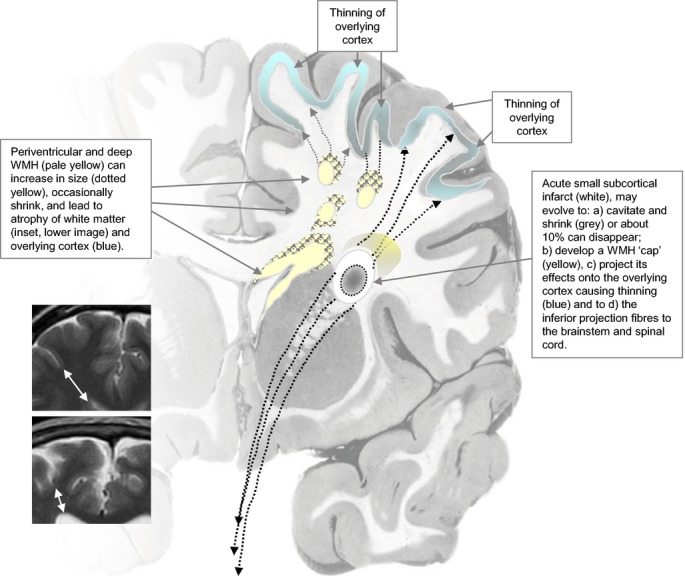
Diagram of dynamic mechanisms by which WMH and SVD lead to brain damage. See separate file. SVD indicates small vessel disease; WMH, white matter hyperintensities.
The effects of all these SVD features on cognition are cumulative,65 (in submission) providing further indication that together these SVD features are closely related pathologically,52 and represent cumulative brain damage,32 the prevention of which should help ameliorate brain tissue damage, reduce loss of normal brain cognitive and physical function and preserve independent survival in old age.43
What Do Pathology Studies Suggest That WMH Are Due To?
Pathology studies are, unfortunately, infrequent12,66,67 compared with the number of WMH captured in imaging studies. There are particularly few pathology studies that have linked individual lesions seen on MRI with their pathological examination.12,68,69 Pathology studies have been hampered by difficulty in matching up individual small lesions on imaging with their pathological counterpart,11,68 with limitations of sampling,13 of fixation,70 of definitions,71–73 they provide “snapshots” of disease evolution, and because end-stage damage may obliterate the earliest stages of disease.
As described above, the earlier pathology reports focused on demyelination and axonal loss in WMH7 and described the changes as “ischemic”.74,75 Demyelination and axonal destruction imply that the changes are permanent. Indeed, extensive WMH were associated with reduced density of glia and vacuolation.8 More subtle WMH on MRI were associated with microglial and endothelial activation.13 Some studies differentiate periventricular from deep WMH12,76,77 although imaging studies indicate that periventricular and deep WMH are probably mostly part of a continuous pathology.76,78 A recent very large study in 2699 patients with stroke from 11 stroke centers in China created statistical maps of WMH distribution and provided more evidence to support treating periventricular and deep WMH as a continuous pathology, any apparent difference in distribution in some patients simply reflecting an earlier stage in disease.35 Notwithstanding, the available pathology describes periventricular WMH as having discontinuous ependyma, gliosis, loosening of the white matter fibers, and myelin loss around tortuous venules in perivascular spaces,11,12,79 the gliosis, demyelination, and fiber loss worsening as the periventricular WMH worsened. In deep WMH, there was demyelination, gliosis, and axonal loss around perivascular spaces, with vacuolation and increased tissue loss as the lesions became more severe.12 The changes were heterogenous.77 WMH in patients with AD showed more microglial activation than in WMH of age-matched controls.80 The variation in pathological severity might help explain some of the variation in the association between WMH severity and cognitive change in old age80 although this needs to be verified in larger and more heterogeneous populations with good cognitive, dementia and SVD phenotyping.
Some reports indicate the presence of proteins in the perivascular tissues in human WMH81 and suggest that the arteriolar wall thickening seen in SVD is also a consequence of the movement of plasma proteins into the vessel walls.82 The proteins include fibrinogen, immunoglobulins, thrombomodulin,83 and occur in subcortical grey and white matter and are also seen in normal appearing white matter and are associated with microglia.81 The microglia and proteins were more frequent in areas of WMH with more advanced tissue loss.81 Increased albumin was found in the interstitial tissues of brains of older subjects with WMH84 although it was uncertain as to where the albumin had come from in this study as the endothelial tight junction proteins were said to be intact. Others have not identified direct evidence of blood-brain barrier (BBB) impairment despite identifying proteins associated with endothelial activation83 and that had extravasated into the perivascular tissues.85 However, the cerebral blood flow and the cerebrovascular endothelial surface area are both so large that there would not have to be much breach of the BBB for proteins and fluid to accumulate in the interstitial spaces. It is likely also that such tissue fluid shifts are difficult to identify pathologically or overlooked as fixation artifact, where fixation methods involve freezing or dehydration, which may affect tissue content.70
Numerous in vivo studies have found raised CSF:plasma albumin ratios with advancing age, in patients with Alzheimer’s disease, in vascular dementia, and in patients with WMH,86 and suggested a role for chronic brain edema in forming WMH and more advanced damage in the form of lacunes.87–89 Undoubtedly the pathological picture is mixed and complex90: despite the risk factor association, immunohistochemical and gene expression microarray studies suggesting a role for ischemia, hypoxia, or hypoperfusion, studies also show immune activation, BBB dysfunction, altered cell metabolic pathways, and glial injury.90 The abnormalities are now being recognized in normal-appearing white matter as well as in WMH. Therefore, regardless of where the albumin or other plasma proteins came from, or how they got into the interstitial tissues, there does appear to be a role for loss of normal BBB function and fluid shifts into the brain leading to secondary brain damage91,92; if arrested or reversed early, the interstitial fluid shifts may be more reversible than demyelination and axonal loss.
What Does Imaging Suggest?
To understand more about the pathophysiology of WMH, we must turn to imaging methods that allow us to detect and quantify subvisible tissue changes on a per voxel basis in vivo. Structural changes in the integrity of the brain’s white matter are commonly observed through MRI methods such as diffusion tensor imaging (DTI), a widely available imaging technique that provides quantitative measures of the mobility of water molecules in vivo. Parameters obtained from the water diffusion tensor are used as diagnostic markers for clinical applications. The most commonly used are fractional anisotropy (FA), which indicates the deviation from pure isotropic diffusion of water mobility in vivo, and mean diffusivity (MD), which measures the magnitude of diffusion of the water molecules.93 Both the magnitude and directionality of the water diffusion are affected by the underlying tissue architecture and can demonstrate, for example, alterations in axonal microstructure or interstitial fluid.94–98
Further potential MRI biomarkers of white matter damage are the magnetization transfer ratio (MTR) and the longitudinal relaxation time (T1). MTR is obtained from magnetization transfer MRI99 and can show pathological changes in the white matter structure that involve macromolecules in the cell membrane, such as inflammation or demyelination.100 T1 relaxation time is a weighted average of the free and bound water phases101 providing quantitative information on brain water content, and is therefore a potential marker for edematous brain tissue.94
Other methods of assessing alterations in normal brain tissue function use dynamic imaging following intravenous injection of a contrast agent. In dynamic contrast-enhanced MRI102 a series of T1-weighted images are acquired dynamically after injection, enabling the measurement of BBB permeability.103,104 Similarly, dynamic susceptibility contrast MRI is used to measure cerebral perfusion and estimate regional cerebral blood volume and cerebral blood flow (CBF), again by tracking a contrast agent bolus using a T2*-weighted sequence.105,106
The measurement of these MR imaging biomarkers in addition to structural “visible” brain changes, can help to identify the pathophysiological changes within normal-appearing white matter and WMH in vivo and inform our understanding of their pathophysiology.
Studies in humans have shown that MD and T1 increase while FA and MTR decrease significantly in areas of WMH when compared to normal appearing white matter,98,107–109 indicating pathological processes involving increased water content and mobility, demyelination, and axonal loss. MD was reported as the parameter that discriminated best between normal-appearing white matter and WMH (Figure 4).109 Perfusion MRI studies also showed decreased CBF in regions of WMH,110,111 although it remains uncertain as to how much the blood flow reduction represents reduced flow due to having less tissue to supply but is not the primary cause of the damage,37,112 or is the primary cause of worsening of tissue damage:113,114 there is some evidence for both explanations.115 The dynamics of WMH progression and associations with CBF are complex and regionally specific.116
Figure 4.
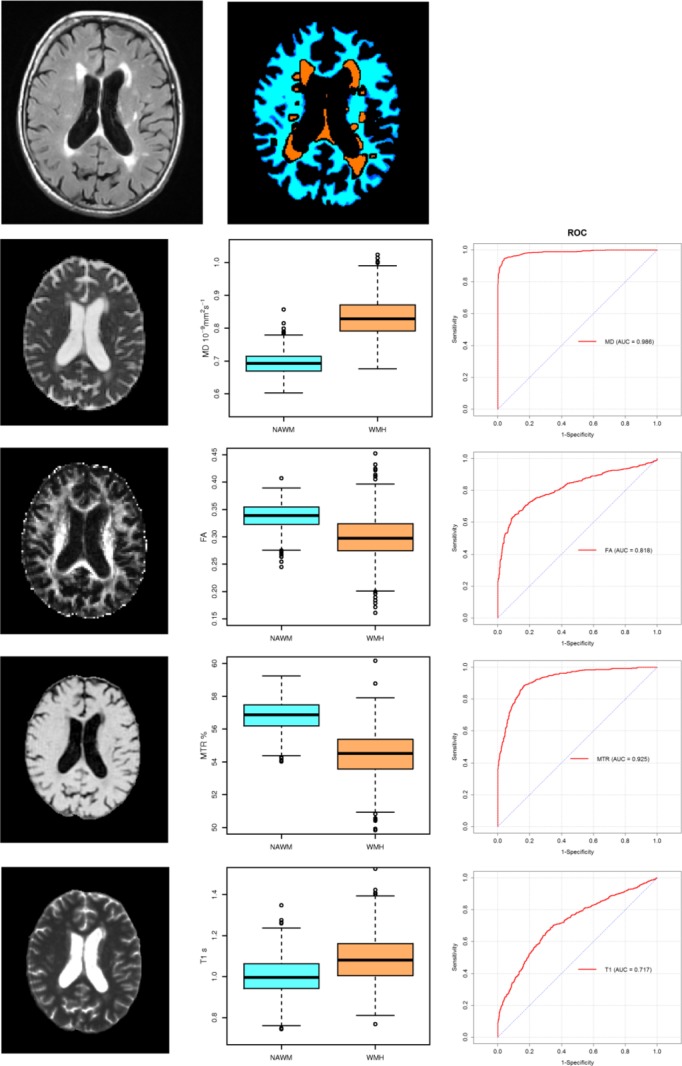
Images for FA, MD, T1, and MTR and corresponding values in normal-appearing white matter and WMH. And corresponding ROC curves for each parameter’s ability to differentiate normal white matter from WMH. MD shows a near perfect ROC curve. Top 2 images show the original FLAIR image and the tissue segmentation into normal white matter and WMH. FA indicates fractional anisotropy; FLAIR, fluid attenuated inversion recovery; MD, mean diffusivity; MTR, magnetisation transfer ratio; NAWM, normal-appearing white matter; ROC, receiver operator characteristic; WMH, white matter hyperintensities.
Imaging demonstrates that WMH are heterogeneous, ie, they represent different amounts of tissue damage, as reflected in their degree of “whiteness” and in features seen on more recent MR scanners such as “dirty white matter” (Figure 5). Moreover, studies using MTR show that MTR differs between frontal and occipital WMH,117 either indicating different stages of tissue damage or possibly different underlying tissue constructs.
Figure 5.
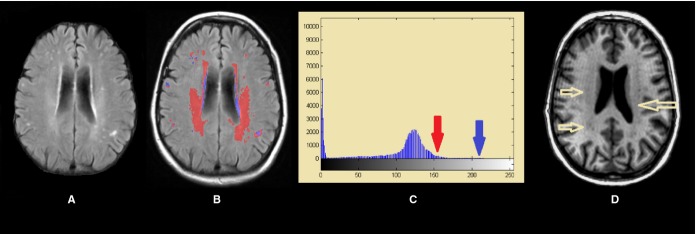
FLAIR image through the lateral ventricles showing severe (ie, intense) WMH and less-intense white matter damage (A), represented in blue and red, respectively in (B) and which correspond with the intensities arrowed in the histogram (C). Less-intense damage can be also observed in the T1-weighted modality as the yellow arrows show (D). FLAIR indicates fluid-attenuation inversion recovery; WMH, white matter hyperintensities.
The relationships between different parameters observed in WMH differed from those relationships in normal-appearing white matter (Figure 6). Significant correlations appeared between MTR and both FA and MD in WMH, whereas these parameters were not correlated in normal-appearing white matter, indicating that cellular breakdown in WMH allows quantitative MRI parameters to take a much wider range of values than in healthy tissue, where they are kept within tight bounds and are likely to be independent.98
Figure 6.
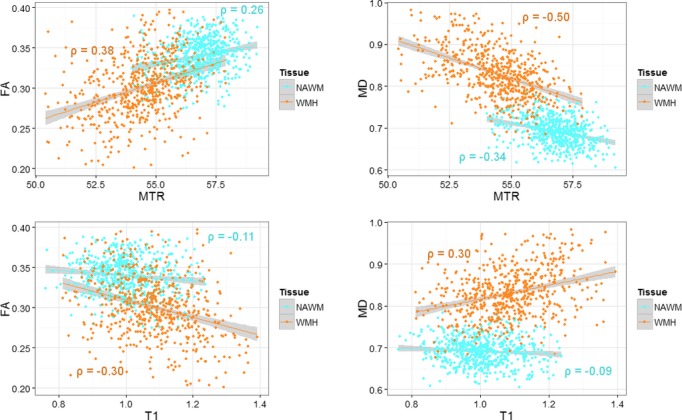
Correlations between FA, MTR, MD and T1 in NAWM and WMH. In general, the T1 and FA, MD and MTR show stronger correlations in WMH than in NAWM. FA indicates fractional anisotropy; MD, mean diffusivity; MTR, magnetization transfer ratio; NAWM, normal-appearing white matter; WMH, white matter hyperintensities.
Several reports indicate that the tissue structural and vascular changes spread further than the visible area of the WMH, rather than being confined to the visible WMH109,111,118–120 consistent with recent pathological reports.90 The changes radiate into normal-appearing white matter, particularly in the immediate peri-WMH tissue, indicating that the underlying pathology is a diffuse process affecting much of the white matter and even other parts of the brain, and that visible lesions, ie, the WMH, are probably only the “tip of the iceberg.”
This compromised normal-appearing white matter integrity in the presence of WMH has been observed through different quantitative imaging techniques. For example, CBF121 and cerebrovascular reactivity were reduced and BBB permeability was increased in the normal appearing white matter of healthy elderly subjects and all were associated with the presence of WMH.122 BBB permeability increases with advancing age during normal aging, but is further increased in dementia particularly in patients with vascular dementia and in patients with WMH.86 Others have found increases in BBB permeability in NAWM in patients with WMH,123 in patients with lacunar versus cortical ischemic stroke, with increasing age and numbers of enlarged perivascular spaces,124 and in WHM in vascular dementia.125 The MD and FA of NAWM have been also associated with WMH volume.120,126–128
However, studies typically include subjects of widely varying age and the changes observed in NAWM integrity relative to WMH load could also be a consequence of the older age of those subjects with more WMH.17,129,130 A more recent study in a large cohort of older people of near-homogeneous age reported that FA, MD, MTR, and T1 were all associated with the severity of WMH (highest Fazekas scores) – even after accounting for age, gender, exposure to common vascular risk factors and the proximity to WMH – proving that the changes observed were not just a function of age.109 Moreover, although all 4 parameters measured in NAWM were related to WMH severity in those with most WMH, only the MD of NAWM showed changes within the mildest range of WMH. Additionally, of the 4 quantitative parameters of MD, FA, MTR and T1, it was MD that showed the best differentiation of WMH from normal-appearing white matter, performing substantially better on received operator characteristic (ROC) curves than did FA, MTR, or T1. This combination of findings suggests that the earliest pathological processes responsible for WMH involve changes in interstitial fluid mobility.109
Although observed by others,98 the concept of “WMH penumbra” was introduced by Maillard et al118 after they observed that the effects on FA are not only globally influenced by the WMH load, but also locally influenced by the distance into normal-appearing white matter from the edge of the WMH. This idea of the more abnormal the tissue, the closer the proximity to the WMH, was recently corroborated by measuring MRI quantitative parameters in the normal-appearing white matter in “contours” set at increasing distance from the visible edge of the WMH on FLAIR. In this contour-based analysis, MD decreased and MTR increased with increasing distance from the WMH over all distances assessed, whereas FA and T1 mainly showed only slight changes in the closest contours to the WMH (Figure 7).109
Figure 7.
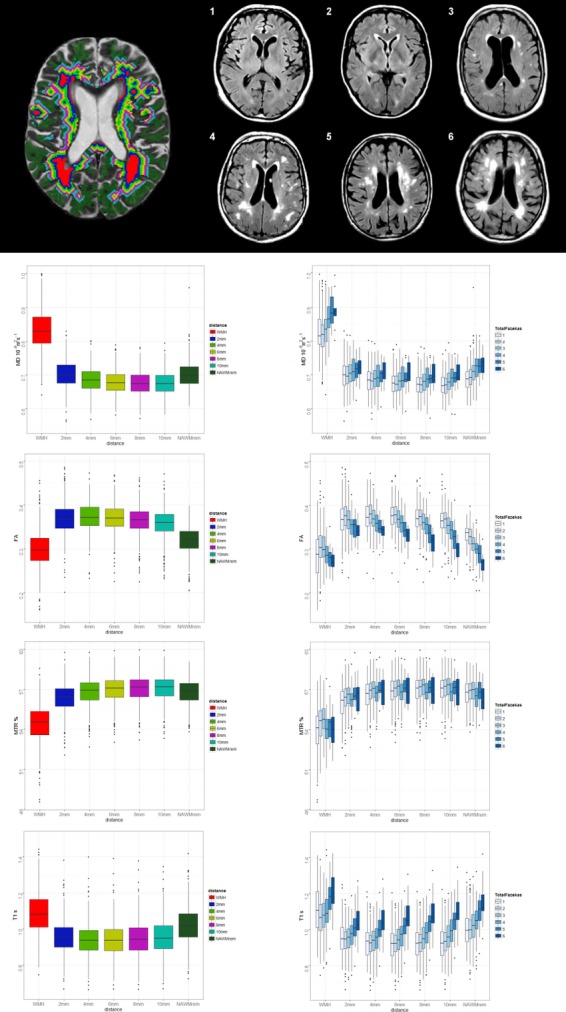
Effect on MD, FA, MTR, and T1 of increasing burden of WMH, in the WMH and at 2 mm distance increments from the WMH edge into the NAWM (2 mm-NAWMrem). Top left, illustrates WMH (red) and contours (different color bands), right, 1 to 6, WMH Fazekas scores. Lower left graphs show change in the 4 MR parameters from WMH and at increasing distance into the NAWM; lower right graphs show the parameter changes at increasing distance into NAWM split by total WMH burden (Fazekas score). Adapted from Muñoz-Maniega et al.109 FA indicates fractional anisotropy; MD, mean diffusivity; MTR, magnetisation transfer ratio; NAWM, normal-appearing white matter; WMH, white matter hyperintensities.
Longitudinal studies suggest that people with lower white matter integrity at baseline are more likely to progress to cognitive impairment or frank Alzheimer’s disease than are those with higher white matter integrity.131 Having a high WMH burden increases the risk of worsening WMH several years later,132 as well as of stroke, dementia, and death.18 New lacunes form at the edges of WMH55 and WMH form at the edges of small subcortical infarcts or lacunes,56 ie, damage begets damage (Figure 3).
The precise sequence of pathologic processes underpinning the microstructural changes in white matter integrity within and around WMH are yet to be fully described. Pathology studies have described rarefaction, demyelination, and axonal loss in WMH as outlined above, which are compatible with the observed increases in MD and T1, and the decreases in FA, MTR, and CBF detected using neuroimaging. Some changes such as minor fluxes in fluid content may be relatively easier to detect with MR imaging, which is highly sensitive to water shifts. Hence, neuroimaging in vivo is highly complementary to pathology by providing tools to aid the identification of the earliest stages in the pathological processes that end in the development of visible WMH.46 The increase in MD in NAWM seen even in the presence of the mildest WMH burden, and the fact that this parameter also provides excellent discrimination between both tissue types on ROC curves, suggests that altered mobility of interstitial fluid occurs earlier in the developing pathology of WMH in the aging brain than do changes in myelin (MTR), axonal integrity (FA), or total water content (T1). However, further work relating these imaging biomarkers to histopathological findings, especially at early stages in disease, and in longitudinal studies, is required to understand fully the pathological processes that are responsible for white matter damage within and around the WMH.
Limitations of Imaging Approaches to Determining WMH Pathophysiology
MRI processing methods for WMH detection and differentiation from artifacts, co-registration of different types of images, and image processing methods such as bias field correction, affect measurements of lesions and brain tissue parameters. The full analysis of these limitations is beyond the remit of this paper, but these limitations are important but rarely mentioned in imaging papers so are discussed briefly here for completeness. Indeed the full scope of the effects of these limitations is only just beginning to be understood by the clinical research community.
Methods to quantify WMH volume are evolving rapidly. Many were developed for use in one study, reflect the particular subject, image acquisition characteristics and WMH burden of that study population. Few, if any, are in use in clinical practice. Many research groups develop their scanning protocol and WMH segmentation approach and apply it to subsequent studies, without further validation. The protocol may not be changed or improved partly due to lack of availability of source codes and/or software and because of a natural desire to minimize the effect of protocol changes on measured variables. Most studies use a semi-automatic thresholding approach to identify WMH on FLAIR images. These threshold selection methods may then be applied in different studies assuming that the reliability will not change, which is unlikely to be correct as FLAIR images are not quantitative and the signal to noise ratio may not be the same. Thresholding on a single image such as FLAIR requires individualized thresholds (“one size” does not “fit all cases”); multispectral approaches using several sequences combined are more accurate.133 A full description of the WMH volume measurement methods used in different studies to date is beyond the scope of this paper but is available upon request.
WMH volume measurement is time consuming, hence larger studies seek automated approaches but it is not known whether all studies check each case individually for the accuracy of segmentation, or the rigor with which this is performed where done. However, there is as yet no automated approach that can identify WMH accurately without any human input – all require visual assessment and manual correction, particularly in populations with advanced age or stroke where the brains are more likely to be abnormal (Figure 8) and features of similar signal characteristics like stroke lesions, if not excluded, will distort the WMH volume measurements with subsequent alterations on the outcome of the study.134
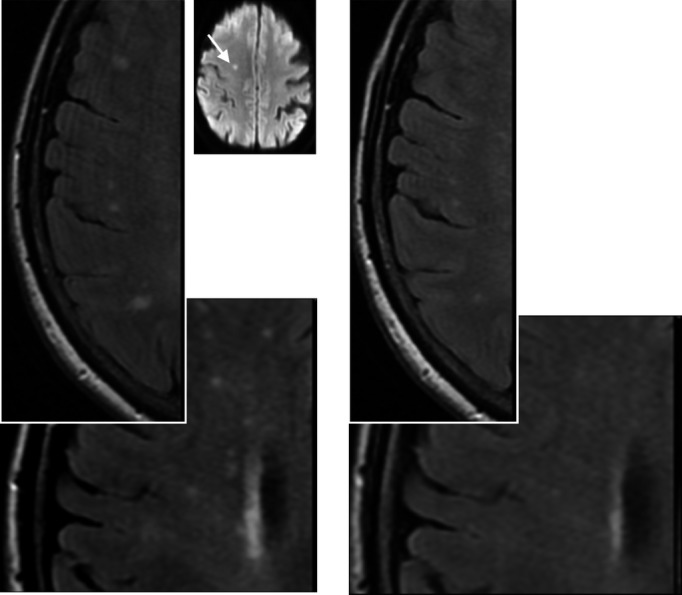
Figure 8.
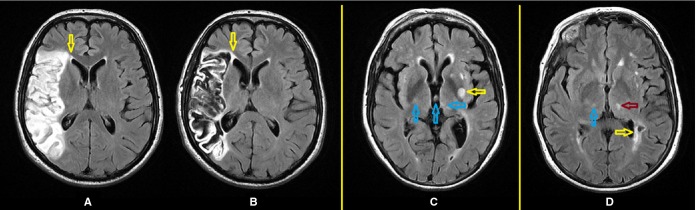
Some factors which confound the delineation of WMH. FLAIR axial images from a patient 4 days after a stroke (A) and a year later (B): while the boundary of the periventricular WMH can be well perceived on the baseline scan, it coalesces with the large infarct after a year (yellow arrow) making it impossible to quantitatively determine accurately the increase in the stroke lesion separated from the increase in the WMH. Different patient (C) has a recent small subcortical stroke lesion arrowed in yellow, and artifacts arrowed in blue; (D) a lacune (yellow arrow) confluent with the periventricular WMH, real thalamic hyperintensity arrowed in magenta and thalamic artifact arrowed in blue create difficulties for measuring the WMH. FLAIR indicates fluid attenuation inversion recovery; WMH, white matter hyperintensities.
Artifacts that mimic WMH (to a computer algorithm) are numerous (Table 1) and require manual editing.135,136 Guidelines exist to differentiate WMH from artifacts,135,137 but these lack uniformity and consensus. Some class periventricular hyperintense thin lines around the lateral ventricles as artifact,135,139 but others found a high correlation between signal intensity levels and width of the periventricular WMH, total WMH volumes, periventricular WMH severity, vascular risk factors, and stroke,76 indicating that periventricular WMH are true tissue abnormalities and should not be considered artifacts.78
Table 1.
Common Artifacts That Confound the Identification of WMH on FLAIR MRI
| Artifact Type | Artifact Location | Characteristic Effect | References |
|---|---|---|---|
| CSF flow | Fourth ventricle, aqueduct, cistern ventral to mesencephalon | Hyperintense tissue surrounding these structures; periventricular hyperintensity with constant gradient | 136,138–145 |
| CSF flow | Bilateral sylvian fissures and insular cortex | Uniform hyperintensity along the external capsule | 136,146,147 |
| CSF flow | Third ventricle and Fornix | Hyperintense tissue surrounding the third ventricle and fornix; diffuse periventricular hyperintensity gradually decereasing in strength towards the antero-medial thalamic nucleus and internal capsule | 136,140,142,144,147 |
| CSF flow | Lateral ventricles | Hyperintense cluster near the walls of the anterior horns of the lateral ventricles | 136,140,142,144,147 |
| CSF flow | Choroid plexus | Small hyperintense cluster above the temporal horns of the lateral ventricles | 144 |
| Corticospinal tract | Pathways of the corticospinal tracts | Bilateral and symmetric hyperintensities with similar signal level in the junction between the internal capsule and the medial thalamic nucleus | 147 |
| Magnetic field susceptibility | Amygdaloid nucleus and anterior temporal poles | Wide hyperintense clusters covering the amygdaloid nuclus and the anterior temporal poles | 136,145,148 |
| Magnetic field susceptibility and CSF flow | Cingulate gyrus | Hyperintense tissue along the longitudinal cerebral fissure on the anterior section and on the territory of the anterior cerebral artery | 136 |
| Patient motion (eye movement) | Around the eyes | Ghosting effect on tissue around the eyes | 136,143 |
| Patient motion (Head movement) | Throughout the whole image | Concentric hyperintense rings that distort/mask real WMH | 136,138,148,149 |
| Image reconstruction (Gibbs ringing) | Throughout the brain accentuated near the skull borders | Concentric hyperintense rings that follow signal intensity borders and distort/mask small WMH | 145 |
| Blood flow | Near the sinuses and main arteries | Small linear hyperintensities near the sinuses and carotid arteries | 145 |
Note, only publications that were dedicated to analyse and describe these artifacts on FLAIR MRI and/or propose methods to compensate them are referenced. CSF indicates cerebrospinal fluid; FLAIR, Fluid Attenuated Inversion Recovery; MRI, magnetic resonance imaging; WMH, white matter hyperintensities.
Differentiating WMH from other SVD lesions such as perivascular spaces6,8,150 and lacunes6 may be difficult. Differences in magnet strengths can lead to inconsistent assessment of WMH, eg, subtle tissue changes in normal-appearing white matter could go unnoticed at 3 T due to noise151,152 or vice versa (Figure 9).153 Reported mean intra- and inter-scanner coefficients of variation in automatic volumetric measurements of brain structures range from 0.87% to 15.1% (median 4.80%). Only limited information is available for the range of values for direct comparisons of WMH assessed at 1.5 and 3 T.153,154
Figure 9.
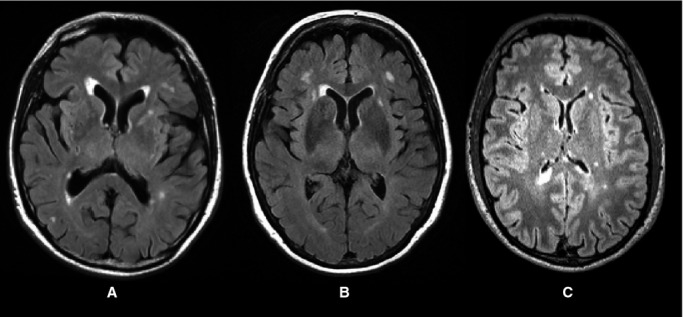
Three different patients, but with similar amounts of WMH, scanned with slightly different slice thicknesses and at 1.5 or 3 T, illustrate the resulting differences in signal of WMH and normal tissues and hence the need for changes in tissue and WMH volume measurement methods. Slice thickness 1 mm2 (A), 0.479 mm2 (B), and 1 mm2 (C) and MR scanner field strength—1.5 T (A and B) and 3 T (C) affect image appearance. Alterations in imaging parameters influence the image appearance and hence the performance of any software used to measure the WMH as all software ultimately rely on differences in signal characteristics between the tissue and lesions of interest. MR indicates magnetic resonance; WMH, white matter hyperintensities.
Image registration methods impose limitations, eg, native versus standard space, atlases, and registering structural to DTI or other echoplanar images, all can distort lesion location and size. In one study of recent small subcortical infarcts of <1.5 cm diameter, we found that the volume of some acute lesions was more than doubled if measured after registering the image in standard space against a routinely available atlas, rather than performing the measurement in native space (ie, on the patient’s own brain scan) prior to registration. Mapping the images of interest against brain atlases allows analysis of lesion distribution (eg, lobar distribution, vascular territories, etc), but relies on accurate registration of a brain template to the brains of the subjects in the population of interest. While state-of-art non-linear registration methods155 have demonstrated very good performance, these have yet to be tested in SVD or aging studies. This is important as it may influence perceived lesion or tract location and represents a complex challenge that needs to be addressed. In general, atlases should be used that are as representative as possible of the age range and population of interest. Unfortunately, no atlases as yet include structures that are typically affected by WMH, such as the major arterial “borderzones,”156 but variation in vascular territories may account for some variation in WMH burden.157
Irrespective of the method used to quantify WMH, one factor that affects the assessment of WMH is the subtle variation in the radio-frequency magnetic field known as magnetic field inhomogeneity. Image processing methods that correct for magnetic field inhomogeneities have been used in some studies.158–162 Some of these methods are scanner and protocol-specific159,162 while others are part of publicly available software where the algorithms assume that the software is applied to brain images with only voxels containing CSF, gray matter, and white matter, after all other tissue types are removed (http://brainsuite.org/processing/surfaceextraction/bfc/, http://bioimagesuite.yale.edu/manual/guide/correction.aspx). If applied to FLAIR images with WMH, these tools may try to remove the WMH or focal infarcts, which are interpreted as inhomogeneities (Figure 10). Hence, these methods should be avoided until it is clear that they do not simply remove the WMH or alter their apparent distribution.
Figure 10.
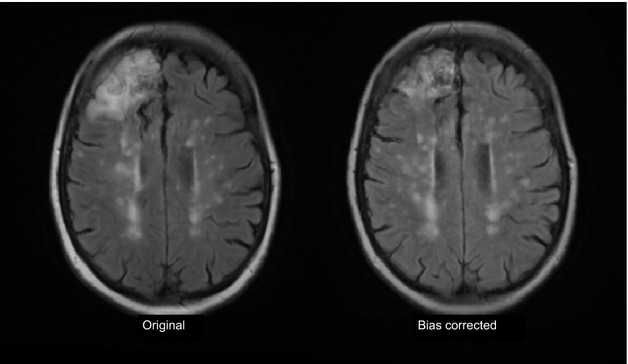
Effect of incautious use of bias field correction on cortical infarct and WMH. The left image shows the original MR FLAIR image with a right frontal cortical infarct (arrow) and numerous WMH. Following bias field correction (left) the frontal infarct appears much smaller, some of the WMH have become more (eg, posterior areas) and some now appear split into smaller components (mid centrum semiovale) as the bias field smoothing software tries to “even out” the distribution of signal intensities across the image. FLAIR indicates fluid attenuation inversion recovery; MR, magnetic resonance; WMH, white matter hyperintensities.
Two final features of WMH that have been overlooked to date are (1) the presence of ill-defined subtle hyperintense white matter that are non-continuous and diffuse, with varying erratic intensity patterns emerging from the lateral ventricle walls, sometimes known as “dirty white matter”163 and which may be an indicator of pre-lesional changes (Figure 5); and (2) the fact that WMH can get smaller or disappear rather than continuously enlarging (Figure 1). “Dirty white matter” is probably a real feature indicating subtle tissue damage, as suggested by the signal change in Figure 5. It will influence where the boundary of the WMH is set and hence associations with other MR parameters like FA and MD.
Figure 11.
Example of disappearing white matter hyperintensities. Left, scan at presentation with small subcortical infarct. Right, scan 1 year later. Inset image is diffusion image from original presentation showing small subcortical infarct that precipitated medical consultation. The images were obtained on the same scanner, using the same sequence with careful quality assurance maintained throughout. Note the lesions have become smaller and less white at 1 year compared with presentation.
That WMH can reduce or disappear should not be a surprise if we accept that much of the signal change on FLAIR or T2 is due to shifts in water content and not just permanent myelin loss or axonal damage. WMH regression was noted in only one previous published case.164 Most longitudinal studies report “no change” or “progression” of WMH. Three studies mentioned “minor regression” in some patients, but classified these as “no progression” without further exploration,165 attributed reductions in WMH volume to measurement variability,166 or reported (small) negative volume changes without comment.167 We have noted reductions in WMH volume as well as increases, eg, about a third of 200 patients who presented with minor stroke had a small reduction in WMH volume on repeat MRI a year after stroke (in submission). In a few cases, the changes were more obvious (Figure 1). The reasons for reduction in WMH are unclear but might relate to improved vascular risk factor control. If some WMH are areas of tissue edema, then reduction in tissue edema would both reduce WMH and decrease brain volume. Indeed, in patients with CADASIL new WMH were associated with subtle increased brain volume.168 Finally, fluctuations in WMH and white matter subvisible damage might account for the return to normal cognition seen in a few studies in patients with mild cognitive impairment.2 Although these fluctuations have been attributed to recovery from depression, delirium, heart failure, or autoimmune disorders, the improving cognition could equally be attributed to resolution of transient fluid-related white matter damage before permanent axonal injury or demyelination has occurred.
Implications for Clinical Practice
There is strong evidence that WMH are clinically important markers of increased risk of stroke, dementia, death, depression, impaired gait, and mobility, in cross-sectional and in longitudinal studies. They associate with brain damage such as global atrophy59 and other features of small vessel brain damage,32 with focal progressive visible brain damage,55,57 are markers of underlying subvisible diffuse brain damage,19,98,109,119 and predict infarct growth and worse outcome after large artery stroke.60,61 They could be considered as the neuroimaging marker of “brain frailty.”169
However, they should not be viewed only as “untreatable” or “permanent”: in vivo imaging indicates that water shifts and water content are prominent and represent early changes in WMH. Given the associations of WMH with traditional vascular risk factors, it is reasonable to manage risk factors according to current guidelines until further data from randomized controlled trials are available. Future trials should assess the effect of risk factor reduction by age group because common vascular risk factors may act differently at different ages. For example, blood pressure reduction in older people may need to work to less stringent target levels than in younger people because some older people with less reactive vasculature may become more dependent on blood pressure for cerebral perfusion than in subjects whose vasculature retains its elasticity and responsiveness. Similarly, cholesterol reduction may be relatively more important in older people to protect the brain than in younger people where its main action may be on the heart. These speculations are based on emerging observations (eg, and the PODCAST trial, paper in preparation) and require careful testing in future trials.
Given the lack of readily available computational analysis methods, and the simplicity and durability of deriving visual WMH scores,170 it is reasonable to use visual scores in clinical practice – at least these would provide some more precise quantification than purely descriptive reports. The addition of imaging methods such as DTI to routine clinical assessment of patients with minor stroke, cognitive, or aging would facilitate quantification of mean diffusivity or fractional anisotropy in normal-appearing white matter to indicate subvisible brain damage.
Implications for Research
Research should target the enormous unfinished agenda that constitutes brain damage represented by WMH and diffuse small vessel disease. There should be more imaging-neuropathology analyses of individual lesions in humans and in relevant experimental models. There should be more awareness that WMH are heterogeneous, can diminish as well as increase, that they represent a tip of the iceberg in terms of damage to the brain and lead to progressive global brain damage through local and remote brain tissue damage. More longitudinal multimodal imaging studies in well characterized subjects from middle to old age, from different ethnic, socioeconomic, and clinical backgrounds, are required to fully understand what influences the varying patterns of WMH and their associations with cognition, gait, mood, and vulnerability to stroke. Multimodal imaging is needed to assess parameters like MD, FA, MTR, T1, perfusion, etc, contemporaneously in normal and abnormal white and gray matter. Better methods to measure WMH are needed that are reliable and efficient, with minimal human input, for large population studies. These need to be more sophisticated to detect subtleties of WMH, change over time and response to treatment. These should be able to detect differences in intensity of WMH, not just size, and to recognize underlying general changes in brain white matter with increasing age and by exposure to risk factors. Better measurement methods are essential for new trials to test risk factor modification, repurposed drugs, new drugs, lifestyle modifications, etc, to prevent progressive brain damage from WMH. Finally, rather than focusing clinical trials on “Alzheimer’s disease” or “Vascular cognitive impairment”, clinical diagnoses which likely represent mixtures of pathologies, perhaps it would be better to focus on intermediary markers of brain damage, such as WMH, which likely reflect more specific pathologic mechanisms.
Sources of Funding
The authors acknowledge institutional research funding from The Row Fogo Charitable Trust (salary support for Valdés Hernández) and Age UK (salary support for Muñoz-Maniega). In addition, the concepts developed in the review derive from research funded by numerous sources over many years but primarily including the Scottish Government Chief Scientist Office, the Wellcome Trust, the UK Medical Research Council, the Scottish Funding Council SINAPSE Initiative, The Stroke Association, and Chest Heart Stroke Scotland.
Disclosures
None.
References
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin AA, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O’Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, III, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De Leon FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorelick PB, Scuteri A, Black SE, DeCarli C, Greenberg SM, Iadecola C, Launer LJ, Laurent S, Lopez OL, Nyenhuis D, Petersen RC, Schneider JA, Tzourio C, Arnett DK, Bennett DA, Chui HC, Higashida RT, Lindquist R, Nilsson PM, Roman GC, Sellke FW, Seshadri S. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:2672–2713. doi: 10.1161/STR.0b013e3182299496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smallwood A, Oulhaj A, Joachim C, Christie S, Sloan C, Smith AD, Esiri M. Cerebral subcortical small vessel disease and its relation to cognition in elderly subjects: a pathological study in the Oxford Project to Investigate Memory and Ageing (OPTIMA) cohort. Neuropathol Appl Neurobiol. 2012;38:337–343. doi: 10.1111/j.1365-2990.2011.01221.x. [DOI] [PubMed] [Google Scholar]
- Iadecola C. The pathobiology of vascular dementia. Neuron. 2013;80:844–866. doi: 10.1016/j.neuron.2013.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hachinski VC, Potter P, Merskey H. Leuko-araiosis. Arch Neurol. 1987;44:21–23. doi: 10.1001/archneur.1987.00520130013009. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, Lindley RI, O’Brien JT, Barkhof F, Benavente OR, Black S, Brayne C, Breteler M, Chabriat H, DeCarli C, de Leeuw F-E, Doubal F, Duering M, Fox N, Greenberg S, Hachinski V, Kilimann I, Mok V, van Oostenbrugge R, Pantoni L, Speck O, Stephan BC, Teipel S, Viswanathan A, Werring D, Chen C, Smith C, van Buchem M, Norrving B, Gorelick PB, Dichgans M. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration: a united approach. Lancet Neurol. 2013;12:822–838. doi: 10.1016/S1474-4422(13)70124-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F, Radner H, Lechner H. Pathologic correlates of incidental MRI white matter signal hyperintensities. Neurology. 1993;43:1683–1689. doi: 10.1212/wnl.43.9.1683. [DOI] [PubMed] [Google Scholar]
- Munoz DG, Hastak SM, Harper B, Lee D, Hachinski VC. Pathologic correlates of increased signals of the centrum ovale on magnetic resonance imaging. Arch Neurol. 1993;50:492–497. doi: 10.1001/archneur.1993.00540050044013. [DOI] [PubMed] [Google Scholar]
- Fisher CM. Lacunes: small, deep cerebral infarcts. Neurology. 1965;15:774–784. doi: 10.1212/wnl.15.8.774. [DOI] [PubMed] [Google Scholar]
- Fisher CM. Lacunar strokes and infarcts: a review. Neurology. 1982;32:871. doi: 10.1212/wnl.32.8.871. [DOI] [PubMed] [Google Scholar]
- Black S, Gao F, Bilbao J. Understanding white matter disease. Imaging-pathological correlations in vascular cognitive impairment. Stroke. 2009;40:S48–S52. doi: 10.1161/STROKEAHA.108.537704. [DOI] [PubMed] [Google Scholar]
- Gouw AA, Seewann A, van der Flier WM, Barkhof F, Rozemuller AM, Scheltens P, Geurts JJ. Heterogeneity of small vessel disease: a systematic review of MRI and histopathology correlations. J Neurol Neurosurg Psychiatry. 2011;82:126–135. doi: 10.1136/jnnp.2009.204685. [DOI] [PubMed] [Google Scholar]
- Fernando MS, O’Brien JT, Perry RH, English P, Forster G, McMeekin W, Slade JY, Golkhar A, Matthews FE, Barber R, Kalaria RN, Ince PG. Comparison of the pathology of cerebral white matter with post-mortem magnetic resonance imaging (MRI) in the elderly brain. Neuropathol Appl Neurobiol. 2004;30:385–395. doi: 10.1111/j.1365-2990.2004.00550.x. [DOI] [PubMed] [Google Scholar]
- Lee DY, Fletcher E, Martinez O, Ortega M, Zozulya N, Kim J, Tran J, Buonocore M, Carmichael O, DeCarli C. Regional pattern of white matter microstructural changes in normal aging, MCI, and AD. Neurology. 2009;73:1722–1728. doi: 10.1212/WNL.0b013e3181c33afb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Walderveen MA, Kamphorst W, Scheltens P, van Waesberghe JH, Ravid R, Valk J, Polman CH, Barkhof F. Histopathologic correlate of hypointense lesions on T1-weighted spin-echo MRI in multiple sclerosis. Neurology. 1998;50:1282–1288. doi: 10.1212/wnl.50.5.1282. [DOI] [PubMed] [Google Scholar]
- Bailey EL, Smith C, Sudlow CLM, Wardlaw JM. Pathology of lacunar ischaemic stroke in humans—a systematic review. Brain Pathol. 2012;22:583–591. doi: 10.1111/j.1750-3639.2012.00575.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris Z, Whiteley WN, Longstreth WT, Jr, Weber F, Lee YC, Tsushima Y, Alphs H, Ladd SC, Warlow C, Wardlaw JM, Al-Shahi Salman R. Incidental findings on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2009;339:b3016. doi: 10.1136/bmj.b3016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666. doi: 10.1136/bmj.c3666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Laat KF, Tuladhar AM, van Norden AGW, Norris DG, Zwiers MP, de Leeuw F-E. Loss of white matter integrity is associated with gait disorders in cerebral small vessel disease. Brain. 2011;134:73–83. doi: 10.1093/brain/awq343. [DOI] [PubMed] [Google Scholar]
- Baezner H, Blahak C, Poggesi A, Pantoni L, Inzitari D, Chabriat H, Erkinjuntti T, Fazekas F, Ferro JM, Langhorne P, O’Brien J, Scheltens P, Visser MC, Wahlund LO, Waldemar G, Wallin A, Hennerici MG. Association of gait and balance disorders with age-related white matter changes: the LADIS study. Neurology. 2008;70:935–942. doi: 10.1212/01.wnl.0000305959.46197.e6. [DOI] [PubMed] [Google Scholar]
- Herrmann LL, Le Masurier M, Ebmeier KP. White matter hyperintensities in late life depression: a systematic review. J Neurol Neurosurg Psychiatry. 2008;79:619–624. doi: 10.1136/jnnp.2007.124651. [DOI] [PubMed] [Google Scholar]
- Turner ST, Jack CR, Fornage M, Mosley TH, Boerwinkle E, de Andrade M. Heritability of leukoaraiosis in hypertensive sibships. Hypertension. 2004;43:483–487. doi: 10.1161/01.HYP.0000112303.26158.92. [DOI] [PubMed] [Google Scholar]
- Altmann-Schneider I, van der Grond J, Slagboom PE, Westendorp RG, Maier AB, van Buchem MA, de Craen AJ. Lower susceptibility to cerebral small vessel disease in human familial longevity: the Leiden Longevity Study. Stroke. 2013;44:9–14. doi: 10.1161/STROKEAHA.112.671438. [DOI] [PubMed] [Google Scholar]
- Valdes Hernandez M, Booth T, Murray C, Gow A, Penke L, Morris Z, Munoz ManiegaS, Royle N, Aribisala B, Bastin M, Starr J, Deary I, Wardlaw J. Brain white matter damage in aging and cognitive ability in youth and older age. Neurobiol Aging. 2013;34:2740–2747. doi: 10.1016/j.neurobiolaging.2013.05.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dufouil C, Alperovitch A, Tzourio C. Influence of education on the relationship between white matter lesions and cognition. Neurology. 2003;60:831–836. doi: 10.1212/01.wnl.0000049456.33231.96. [DOI] [PubMed] [Google Scholar]
- Deary IJ, Bastin ME, Pattie A, Clayden JD, Whalley LJ, Starr JM, Wardlaw JM. White matter integrity and cognition in childhood and old age. Neurology. 2006;66:505–512. doi: 10.1212/01.wnl.0000199954.81900.e2. [DOI] [PubMed] [Google Scholar]
- Dufouil C, De Kersaint-Gilly A, Besancon V, Levy C, Auffray E, Brunnereau L, Alperovitch A, Tzourio C. Longitudinal study of blood pressure and white matter hyperintensities: the EVA MRI Cohort. Neurology. 2001;56:921–926. doi: 10.1212/wnl.56.7.921. [DOI] [PubMed] [Google Scholar]
- van Dijk EJ, Breteler MMB, Schmidt R, Berger K, Nilsson LG, Oudkerk M, Pajak A, Sans S, de Ridder M, Dufouil C, Fuhrer R, Giampaoli S, Launer LJ, Hofman A for the CASCADE Consortium. The association between blood pressure, hypertension, and cerebral white matter lesions: cardiovascular determinants of dementia study. Hypertension. 2004;44:625–630. doi: 10.1161/01.HYP.0000145857.98904.20. [DOI] [PubMed] [Google Scholar]
- Maillard P, Seshadri S, Beiser A, Himali JJ, Au R, Fletcher E, Carmichael O, Wolf PA, DeCarli C. Effects of systolic blood pressure on white-matter integrity in young adults in the Framingham Heart Study: a cross-sectional study. Lancet Neurol. 2012;11:1039–1047. doi: 10.1016/S1474-4422(12)70241-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferguson SC, Blane A, Perros P, McCrimmon RJ, Best JJ, Wardlaw J, Deary IJ, Frier BM. Cognitive ability and brain structure in type 1 diabetes: relation to microangiopathy and preceding severe hypoglycaemia. Diabetes. 2003;52:149–156. doi: 10.2337/diabetes.52.1.149. [DOI] [PubMed] [Google Scholar]
- Gons RA, van Norden AG, de Laat KF, van Oudheusden LJ, van Uden I, Zwiers MP, Norris DG, de Leeuw FE. Cigarette smoking is associated with reduced microstructural integrity of cerebral white matter. Brain. 2011;134:2116–2124. doi: 10.1093/brain/awr145. [DOI] [PubMed] [Google Scholar]
- Staals J, Makin SDJ, Doubal F, Dennis M, Wardlaw JM. Stroke subtype, vascular risk factors and total MRI brain small vessel disease burden. Neurology. 2014;83:1228–1234. doi: 10.1212/WNL.0000000000000837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wardlaw JM, Allerhand M, Doubal FN, Valdes Hernandez M, Morris Z, Gow AJ, Bastin M, Starr JM, Dennis MS, Deary IJ. Vascular risk factors, large artery atheroma and brain white matter hyperintensities. Neurology. 2014;82:1331–1338. doi: 10.1212/WNL.0000000000000312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Debette S, Seshadri S, Beiser A, Au R, Himali JJ, Palumbo C, Wolf PA, DeCarli C. Midlife vascular risk factor exposure accelerates structural brain aging and cognitive decline. Neurology. 2011;77:461–468. doi: 10.1212/WNL.0b013e318227b227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryu WS, Woo SH, Schellingerhout D, Chung MK, Kim CK, Jang MU, Park KJ, Hong KS, Jeong SW, Na JY, Cho KH, Kim JT, Kim BJ, Han MK, Lee J, Cha JK, Kim DH, Lee SJ, Ko Y, Cho YJ, Lee BC, Yu KH, Oh MS, Park JM, Kang K, Lee KB, Park TH, Lee J, Choi HK, Lee K, Bae HJ, Kim DE. Grading and interpretation of white matter hyperintensities using statistical maps. Stroke. 2014;45:3567–3575. doi: 10.1161/STROKEAHA.114.006662. [DOI] [PubMed] [Google Scholar]
- Brisset M, Boutouyrie P, Pico F, Zhu Y, Zureik M, Schilling S, Dufouil C, Mazoyer B, Laurent S, Tzourio C, Debette S. Large-vessel correlates of cerebral small-vessel disease. Neurology. 2013;80:662–669. doi: 10.1212/WNL.0b013e318281ccc2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aribisala BS, Morris Z, Eadie E, Thomas A, Gow A, Valdes Hernandez MC, Royle NA, Bastin ME, Starr J, Deary IJ, Wardlaw JM. Blood pressure, internal carotid artery flow parameters and age-related white matter hyperintensities. Hypertension. 2014;63:1011–1018. doi: 10.1161/HYPERTENSIONAHA.113.02735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singer J, Trollor JN, Baune BT, Sachdev PS, Smith E. Arterial stiffness, the brain and cognition: a systematic review. Ageing Res Rev. 2014;15C:16–27. doi: 10.1016/j.arr.2014.02.002. [DOI] [PubMed] [Google Scholar]
- Dufouil C, Chalmers J, Coskun O, Besancon V, Bousser MG, Guillon P, MacMahon S, Mazoyer B, Neal B, Woodward M, Tzourio-Mazoyer N, Tzourio C. Effects of blood pressure lowering on cerebral white matter hyperintensities in patients with stroke: the PROGRESS (Perindopril Protection Against Recurrent Stroke Study) Magnetic Resonance Imaging Substudy. Circulation. 2005;112:1644–1650. doi: 10.1161/CIRCULATIONAHA.104.501163. [DOI] [PubMed] [Google Scholar]
- Weber R, Weimar C, Blatchford J, Hermansson K, Wanke I, Moller-Hartmann C, Gizewski ER, Forsting M, Demchuck AM, Sacco RL, Saver JL, Warach S, Diener HC, Diehl A for the PRoFESS Imaging Substudy Group. Telmisartan on top of antihypertensive treatment does not prevent progression of cerebral white matter lesions in the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) MRI substudy. Stroke. 2012;43:2336–2342. doi: 10.1161/STROKEAHA.111.648576. [DOI] [PubMed] [Google Scholar]
- Bath PM, Wardlaw JM. Pharmacological treatment and prevention of cerebral small vessel disease: a review of potential interventions. Int J Stroke. 2015;10:469–478. doi: 10.1111/ijs.12466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabayan B, van Vliet P, de Ruijter W, Gussekloo J, de Craen AJ, Westendorp RG. High blood pressure, physical and cognitive function, and risk of stroke in the oldest old: the Leiden 85-Plus Study. Stroke. 2013;44:15–20. doi: 10.1161/STROKEAHA.112.663062. [DOI] [PubMed] [Google Scholar]
- Gow AJ, Bastin ME, Munoz Maniega S, Valdes Hernandez MC, Morris Z, Murray C, Royle NA, Starr JM, Deary IJ, Wardlaw JM. Neuroprotective lifestyles and the aging brain: activity, atrophy and white matter integrity. Neurology. 2012;79:1802–1808. doi: 10.1212/WNL.0b013e3182703fd2. [DOI] [PubMed] [Google Scholar]
- Fleischman DA, Yang J, Arfanakis K, Arvanitakis Z, Leurgans SE, Turner AD, Barnes LL, Bennett DA, Buchman AS. Physical activity, motor function, and white matter hyperintensity burden in healthy older adults. Neurology. 2015;84:1294–1300. doi: 10.1212/WNL.0000000000001417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camicioli R, Verghese J. Physical activity, white matter hyperintensities, and motor function: bringing out the reserves. Neurology. 2015;84:1288–1289. doi: 10.1212/WNL.0000000000001426. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Smith C, Dichgans M. Mechanisms of sporadic cerebral small vessel disease: insights from neuroimaging. Lancet Neurol. 2013;12:483–497. doi: 10.1016/S1474-4422(13)70060-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Makin S, Turpin S, Dennis M, Wardlaw J. Cognitive impairment after lacunar stroke: systematic review and meta-analysis of incidence, prevalence and comparison with other stroke sub-types. J Neurol Neurosurg Psychiatry. 2013;84:893–900. doi: 10.1136/jnnp-2012-303645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vermeer SE, Longstreth WT, Jr, Koudstaal PJ. Silent brain infarcts: a systematic review. Lancet Neurol. 2007;6:611–619. doi: 10.1016/S1474-4422(07)70170-9. [DOI] [PubMed] [Google Scholar]
- Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brain microbleeds: systematic review, subgroup analyses and standards for study design and reporting. Brain. 2007;130:1988–2003. doi: 10.1093/brain/awl387. [DOI] [PubMed] [Google Scholar]
- MacLullich AM, Wardlaw JM, Ferguson KJ, Starr JM, Seckl JR, Deary IJ. Enlarged perivascular spaces are associated with cognitive function in healthy elderly men. J Neurol Neurosurg Psychiatry. 2004;75:1519–1523. doi: 10.1136/jnnp.2003.030858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Royle NA, Booth T, Valdes Hernandez MC, Penke L, Murray C, Gow AJ, Munoz Maniega S, Starr J, Bastin ME, Deary IJ, Wardlaw JM. Estimated maximal and current brain volume predict cognitive ability in old age. Neurobiol Aging. 2013;34:2726–2733. doi: 10.1016/j.neurobiolaging.2013.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Potter GM, Doubal FN, Jackson CA, Chappell FM, Sudlow CL, Dennis MS, Wardlaw JM. Counting cavitating lacunes underestimates the burden of lacunar infarction. Stroke. 2010;41:267–272. doi: 10.1161/STROKEAHA.109.566307. [DOI] [PubMed] [Google Scholar]
- Loos CM, Staals J, Wardlaw JM, van Oostenbrugge RJ. Cavitation of deep lacunar infarcts in patients with first-ever lacunar stroke: a 2-year follow-up study with MR. Stroke. 2012;43:2245–2247. doi: 10.1161/STROKEAHA.112.660076. [DOI] [PubMed] [Google Scholar]
- Moreau F, Patel S, Lauzon ML, McCreary CR, Goyal M, Frayne R, Demchuk AM, Coutts SB, Smith EE. Cavitation after acute symptomatic lacunar stroke depends on time, location, and MRI sequence. Stroke. 2012;43:1837–1842. doi: 10.1161/STROKEAHA.111.647859. [DOI] [PubMed] [Google Scholar]
- Duering M, Csanadi E, Gesierich B, Jouvent E, Herve D, Seiler S, Belaroussi B, Ropele S, Schmidt R, Chabriat H, Dichgans M. Incident lacunes preferentially localize to the edge of white matter hyperintensities: insights into the pathophysiology of cerebral small vessel disease. Brain. 2013;136:2717–2726. doi: 10.1093/brain/awt184. [DOI] [PubMed] [Google Scholar]
- Loos CM, van Oostenbrugge RJ, Staals J. The appearance of a new white matter lesion adjacent to the old infarct in first-ever lacunar stroke patients: a two-year follow-up study with MRI. Cerebrovasc Dis. 2012;34:443–445. doi: 10.1159/000344003. [DOI] [PubMed] [Google Scholar]
- Duering M, Righart R, Csanadi E, Jouvent E, Herve D, Chabriat H, Dichgans M. Incident subcortical infarcts induce focal thinning in connected cortical regions. Neurology. 2012;79:2025–2028. doi: 10.1212/WNL.0b013e3182749f39. [DOI] [PubMed] [Google Scholar]
- de Leeuw F-E, Korf E, Barkhof F, Scheltens P. White matter lesions are associated with progression of medial temporal lobe atrophy in Alzheimer disease. Stroke. 2006;37:2248–2252. doi: 10.1161/01.STR.0000236555.87674.e1. [DOI] [PubMed] [Google Scholar]
- Aribisala BS, Valdes Hernandez MC, Royle NA, Morris Z, Munoz Maniega S, Bastin ME, Deary IJ, Wardlaw JM. Brain atrophy associations with white matter lesions in the ageing brain: the Lothian Birth Cohort 1936. Eur Radiol. 2013;23:1084–1092. doi: 10.1007/s00330-012-2677-x. [DOI] [PubMed] [Google Scholar]
- Rivers CS, Wardlaw JM, Armitage P, Bastin ME, Carpenter TK, Cvoro V, Hand PJ, Dennis MS. Do acute diffusion- and perfusion-weighted MRI lesions identify final infarct volume in ischemic stroke? Stroke. 2006;37:98–104. doi: 10.1161/01.STR.0000195197.66606.bb. [DOI] [PubMed] [Google Scholar]
- Ay H, Arsava EM, Rosand J, Furie KL, Singhal AB, Schaefer PW, Wu O, Gonzalez RG, Koroshetz WJ, Sorensen AG. Severity of leukoaraiosis and susceptibility to infarct growth in acute stroke. Stroke. 2008;39:1409–1413. doi: 10.1161/STROKEAHA.107.501932. [DOI] [PubMed] [Google Scholar]
- The IST-3 Collaborative Group. Association between brain imaging signs, early and late outcomes, and response to intravenous alteplase after acute ischaemic stroke in the third International Stroke Trial (IST-3): secondary analysis of a randomised controlled trial. Lancet Neurol. 2015;14:485–496. doi: 10.1016/S1474-4422(15)00012-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang HJ, Stewart R, Park MS, Bae KY, Kim SW, Kim JM, Shin IS, Cho KH, Yoon JS. White matter hyperintensities and functional outcomes at 2 weeks and 1 year after stroke. Cerebrovasc Dis. 2013;35:138–145. doi: 10.1159/000346604. [DOI] [PubMed] [Google Scholar]
- Liou LM, Chen CF, Guo YC, Cheng HL, Lee HL, Hsu JS, Lin RT, Lin HF. Cerebral white matter hyperintensities predict functional stroke outcome. Cerebrovasc Dis. 2010;29:22–27. doi: 10.1159/000255970. [DOI] [PubMed] [Google Scholar]
- Huijts M, Duits A, van Oostenbrugge RJ, Kroon AA, de Leeuw PW, Staals J. Accumulation of MRI markers of cerebral small vessel disease is associated with decreased cognitive function. A study in first-ever lacunar stroke and hypertensive patients. Front Aging Neurosci. 2013;5:72. doi: 10.3389/fnagi.2013.00072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pantoni L, Garcia JH. Pathogenesis of leukoaraiosis: a review. Stroke. 1997;28:652–659. doi: 10.1161/01.str.28.3.652. [DOI] [PubMed] [Google Scholar]
- Moran C, Phan TG, Srikanth VK. Cerebral small vessel disease: a review of clinical, radiological, and histopathological phenotypes. Int J Stroke. 2012;7:36–46. doi: 10.1111/j.1747-4949.2011.00725.x. [DOI] [PubMed] [Google Scholar]
- Shoamanesh A, Kwok CS, Benavente O. Cerebral microbleeds: histopathological correlation of neuroimaging. Cerebrovasc Dis. 2011;32:528–534. doi: 10.1159/000331466. [DOI] [PubMed] [Google Scholar]
- De Reuck J, Auger F, Cordonnier C, Deramecourt V, Durieux N, Pasquier F, Bordet R, Maurage CA, Leys D. Comparison of 7.0-T T*-magnetic resonance imaging of cerebral bleeds in post-mortem brain sections of Alzheimer patients with their neuropathological correlates. Cerebrovasc Dis. 2011;31:511–517. doi: 10.1159/000324391. [DOI] [PubMed] [Google Scholar]
- Love S, Miners JS. White matter hypoperfusion and damage in dementia: post-mortem assessment. Brain Pathol. 2015;25:99–107. doi: 10.1111/bpa.12223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pantoni L, Sarti C, Alafuzoff I, Jellinger K, Munoz DG, Ogata J, Palumbo V. Postmortem examination of vascular lesions in cognitive impairment: a survey among neuropathological services. Stroke. 2006;37:1005–1009. doi: 10.1161/01.STR.0000206445.97511.ae. [DOI] [PubMed] [Google Scholar]
- Grinberg LT, Heinsen H. Toward a pathological definition of vascular dementia. J Neurol Sci. 2010;299:136–138. doi: 10.1016/j.jns.2010.08.055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deramecourt V, Slade JY, Oakley AE, Perry RH, Ince PG, Maurage CA, Kalaria RN. Staging and natural history of cerebrovascular pathology in dementia. Neurology. 2012;78:1043–1050. doi: 10.1212/WNL.0b013e31824e8e7f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalaria RN, Kenny RA, Ballard CG, Perry R, Ince P, Polvikoski T. Towards defining the neuropathological substrates of vascular dementia. J Neurol Sci. 2004;226:75–80. doi: 10.1016/j.jns.2004.09.019. [DOI] [PubMed] [Google Scholar]
- Fernando MS, Simpson JE, Matthews F, Brayne C, Lewis CE, Barber R, Kalaria RN, Forster G, Esteves F, Wharton SB, Shaw PJ, O’Brien JT, Ince PG. White matter lesions in an unselected cohort of the elderly: molecular pathology suggests origin from chronic hypoperfusion injury. Stroke. 2006;37:1391–1398. doi: 10.1161/01.STR.0000221308.94473.14. [DOI] [PubMed] [Google Scholar]
- Hernandez MC, Piper RJ, Bastin ME, Royle NA, Maniega SM, Aribisala BS, Murray C, Deary IJ, Wardlaw JM. Morphologic, distributional, volumetric, and intensity characterization of periventricular hyperintensities. AJNR Am J Neuroradiol. 2014;35:55–62. doi: 10.3174/ajnr.A3612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim KW, MacFall JR, Payne ME. Classification of white matter lesions on magnetic resonance imaging in elderly persons. Biol Psychiatry. 2008;64:273–280. doi: 10.1016/j.biopsych.2008.03.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fazekas F. Incidental periventricular white matter hyperintensities revisited: what detailed morphologic image analyses can tell us. AJNR Am J Neuroradiol. 2014;35:63–64. doi: 10.3174/ajnr.A3714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moody DM, Brown WR, Challa VR, Anderson RL. Periventricular venous collagenosis: association with leukoaraiosis. Radiology. 1995;194:469–476. doi: 10.1148/radiology.194.2.7824728. [DOI] [PubMed] [Google Scholar]
- Gouw AA, Seewann A, Vrenken H, van der Flier WM, Rozemuller JM, Barkhof F, Scheltens P, Geurts JJ. Heterogeneity of white matter hyperintensities in Alzheimer’s disease: post-mortem quantitative MRI and neuropathology. Brain. 2008;131:3286–3298. doi: 10.1093/brain/awn265. [DOI] [PubMed] [Google Scholar]
- Tomimoto H, Akiguchi I, Suenaga T, Nishimura M, Wakita H, Nakamura S, Kimura J. Alterations of the blood-brain barrier and glial cells in white matter lesions in cerebrovascular and Alzheimer’s disease patients. Stroke. 1996;27:2069–2074. doi: 10.1161/01.str.27.11.2069. [DOI] [PubMed] [Google Scholar]
- Munoz DG. Small vessel disease: neuropathology. Int Psychogeriatr. 2003;15:67–69. doi: 10.1017/S1041610203008986. [DOI] [PubMed] [Google Scholar]
- Giwa MO, Williams J, Elderfield K, Jiwa NS, Bridges LR, Kalaria RN, Markus HS, Esiri MM, Hainsworth AH. Neuropathologic evidence of endothelial changes in cerebral small vessel disease. Neurology. 2012;78:167–174. doi: 10.1212/WNL.0b013e3182407968. [DOI] [PubMed] [Google Scholar]
- Simpson JE, Wharton SB, Cooper J, Gelsthorpe C, Baxter L, Forster G, Shaw PJ, Savva G, Matthews FE, Brayne C, Ince PG. Alterations of the blood-brain barrier in cerebral white matter lesions in the ageing brain. Neurosci Lett. 2010;486:246–251. doi: 10.1016/j.neulet.2010.09.063. [DOI] [PubMed] [Google Scholar]
- Hainsworth AH, Oommen AT, Bridges LR. Endothelial cells and human cerebral small vessel disease. Brain Pathol. 2015;25:44–50. doi: 10.1111/bpa.12224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrall AJ, Wardlaw JM. Blood brain barrier: ageing and microvascular disease—systemic review and meta-analysis. Neurobiol Aging. 2009;30:337–352. doi: 10.1016/j.neurobiolaging.2007.07.015. [DOI] [PubMed] [Google Scholar]
- Ma K-C, Olsson Y. Structural and vascular permeability abnormalities associated with lacunes of the human brain. Acta Neurol Scand. 1993;88:100–107. doi: 10.1111/j.1600-0404.1993.tb04199.x. [DOI] [PubMed] [Google Scholar]
- Ma K-C, Olsson Y. The role of chronic brain oedema in the formation of lacunes in Binswanger’s encephalopathy. Cerebrovasc Dis. 1997;7:324–331. [Google Scholar]
- Lammie GA, Brannan F, Slattery J, Warlow C. Nonhypertensive cerebral small-vessel disease. An autopsy study. Stroke. 1997;28:2222–2229. doi: 10.1161/01.str.28.11.2222. [DOI] [PubMed] [Google Scholar]
- Wharton SB, Simpson JE, Brayne C, Ince PG. Age-associated white matter lesions: the MRC Cognitive Function and Ageing Study. Brain Pathol. 2015;25:35–43. doi: 10.1111/bpa.12219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lammie GA, Brannan F, Wardlaw JM. Incomplete lacunar infarction (type 1b lacunes) Acta Neuropathol. 1998;96:163–171. doi: 10.1007/s004010050877. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Sandercock PA, Dennis MS, Starr J. Is breakdown of the blood-brain barrier responsible for lacunar stroke, leukoaraiosis, and dementia? Stroke. 2003;34:806–812. doi: 10.1161/01.STR.0000058480.77236.B3. [DOI] [PubMed] [Google Scholar]
- Basser PJ, Pierpaoli C. Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. J Magn Reson B. 1996;111:209–219. doi: 10.1006/jmrb.1996.0086. [DOI] [PubMed] [Google Scholar]
- Bastin ME, Sinha S, Whittle IR, Wardlaw JM. Measurements of water diffusion and T1 values in peritumoural oedematous brain. Neuroreport. 2002;13:1335–1340. doi: 10.1097/00001756-200207190-00024. [DOI] [PubMed] [Google Scholar]
- Bastin ME, Sinha S, Whittle IR, Farrall AJ, Wardlaw JM. Diffuse brain oedema in idiopathic intracranial hypertension: a quantitative MR imaging study. J Neurol Neurosurg Psychiatry. 2003;74:1693–1696. doi: 10.1136/jnnp.74.12.1693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muñoz Maniega S, Bastin ME, Armitage PA, Farrall AJ, Carpenter TK, Hand PJ, Cvoro V, Rivers CS, Wardlaw JM. Temporal evolution of water diffusion parameters is different in grey and white matter in human ischaemic stroke. J Neurol Neurosurg Psychiatry. 2004;75:1714–1718. doi: 10.1136/jnnp.2003.033852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bastin ME, Carpenter TK, Armitage PA, Sinha S, Wardlaw JM, Whittle IR. Effects of dexamethasone on cerebral perfusion and water diffusion in patients with high-grade glioma. AJNR Am J Neuroradiol. 2006;27:402–408. [PMC free article] [PubMed] [Google Scholar]
- Bastin ME, Clayden JD, Pattie A, Gerrish IF, Wardlaw JM, Deary IJ. Diffusion tensor and magnetization transfer MRI measurements of periventricular white matter hyperintensities in old age. Neurobiol Aging. 2009;30:125–136. doi: 10.1016/j.neurobiolaging.2007.05.013. [DOI] [PubMed] [Google Scholar]
- Silver NC, Barker GJ, MacManus DG, Tofts PS, Miller DH. Magnetisation transfer ratio of normal brain white matter: a normative database spanning four decades of life. J Neurol Neurosurg Psychiatry. 1997;62:223–228. doi: 10.1136/jnnp.62.3.223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller DH, Thompson AJ, Filippi M. Magnetic resonance studies of abnormalities in the normal appearing white matter and grey matter in multiple sclerosis. J Neurol. 2003;250:1407–1419. doi: 10.1007/s00415-003-0243-9. [DOI] [PubMed] [Google Scholar]
- Naruse S, Horikawa Y, Tanaka C, Hirakawa K, Nishikawa H, Yoshizaki K. Significance of proton relaxation time measurement in brain edema, cerebral infarction and brain tumors. Magn Reson Imaging. 1986;4:293–304. doi: 10.1016/0730-725x(86)91039-8. [DOI] [PubMed] [Google Scholar]
- Heye AK, Culling RD, Valdes Hernandez MC, Thrippleton MJ, Wardlaw JM. Assessment of blood–brain barrier disruption using dynamic contrast-enhanced MRI. A systematic review. Neuroimage Clin. 2014;6:262–274. doi: 10.1016/j.nicl.2014.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tofts PS, Kermode AG. Measurement of the blood-brain barrier permeability and leakage space using dynamic MR imaging. 1. Fundamental concepts. Magn Reson Imaging. 1991;17:357–367. doi: 10.1002/mrm.1910170208. [DOI] [PubMed] [Google Scholar]
- Armitage PA, Farrall AJ, Carpenter TK, Doubal FN, Wardlaw JM. Use of dynamic contrast-enhanced MRI to measure subtle blood-brain barrier abnormalities. Magn Reson Imaging. 2011;29:305–314. doi: 10.1016/j.mri.2010.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barbier EL, Lamalle L, Decorps M. Methodology of brain perfusion imaging. J Magn Reson Imaging. 2001;13:496–520. doi: 10.1002/jmri.1073. [DOI] [PubMed] [Google Scholar]
- Carpenter T, Armitage PA, Bastin ME, Wardlaw JM. DSC perfusion MRI—quantification and reduction of systematic errors arising in areas of reduced cerebral blood flow. Magn Reson Med. 2006;55:1342–1349. doi: 10.1002/mrm.20908. [DOI] [PubMed] [Google Scholar]
- Fazekas F, Ropele S, Enzinger C, Gorani F, Seewann A, Petrovic K, Schmidt R. MTI of white matter hyperintensities. Brain. 2005;128:2926–2932. doi: 10.1093/brain/awh567. [DOI] [PubMed] [Google Scholar]
- O’Sullivan M, Morris RG, Huckstep B, Jones DK, Williams SCR, Markus HS. Diffusion tensor MRI correlates with executive dysfunction in patients with ischaemic leukoaraiosis. J Neurol Neurosurg Psychiatry. 2004;75:441–447. doi: 10.1136/jnnp.2003.014910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Munoz Maniega S, Valdes Hernandez M, Clayden JD, Royle NA, Murray C, Morris Z, Aribisala BS, Gow AJ, Starr JM, Bastin ME, Deary IJ, Wardlaw JM. White matter hyperintensities and normal-appearing white matter integrity in the aging brain. Neurobiol Aging. 2015;36:909–918. doi: 10.1016/j.neurobiolaging.2014.07.048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markus HS, Lythgoe DJ, Ostegaard L, O’Sullivan M, Williams SC. Reduced cerebral blood flow in white matter in ischaemic leukoaraiosis demonstrated using quantitative exogenous contrast based perfusion MRI. J Neurol Neurosurg Psychiatry. 2000;69:48–53. doi: 10.1136/jnnp.69.1.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Sullivan M, Lythgoe DJ, Pereira AC, Summers PE, Jarosz JM, Williams SC, Markus HS. Patterns of cerebral blood flow reduction in patients with ischemic leukoaraiosis. Neurology. 2002;59:321–326. doi: 10.1212/wnl.59.3.321. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Doubal FN, Eadie E, Chappell F, Shuler K, Cvoro V. Little association between intracranial arterial stenosis and lacunar stroke. Cerebrovasc Dis. 2011;31:12–18. doi: 10.1159/000319773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ten Dam H, van den Heuvel D, de Craen A, Bollen E, Murray H, Westendorp R, Blauw G, van Buchem M. Decline in total cerebral blood flow is linked with increase in periventricular but not deep white matter hyperintensities. Radiology. 2007;243:198–203. doi: 10.1148/radiol.2431052111. [DOI] [PubMed] [Google Scholar]
- Appelman APA, van der Graaf Y, Vincken KL, Tiehuis AM, Witkamp TD, Mali WPTM, Geerlings MI for the SMART Study Group. Total cerebral blood flow, white matter lesions and brain atrophy: the SMART-MR study. J Cereb Blood Flow Metab. 2008;28:633–639. doi: 10.1038/sj.jcbfm.9600563. [DOI] [PubMed] [Google Scholar]
- Picano E, Bruno RM, Ferrari GF, Bonuccelli U. Cognitive impairment and cardiovascular disease: so near, so far. Int J Cardiol. 2014;175:21–29. doi: 10.1016/j.ijcard.2014.05.004. [DOI] [PubMed] [Google Scholar]
- Kraut MA, Beason-Held LL, Elkins WD, Resnick SM. The impact of magnetic resonance imaging-detected white matter hyperintensities on longitudinal changes in regional cerebral blood flow. J Cereb Blood Flow Metab. 2008;28:190–197. doi: 10.1038/sj.jcbfm.9600512. [DOI] [PubMed] [Google Scholar]
- Spilt A, Goekoop R, Westendorp RG, Blauw GJ, de Craen AJ, van Buchem MA. Not all age-related white matter hyperintensities are the same: a magnetization transfer imaging study. AJNR Am J Neuroradiol. 2006;27:1964–1968. [PMC free article] [PubMed] [Google Scholar]
- Maillard P, Fletcher E, Harvey D, Carmichael O, Reed B, Mungas D, DeCarli C. White matter hyperintensity penumbra. Stroke. 2011;42:1917–1922. doi: 10.1161/STROKEAHA.110.609768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maillard P, Fletcher E, Lockhart SN, Roach AE, Reed B, Mungas D, DeCarli C, Carmichael OT. White matter hyperintensities and their penumbra lie along a continuum of injury in the aging brain. Stroke. 2014;45:1721–1726. doi: 10.1161/STROKEAHA.113.004084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leritz EC, Shepel J, Williams VJ, Lipsitz LA, McGlinchey RE, Milberg WP, Salat DH. Associations between T1 white matter lesion volume and regional white matter microstructure in aging. Hum Brain Mapp. 2014;35:1085–1100. doi: 10.1002/hbm.22236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brickman AM, Zahra A, Muraskin J, Steffener J, Holland CM, Habeck C, Borogovac A, Ramos MA, Brown TR, Asllani I, Stern Y. Reduction in cerebral blood flow in areas appearing as white matter hyperintensities on magnetic resonance imaging. Psychiatry Res. 2009;172:117–120. doi: 10.1016/j.pscychresns.2008.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uh J, Yezhuvath U, Cheng Y, Lu H. In vivo vascular hallmarks of diffuse leukoaraiosis. J Magn Reson Imaging. 2010;32:184–190. doi: 10.1002/jmri.22209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Topakian R, Barrick TR, Howe FA, Markus HS. Blood-brain barrier permeability is increased in normal-appearing white matter in patients with lacunar stroke and leucoaraiosis. J Neurol Neurosurg Psychiatry. 2010;81:192–197. doi: 10.1136/jnnp.2009.172072. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Doubal F, Armitage P, Chappell F, Carpenter T, Maniega SM, Farrall A, Sudlow C, Dennis M, Dhillon B. Lacunar stroke is associated with diffuse blood-brain barrier dysfunction. Ann Neurol. 2009;65:194–202. doi: 10.1002/ana.21549. [DOI] [PubMed] [Google Scholar]
- Taheri S, Gasparovic C, Huisa BN, Adair JC, Edmonds E, Prestopnik J, Grossetete M, Shah NJ, Wills J, Qualls C, Rosenberg GA. Blood-brain barrier permeability abnormalities in vascular cognitive impairment. Stroke. 2011;42:2158–2163. doi: 10.1161/STROKEAHA.110.611731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Firbank MJ, Minett T, O’Brien JT. Changes in DWI and MRS associated with white matter hyperintensities in elderly subjects. Neurology. 2003;61:950–954. doi: 10.1212/01.wnl.0000086375.33512.53. [DOI] [PubMed] [Google Scholar]
- Taylor WD, Bae JN, MacFall JR, Payne ME, Provenzale JM, Steffens DC, Krishnan KR. Widespread effects of hyperintense lesions on cerebral white matter structure. AJR Am J Roentgenol. 2007;188:1695–1704. doi: 10.2214/AJR.06.1163. [DOI] [PubMed] [Google Scholar]
- Vernooij MW, de Groot M, van der Luqt L, Ikram M, Krestin GP, Hofman A, Niessen WJ, Breteler MMB. White matter atrophy and lesion formation explain the loss of structural integrity of white matter in aging. Neuroimage. 2008;43:470–477. doi: 10.1016/j.neuroimage.2008.07.052. [DOI] [PubMed] [Google Scholar]
- Bennett IJ, Madden DJ, Vaidya CJ, Howard DV, Howard JH., Jr Age-related differences in multiple measures of white matter integrity: a diffusion tensor imaging study of healthy aging. Hum Brain Mapp. 2010;31:378–390. doi: 10.1002/hbm.20872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsu JL, Van Hecke W, Bai CH, Lee CH, Tsai YF, Chiu HC, Jaw FS, Hsu CY, Leu JG, Chen WH, Leemans A. Microstructural white matter changes in normal aging: a diffusion tensor imaging study with higher-order polynomial regression models. Neuroimage. 2010;49:32–43. doi: 10.1016/j.neuroimage.2009.08.031. [DOI] [PubMed] [Google Scholar]
- Zhuang L, Sachdev PS, Trollor JN, Kochan NA, Reppermund S, Brodaty H, Wen W. Microstructural white matter changes in cognitively normal individuals at risk of amnestic MCI. Neurology. 2012;79:748–754. doi: 10.1212/WNL.0b013e3182661f4d. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Doubal FN, Valdes-Hernandez MC, Wang X, Chappell FM, Shuler K, Armitage P, Carpenter T, Dennis MS. Blood-brain barrier permeability and long term clinical and imaging outcomes in cerebral small vessel disease. Stroke. 2013;44:525–527. doi: 10.1161/STROKEAHA.112.669994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valdes Hernandez MC, Gallacher PJ, Bastin ME, Royle NA, Maniega SM, Deary IJ, Wardlaw JM. Automatic segmentation of brain white matter and white matter lesions in normal aging: comparison of five multispectral techniques. Magn Reson Imaging. 2012;30:222–229. doi: 10.1016/j.mri.2011.09.016. [DOI] [PubMed] [Google Scholar]
- Wang X, Valdes Hernandez MC, Doubal F, Chappell FM, Wardlaw JM. How much do focal infarcts distort white matter lesions and global cerebral atrophy measures? Cerebrovasc Dis. 2012;34:336–342. doi: 10.1159/000343226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Payne ME, Fetzer DL, MacFall JR, Provenzale JM, Byrum CE, Krishnan KRR. Development of a semi-automated method for quantification of MRI gray and white matter lesions in geriatric subjects. Psychiatry Res. 2002;115:63–77. doi: 10.1016/s0925-4927(02)00009-4. [DOI] [PubMed] [Google Scholar]
- Wang X. 2013. University of Edinburgh The role of blood brain failure in progression of cerebral small vessel disease: a detailed magnetic resonance imaging study.
- Gawne-Cain ML, Silver NC, Moseley IF, Miller DH. Fast FLAIR of the brain: the range of appearances in normal subjects and its application to quantification of white-matter disease. Neuroradiology. 1997;39:243–249. doi: 10.1007/s002340050402. [DOI] [PubMed] [Google Scholar]
- Alkan O, Kizilkilic O, Yildirim T, Alibek S. Comparison of contrast-enhanced T1-weighted FLAIR with BLADE, and spin-echo T1-weighted sequences in intracranial MRI. Diagn Interv Radiol. 2009;15:75–80. [PubMed] [Google Scholar]
- Bailey WM. Fast fluid attenuated inversion recovery (FLAIR) imaging and associated artefacts in magnetic resonance imaging (MRI) Radiography. 2007;13:283–290. [Google Scholar]
- Bakshi R, Caruthers SD, Janardhan V, Wasay M. Intraventricular CSF pulsation artifact on fast fluid-attenuated inversion-recovery MR images: analysis of 100 consecutive normal studies. AJNR Am J Neuroradiol. 2000;21:503–508. [PMC free article] [PubMed] [Google Scholar]
- Kallmes DF, Hui FK, Mugler JP., III Suppression of cerebrospinal fluid and blood flow artifacts in FLAIR MR imaging with a single-slab three-dimensional pulse sequence: initial experience. Radiology. 2001;221:251–255. doi: 10.1148/radiol.2211001712. [DOI] [PubMed] [Google Scholar]
- Lummel N, Schoepf V, Burke M, Brueckmann H, Linn J. 3D fluid-attenuated inversion recovery imaging: reduced CSF artifacts and enhanced sensitivity and specificity for subarachnoid hemorrhage. AJNR Am J Neuroradiol. 2011;32:2054–2060. doi: 10.3174/ajnr.A2682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stuckey SL, Goh TD, Heffernan T, Rowan D. Hyperintensity in the subarachnoid space on FLAIR MRI. AJR Am J Roentgenol. 2007;189:913–921. doi: 10.2214/AJR.07.2424. [DOI] [PubMed] [Google Scholar]
- Lisanti C, Carlin C, Banks KP, Wang D. Normal MRI appearance and motion-related phenomena of CSF. AJR Am J Roentgenol. 2007;188:716–725. doi: 10.2214/AJR.05.0003. [DOI] [PubMed] [Google Scholar]
- Vargas MI, Delavelle J, Kohler R, Becker CD, Lovblad K. Brain and spine MRI artifacts at 3Tesla. J Neuroradiol. 2009;36:74–81. doi: 10.1016/j.neurad.2008.08.001. [DOI] [PubMed] [Google Scholar]
- Naganawa S, Koshikawa T, Nakamura T, Kawai H, Fukatsu H, Ishigaki T, Komada T, Maruyama K, Takizawa O. Comparison of flow artifacts between 2D-FLAIR and 3D-FLAIR sequences at 3 T. Eur Radiol. 2004;14:1901–1908. doi: 10.1007/s00330-004-2372-7. [DOI] [PubMed] [Google Scholar]
- Neema M, Guss ZD, Stankiewicz JM, Arora A, Healy BC, Bakshi R. Normal findings on brain fluid-attenuated inversion recovery MR images at 3T. AJNR Am J Neuroradiol. 2009;30:911–916. doi: 10.3174/ajnr.A1514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willinek WA, Gieseke J, von Falkenhausen M, Neuen B, Schild HH, Kuhl CK. Sensitivity encoding for fast MR imaging of the brain in patients with stroke. Radiology. 2003;228:669–675. doi: 10.1148/radiol.2283020243. [DOI] [PubMed] [Google Scholar]
- Nyberg E, Sandhu GS, Jesberger J, Blackham KA, Hsu DP, Griswold MA, Sunshine JL. Comparison of brain MR images at 1.5T using BLADE and rectilinear techniques for patients who move during data acquisition. AJNR Am J Neuroradiol. 2012;33:77–82. doi: 10.3174/ajnr.A2737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valdes Hernandez MC, Piper RJ, Wang X, Deary IJ, Wardlaw JM. Towards the automatic computational assessment of enlarged perivascular spaces on brain magnetic resonance images: a systematic review. J Magn Reson Imaging. 2013;38:774–785. doi: 10.1002/jmri.24047. [DOI] [PubMed] [Google Scholar]
- Naganawa S, Kawai H, Fukatsu H, Ishigaki T, Komada T, Maruyama K, Takizawa O. High-speed imaging at 3 Tesla: a technical and clinical review with an emphasis on whole-brain 3D imaging. Magn Reson Med Sci. 2004;3:177–187. doi: 10.2463/mrms.3.177. [DOI] [PubMed] [Google Scholar]
- Wardlaw JM, Brindle W, Casado AM, Shuler K, Henderson M, Thomas B, Macfarlane J, Munoz Maniega S, Lymer K, Morris Z, Pernet C, Nailon W, Ahearn T, Mumuni AN, Mugruza C, McLean J, Chakirova G, Tao YT, Simpson J, Stanfield AC, Johnston H, Parikh J, Royle NA, DeWilde J, Bastin ME, Weir N, Farrall A, Valdes Hernandez MC. A systematic review of the utility of 1.5 versus 3 Tesla magnetic resonance brain imaging in clinical practice and research. Eur Radiol. 2012;22:2295–2303. doi: 10.1007/s00330-012-2500-8. [DOI] [PubMed] [Google Scholar]
- Di Perri C, Dwyer MG, Bergsland N, Schirda C, Poloni GU, Wack D, Cox JL, Dalaker TO, Ranza L, Saluste E, Hussein S, Bastianello S, Zivadinov R. White matter hyperintensities on 1.5 and 3 Tesla brain MRI in healthy individuals. J Biomed Graph Comput. 2013;3:53–62. [Google Scholar]
- Huppertz HJ, Kroll-Seger J, Kloppel S, Ganz RE, Kassubek J. Intra- and interscanner variability of automated voxel-based volumetry based on a 3D probabilistic atlas of human cerebral structures. Neuroimage. 2010;49:2216–2224. doi: 10.1016/j.neuroimage.2009.10.066. [DOI] [PubMed] [Google Scholar]
- Modat M, Ridgway GR, Taylor ZA, Lehmann M, Barnes J, Hawkes DJ, Fox NC, Ourselin S. Fast free-form deformation using graphics processing units. Comput Methods Programs Biomed. 2010;98:278–284. doi: 10.1016/j.cmpb.2009.09.002. [DOI] [PubMed] [Google Scholar]
- van der Zwan A, Hillen B. Review of the variability of the territories of the major cerebral arteries. Stroke. 1991;22:1078–1084. doi: 10.1161/01.str.22.8.1078. [DOI] [PubMed] [Google Scholar]
- van Laar PJ, Hendrikse J, Golay X, Lu H, van Osch MJ, van der Grond J. In vivo flow territory mapping of major brain feeding arteries. Neuroimage. 2006;29:136–144. doi: 10.1016/j.neuroimage.2005.07.011. [DOI] [PubMed] [Google Scholar]
- de Bresser J, Tiehuis AM, van den Berg E, Reijmer YD, Jongen C, Kappelle LJ, Mali WP, Viergever MA, Biessels GJ. Progression of cerebral atrophy and white matter hyperintensities in patients with type 2 diabetes. Diabetes Care. 2010;33:1309–1314. doi: 10.2337/dc09-1923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Callisaya ML, Beare R, Phan TG, Blizzard L, Thrift AG, Chen J, Srikanth VK. Brain structural change and gait decline: a longitudinal population-based study. J Am Geriatr Soc. 2013;61:1074–1079. doi: 10.1111/jgs.12331. [DOI] [PubMed] [Google Scholar]
- Grool AM, van der Graaf Y, Witkamp TD, Vincken KL, Mali WP, Geerlings MI. Progression of white matter lesion volume and health-related quality of life in patients with symptomatic atherosclerotic disease: the SMART-MR study. J Aging Res. 2011;2011:280630. doi: 10.4061/2011/280630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verhaaren BF, Vernooij MW, de Boer R, Hofman A, Niessen WJ, van der Lugt A, Ikram MA. High blood pressure and cerebral white matter lesion progression in the general population. Hypertension. 2013;61:1354–1359. doi: 10.1161/HYPERTENSIONAHA.111.00430. [DOI] [PubMed] [Google Scholar]
- Maillard P, Crivello F, Dufouil C, Tzourio-Mazoyer N, Tzourio C, Mazoyer B. Longitudinal follow-up of individual white matter hyperintensities in a large cohort of elderly. Neuroradiology. 2009;51:209–220. doi: 10.1007/s00234-008-0489-0. [DOI] [PubMed] [Google Scholar]
- Valdes Hernandez MC, Morris Z, Dickie DA, Royle NA, Munoz Maniega S, Aribisala BS, Bastin ME, Deary IJ, Wardlaw JM. Close correlation between quantitative and qualitative assessments of white matter lesions. Neuroepidemiology. 2012;40:13–22. doi: 10.1159/000341859. [DOI] [PubMed] [Google Scholar]
- Moriya Y, Kozaki K, Nagai K, Toba K. Attenuation of brain white matter hyperintensities after cerebral infarction. AJNR Am J Neuroradiol. 2009;30:E43. doi: 10.3174/ajnr.A1340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Dijk EJ, Prins ND, Vrooman HA, Hofman A, Koudstaal PJ, Breteler MM. Progression of cerebral small vessel disease in relation to risk factors and cognitive consequences: Rotterdam Scan study. Stroke. 2008;39:2712–2719. doi: 10.1161/STROKEAHA.107.513176. [DOI] [PubMed] [Google Scholar]
- Schmidt R, Enzinger C, Ropele S, Schmidt H, Fazekas F. Progression of cerebral white matter lesions: 6-year results of the Austrian Stroke Prevention Study. Lancet. 2003;361:2046–2048. doi: 10.1016/s0140-6736(03)13616-1. [DOI] [PubMed] [Google Scholar]
- Prins ND, van Straaten ECW, van Dijk EJ, Simoni M, van Schijndel RA, Vrooman HA, Koudstaal PJ, Scheltens P, Breteler MMB, Barkhof F. Measuring progression of cerebral white matter lesions on MRI. Visual rating and volumetrics. Neurology. 2004;62:1533–1539. doi: 10.1212/01.wnl.0000123264.40498.b6. [DOI] [PubMed] [Google Scholar]
- Yao M, Jouvent E, Duering M, Godin O, Herve D, Guichard JP, Zhu YC, Gschwendtner A, Opherk C, Dichgans M, Chabriat H. Extensive white matter hyperintensities may increase brain volume in cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Stroke. 2012;43:3252–3257. doi: 10.1161/STROKEAHA.112.664854. [DOI] [PubMed] [Google Scholar]
- Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, Mitnitski A. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173:489–495. doi: 10.1503/cmaj.050051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signal abnormalities at 1.5T in Alzheimer’s dementia and normal aging. AJR Am J Roentgenol. 1987;149:351–356. doi: 10.2214/ajr.149.2.351. [DOI] [PubMed] [Google Scholar]