

Abstract
To demonstrate the feasibility and clinical significance of cervical vestibular-evoked myogenic potential (cVEMP) test in pediatric patients.
Retrospective review study was conducted in a pediatric tertiary care facility. A total of 278 patients were identified with adequate data, including medical notes, results of cVEMP, and imaging studies.
Among the total of 278 pediatric patients, only 3 children were not able to finish the cVEMP test successfully. In about 90% of the cases, the cVEMP test was requested to investigate a patient’s hearing loss and/or vestibular complaints. Over 90% of the cVEMP tests were ordered by specialists such as pediatric otolaryngologists or otologists. Obtained cVEMP results provided useful information in clinical diagnosis and management in all cases.
It is feasible to conduct cVEMP testing in children, including infants, and cVEMP testing can provide valuable information in the diagnosis and management of hearing loss and vestibular impairment. This simple and noninvasive test should be embraced by pediatric professionals.
INTRODUCTION
Since the initial depiction by Colebatch et al about twenty years ago, vestibular-evoked myogenic potential (VEMP) has been investigated by clinicians and researchers worldwide and has become an important part of the comprehensive vestibular evaluation.1–5 Evoked primarily by intense acoustic stimuli such as clicks or tonebursts, VEMP is a short-latency myogenic reflex mediated via otolith organs (the saccule and the utricles) and vestibular nerves. VEMP responses can be recorded from neck muscles, known as cervical VEMP (cVEMP), or extraocular muscles, also known as ocular VEMP (oVEMP).6–9 Extensive research studies have shown that cVEMP test is a useful, noninvasive method for assessment of otolith function and the functional integrity of the vestibular nerve.10–14 Clinically, cVEMP test is relatively easy to perform and well tolerated by patients of all ages. Complementing the traditional vestibular test battery such as caloric and rotational test, cVEMP test has been used in the evaluation of a variety of vestibular disorders, including Meniere’s disease, vestibular schwannoma, and labyrinthitis/vestibular neuritis.5,15–19 Moreover, most of the recent studies have demonstrated cVEMP test to be very sensitive in detecting inner ear structural anomalies such as superior semicircular canal dehiscence (SSCD) and enlarged vestibular aqueduct (EVA).20–24
Although cVEMP has been well studied in animals and human subjects, the majority of clinical research is focused on adults while cVEMP studies in children are relatively insufficient. Early studies of cVEMP testing in children included small numbers of cases and did not draw significant attention. The first cVEMP study that included a larger number of children was reported by Sheykholeslami et al25 in 2005, in which they described their success in conducting cVEMP test in 12 healthy neonates and 12 neonates with various otologic disorders. To demonstrate the feasibility of reliable cVEMP testing in normal children, Kelsch et al26 in 2006 conducted a study of cVEMP test in 30 subjects ages from 3 to 11 years and established their cVEMP normative data, including latencies and amplitudes. In subsequent years, similar cVEMP studies in normal pediatric subjects have provided further evidence in establishing the cVEMP test as a valid technique for evaluation of pediatric vestibular function.27–31 Regarding clinical applications, the cVEMP test for children with known medical conditions are primarily limited to the topics of otitis media, ototoxic effects, congenital hearing loss, and cochlear implants.32–40
In 2006, we started to implement cVEMP test for children at our facility to meet the increasing demand of clinical evaluation for pediatric patients with auditory and vestibular complaints. To demonstrate the clinical value of cVEMP in children and share our experience of this practice, we decided to conduct this retrospective review of cVEMP testing in >200 pediatric cases.
MATERIALS AND METHODS
Our study was approved by the institutional review board at Boston Children’s Hospital.
Patient Selection
After reviewing all available records, we identified a total of 278 pediatric patients who underwent cVEMP testing between July 2006 and July 2012. All selected cases had usable records, including physicians’ visit notes, clinical/working diagnoses, imaging studies, and cVEMP outcomes.
Conducting cVEMP Test and Other Audiologic Evaluations
Prior to cVEMP testing, all patients had a hearing evaluation with air and bone conduction threshold testing. Tympanometry and acoustic reflex thresholds were also obtained if clinically warranted. We used a commercial evoked potential system (NavigatorPro, Natus Medical Inc., San Carlos, CA) to record cVEMP under a customized pediatric protocol. All normative cVEMP parameters, including threshold, amplitude and latencies, were established at our facility. The details of the protocol can be found in our previous publications.24,37 Briefly, acoustic stimuli (500 Hz tonebursts and/or clicks) were presented via insert phones or bone oscillator. All cVEMP was recorded from sternocleidomastoid muscle. Head-turning is required to have sternocleidomastoid muscle contracted and the contraction is monitored to ensure its appropriateness. For younger children, an assistant was employed to attract the patients’ attention, allowing them to make a head turn to toys with colorful lights. To obtain cVEMP thresholds, a stimulus level of 90 dB normal hearing level (nHL) was used as the default starting intensity. The stimulus intensity would decrease in steps of 10 dB or increase in steps of 5 dB depending upon the presence or absence of cVEMP, respectively. The lowest stimulus intensity at which a clear and repeatable wave was observed would be recorded as the cVEMP threshold. Amplitude and latency were measured respective to the cVEMP response to stimuli presented at 90 dB nHL. If no reliable response was found at the maximal stimulation level, the cVEMP would be considered absent. For patients with middle ear pathologies and conductive hearing loss, bone-conducted stimuli were also used to elicit cVEMP if air-conducted stimuli were not sufficient.
Data analysis
We exclusively used descriptive analysis in this study. Age, sex, reasons for cVEMP test, referring physician, and so on were summarized for all patients.
RESULTS
General Information
Among the 278 patients included in this study, there were 119 boys and 159 girls. The average age was 10.5 years (SD = 4.6), with the youngest at the age of 5 months. To better demonstrate patients’ makeup, we classified them into 6 age groups, from the youngest group of “Age 3 & Under” to the oldest group of “Age 16 to 18”, as shown in Figure 1. Notably, there were a significant number of children in each age group, and even in the youngest group there were >20 children although the Age 13 to 15 group had the largest case number at 72 (259% of the total). Similarly, we divided the numbers of cVEMP testing conducted by calendar year, demonstrated in Figure 2. As shown, we have conducted 30 to 50 cVEMP tests in pediatric patients each year, except the beginning year of 2006. Of note, the number of cVEMP performed trended toward to an increase in 2012 since the number in 2006 and 2012 reflected only 6 months of clinical work.
FIGURE 1.
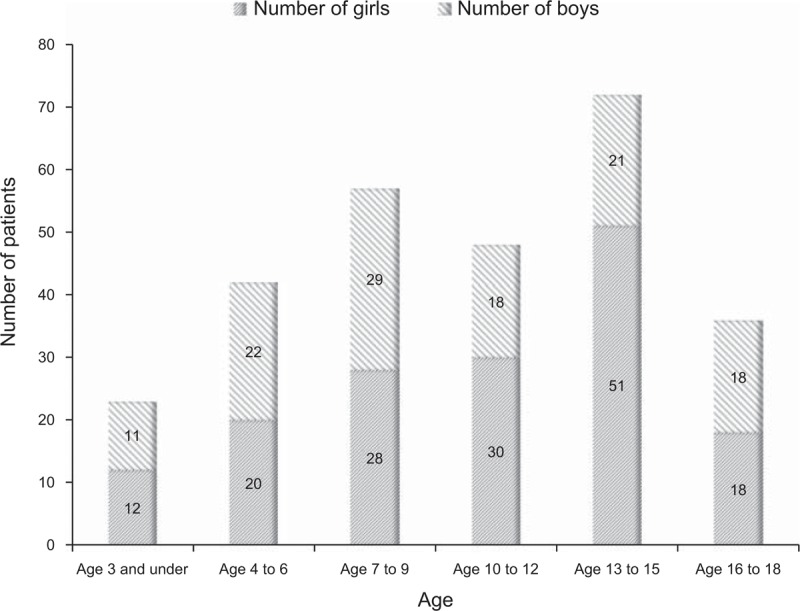
Enumerated data of pediatric VEMP test conducted in 6 age groups.
FIGURE 2.
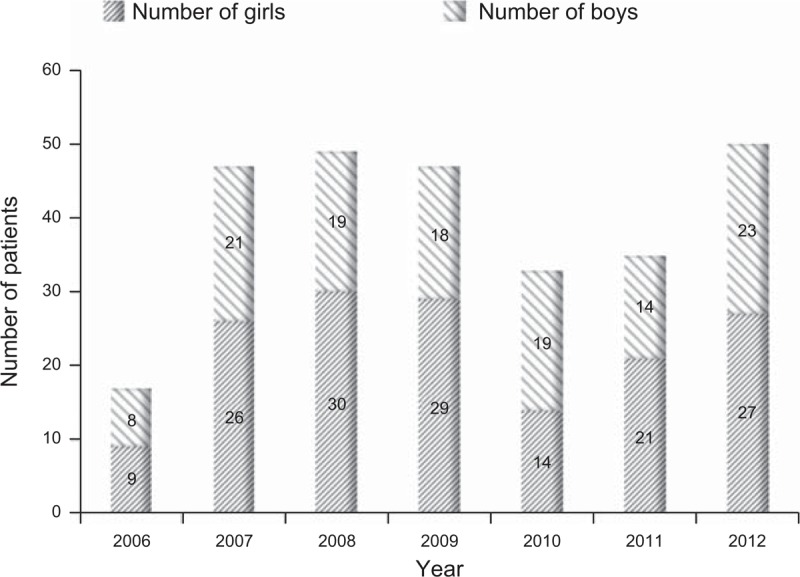
Numbers of pediatric VEMP test conducted in each calendar year at our facility from 2006 to 2012. Of note, the number in 2006 and 2012 reflected only 6 months of clinical work.
VEMP Referrals
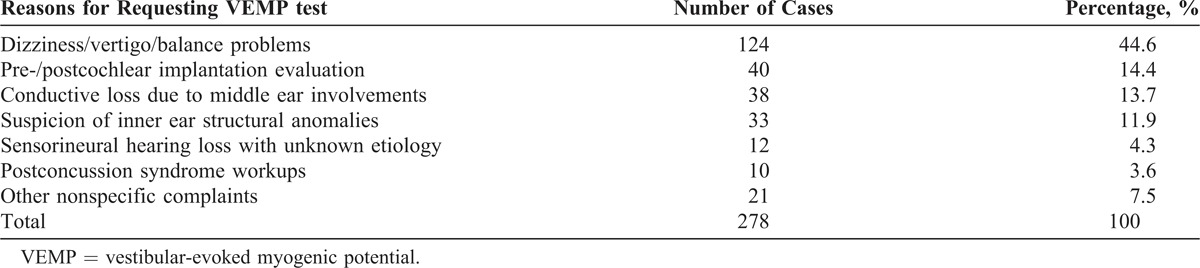
Various reasons for cVEMP testing were documented in patients’ medical records and these were summarized in Table 1. As listed, the main reason for requesting a cVEMP test was to evaluate children’s dizziness, vertigo or balance issues, and accounted for almost 45% of the total requests. The second leading reason for cVEMP testing in our facility was pre- and postcochlear implant workup that accounted for nearly 15%. Investigation of middle ear–related conductive hearing loss and inner ear structural anomalies such as SSCD and EVA by cVEMP testing, accounted for 13.7% and 11.9% respectively. Twelve children with sensorineural hearing loss caused by unknown etiology underwent cVEMP testing because of a concern of possible coexisting vestibulopathy. Ten children with postconcussion syndrome also underwent cVEMP testing as a part of a comprehensive workup. The remaining 21 children, 7.5% of the total, were referred for other nonspecific complaints such as tinnitus or headache.
Table 1.
Summarization of Reasons for Requesting VEMP Testing in Our Study
In addition to tracking the reasons for cVEMP test, we also looked over the referring physicians and their specialties. As shown in Table 2, the overwhelming majority of patients were referred by pediatric otolaryngologists (about 48%) and otologists/neurotologists (45%). Referrals by neurologists and neurosurgeons accounted for only 5%. Fewer than 3% of the referrals originated from other specialists such as audiologists.
Table 2.
Breakdown of Referrals by Specialists for VEMP Testing in Our Study

Outcomes of cVEMP in Pediatric Patients
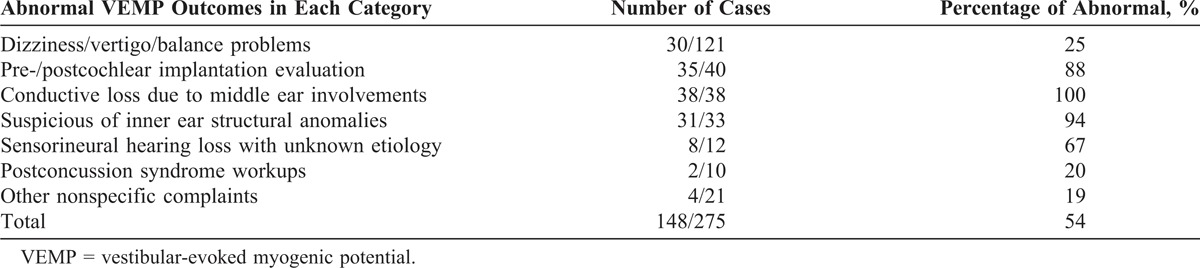
Among the 278 children in this study, only 3 children were not able to complete cVEMP testing, mostly due to fears of recording electrodes and wires, or they were intolerant of insert phones. VEMP results obtained from the remaining 275 children were analyzed. If no repeatable cVEMP responses were present at the highest intensity of the stimuli, we would call the cVEMP absent. If present, the cVEMP threshold would be determined along with the cVEMP latency and amplitude, as described in the method section. Abnormal cVEMP outcomes found in each referring category are summarized in Table 3. As shown, abnormal cVEMP responses were found in all children with conductive hearing loss related to middle ear pathologies, most had absent cVEMP responses to air-conducted stimuli; however, robust cVEMP were present when bone-conducted stimuli were used in these cases. Also, the cVEMP seemed to be very responsive, at 94%, to inner ear structural anomalies such as EVA and SSCD. Typical cVEMP findings related to EVA and SSCD included a lower cVEMP threshold and higher amplitude. In children with cochlear implant(s), abnormal cVEMPs (absent cVEMP, elevated cVEMP thresholds, and reduced amplitude) were found in 35 of 40 cases. Only 25% of children with complaints of dizziness or vertigo had an abnormal cVEMP. Approximately two-thirds of the children with congenital hearing loss had abnormal cVEMP, indicating possible cochlear-vestibulopathy although the exact etiology is unknown. Overall, abnormal cVEMP results were found in 54% of children who completed the test.
Table 3.
Occurrence of Abnormal VEMP Results in 275 Pediatric Patients
DISCUSSION
Our study has revealed a successful experience of carrying out cVEMP testing in pediatric patients, from infants to teenagers, in a busy clinical setting. In fact, cVEMP testing is a noninvasive procedure and is generally well tolerated by children of all ages. Although the literatures on cVEMP testing in children revealed its feasibility, many pediatric professionals have reservations about the clinical value of cVEMP testing, considering most of the published studies were conducted using normal subjects or had a limited number of children.20,29,31,33,41,42 In fact, a recent survey completed by our group presented a dismal picture of the use of cVEMP test in children currently: among the 117 pediatric otolaryngologists who finished our online survey, about 90% believed that cVEMP test cannot be performed in children and more than 80% thought cVEMP testing was unreliable (unpublished data). One encouraging finding from the survey, however, was that the majority of pediatric otolaryngologists have basic knowledge about the test. Consequently, we determined to conduct this current study to demonstrate that cVEMP testing not only is feasible but also has clinical value in evaluating pediatric patients for a variety of clinical scenarios.
We have shown, for the first time, a variety of clinical applications of cVEMP testing in a large group of pediatric patients. The sensitivity of the cVEMP test may vary depending upon the medical conditions present or referring diagnoses. When middle ear pathology associated conductive hearing loss is suspected, our study demonstrated 100% sensitivity of the cVEMP test to confirm such conditions. Specifically, the cVEMP is absent when air-conducted stimuli are used to elicit the cVEMP response. In contrast, cVEMP is usually present if bone-conducted stimuli are used to elicit response, indicating the existence of a sound transmission problem via the middle ear system. Also, cVEMP test has shown to be very sensitive to detect inner ear structural anomalies such as EVA or SSCD, especially when conductive hearing loss or air-bone gaps are exhibited on the audiogram. Although our study showed a relatively low sensitivity of cVEMP test in evaluating children with dizziness, vertigo, or balance problem, and its diagnostic value should not be overlooked. In these circumstances, the cVEMP test can only assess the otolith function without semicircular canal function involved, which is a limitation. Therefore, cVEMP test can be a complimentary procedure to standard rotational and caloric test.
Conducting VEMP test in pediatric patients, especially in young children can be a challenge. Most older children (i.e., age 7 to 18 years, can follow instructions during cVEMP testing and make proper head turns to achieve sufficient muscle contraction. When testing younger children (e.g., age 4 to 6 years), on the other hand, an assistant will be helpful to draw patients’ attention so that valid cVEMP responses can be recorded. For younger children who are unable or unwilling to sit by themselves, sitting in their parents’ lap can be adopted to have a better control of the patients. Light-up toys are effective tools to attract patients’ attention but any noise-making toys should be avoided. It’s also important to allow ample time for younger children to “warm-up” before putting recording electrodes and insert phones on them so that their fear of the testing procedure can be reduced.
CONCLUSION
Based on our clinical experience, cVEMP test can be successfully conducted in pediatric patients. Conducting cVEMP test is not only feasible but also valuable in the clinical evaluation of children with auditory and/or vestibular complaints. Although the sensitivity of cVEMP test may vary depending upon medical conditions, it provides diagnostic information in most cases. This noninvasive and low-cost test procedure can be easily implemented in any audiologic clinic where an evoked potential recording system is available. Most importantly, pediatric professionals should embrace this cutting-edge technology and consider cVEMP testing before ordering more expensive tests such as MRI and CT scans, which usually bring unpleasant experiences to pediatric patients.
Footnotes
Abbreviations: cVEMP = cervical vestibular-evoked myogenic potential, EVA = enlarged vestibular aqueduct, SSCD = superior semicircular canal dehiscence.
The authors have no funding or conflicts of interest to disclose.
REFERENCES
- 1.Colebatch JG, Halmagyi GM, Skuse NF. Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry. 1994; 57:190–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Halmagyi GM, Colebatch JG, Curthoys IS. New tests of vestibular function. Baillieres Clin Neurol. 1994; 3:485–500. [PubMed] [Google Scholar]
- 3.Welgampola MS, Colebatch JG. Characteristics and clinical applications of vestibular-evoked myogenic potentials. Neurology. 2005; 64:1682–1688. [DOI] [PubMed] [Google Scholar]
- 4.Brantberg K, Granath K, Schart N. Age-related changes in vestibular evoked myogenic potentials. Audiol Neurootol. 2007; 12:247–253. [DOI] [PubMed] [Google Scholar]
- 5.Ushio M, Iwasaki S, Murofushi T, et al. The diagnostic value of vestibular-evoked myogenic potential in patients with vestibular schwannoma. Clin Neurophysiol. 2009; 120:1149–1153. [DOI] [PubMed] [Google Scholar]
- 6.Todd NP, Rosengren SM, Aw ST, Colebatch JG. Ocular vestibular evoked myogenic potentials (OVEMPs) produced by air- and bone-conducted sound. Clin Neurophysiol. 2007; 118:381–390. [DOI] [PubMed] [Google Scholar]
- 7.Rosengren SM, Welgampola MS, Colebatch JG. Vestibular evoked myogenic potentials: past, present and future. Clin Neurophysiol. 2010; 121:636–651. [DOI] [PubMed] [Google Scholar]
- 8.Rosengren SM, Govender S, Colebatch JG. Ocular and cervical vestibular evoked myogenic potentials produced by air- and bone-conducted stimuli: comparative properties and effects of age. Clin Neurophysiol. 2011; 122:2282–2289. [DOI] [PubMed] [Google Scholar]
- 9.Lim LJ, Dennis DL, Govender S, Colebatch JG. Differential effects of duration for ocular and cervical vestibular evoked myogenic potentials evoked by air- and bone-conducted stimuli. Exp Brain Res. 2013; 224:437–445. [DOI] [PubMed] [Google Scholar]
- 10.Murofushi T, Halmagyi GM, Yavor RA, Colebatch JG. Absent vestibular evoked myogenic potentials in vestibular neurolabyrinthitis. An indicator of inferior vestibular nerve involvement? Arch Otolaryngol Head Neck Surg. 1996; 122:845–848. [DOI] [PubMed] [Google Scholar]
- 11.Colebatch JG, Halmagyi GM. Vestibular evoked myogenic potentials in humans. Acta Otolaryngol. 2000; 120:112. [DOI] [PubMed] [Google Scholar]
- 12.Sheykholeslami K, Murofushi T, Kermany MH, Kaga K. Bone-conducted evoked myogenic potentials from the sternocleidomastoid muscle. Acta Otolaryngol. 2000; 120:731–734. [DOI] [PubMed] [Google Scholar]
- 13.Gonzalez-Garcia E, Piqueras-Del Rey A, Martin-Alba V, et al. The vestibulocollic reflex: assessment and characteristics of vestibular-evoked myogenic potentials analysed by age groups. Rev Neurol. 2007; 44:339–342. [PubMed] [Google Scholar]
- 14.Colebatch JG. Vestibular evoked myogenic potentials in multiple sclerosis. Clin Neurophysiol. 2012; 123:1693–1694. [DOI] [PubMed] [Google Scholar]
- 15.Chang CH, Young YH. Caloric and vestibular evoked myogenic potential tests in evaluating children with benign paroxysmal vertigo. Int J Pediatr Otorhinolaryngol. 2007; 71:495–499. [DOI] [PubMed] [Google Scholar]
- 16.Egami N, Ushio M, Yamasoba T, Murofushi T, Iwasaki S. Indication of the side of delayed endolymphatic hydrops by vestibular evoked myogenic potential and caloric test. ORL J Otorhinolaryngol Relat Spec. 2010; 72:242–246. [DOI] [PubMed] [Google Scholar]
- 17.Lin KY, Hsu YS, Young YH. Brainstem lesion in benign paroxysmal vertigo children: evaluated by a combined ocular and cervical vestibular-evoked myogenic potential test. Int J Pediatr Otorhinolaryngol. 2010; 74:523–527. [DOI] [PubMed] [Google Scholar]
- 18.Timmer FC, Zhou G, Guinan JJ, Kujawa SG, Herrmann BS, Rauch SD. Vestibular evoked myogenic potential (VEMP) in patients with Meniere’s disease with drop attacks. Laryngoscope. 2006; 116:776–779. [DOI] [PubMed] [Google Scholar]
- 19.Lin MY, Timmer FC, Oriel BS, et al. Vestibular evoked myogenic potentials (VEMP) can detect asymptomatic saccular hydrops. Laryngoscope. 2006; 116:987–992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sheykholeslami K, Schmerber S, Habiby Kermany M, Kaga K. Vestibular-evoked myogenic potentials in three patients with large vestibular aqueduct. Hear Res. 2004; 190:161–168. [DOI] [PubMed] [Google Scholar]
- 21.Zhou G, Gopen Q. Characteristics of vestibular evoked myogenic potentials in children with enlarged vestibular aqueduct. Laryngoscope. 2011; 121:220–225. [DOI] [PubMed] [Google Scholar]
- 22.Wu Z, Zhang S, Zhou N, et al. Significance of some otologic function tests in diagnosis of Meniere’s disease. Lin Chuang Er Bi Yan Hou Ke Za Zhi. 2006; 20:433–435. [PubMed] [Google Scholar]
- 23.Rosengren SM, Aw ST, Halmagyi GM, Todd NP, Colebatch JG. Ocular vestibular evoked myogenic potentials in superior canal dehiscence. J Neurol Neurosurg Psychiatry. 2008; 79:559–568. [DOI] [PubMed] [Google Scholar]
- 24.Zhou G, Gopen Q, Poe DS. Clinical and diagnostic characterization of canal dehiscence syndrome: a great otologic mimicker. Otol Neurotol. 2007; 28:920–926. [PubMed] [Google Scholar]
- 25.Sheykholeslami K, Megerian CA, Arnold JE, Kaga K. Vestibular-evoked myogenic potentials in infancy and early childhood. Laryngoscope. 2005; 115:1440–1444. [DOI] [PubMed] [Google Scholar]
- 26.Kelsch TA, Schaefer LA, Esquivel CR. Vestibular evoked myogenic potentials in young children: test parameters and normative data. Laryngoscope. 2006; 116:895–900. [DOI] [PubMed] [Google Scholar]
- 27.Chen CN, Wang SJ, Wang CT, Hsieh WS, Young YH. Vestibular evoked myogenic potentials in newborns. Audiol Neurootol. 2007; 12:59–63. [DOI] [PubMed] [Google Scholar]
- 28.Picciotti PM, Fiorita A, Di Nardo W, Calo L, Scarano E, Paludetti G. Vestibular evoked myogenic potentials in children. Int J Pediatr Otorhinolaryngol. 2007; 71:29–33. [DOI] [PubMed] [Google Scholar]
- 29.Erbek S, Erbek SS, Gokmen Z, Ozkiraz S, Tarcan A, Ozluoglu LN. Clinical application of vestibular evoked myogenic potentials in healthy newborns. Int J Pediatr Otorhinolaryngol. 2007; 71:1181–1185. [DOI] [PubMed] [Google Scholar]
- 30.Young YH, Chen CN, Hsieh WS, Wang SJ. Development of vestibular evoked myogenic potentials in early life. Eur J Paediatr Neurol. 2009; 13:235–239. [DOI] [PubMed] [Google Scholar]
- 31.Wang SJ, Hsieh WS, Young YH. Development of ocular vestibular-evoked myogenic potentials in small children. Laryngoscope. 2013; 123:512–517. [DOI] [PubMed] [Google Scholar]
- 32.Jin Y, Nakamura M, Shinjo Y, Kaga K. Vestibular-evoked myogenic potentials in cochlear implant children. Acta Otolaryngol. 2006; 126:164–169. [DOI] [PubMed] [Google Scholar]
- 33.Monobe H, Murofushi T. Vestibular neuritis in a child with otitis media with effusion; clinical application of vestibular evoked myogenic potential by bone-conducted sound. Int J Pediatr Otorhinolaryngol. 2004; 68:1455–1458. [DOI] [PubMed] [Google Scholar]
- 34.Zagolski O. Vestibular tests in infants after treatment with aminoglycosides. Pol Merkur Lekarski. 2005; 19:638–641. [PubMed] [Google Scholar]
- 35.Wang J, Shi L, Gao L, Xie J, Han L. Audiological characteristics of unilateral auditory neuropathy: 11 case study. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2007; 21:436–440. [PubMed] [Google Scholar]
- 36.Cushing SL, Papsin BC, Rutka JA, James AL, Blaser SL, Gordon KA. Vestibular end-organ and balance deficits after meningitis and cochlear implantation in children correlate poorly with functional outcome. Otol Neurotol. 2009; 30:488–495. [DOI] [PubMed] [Google Scholar]
- 37.Licameli G, Zhou G, Kenna MA. Disturbance of vestibular function attributable to cochlear implantation in children. Laryngoscope. 2009; 119:740–745. [DOI] [PubMed] [Google Scholar]
- 38.Zagolski O. Vestibular-evoked myogenic potentials and caloric tests in infants with congenital rubella. B-ENT. 2009; 5:7–12. [PubMed] [Google Scholar]
- 39.De Kegel A, Maes L, Baetens T, Dhooge I, Van Waelvelde H. The influence of a vestibular dysfunction on the motor development of hearing-impaired children. Laryngoscope. 2012; 122:2837–2843. [DOI] [PubMed] [Google Scholar]
- 40.Shinjo Y, Jin Y, Kaga K. Assessment of vestibular function of infants and children with congenital and acquired deafness using the ice-water caloric test, rotational chair test and vestibular-evoked myogenic potential recording. Acta Otolaryngol. 2007; 127:736–747. [DOI] [PubMed] [Google Scholar]
- 41.Wang SJ, Chen CN, Hsieh WS, Young YH. Development of vestibular evoked myogenic potentials in preterm neonates. Audiol Neurootol. 2008; 13:145–152. [DOI] [PubMed] [Google Scholar]
- 42.Valente M. Maturational effects of the vestibular system: a study of rotary chair, computerized dynamic posturography, and vestibular evoked myogenic potentials with children. J Am Acad Audiol. 2007; 18:461–481. [DOI] [PubMed] [Google Scholar]