

Abstract
Spindle-cell hemangioendothelioma (SCHE) comprise a rare subset of vascular tumors, and here, we describe such a case and review the clinical presentation, patho-physiology, differential diagnosis of these tumors to promote early identification and discussion guidance. A 25-years-old male patient presented with multiple painful elevated swellings of both left upper and lower extremities for last 15 years without any systemic involvement. After excluding close differential diagnosis by relevant investigations an excisional biopsy was performed. Based on clinical, radiological and histopathological findings, diagnosis of SCHE was made and full thickness excision and skin grafting were performed. The case is reported due to its rarity and adds our knowledge to the existing literature.
Keywords: Hemangioendothelioma, vascular tumor, spindle cell
What was known?
Spindle-cell hemangioendothelioma is a very rare benign vascular tumor of skin predominantly affecting the lower extremity of young adults.
Introduction
Spindle-cell hemangioendothelioma (SCHE) is a rare vascular tumor that was first described in 1986 by Sharon Weiss.[1] SCHE commonly starts at childhood or young adult though the tumor may affect all the age group.[2] Males and females are equally affected by this tumor. Clinically, the tumor presents as a superficially located firm red to brown nodules on the distal extremities. Most of the reports found that the most common site of occurrence of the tumor is the lower extremities.[2,3] Histologically, multiple cavernous blood vessels alternating with cellular areas consist of collapsed vascular spaces separated by spindle shaped fibroblastic cells constitute the bulk of the tumor. Here, we present a young adult who presented to us with multiple spindle cell hemangioendotheliomas. The case is reported due to its rarity.
Case Report
A 25-year-old male patient presented to outpatient department of tertiary care hospital with multiple painful elevated swellings of both left upper and lower extremities for last 15 years. Fifteen years back, he first noticed a small pea-shaped mildly painful swelling on the center of his chest. Subsequently the number of the lesions increased in number as well as in size and new lesions appeared on left foot, thigh, hand and forearm. These lesions initially were firm, but with progression of the disease some of the lesions became soft. No history of fever or systemic symptom was associated. No history of aggravation following trauma. No history of gastrointestinal bleeding or pathological fracture was present. With above complaints, the patient attended to local doctor and applied some ayurvedic medications over the lesions and developed some oozing and crusting and blister formation with serosangunous discharge from the dorsal aspect of the left foot. With this scenario he was referred to the OPD of a tertiary care hospital.
Examination of the lesions revealed multiple nodules and tumors of 2–6 cm in size distributed over planter and dorsal aspect of left foot [Figure 1], dorsal aspect of left hand and fingers [Figure 2] and front and back of the left leg. Most of the lesions were oval to globular in shape, skin colored and with a well-defined margin. Some of the lesion showed crusting, oozing and post-inflammatory hyper-pigmentations.
Figure 1.

Multiple skin-colored well-defined nodules and tumors 2–6 cm on planter and dorsal aspect of left foot
Figure 2.

Multiple skin-colored well-defined nodules and tumors 2–6 cm on dorsal aspect of left hand and fingers
Lesions were non-tender, soft to firm in consistency and partially compressible. Complete hemogram, sugar, urea, creatinine urine analyses were within the normal limits. However, liver function tests revealed elevation of transaminase level (SGOT-71, SGPT-114 and ALP-181). Chest X-ray was normal. X-ray of the hand and feet showed soft tissue swelling with calcification without any bony abnormality. We carried out color Doppler study of the patient which revealed dilated veins with phleboleiths.
Most interestingly, histopathology of the patient revealed multiple vascular spaces; some were dilated and other were collapsed with slit-like openings. Some of the intravascular areas were showing intramural thrombi. The cellular elements of the tumor were mainly composed of multiple spindle-shaped cells with vesicular nucleus [Figure 3]. Based on clinical, radiological and histopathological findings, diagnosis of SCHE was made and the patient was referred to plastic surgeon and excision followed by full thickness skin grafting was done of the leg lesions. However, the result was unacceptable to the patient. The patient was lost to follow-up after discharge.
Figure 3.
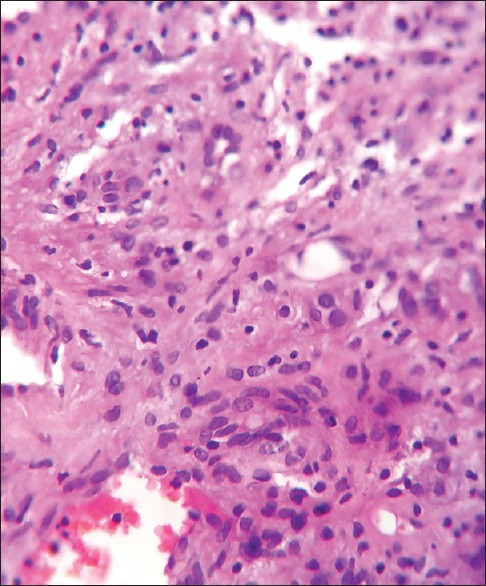
H and E staining showing multiple cavernous blood vessels alternating with cellular areas consisting of collapsed vascular spaces separated by spindle-shaped fibroblastic cells
Discussion
SCHE is a benign vascular tumor. Previously, it was thought that SCHE is a low-grade malignant tumor with a high tendency for local recurrence and minimal potential for distant metastasis. However, further studies prove that it is a benign multifocal process[3] and the present study indicates that it is a reactive vascular proliferation.[4] SCHE has been reported to occur in association with various vascular malformations.[4,5,6]
Often the lesions of SCHE affect children and young adult though any age group can be affected by this tumor.[2] Commonly the tumor affects the distal limbs though the occurrence of SCHE in neck and oral mucosa has also been reported.[7,8] Clinically, SCHE presents as multiple cutaneous or subcutaneous bluish or red nodules, which occasionally may be painful. The natural course of the disease is persisting lesions and appearance of newer lesions along with the passage of time.
Histological character of the tumor is multifocal, totally or partially intravascular, irregularly dilated thin-walled cavernous spaces with thrombi and phleboliths intermixed. Commonly, solid focal area of aggregates of spindle-shaped cells is found in between the cell.[9]
When we first show the case, the differential diagnosis was other vascular tumor like Maffucii syndrome, Gorham's disease, Kaposi's sarcoma, cystic lymphatic malformation, Masson's hemangioendotheliome vegetant intravasculaire and spindle-cell hemangioma.
Maffucii syndrome also occurs in puberty; however, in addition to vascular tumor it also affects bone. In this case, the absence of the bone lesions helped us to exclude this diagnosis. The absence of osteolytic bony lesions and lymphatic malformations exclude the possibility of Gorham's disease also. Blue rubber bleb nevus syndrome usually starts at birth or early childhood, predominantly affecting the trunks and extremities and associated with gastrointestinal bleeding. The profile of our case did not match with blue rubber bleb syndrome in the absence of any gastrointestinal involvement.
What is new?
This patient presented to us after a decade long persistence of painful nodules, which first appeared in chest rather than starting from lower extremity. The patient relied more on traditional medicines than modern medicine and option of cosmetic surgery was unacceptable to him
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Weiss SW, Enzinger FM. Spindle cell hemangioendothelioma: A low-grade angiosarcoma resembling a cavernous hemangioma and Kaposi's sarcoma. Am J Surg Pathol. 1986;10:521–30. [PubMed] [Google Scholar]
- 2.Perkins P, Weiss SW. Spindle cell hemangioendothelioma: An analysis of 78 cases with reassessment of its pathogenesis and biologic behavior. Am J Surg Pathol. 1996;20:1196–204. doi: 10.1097/00000478-199610000-00004. [DOI] [PubMed] [Google Scholar]
- 3.Fletcher CD, Beham A, Schmid C. Spindle cell haemangioendothelioma: A clinicopathological and immunohistochemical study indicative of a non-neoplastic lesion. Histopathology. 1991;18:291–301. doi: 10.1111/j.1365-2559.1991.tb00849.x. [DOI] [PubMed] [Google Scholar]
- 4.Imayama S, Murakamai Y, Hashimoto H, Hori Y. Spindle cell hemangioendothelioma exhibits the ultrastructural features of reactive vascular proliferation rather than angiosarcoma. Am J Clin Pathol. 1992;97:279–87. doi: 10.1093/ajcp/97.2.279. [DOI] [PubMed] [Google Scholar]
- 5.Ding J, Hashimoto H, Imayama S, Tsuneyoshi M, Enjoji M. Spindle cell hemangioendothelioma, probably a benign vascular lesion not a low grade angiosarcoma: A cliniopathological, ultra structural and immunochemical study. Virchows Arch A Pathol Anat Histopathol. 1992;420:77–85. doi: 10.1007/BF01605988. [DOI] [PubMed] [Google Scholar]
- 6.Fanbung JC, Meis Kindblom JM, Rosenberg AE. Multiple enchondromas associated with spindle cell hemangioendotheliomas: An overlook variant Maffucci's syndrome. Am J Surg Pathol. 1995;19:1029–38. doi: 10.1097/00000478-199509000-00006. [DOI] [PubMed] [Google Scholar]
- 7.Sheehan M, Roumpf SO, Summerlin DJ, Billings SD. Spindle cell hemangioma: Report of casepresenting in the oral cavity. J Cutan Pathol. 2007;34:797–800. doi: 10.1111/j.1600-0560.2006.00708.x. [DOI] [PubMed] [Google Scholar]
- 8.Tosion KI, Gouveris I, Sklavounou A, Koutlas IG. Spindle cell hemangioma (hemangioendothelioma) of the hand and neck: Report of unusual (or undiagonosed) tumor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:216–21. doi: 10.1016/j.tripleo.2007.03.005. [DOI] [PubMed] [Google Scholar]
- 9.Calonge E, Edward WJ. Vascular Tumors: Tumors and Tumor like condition s of blood vessels and lymphatics. In: Elder DE, editor. Lever's histopathology of the skin. 9th Ed. Philadelphia: Lippincott Williams and Wilkins; 2005. pp. 1016–53. [Google Scholar]