

Abstract
A 75-year-old man presented with a slowly growing mass at the right side of the base of the tongue for 4 months. The mass was painless initially but had become very painful during preceding 4 weeks. On examination a 3 cm diameter, oval swelling was observed at the right side of the base of the tongue. It was firm in consistency, slightly tender, non-ulcerative, and with irregular surface. A deep incisional biopsy was taken from mass under general anesthesia. Histopathology report identified the mass consistent with neurofibroma. It featured typical pallisading arrangement of fascicles of spindle-shaped cells and there was no evidence of malignancy. An absence of Verocay body and thick hyalinized vessels ruled out Schwannoma. No similar lesions were found in any other part of the patient's body. He exhibited no skin pigmentation, no hearing deficit, and no evidence suggestive of any systemic disorders that might have been attributable to the tongue base neurofibroma. His family history was also negative. Thus, a diagnosis of isolated neurofibroma of the tongue was established. The patient was advised excision of the mass but he refused and lost in follow up.
Keywords: Base of the tongue, neurofibroma, solitary
What was known?
Neurofibromas present as either solitary mass or as part of neurofibromatosis syndrome. Oral cavity neurofibromas are characteristically associated with multiple lesions elsewhere in the body and are manifestations of neurofibromatosis type 1 (von Recklinghausen syndrome) or neurofibromatosis type 2 (bilateral acoustic neuroma/central neurofibromatosis). Though tongue is the most common location but the base of the tongue is the rare site of affection.
Introduction
Neurofibromas may present either as a solitary lesion or as part of a syndrome, i.e. neurofibromatosis. When only one or two such lesions are found they are generally sporadic in nature without any internal manifestations. The diagnosis of neurofibromatosis should be considered when three or more of them are present. They are associated with developmental changes in nervous system, bones and skin. Multiple neurofibromas have also been associated with polyglandular syndrome multiple endocrine neoplasia type 3.[1] Clinicopathologic subtypes of neurofibroma include localized neurofibroma (sporadic neurofibroma), diffuse neurofibroma, plexiform neurofibroma, and epithelioid neurofibroma. Localized or solitary neurofibroma develops along a peripheral nerve as a focal mass with well-defined margins but is not encapsulated. This differs from a plexiform neurofibroma which arises from multiple nerves, usually as a solitary large pendulous mass with overlying pigmentation and is encapsulated. Most of them appear in the third to fourth decades of life but may also occur during the teenage years.
When a neurofibroma grows in the head and neck region, it presents with symptoms, such as upper airway obstruction, swallowing difficulty, mastication deficits, or cosmetic distortion of the face.[2] Microscopically the tumor is composed of an irregular pattern of proliferative spindle cells. The stroma is composed of collagen fibers and mucoid masses. Neurofibromas are immunopositive for the S-100 protein in 85% to 100% of the cases, indicating its neural origin.
Here we describe a case of oral solitary neurofibroma appearing unusually from the right side of the base of the tongue leading to mechanical obstruction manifesting as difficulty in deglutition, nasal regurgitation and nasal intonation of voice.
Case Report
A 75-year-old male patient presented with difficulty in swallowing for 4 months. He also complained of a gradually increasing painless tongue swelling along with slight difficulty in mobility for the same duration. The patient had slight breathing difficulty along with nasal intonation in voice and nasal regurgitation of food. On examination, there was a circumscribed sessile swelling of about 3 cm diameter at the right side of the base of the tongue [Figure 1]. There was no evidence of macroglossia. Lateral soft tissue X-ray was done which showed a radio-opaque mass at the base of the tongue. X-ray skull revealed no apparent abnormality. Radio-iodine scan excluded lingual thyroid by showing a normally situated thyroid and there was no uptake in the mass. CT scan showed mass of low density at the base of the tongue.
Figure 1.
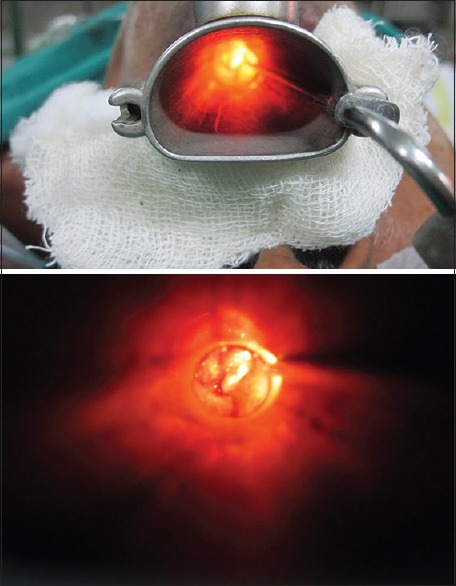
Patient presenting with a solitary swelling at the base of the tongue, leading to mild airway obstruction
A direct laryngoscopic biopsy with tracheostomy was planned under general anesthesia. A deep incisional biopsy was taken from the swelling. Microscopy revealed that the circumscribed but un-encapsulated tumor consisted of proliferation of interlacing bundles of spindle cells with wavy nuclei [Figure 2]. Spindle cells were intermixed with foci comprising dense bundles of collagen fibers giving a whirling pattern [Figure 3]. Pathological diagnosis was a neurofibroma with no signs of malignancy.
Figure 2.
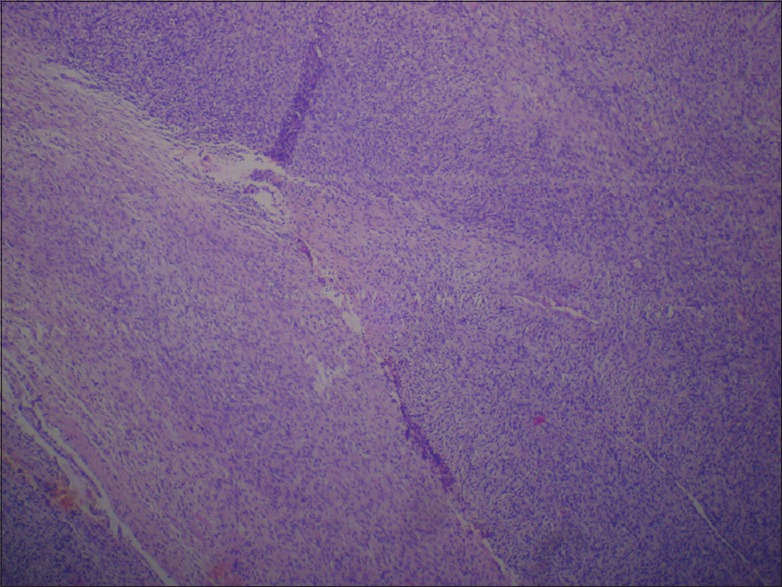
Histopathology of the lesion in × 100 in H and E stain showing interlacing bundles of spindle cells with wavy nuclei. Spindle cells were intermixed with foci comprising dense bundles of collagen fibers giving a whirling pattern
Figure 3.
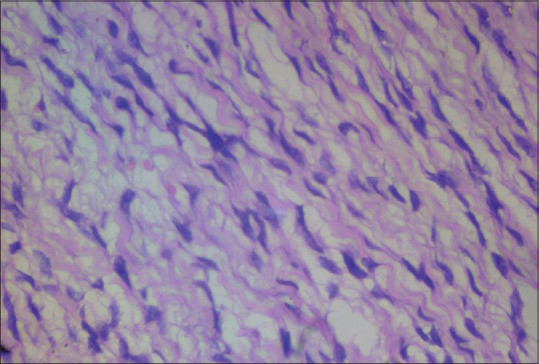
Histopathology of the lesion in × 400 in H and E stain showing interlacing bundles of spindle cells
The patient had no café-au-lait spots, any hearing deficits, or any lisch nodules on slit-lamp examination. There was no history of the presence of similar illness, or any history suggestive of neurofibromatosis in the family.
Discussion
Solitary neurofibroma is a hyperplastic hamartomatous malformations rather than a neoplastic disease originating from the nerves that is composed of Schwann cells, perineural cells and fibroblasts.[3] Generally, neurofibromas present as either solitary mass or as part of neurofibromatosis syndrome. 25% of all neurofibromas occur in head and neck region. About 6.5% of patients have oral manifestation.[4] The following are the common distribution found in the literature: Tongue, palate, mandibular ridge/vestibule, maxillary ridge/vestibule, buccal mucosa, lip, gingiva.[2] The tongue is the most common site affected.[5] The base of the tongue is a relatively rare location and it is important to note in this context that tumors in this region may lead to an upper airway obstruction.[6] Reports of solitary neurofibroma arising from the base of the tongue from India have been rare too. Only one case has been reported so far.[7]
Oral cavity neurofibromas are characteristically associated with multiple lesions elsewhere in the body and are manifestations of neurofibromatosis type 1 (von Recklinghausen syndrome) or neurofibromatosis type 2 (bilateral acoustic neuroma/central neurofibromatosis). Isolated neurofibromas in the oral cavity, on the other hand, are very rare.[8,9] The case discussed here is a solitary neurofibroma not being associated with café au lait macules, skeletal abnormality, and Lisch nodule. Clinically, oral neurofibromas usually appear as pedunculated or sessile nodule, with slow growth. They are usually painless, but pain or paresthesia may occur due to nerve compression. Tumors arising from the base of the tongue may also present with signs of mechanical obstruction.
The case in our discussion is a solitary, sessile relatively huge neurofibroma of the floor of the mouth leading to mechanical obstruction to the upper airways, difficulty in deglutition and nasal intonation of voice.
The etiology of isolated neurofibromas is largely unknown, and they appear to develop sporadically. Some studies have suggested that they represent more of a hamartoma or simple hyperplasia than a true neoplastic lesion.[3]
It is important to differentiate the other swellings of the base of the tongue. Differential diagnosis includes lingual thyroid, lipoma, foregut duplication cyst, lymphatic hemangioma, vascular malformations, infection of tongue, schwannoma, malignant neoplasm. On CT scan, lingual thyroids are characteristically hyperattenuating relative to muscle due to (a) the iodine content of thyroid tissue and (b) moderate contrast enhancement. Lipomas are usually easily identified, well-encapsulated lesions with the attenuation or signal intensity of fat. Foregut duplication cysts are rarely seen in the root of the tongue. Lingual hemangiomas enhance intensely and often have prominent lesional and perilesional vasculature. An abscess usually has a more acute onset, painful and manifest as thick-rim enhancing fluid-attenuated lesions.
CT scan in our case showed mass of low density at the base of the tongue but a definitive diagnosis of such lesion is thus established only by histopathological examination which shows well circumscribed but unencapsulated mass with proliferation of spindled cells with wavy nuclei in whorling pattern, neural bundles and blood vessels. An absence of Verocay bodies (Antoni type A areas) and thick hyalinized blood vessels ruled out a schwannoma. Thus, histopathology is of immense value in establishing definitive diagnosis and also to rule out the possibility of malignancy.[10]
What is new?
Solitary neurofibroma presenting in the oral cavity at an uncommon site i.e. the base of the tongue.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Depprich R, Singh DD, Reinecke P, Kübler NR, Handschel J. Solitary submucous neurofibroma of the mandible: Review of the literature and report of a rare case. Head Face Med. 2009;5:24. doi: 10.1186/1746-160X-5-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Maruyama M, Fushiki H, Watanabe Y. Solitary Neurofibroma of the Floor of the Mouth: A case report. Case Rep Otolaryngol 2011. 2011 doi: 10.1155/2011/967896. 967896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Marocchio LS, Oliveira DT, Pereira MC, Soares CT, Fleury RN. Sporadic and multiple neurofibromas in the head and neck region: A retrospective study of 33 years. Clin Oral Investig. 2007;11:165–9. doi: 10.1007/s00784-006-0096-6. [DOI] [PubMed] [Google Scholar]
- 4.Geist JR, Gander DL, Stefanac SJ. Oral manifestations of neurofibromatosis types I and II. Oral Surg Oral Med Oral Pathol. 1992;73:376–82. doi: 10.1016/0030-4220(92)90139-h. [DOI] [PubMed] [Google Scholar]
- 5.Cherrick HM, Eversole LR. Benign neural sheath neoplasm of the oral cavity: Report of thirty-seven cases. Oral Surg Oral Med Oral Pathol. 1971;32:900–9. doi: 10.1016/0030-4220(71)90177-0. [DOI] [PubMed] [Google Scholar]
- 6.Papadopoulos H, Zachariades N, Angelopoulos AP. Neurofibroma of the mandible: Review of the literature and report of a case. Int J Oral Surg. 1981;10:293–7. doi: 10.1016/s0300-9785(81)80074-9. [DOI] [PubMed] [Google Scholar]
- 7.Dutta M, Ghatak S. Isolated neurofibroma of the tongue presenting as a papilloangiomatous mass. Ear Nose Throat J. 2011;90:58–9. doi: 10.1177/014556131109000205. [DOI] [PubMed] [Google Scholar]
- 8.Lahoz Zamarro MT, GaWe Royo A. Neurofibroma of the tongue. An Otorrinolaringol Ibero Am. 1990;17:287–95. [PubMed] [Google Scholar]
- 9.Gariboldi LM, Avanzini F, Ferri T. Neurofibroma of the tongue: A clinical case. Acta Biomed Ateneo Parmense. 1984;55:311–4. [PubMed] [Google Scholar]
- 10.Surwald CJ, Salam MA, Rowe RC. A solitary neurofibroma of the palatine tonsil. J Laryngol Otol. 2002;116:1050–2. doi: 10.1258/002221502761698838. [DOI] [PubMed] [Google Scholar]