

Abstract
Placebo control is a useful method for determining the efficacy of a therapy. In acupuncture researches, the preferred method for placebo control is acupuncture using a placebo needle that has a blunt tip and achieves no skin penetration.
We performed a crossover study to validate the blinding effect of a new type of placebo needle. Sixty volunteers were randomized to receive acupuncture using 2 types of needles with different sequences: sequence AB, involving first the pragmatic placebo needle and then the real needle, and sequence BA, in a reverse order. Placebo acupuncture was performed by administering the placebo needle through an adhesive pad without skin penetration on the acupoints LI4, RN12, BL25, and BL36. Real acupuncture was performed by needling through the pad and penetrating the skin to 15 mm using a real needle on the same acupoints. The acupuncture was administered every other day with 3 sessions for 1 type of needle. The primary outcome was the perception of needle penetration. Besides degree of acupuncture pain, type, and degree of needle sensation, needle acceptability and factors influencing the subject blinding effect were assessed.
Needle penetration was felt by 100%, 90% (54/60), 88.3% (53/60), and 95% (57/60) of volunteers receiving placebo acupuncture and 98.3% (59/60), 96.7% (58/60), 95% (57/60), and 95% (57/60) of volunteers receiving real acupuncture on LI4, RN12, BL25, and BL36, respectively. Differences of the volunteers’ perception of needle penetration between the placebo needle and real needle were not significant for the 4 acupoints (all P > 0.05). Volunteers experienced fewer distension sensations (P = 0.01), a lower degree of needle sensation (P = 0.007), and less pain (P = 0.006) during placebo acupuncture than during real acupuncture. The placebo needle was more easily accepted than the real needle (OR = 1.63, 95% CI, 1.01–2.64). The influences of age, sex, educational level, acupuncture experience, needle sensation, acupuncture pain, and needle acceptability on volunteers’ perception of needle penetration were not significant.
The pragmatic placebo needle is a valid control for acupuncture research. It produces a good subject blinding effect with a similar appearance to conventional acupuncture needles and no skin penetration when applied.
INTRODUCTION
Placebo control is a crucial tool to identify whether the effect of an intervention is truly because of its specific elements, rather than the placebo effect. This tool can minimize the subjective expectation and bias of both subjects and researchers and assist in the implementation of blinding. To explore the specific effects of acupuncture, a suitable placebo control is required.
To date, many efforts have been made toward developing acupuncture placebo controls. There appears to be a consensus that a good acupuncture placebo control should satisfy 2 points: the appearance of the placebo needles cannot be differentiated from the real needle and the placebo acupuncture has the least curative effects. In general, the placebo controls commonly used in acupuncture studies can be divided into 2 categories according to whether the needle penetrates the skin or not: sham acupuncture and placebo acupuncture, respectively.
Sham acupuncture, also called superficial acupuncture or minimal acupuncture, is a type of control involving needles penetrating the skin. Compared with real acupuncture, sham acupuncture needles are applied either on acupoints with a shallower depth or to nonacupoints with a similar or shallower depth.1 As a slight stimulus of gentle touch can activate C tactile afferents and thus play a role in pain inhibition,2 a stronger stimulus, such as skin penetration, results in greater neurological responses related to the treatment effect. Thus, it is difficult for sham acupuncture to be as inert as desired. The effect of sham acupuncture has been proven to be comparable with real acupuncture and standard drug therapy, superior to drug placebo in several studies of migraine treatment,3–5 based on a reanalysis of a systematic review.6 Therefore, it is questionable whether sham acupuncture is an effective control.7,8
Placebo acupuncture is a type of control without skin penetration based on the application of placebo needles with blunt needle tips.1 The skin penetration of acupuncture needle is one of the key points inducing effect, treatment effect, or placebo effect. There were no researches comparing the extent of treatment effect between the placebo and the sham acupuncture and no proof that the placebo needle induced no treatment effect. Nonetheless, by removing the skin penetration of needle, less treatment effect is inferred to be induced in placebo acupuncture than in sham acupuncture. Thus, the placebo needle has become a new hotspot in acupuncture control research. Currently, there are 3 types of placebo needles that have been the most validated in acupuncture studies: Streitberger placebo needles,9 Park sham devices,10 and double-blind placebo acupuncture needles.11 The common characteristics of these placebo needles are blunt needle tips, a retractable needle handle, and a fixed device that can be pasted on the skin. When used in practice, the bodies of these placebo needles can retract into their needle handles, providing an illusion that the needles are inserted into the skin. This allows the placebo needles to appear identical to their matched real needles, which aids in achieving successful blinding. However, the composition and manipulation of these placebo needles are more complicated than conventional acupuncture needles. These dissimilarities may induce subjects familiar with conventional acupuncture needles to believe the acupuncture they received is not real acupuncture, regardless of whether what they actually received is placebo acupuncture or real acupuncture. Thus, it is slightly difficult when using these placebo needles to successfully achieve blinding of subjects familiar with conventional needles. For subjects without acupuncture experience, a good blinding effect was observed when using both Streitberger placebo needles9 and Park sham devices,10 but 60% of subjects who have a good knowledge of acupuncture can differentiate a Park sham needle from its matched real needle.12 In China, the public displays a high level of awareness of acupuncture, which can be observed with the changes in the number of outpatients in the acupuncture and moxibustion departments in Chinese hospitals. An investigation revealed that the maximum number of outpatients was not >48,000 in 1997 but increased to 300,000 in 2007.13 Compared with the western public, the Chinese public tends to display a better understanding of acupuncture but a poorer understanding of voluntarily entering clinical trials. The large differences in the appearance between placebo needles and conventional acupuncture needles may affect the compliance of subjects, and it is imaginable that the application of the above placebo needles may face a more severe difficulty in China. Overall, these reasons indicate the necessity of the development of a better placebo control method for acupuncture research.
The purpose of this study was to validate the blinding effect of a new type of placebo needle. This placebo needle was designed to blind subjects only with the help of the blunt needle tips and a simple adhesive pad (for fixation). Without complicated fixation devices and retractable needle handles, the device is more pragmatic and closer to conventional acupuncture needles in appearance. We hypothesized that this pragmatic placebo needle would be effective for blinding subjects, that is, subjects would not be able to distinguish between placebo and real acupuncture based on the perception of needle penetration.
METHODS
This was a randomized, controlled, single blind, crossover study. This study was approved by the hospital's ethics committee (ethics approval number, 2013EC089-01) and conducted in accordance with the provisions of the Declaration of Helsinki. This study was registered on ClinicalTrials.gov (identifier, NCT01948375).
Participants
This study was performed between August 2013 and December 2013 at Guang’anmen Hospital of China Academy of Chinese Medical Sciences, Beijing, China. Volunteers were recruited via poster advertisements. Volunteers who were aged between 18 and 74 years and had basic Chinese language proficiency were enrolled in the study. Volunteers were excluded from the study if they met any of the following criteria: acute or chronic pain; taking analgesics or drugs inducing abnormal sensation; diseases causing sensory disturbance or sensory loss; alcohol or drug abuse history; serious cardiovascular, cerebral, hepatic, renal, hematopoietic, hemorrhagic or psychiatric diseases; diabetes mellitus or dermatological disease; women who were pregnant or lactating; and had cardiac pacemaker, metal allergy, or severe needle phobia. Eligible volunteers were informed of the potential risks of acupuncture and they provided written informed consent.
Randomization and Masking
Eligible patients were randomized equally to receive acupuncture with 2 types of needles with different sequences: sequence AB, involving first the pragmatic placebo needle and then the real needle and sequence BA, involving first the real needle and then the placebo needle. The random allocation was performed using predictive analytics software (PASW) Statistics 20 (International Business Machines Corporation, Beijing, China) and implemented by an acupuncturist. A postgraduate student was responsible for information collection and outcome assessment, and a statistician from the Clinical Evaluation Center of China Academy of Chinese Medical Sciences was responsible for statistical analysis. In this study, the subjects, outcome assessor (postgraduate student), and statistician were blinded to intervention allocation.
Pragmatic Placebo Needle
The pragmatic placebo needle is 0.30 mm in diameter and 25 mm in length. It consists of an adhesive pad and placebo needle with a blunt tip (Figure 1). The adhesive pad is made of a sterile cylindrical polyethylene foam (diameter 10 mm and height 5 mm) with a double-sided adhesive tape at the bottom. The adhesive pad has 2 functions: one is fixation of the placebo needle on the acupoints when used in placebo acupuncture and the other function is assisting the implementation of blinding when used in both placebo and real acupuncture. The real needle used in this study was not especially designed to match the placebo needle and is a commonly used conventional acupuncture needle.
FIGURE 1.
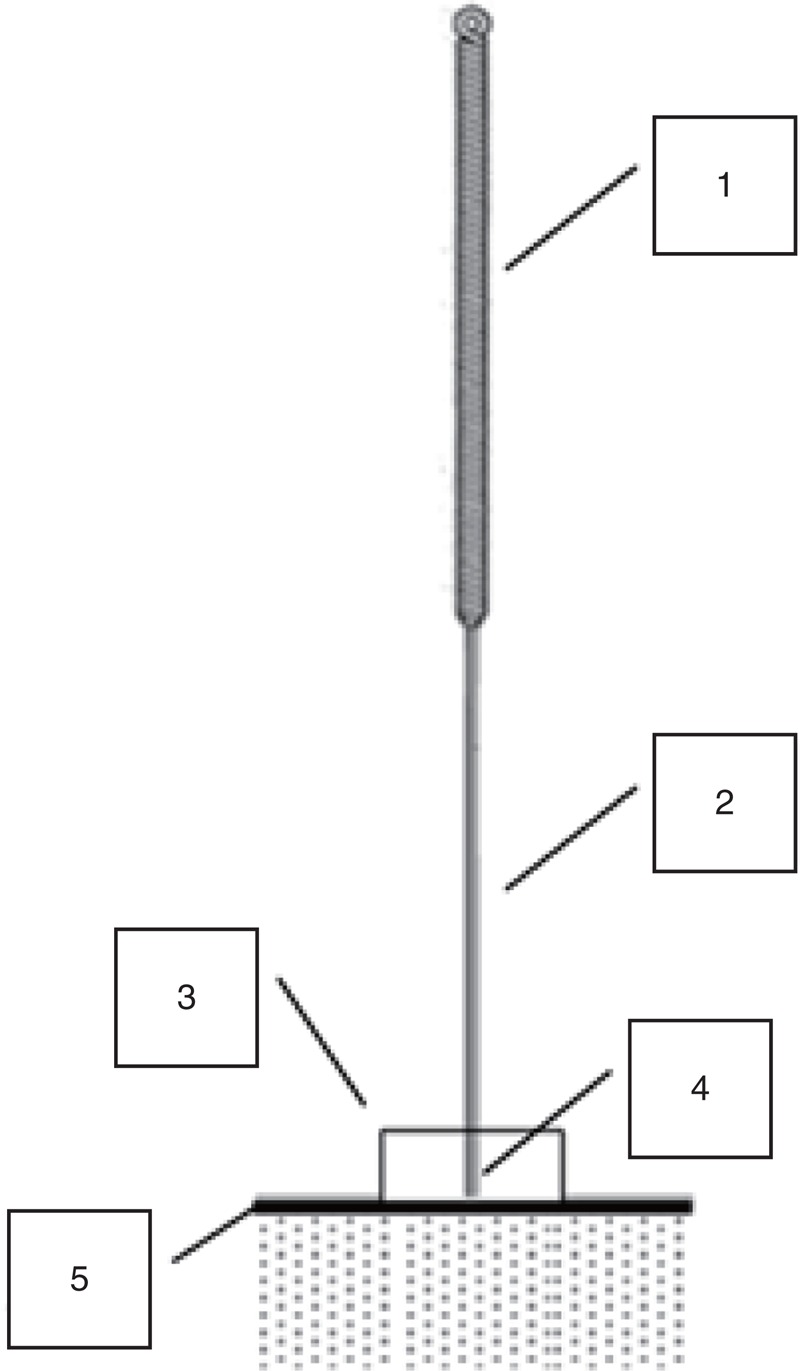
Pragmatic placebo needle: 1, needle handle; 2, needle body; 3, adhesive pad; 4, blunt tip; 5, cutis.
Interventions
Before acupuncture intervention, volunteers were asked to finish a questionnaire on acupuncture knowledge under the guidance of the postgraduate student. There were 4 parts in the questionnaire: demographic profile (information on sex, age, and educational level), acupuncture experience (mainly including the number of acupuncture sessions, nervousness toward acupuncture, and discomfort with acupuncture), acupuncture knowledge (mainly including understanding the needle sensation and type of needle sensation experienced), and acupuncture acceptability (acceptability of acupuncture and intention to seek further acupuncture treatment).
Acupuncture Interventions
Volunteers were told that we were testing a new type of needle to determine whether there were differences in the perception of needle penetration, degree of acupuncture pain, and type and degree of needle sensation as compared with the conventional acupuncture needle type. An experienced licensed acupuncturist was trained on the usage of the placebo needle and applied both the placebo and real acupuncture throughout the whole study. To explore the influence of different acupoints on the blinding effect of the pragmatic placebo needle, 4 points were selected after consideration of their location parts, sensitivity, and visibility: Hegu (LI4), located in a distal limb, sensitive with a strong needle sensation of sourness, numbness and distension, and visible; Chengfu (BL36), located in a proximal limb, insensitive, and invisible; Zhongwan (RN12), located in the abdomen, sensitive with a strong needle sensation of distension, and invisible; and Dachangshu (BL25), located in the waist, insensitive, and invisible. Volunteers received acupuncture with either the pragmatic placebo needle (A) or real needle (B) according to the randomized sequence AB or BA. In each acupuncture application, an adhesive pad was first pasted onto the chosen acupoint. All acupoints were needled through the pad but just pressed against the skin without penetration when using the pragmatic placebo needle (0.30 mm diameter, 25 mm length, Hwato brand; Suzhou Medical Appliance Factory, Suzhou, China), whereas when the real needle (0.30 mm diameter, 40 mm length, Hwato brand, Suzhou Medical Appliance Factory) was used, the acupoints were needled through the pad and 15 mm into the skin. During the acupuncture session, LI4 and RN12 were needled with the volunteers in a supine position for 15 minutes first, and after a 15-minute break, BL36 and BL25 were needled with the volunteers in a prone position for another 15 minutes. Needles were manipulated with even twirling, lifting, and thrusting to elicit deqi or needle sensation (a composite of unique sensations interpreted as the flow of qi induced by acupuncture and essential for clinical efficacy14) 3 times every 5 minutes. After each needle withdrawal, volunteers were asked to meet the independent interviewer in another room to provide their answers to the following 3 questions: do you think the needle penetrates the skin? (yes or no); how was the pain in the acupuncture procedure? (volunteers were asked to give a score using a visual analogue scale [VAS] a numerical scale from 0 to 10, where 0 indicates no pain and 10 indicates the severest pain); what type of needle sensations did you experience during the acupuncture session (as assessed with the Southampton needle sensation questionnaire)? Acupuncture was administered every other day, 3 sessions for each type of needle, a total of 6 sessions for each subject. There was a 2-day interval between the applications of the 2 types of needles.
Outcome Measures
Primary Outcome
Skin penetration is inevitable in acupuncture, and therefore, perception of needle penetration is the key to assessing the placebo needle's blinding effects.
The primary outcome was the difference in the proportion of volunteers’ perception of needle penetration from the placebo and real needles in the third acupuncture session in each period.
Secondary Outcomes
Southampton needle sensation questionnaire: This questionnaire was used to collect the types and degree of needle sensation experienced by volunteers. It was presented with 17 items and had been validated to be capable of accurately recording deqi.15 However, the sensations of soreness and distension frequently reported in acupuncture were not included. In this study, we added the sensations of soreness and distension to the Southampton needle sensation questionnaire, so there were 19 types of total needle sensations. The differences between the 2 types of needles were assessed after the third acupuncture session in each period.
Degree of acupuncture pain: The difference in acupuncture pain between the 2 types of needles was assessed using the VAS value of the third acupuncture session in each period.
Acceptability of needle: After the third acupuncture session in each period, volunteers were asked to indicate their acceptance toward the needle using a 5-point scale: very difficult to accept, a little difficult to accept, acceptable, easy to accept, and very easy to accept. Differences between the 2 types of needles were assessed.
Analysis of factors influencing subject blinding: The success of blinding was defined as the subjects’ perception of needle penetration. The factors influencing subject blinding analyzed mainly involved the demography, needle type, acupuncture experience, needle sensation, acupuncture pain, and needle acceptability data from the third acupuncture session in each period.
Statistical Methods
Sample Size Calculation
In crossover studies, subjects are randomly assigned to a sequence of interventions consisting of 2 or more treatments administered consecutively. Each subject serves as his or her own control. Thus, a crossover design requires fewer subjects than parallel designs. Given that the sample sizes of published crossover studies on placebo needles are all approximately 60 cases, we reasoned that 60 volunteers is an adequate number to obtain a good estimate of the difference of the perception of needle penetration between the placebo needle and the real needle, and we performed no formal sample size calculation.
Statistical Analysis
PASW Statistics 20 (International Business Machines Corporation) was used for data analysis. The primary analysis population was defined as the randomized population who had results for at least 1 period. In our study, all the randomized volunteers finished the trial. Continuous variables were summarized as the mean (standard deviation [SD]). The categorical variables were summarized as case and percentages. The level of significance was established at α < 0.05 with a 2-tailed test. The main objective was to compare the proportion of volunteers’ perception of needle penetration between the placebo and real needles. The null hypothesis was that the differences in the proportion of volunteers’ perception of needle penetration would not be significantly different between the 2 types of needles, whereas the alternative hypothesis was that the placebo needle displayed a lower proportion than the real needle.
In crossover studies, an issue arises concerning treatment comparisons when there may be a carryover effect, an effect that “carries over” from one experimental condition to another. For example, in our study, volunteers’ perception of needle penetration in the second period when treated by placebo needles or real needles may be affected by their experiences in the first period. Any carryover effect, positive or negative, can bias the estimate of treatment effect. Thus, a test for carryover effects was first conducted for each variable in this study. If the carryover effect was significant, only period 1 data could be used to estimate the direct effect of the placebo and real needles; if it was not significant, the pooled data from both periods could be used to estimate the direct effect. For continuous data, the carryover effect could be assessed using the within-individual sums of the results from both periods. The differences between direct effects could be assessed using the within-individual differences between the outcomes in both periods. For comparison of 2 independent samples, the t test or analysis of variance of crossover design was used if the error terms conformed to the normal distribution, whereas nonparametric tests were used if the error terms did not conform to a normal distribution. For binary data, the variables were classified into 3 categories: −1, preferred the first period; 0, no preference in both periods; 1, preferred the second period. Prescott test, in which the period effect was adjusted,16,17 was used to compare the direct effect of the 2 needle types, and the Fisher exact or χ2 tests were used for analysis. In addition, a generalized estimating equation (GEE) was used in the analysis of ranked data, and binary logistic regression was used in the analysis of the factors influencing the blinding effect.
RESULTS
Study Group
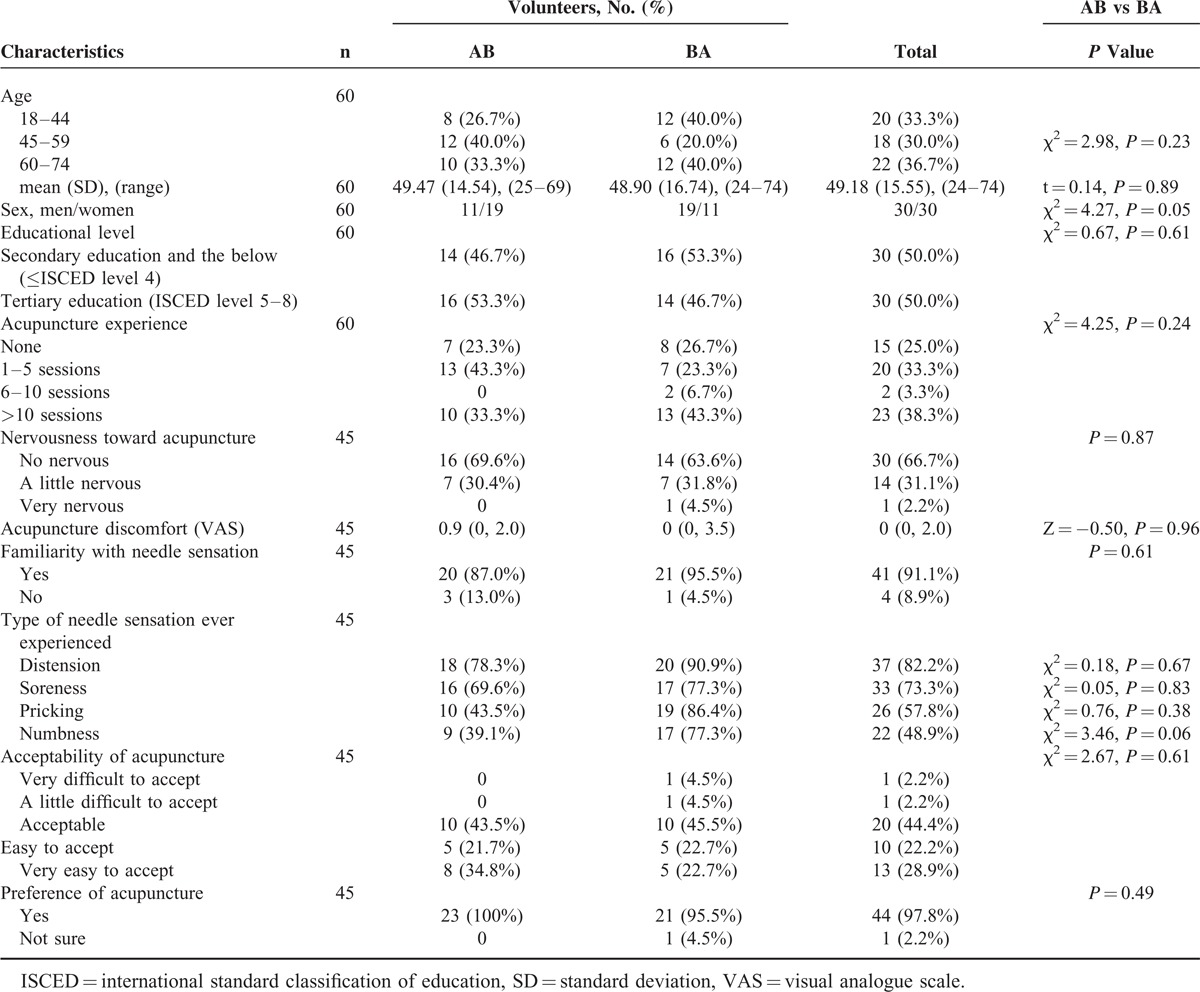
From August 1 to December 30, 2013, 60 randomized volunteers were enrolled into the study. They all completed the study, and no one withdrew (Figure 2). The mean (SD) age of the 60 volunteers was 49.18 (15.55) years. Half were men, and half had received tertiary education. The distribution of age, sex, and educational level did not differ between the 2 groups (Table 1). In the survey on acupuncture knowledge, 15 (25%) volunteers reported no acupuncture experience, 7 in group AB and 8 in group BA; 20 (33.3%) reported past experience with 1 to 5 sessions of acupuncture, 13 in group AB and 7 in group BA; 23 (38.3%) reported past experience with >10 sessions of acupuncture, 10 in group AB and 13 in group BA. Only 2 volunteers in the BA group reported having past experience with 6 to 10 sessions of acupuncture. Overall, there were no significant differences in acupuncture experience between the 2 groups. Of the 45 volunteers with acupuncture experience, 30 (66.7%) reported no nervousness during acupuncture and 14 (31.1%) reported a little nervousness. The median (quartile range) discomfort of acupuncture was 0.9 (0, 2.0) in group AB and 0 (0, 3.5) in group BA, and the differences between the 2 groups were insignificant. A total of 41 (91.1%) of volunteers thought they were familiar with the needle sensations. The types of needle sensations reported by the 45 volunteers with acupuncture experience were ranked from the greatest to the least as follows: distension (37/45), soreness (33/45), pricking (26/45), numbness (22/45), electric shock (18/45), spreading (16/45), throbbing (13/45), warmth (5/45), heaviness (4/45), tingling (3/45), and twinge (2/45). The most reported needle sensations, distension, soreness, pricking, and numbness, did not differ in frequency between the 2 groups. Among the 45 volunteers with acupuncture experience, 43 (95.6%) volunteers reported that acupuncture was acceptable, and 44 (97.8%) volunteers indicated a preference for acupuncture as a treatment option. The distributions of the acceptability and preference of acupuncture in the 2 groups were comparable. The volunteers’ baseline characteristics are summarized in Table 1.
FIGURE 2.
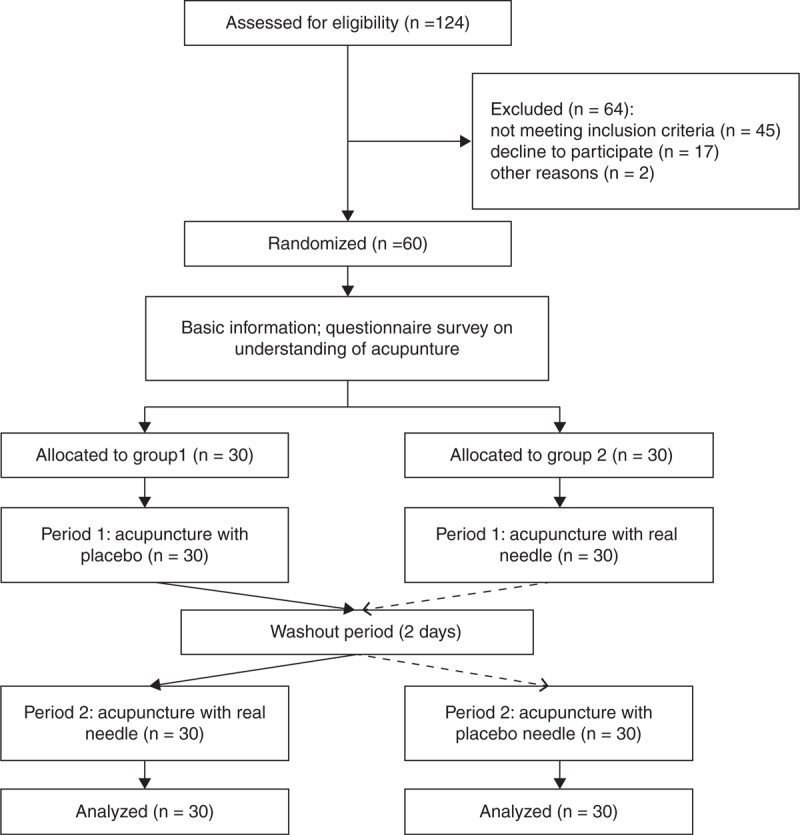
Flow diagram.
TABLE 1.
Baseline Characteristics
Perception of Needle Penetration
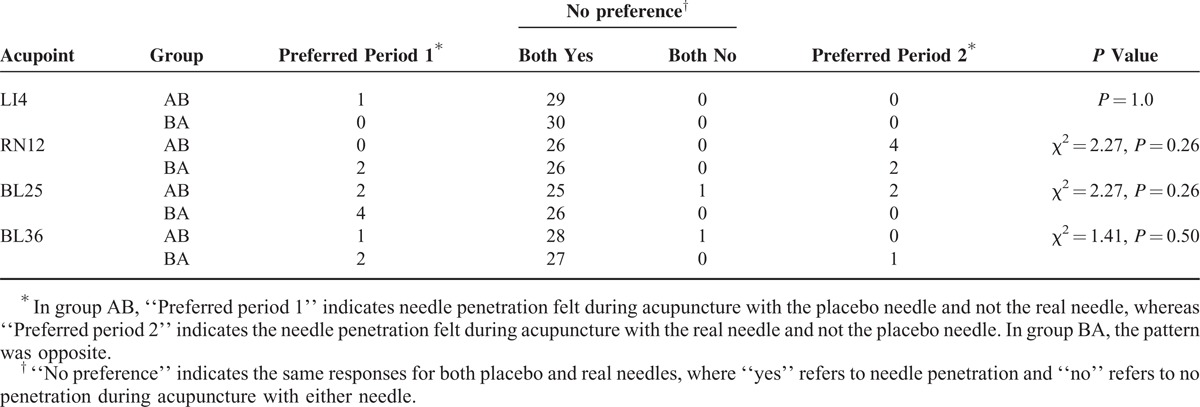
Needle penetration was felt by 60 (100%) volunteers during placebo acupuncture and by 59 (98.3%) of volunteers during real acupuncture when needling LI4. Needle penetration was felt during both placebo and real acupuncture by 59 volunteers, and 1 volunteer felt needle penetration only during placebo acupuncture. During the acupuncture application on the other 3 acupoints, the situation was very similar to that with LI4. Needle penetration was felt by 54 (90.0%), 53 (88.3%), and 57 (95.0%) volunteers during placebo acupuncture application to RN12, BL25, and BL36, respectively, and by 58 (96.7%), 57 (95.0%), and 57 (95.0%) volunteers during real acupuncture application to RN12, BL25, and BL36, respectively. Needle penetration was felt during both placebo and real acupuncture by 52, 51, and 55 volunteers, respectively, during acupuncture application to RN12, BL25, and BL36. Needle penetration was only felt during placebo acupuncture by 2 volunteers at RN12, BL25, and BL36, and during real acupuncture by 6 volunteers at RN12 and BL25 and by 2 volunteers at BL36. The carryover effects of placebo or real needles were not significant for the perception of needle penetration when needling the 4 acupoints LI4, RN12, BL25, and BL36 (all P > 0.05) in the third acupuncture session of each period. There were no significant differences in the perception of needle penetration between the placebo and real acupunctures for LI4 (P > 0.99), RN12 (χ2 = 2.27, P = 0.26), BL25 (χ2 = 2.27, P = 0.26), and BL36 (χ2 = 1.41, P = 0.50). The details are listed in Table 2.
TABLE 2.
Perception of Needle Penetration Between the Placebo and Real Needles
Needle Sensation: Type and Degree
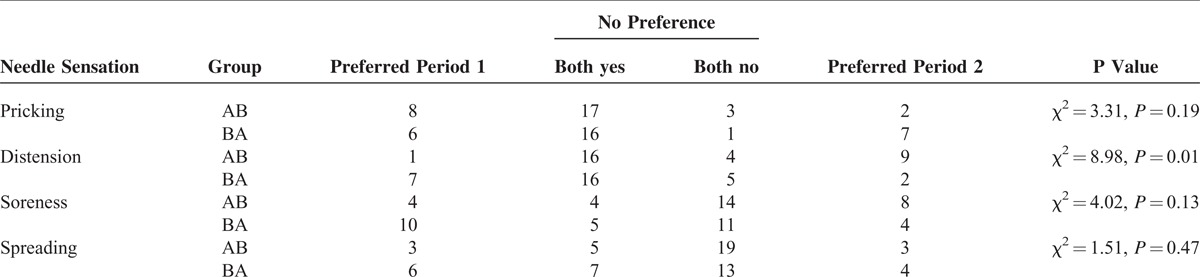
Volunteers experienced almost the same types of needle sensations during placebo and real acupunctures, including pricking, distension, soreness, warmth, sharpness, spreading, tingling, stinging, electric shock, heaviness, numbness, deep ache, throbbing, dull ache, and twinge. Pricking, distension, soreness, and spreading were the most reported needle sensations and reported by 48, 35, 17, and 19 volunteers, respectively, during placebo acupuncture, and by 41, 48, 27, and 21 volunteers, respectively, during real acupuncture. There were no significant differences in the reports of pricking (χ2 = 3.31, P = 0.19), soreness (χ2 = 4.02, P = 0.13), and spreading (χ2 = 1.51, P = 0.47) between the placebo and real acupunctures. However, the sensation of distension displayed a significantly different distribution between the placebo and real acupunctures (χ2 = 8.98, P = 0.01). Volunteers tended to experience more distension sensations during real acupuncture than during placebo acupuncture. Sixteen volunteers reported experiencing more sensation of distension during real acupuncture, whereas only 3 volunteers reported experiencing more sensation of distension during placebo acupuncture. The details are listed in Table 3.
TABLE 3.
Type of Needle Sensation Experienced During Acupuncture With the Placebo and Real Needles
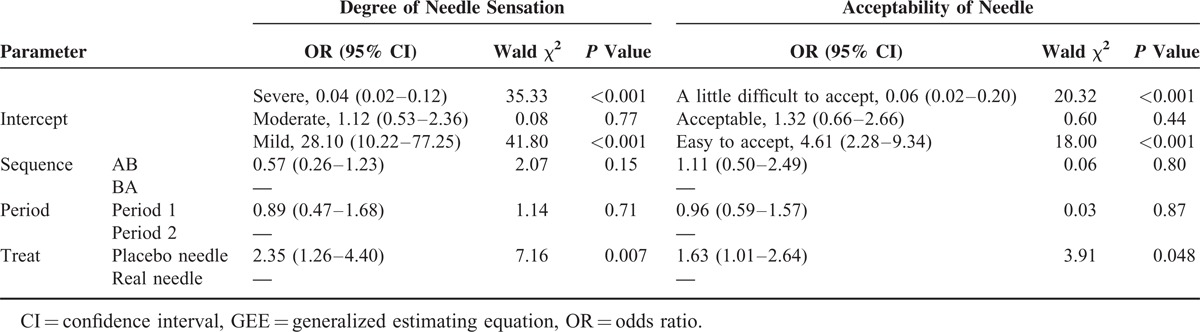
Among the 4 degrees of needle sensation, mild and moderate needle sensations were most reported by volunteers during both placebo and real acupunctures. Mild and moderate degrees of sensation were reported by 51.7% (31/60) and 40% (24/60) of volunteers, respectively, during placebo acupuncture and 38.3% (23/60) and 53.3% (32/60) of volunteers, respectively, during real acupuncture. No sensation was reported by 4 volunteers during placebo acupuncture and 1 volunteer during real acupuncture, whereas a severe sensation was reported by 1 volunteer during placebo acupuncture and 4 volunteers during real acupuncture. The GEE parameter estimate for the degree of needle sensation indicated that there was no significant sequence and period effects (Table 4). The difference between treatments, that is, the placebo and real acupunctures, was significant (P = 0.007). Compared with real acupuncture, the degree of needle sensation induced by placebo acupuncture was slighter (OR = 2.35, 95% CI, 1.26–4.40) (Table 4).
TABLE 4.
GEE Parameter Estimates for Degree of Needle Sensation and Acceptability of Needle
Degree of Acupuncture Pain
The reported acupuncture pain results for the placebo and real needles are shown in Table 5. The mean (SD) of acupuncture pain for the placebo needle was 3.02 (1.87) in group AB and 2.73 (1.41) in group BA, whereas the average acupuncture pain of the real needle was 3.70 (2.22) in group AB and 3.46 (1.98) in group BA. No carryover effect was observed (t = 0.63, P = 0.53). The difference of acupuncture pain between the placebo and needles was significant (t = −2.88, P = 0.006). Volunteers experienced less pain during placebo acupuncture than during real acupuncture. Compared with the real needle, the mean (SD) of acupuncture pain of the placebo needle was decreased by 0.7 (1.88) in the third acupuncture session for each period.
TABLE 5.
Difference of Acupuncture Pain Between the Placebo and Real Needles

Needle Acceptability
No volunteer reported the needle used during their acupuncture session was very difficult to accept. Most of volunteers reported an acceptability of “acceptable” or a higher level (easy to accept or very easy to accept) for both needles, with 59 (98.3%) reported as such for placebo needles and 56 (93.3%) for real needles. In the GEE parameter estimate for needle acceptability, a significant difference was not observed in the sequence or period effect (P = 0.80 and P = 0.87, respectively), but a significant difference was observed for the treatment (P = 0.048) (Table 4). Compared with the real needle, the placebo needle was more easily accepted by the volunteers (OR = 1.63, 95% CI, 1.01–2.64) (Table 4).
Analysis of Factors Influencing Subject Blinding
The success of blinding was defined as subjects’ perception of needle penetration. There were no significant differences in the distributions of subjects’ perception of needle penetration among the 4 acupoints of LI4, RN12, BL25, and BL36 (χ2 = 6.10, P = 0.28). As the most used in the assessment of blinding, the perception of needle penetration at LI4 was selected as representative for the 4 acupoints. Using data from the third acupuncture session in each period, the relation of the blinding effect with age, sex, needle type, educational level, acupuncture experience, type of needle sensation (pricking, distension, soreness, and spreading), degree of needle sensation, acupuncture pain, and needle acceptability was investigated by forward stepwise binary logistic regression. However, none of the above factors were found to be of any significance (P > 0.99).
DISCUSSION
The success of blinding is a fundamental issue in many clinical trials. The validity of a trial may be questioned if this important assumption is violated. As a complex type of intervention, the effect of acupuncture is influenced by various factors such as needle type, specificity of acupoints, needle sensation, method of manipulation, individual difference, and psychological factors.18 To create an effective placebo control for acupuncture, every factor influencing the effect of acupuncture should be well controlled. In this study, using a crossover design, we assessed the blinding effect of a pragmatic placebo needle via several aspects characterizing acupuncture: needle penetration, acupuncture pain, needle sensation, and needle acceptability. We found that the volunteers’ perception of needle penetration in placebo acupuncture presented no significant difference to real acupuncture irrespective of the acupoint used. The placebo needle tended to produce less reported acupuncture pain, a lower degree of needle sensation, and better acceptance.
The perception of needle penetration was considered the most important characteristic for distinguishing the placebo needle from the real needle. Our results indicated that an average of 93.3% (range, 88.3%–100%) of volunteers perceived needle penetration during the placebo acupuncture, and an average of 96.3% (range, 95.0%–98.3%) volunteers perceived needle penetration during the real acupuncture. In this study, significant differences in the volunteers’ perception of needle penetration between the placebo and real acupunctures at either acupoint was not observed, which agrees with previous studies using nonpenetration placebo acupuncture, including a similar placebo needle19 and other retractable placebo needles.20 These findings indicate that the pragmatic placebo needle achieved good subject blinding. The proportion of volunteers perceiving needle penetration of the 2 needles was slightly higher in our study than a study examining Streitberger placebo needles9 (78.3% for placebo needle, 90% for real needle) and another study examining a similar type of placebo needle19 (88% for placebo needle, 79.2% for real needle). We deduced that these results were closely related to the appearance of a placebo needle and study factor that the volunteers were informed about acupuncture. In our study, the placebo needle displayed a similar appearance as the conventional needle except for the blunt tip. Blinding was implemented via the aid of a simple adhesive pad. Moreover, the conventional needle was used as a real needle. Thus, the placebo acupuncture of our study was similar to conventional acupuncture, which made the volunteers more likely to believe they had received real acupuncture. In addition, we told the volunteers that we were testing a new type of needle to determine whether there were differences in the perception of needle penetration, degree of acupuncture pain, type, and degree of needle sensation between the new needle and the conventional acupuncture needle instead of telling them that one type of needle penetrated into the skin and the other type of needle was just placed against the skin without skin penetration. Under these conditions, volunteers could report whether they felt the needle penetrated the skin based on what they actually felt during the acupuncture procedure, which thus avoided the possible bias induced by knowing no skin penetration was occurring with one type of needle. Unlike the previous studies testing placebo needle blinding for a single acupoint, it was worth mentioning that acupoints used in this study were purposely chosen to represent the characteristics of acupoints, that is, location parts, sensitivity, and visibility. There were no significant differences in needle penetration between the placebo and real needles for acupoints of LI4, RN12, BL25, and BL36, which implies that the application of the pragmatic placebo needle as a control for real acupuncture is universally feasible for acupoints.
Needle sensation is always assessed in studies verifying the blinding effect of placebo needle; however, no additional details were presented. In this study, we assessed the types and degrees of the sensations in acupuncture with the placebo and real needles. The results of our study revealed that the most frequent sensations induced by 2 needles were pricking, distension, soreness, and spreading, among which only the sensation of distension displayed a significant difference between the 2 needle types. Compared with the placebo needle, the real needle induced more distending sensations and a higher needle-sensation degree.
Pain during acupuncture is inevitable in clinical practice as real acupuncture is a type of invasive therapy. In our study, the acupuncture pain induced by the placebo needle was 0.70 (1.88) lower than that induced by the real needle. Though the difference of acupuncture pain between the 2 types of needles was significant, its clinical significance is doubtful. The results of previous studies have indicated that the differences between real and placebo needles were too small to reveal the placebo acupuncture to subjects.9 It appears that acupuncture pain was not a negative clue in terms of subject blinding.
A high acceptability was observed in our study, with an acceptability of 98.3% (59/60) for the placebo needle and 93.3% (56/60) for the real needle. These findings are most likely related to the extensive recognition of acupuncture in China. In a survey of feelings of acupuncture acceptability, 81.1% (750/925) of subjects reported easy acceptance of acupuncture.21 It has been reported that subjects who experience less acupuncture pain display a better acupuncture acceptance.21 Thus, it is understandable that a higher acceptability was observed for the placebo acupuncture than the real acupuncture.
No factors were found to significantly influence subject blinding effect in our study. It has been reported that patients with a higher belief in the effect of the treatment preferentially believe they receive real acupuncture, irrespective of age, sex, acupuncture experience, treatment effect, etc.20 Our results agree with that conclusion. We found that age, sex, educational level, needle type, acupuncture experience, needle sensation, acupuncture pain, and needle acceptability did not contribute to the success of subject blinding.
Overall, the pragmatic placebo needle demonstrated a good subject blinding effect in our study. Several advantages of the pragmatic placebo needles need to be addressed when comparing them with retractable placebo needles. First, because it lacks a complicated composition, the pragmatic placebo needle was closer to the conventional acupuncture needle in appearance. Second, the flexible application of conventional acupuncture needles as real needles avoided a potential problem that may exist in acupuncture research using retractable placebo needles: needle-depth limitations of matched real needles. Generally speaking, most acupoints should be needled to a depth of 0.5–1.2 cun (approximately 10–30 mm), and some acupoints should be needled deeply to 2–3 cun (approximately 50–75 mm). However, the maximum needle depth of the matched real needle of the retractable placebo needles do not exceed 30 mm for Streitberger placebo needles,9 15 mm for Park sham devices,10 and 10 mm for double-blind placebo acupuncture needles.22 Therefore, the real acupuncture procedure may not be properly executed because of the limited needle depth. With the help of an adhesive pad, the flexible use of a conventional acupuncture needle not only assists with the implementation of blinding but also overcomes the needle depth limitation. Using a pragmatic placebo needle as control, we can select a conventional acupuncture needle with a proper specification, that is, select a needle with the same diameter and a length which is approximately equal to the sum of the needed needle depth and 25 mm (the height of pragmatic placebo needle), respectively. Third, pragmatic placebo needles are more economical than retractable placebo needles. The price of the conventional acupuncture needle is approximately $0.02/needle, and the pragmatic placebo needle is approximately $0.05/needle, whereas Streitberger placebo needle is approximately $6.3/needle, and Park sham device costs approximately $2.9/needle.1 Taking economic load into consideration, the pragmatic placebo needle is easier to use in clinical trials with large sample sizes.
There were limitations in our study. The study population of our study focused on Chinese population, which implied a better awareness of acupuncture than other populations. This very specific population might be questioned on the external validity and generalizability of results to other populations. Subjects’ knowledge and experience of acupuncture were potential factors that influence the reliability of placebo needling.12 So, it was imaginable that the application of placebo needles might face a more severe difficulty in Chinese population than in other populations. In other words, a placebo needle that passed the validation in the Chinese population might have a high probability of showing a similar generalizability to other populations. A formal sample size calculation was not performed in our study. Therefore, it was not clear how high the chance was to detect differences between the needles and whether finding no statistical difference was a mere result of lack of power. To make up this flaw, a post hoc power analysis was performed on the primary outcome, the difference in the proportion of volunteers’ perceiving needle penetration between the placebo needle and the real needle, to determine whether the sample size used was adequate to support our findings. In our study, an average of 93% and 96% of subjects (the average value of the 4 acupoints) perceived needle penetration in the placebo acupuncture and real acupuncture, respectively. According to the formula of power calculation for difference in proportions of 2 independent groups with equal numbers,23 a sample size of 60 subjects/group ensured a 95% power to fail to detect 15% differences at α level of 0.05. Therefore, a total sample size of 60 subjects was adequate for a crossover design. The findings of nonsignificance of our results should not be interpreted as a lack of power. The blinding effect of the pragmatic placebo needle was preliminarily assessed without using a blinding index providing a comprehensive evaluation of the blindness of clinical trials24 and not in the context of disease. Because of the crossover design, our sample size may not be large enough to explore the influencing factors of blinding. A validation of the pragmatic placebo needle using a blinding index and a study exploring the factors influencing blinding would be useful in future research.
CONCLUSIONS
The findings of the present study suggest that the pragmatic placebo needles display a good subject blinding effect, have a similar appearance to conventional acupuncture needles, and result in no skin penetration during application. The examined placebo needle is a valid control for acupuncture research.
Footnotes
Abbreviation: GEE = generalized estimating equation.
ZL and BL designed this study and revised the paper. HX drafted the manuscript. RM performed the acupuncture. QM performed the data collection and outcome assessment. SY performed the statistical analysis. All the authors read and approved the final paper.
This study was supported by the National Key Technology R&D Program during the Twelfth Five-year Plan Period of China (NO. 2012BAI24B01).
The authors have no funding and conflicts of interest to disclose.
REFERENCES
- 1.Zhu D, Gao Y, Chang J, et al. Placebo acupuncture devices: considerations for acupuncture research. Evid Based Complement Alternat Med 2013; 2013:628907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Olausson H, Wessberg J, Morrison I, et al. The neurophysiology of unmyelinated tactile afferents. Neurosci Biobehav Rev 2010; 34:185–191. [DOI] [PubMed] [Google Scholar]
- 3.van der Kuy PH, Lohman JJ. A quantification of the placebo response in migraine prophylaxis. Cephalalgia 2002; 22:265–270. [DOI] [PubMed] [Google Scholar]
- 4.Linde K, Streng A, Jurgens S, et al. Acupuncture for patients with migraine: a randomized controlled trial. JAMA 2005; 293:2118–2125. [DOI] [PubMed] [Google Scholar]
- 5.Diener HC, Kronfeld K, Boewing G, et al. Efficacy of acupuncture for the prophylaxis of migraine: a multicentre randomised controlled clinical trial. Lancet Neurol 2006; 5:310–316. [DOI] [PubMed] [Google Scholar]
- 6.Linde K, Niemann K, Meissner K. Are sham acupuncture interventions more effective than (other) placebos? A re-analysis of data from the Cochrane review on placebo effects. Forsch Komplementmed 2010; 17:259–264. [DOI] [PubMed] [Google Scholar]
- 7.Lund I, Lundeberg T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct Med 2006; 24:13–15. [DOI] [PubMed] [Google Scholar]
- 8.Lundeberg T, Lund I, Sing A, et al. Is placebo acupuncture what it is intended to be? Evid Based Complement Alternat Med 2011; 2011:932407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet 1998; 352:364–365. [DOI] [PubMed] [Google Scholar]
- 10.Park J, White A, Stevinson C, et al. Validating a new non-penetrating sham acupuncture device: two randomised controlled trials. Acupunct Med 2002; 20:168–174. [DOI] [PubMed] [Google Scholar]
- 11.Takakura N, Takayama M, Kawase A, et al. Tapping-in method (skin penetration technique) with a placebo needle for double-blind acupuncture trials. J Altern Complement Med 2013; 19:308–312. [DOI] [PubMed] [Google Scholar]
- 12.Tsukayama H, Yamashita H, Kimura T, et al. Factors that influence the applicability of sham needle in acupuncture trials: two randomized, single-blind, crossover trials with acupuncture-experienced subjects. Clin J Pain 2006; 22:346–349. [DOI] [PubMed] [Google Scholar]
- 13.Liu W, Qi S, Cheng P, et al. Preliminary investigation on clinical status of acupuncture in China. Chin J InfTCM 2008; 15:1–3. [Google Scholar]
- 14.Hui KK, Nixon EE, Vangel MG, et al. Characterization of the “deqi” response in acupuncture. BMC Complement Altern Med 2007; 7:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.White P, Bishop F, Hardy H, et al. Southampton needle sensation questionnaire: development and validation of a measure to gauge acupuncture needle sensation. J Altern Complement Med 2008; 14:373–379. [DOI] [PubMed] [Google Scholar]
- 16.III JFR. AB/BA crossover trials—binary outcome. J Modern Appl Stat Met 2006; 5:452–457. [Google Scholar]
- 17.Skakun EN, Kling S. A comparison of several score cutting procedures and their effects on success rates. Annu Conf Res Med Educ 1980; 19:9–14. [PubMed] [Google Scholar]
- 18.Shi GX, Yang XM, Liu CZ, et al. Factors contributing to therapeutic effects evaluated in acupuncture clinical trials. Trials 2012; 13:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Goddard G, Shen Y, Steele B, et al. A controlled trial of placebo versus real acupuncture. J Pain 2005; 6:237–242. [DOI] [PubMed] [Google Scholar]
- 20.Enblom A, Johnsson A, Hammar M, et al. The nonpenetrating telescopic sham needle may blind patients with different characteristics and experiences when treated by several therapists. Evid Based Complement Alternat Med 2011; 2011:185034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu B, Xu H, Guo S, et al. Prevalence and correlates of discomfort and acceptability of acupuncture among outpatients in Chinese acupuncture and moxibustion departments: a cross-sectional study. Evid Based Complement Alternat Med 2013; 2013:715480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Takakura N, Takayama M, Kawase A, et al. Double blinding with a new placebo needle: a further validation study. Acupunct Med 2010; 28:144–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sahai H, Khurshid A. Formulae and tables for the determination of sample sizes and power in clinical trials for testing differences in proportions for the two-sample design: a review. Stat Med 1996; 15:1–21. [DOI] [PubMed] [Google Scholar]
- 24.Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials 2004; 25:143–156. [DOI] [PubMed] [Google Scholar]