

Abstract
Hepatocellular carcinoma (HCC) patients with tumor thrombus extended through the major hepatic veins and inferior vena cava into the right atrium (RA) are rare, and most cases are considered as the advanced stage with a poor prognosis.
We report a case of HCC with a tumor thrombus extending into the RA and a tumor thrombus in the portal vein. A literature search for case reports was performed on PubMed.
Compared with the published literature, our case is one of the youngest patients, but with the most advanced HCC that invades both the hepatic inflow and outflow vasculature. For this patient, we resected the tumor thrombus in the RA with the use of cardiopulmonary bypass, and then removed the tumor thrombus in the portal vein and ligated the left branch of portal vein. Because of insufficient remnant liver volume, microwave ablation and transcatheter arterial chemoembolization were performed to control the growth of HCC. The patient survived 6 months after surgery.
This case suggests that for patients with extension of HCC into the RA and portal vein, surgery is a useful therapeutic modality, even in case that liver tumor cannot be resected.
INTRODUCTION
Hepatocellular carcinoma (HCC) is the fifth common malignancy and the second leading cause of cancer-related mortalities in the world.1 It is high aggressive so that tumor thrombus formation in the major vasculature such as portal vein or hepatic vein is frequent in advanced stages.2 In some situation, tumor thrombus can grow from any of 3 main hepatic veins through inferior vena cava (IVC) into the right atrium (RA), which usually has a worse prognosis than that of the patients with tumor thrombus in portal or hepatic vein.3–5 We report a case of HCC with a tumor thrombus extending into the RA and a tumor thrombus in the portal vein, which is rare to see. Besides, compared with the published literature (Table 1), our case is one of the youngest patients with the most advanced HCC that invades both the hepatic inflow and outflow vasculature.
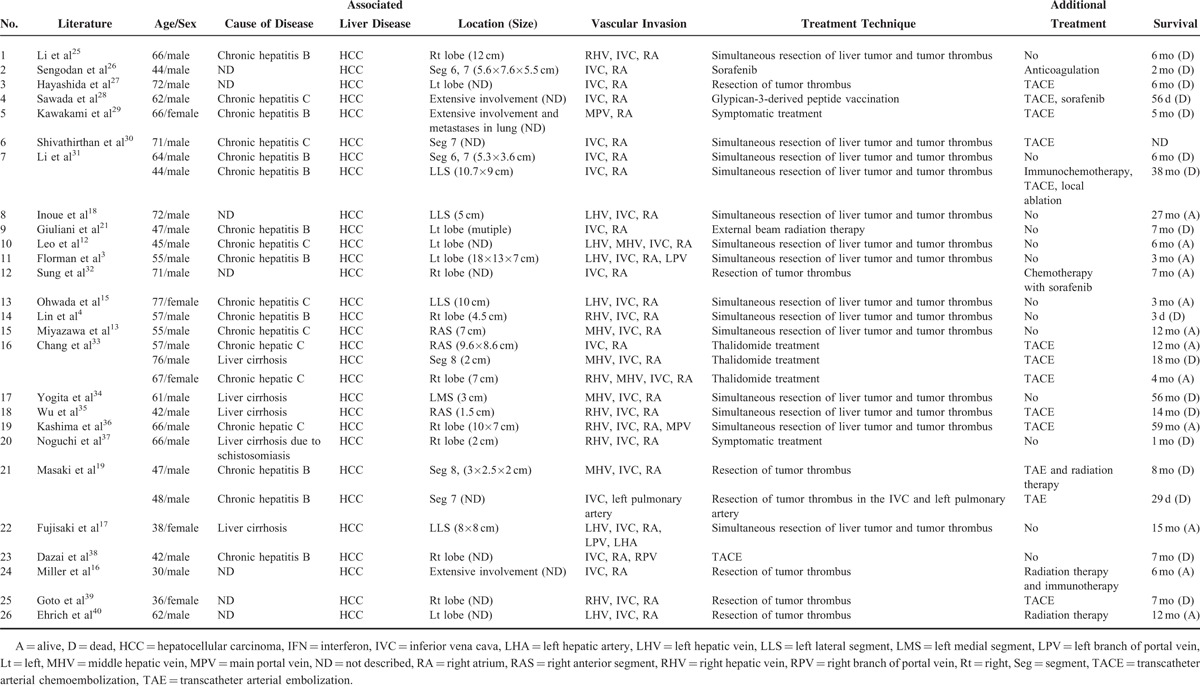
TABLE 1.
Reported Cases of Hepatocellular Carcinoma and Tumor Thrombus in the Right Atrium
CASE REPORT
A 35-year-old man, who is a hepatitis B virus (HBV) carrier, was diagnosed with primary HCC and was thus admitted to our hospital. He claimed abdominal distension. Physical examination was normal. No family or genetic history was found. He had not accepted any therapy before admission. Preoperative computed tomography (CT) revealed multiple carcinoma in the left and right anterior lobe of the liver, with an accompanying tumor thrombus growing from the left hepatic vein through IVC into the RA. It also showed accompanying tumor thrombus in the left branch of the portal vein (Figure 1). Magnetic resonance images showed similar findings with the tumor thrombus severely occupying the RA. Preoperative biochemical examinations revealed alpha-fetoprotein: 3424.53 ng/mL, HBV-DNA 7.09 × 103 copies/mL and Child-Pugh A grade. At the time of admission, the patient had no symptoms of right heat failure or pumonary embolization. However, it may inevitably cause sudden death, as once either of these happens. Therefore, we performed surgery for this patient. A median sternotomy was added to a subcostal arch incision. The patient was placed on cardiopulmonary bypass. A blood removal tube was inserted from the right heart auricle to the superior vena cava. A blood sending tube was inserted to the aorta. The other blood removal tube was inserted to the intrahepatic IVC, and the cardiopulmonary bypass was started. An incision was made from the RA and the IVC to the left hepatic venous root site, and the tumor thrombus was extracted. The RA and the IVC were sutured for closure. The cardiopulmonary bypass was stopped, and the blood removal and sending tubes were removed. Further resection of liver tumor was not possible because of insufficient remnant liver volume that coincided with preoperative analysis. Thus, after resection of tumor thrombus in the portal vein and ligation of the left branch of portal vein, microwave ablation was performed for the liver tumor. Histologic examination of tumor thrombus was consistent with HCC (Figure 2).
FIGURE 1.
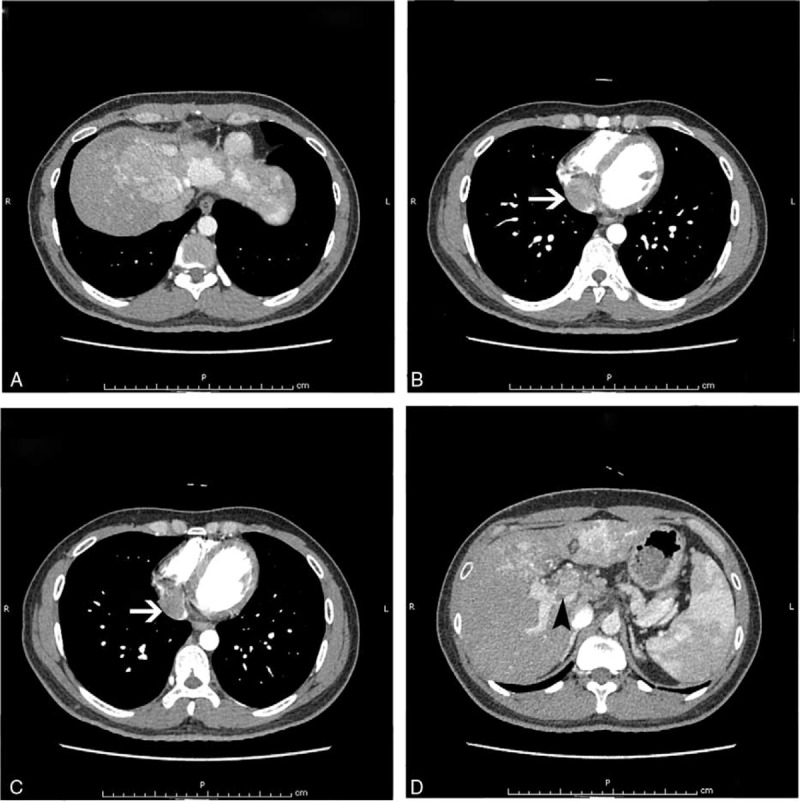
Preoperative CT scanning. (A) Enhanced CT of the abdominal region showed multiple carcinoma in the left and right anterior lobe of the liver. (B, C) Enhanced CT of the chest showed an accompanying tumor thrombus growing into the right atrium (white arrows). (D) Enhanced CT of the abdominal region showed tumor thrombus in the left branch of the portal vein (black arrowhead). CT = computed tomography.
FIGURE 2.
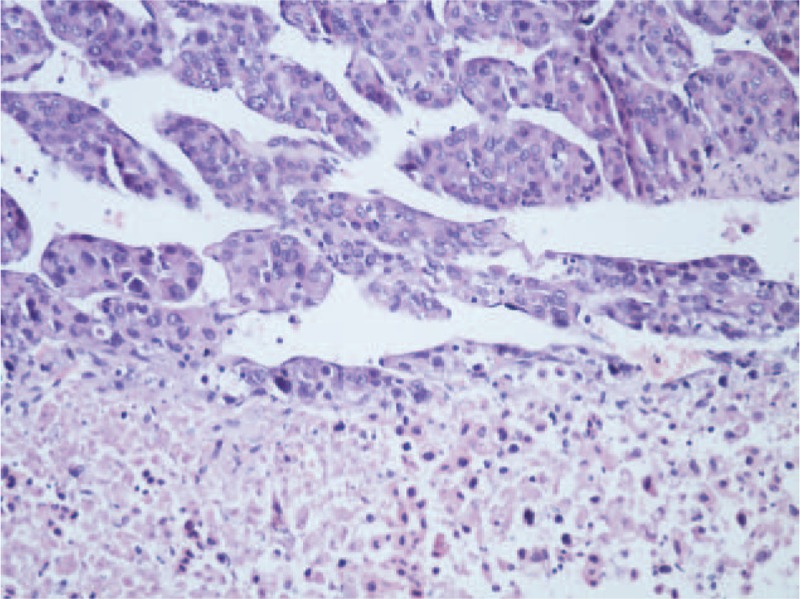
Hematoxylin-eosin staining of the tumor thrombus revealed tumor cells consistent with the patient's HCC (200×). HCC = hepatocellular carcinoma.
The postoperative course was uneventful except for pleural effusion and ascites. On the 14th postoperative day the patient was recovered and discharged. Transcatheter arterial chemoembolization (TACE) was performed to control the growth of tumor mass at 7 weeks after surgery, when the patient's situation allowed this therapy. A month later, CT showed that HCC has expanded to the right posterior lobe of the liver with recurrence of tumor thrombus in the portal vein (Figure 3). Percutaneous microwave ablation was performed. After this treatment, the patient's liver function never recovered to normal, so only symptomatic treatment was performed. At 6 months after the surgery, the patient died with respiratory and circulatory failure induced by hepatic failure.
FIGURE 3.
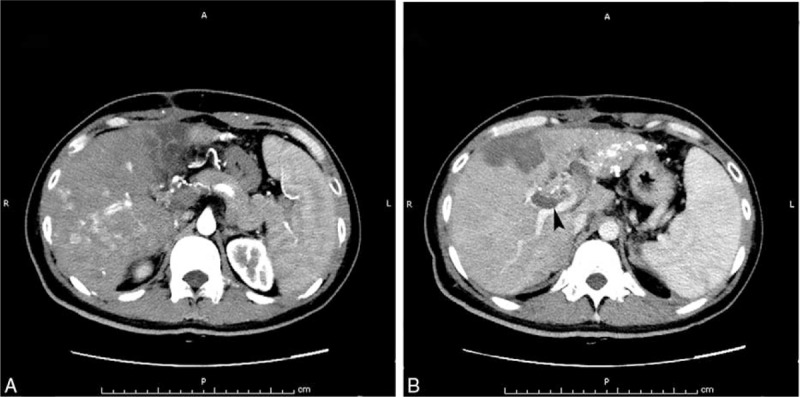
Postoperative examination. (A) Enhanced CT of the abdominal region showed HCC in the right posterior lobe of the liver. (B) Enhanced CT of the abdominal region showed tumor thrombus in the right branch of the portal vein (black arrowhead). CT = computed tomography.
DISSCUSSION
HCC patients with tumor thrombus extending through the major hepatic veins and IVC into the RA are rare, which was reported in 0.67% to 4.1% of autopsies,6,7 and most cases are considered as the advanced stage with a poor prognosis. In our case, the patient is very young, but the tumor thrombus invaded the left branch of portal vein accompanying another tumor thrombus growing from the heptic veins and ICV to the RA. This was an infrequent occurrence and had a dismal prognosis because it carried an increased risk of systemic metastasis and a threat of impending death because of pulmonary embolism or acute heart failure.4,8,9 Hepatic resection with removal of the tumor thrombus was regarded as the most effective therapy.10–15 However, in our case, the patient was an HBV carrier and had severe cirrhotic liver. Preoprerative CT showed multiple carcinoma masses in the left and right anterior lobe of the liver, and the remnant liver volume was not sufficient to tolerate hepatectomy. On the contrary, as the growth of tumor thrombus, heart failure, and pulmonary embolism would be inevitable, it could result in sudden death. Thus, even if the tumor is unresectable, it is necessary to remove the tumor thrombus, which would be beneficial for the patient.
As for the prognosis, we reviewed the published English literature and found that in the 1980s postoperative survival was reported to be 1 to 9 months (mean, 6 months), if only the tumor thrombus was extracted.16 Recently, with the progress of surgical techniques, more and more successful surgical cases for the simultaneous resection of a main liver tumor and tumor thrombus in the RA have been reported.17,18 Miyazawa et al13 had reported that the postoperative survival period of patients whose main tumor of HCC and tumor thrombus in the right atrium could not be extracted without the use of cardiopulmonary bypass ranged from 18 days to 56 months. The mean survival was 20 months. In a retrospective cohort study, Wang et al10 showed that in the treatment of HCC extending into the IVC/RA, hepatectomy and thrombectomy group had a median survival of 19 months, TACE group had a median survival of 4.5 months, and symptomatic treatment had a median survival of 5 months. These data indicated that surgery, either removing thrombus combined with hepatectomy or only tumor thrombus extraction, might result in better survival when compared with other nonsurgical therapies. Our case was consistent with the survival of patients treated by only tumor thrombus extraction.
To further improve the prognosis, postoperative multidisciplinary treatment is important,19 although currently there is no consensus on the modality. The patient in our case was treated by TACE and microwave ablation after the operation to control the growth of the tumor. Being afraid of the side effect, the patient did not accept sorafenib, which was shown to improve the overall survival in patients with advanced HCC.20 In some cases, radiation therapy21,22 and chemotherapy23,24 were also reported to be the promising modality for advanced HCC as one of the multimodel treatment.
In conclusion, for patients with extension of HCC into the RA and portal vein, surgery is a useful therapeutic modality, even in case that liver tumor cannot be resected. The subsequent course will be determined by whether growth of the residual tumor can be controlled by successive multidisciplinary treatments.19
Footnotes
Abbreviations: CT = computed tomography, HBV = hepatitis B virus, HCC = hepatocellular carcinoma, IVC = inferior vena cava, RA = right atrium, TACE = transcatheter arterial chemoembolization.
XL and BZ contributed equally to this article.
Ethical and conflict statement: This article was approved by the Ethics Committee for Clinical Pharmacology in Tongji Medical College. Because our case report does not refer to the patient's privacy, informed consent is not necessary.
The authors have no funding and conflicts of interest to disclose.
REFERENCES
- 1.Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61:69–90. [DOI] [PubMed] [Google Scholar]
- 2.Okuda K. Hepatocellular carcinoma: clinicopathological aspects. J Gastroenterol Hepatol 1997; 12:S314–318. [DOI] [PubMed] [Google Scholar]
- 3.Florman S, Weaver M, Primeaux P, et al. Aggressive resection of hepatocellular carcinoma with right atrial involvement. Am Surg 2009; 75:1104–1108. [PubMed] [Google Scholar]
- 4.Lin HH, Hsieh CB, Chu HC, et al. Acute pulmonary embolism as the first manifestation of hepatocellular carcinoma complicated with tumor thrombi in the inferior vena cava: surgery or not? Dig Dis Sci 2007; 52:1554–1557. [DOI] [PubMed] [Google Scholar]
- 5.Le Treut YP, Hardwigsen J, Ananian P, et al. Resection of hepatocellular carcinoma with tumor thrombus in the major vasculature. A European case-control series. J Gastrointest Surg 2006; 10:855–862. [DOI] [PubMed] [Google Scholar]
- 6.Kojiro M, Nakahara H, Sugihara S, et al. Hepatocellular carcinoma with intra-atrial tumor growth. A clinicopathologic study of 18 autopsy cases. Arch Pathol Lab Med 1984; 108:989–992. [PubMed] [Google Scholar]
- 7.Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer 1954; 7:462–503. [DOI] [PubMed] [Google Scholar]
- 8.Papp E, Keszthelyi Z, Kalmar NK, et al. Pulmonary embolization as primary manifestation of hepatocellular carcinoma with intracardiac penetration: a case report. World J Gastroenterol 2005; 11:2357–2359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Saynak M, Ozen A, Kocak Z, et al. Sudden death: a case report of hepatocellular carcinoma with tumor thrombus extending into the right atrium. J BUON 2007; 12:556. [PubMed] [Google Scholar]
- 10.Wang Y, Yuan L, Ge RL, et al. Survival benefit of surgical treatment for hepatocellular carcinoma with inferior vena cava/right atrium tumor thrombus: results of a retrospective cohort study. Ann Surg Oncol 2013; 20:914–922. [DOI] [PubMed] [Google Scholar]
- 11.Fukuda S, Okuda K, Imamura M, et al. Surgical resection combined with chemotherapy for advanced hepatocellular carcinoma with tumor thrombus: report of 19 cases. Surgery 2002; 131:300–310. [DOI] [PubMed] [Google Scholar]
- 12.Leo F, Rapisarda F, Stefano PL, et al. Cavo-atrial thrombectomy combined with left hemi-hepatectomy for vascular invasion from hepatocellular carcinoma on diseased liver under hypothermic cardio-circulatory arrest. Interact Cardiovasc Thorac Surg 2010; 10:473–475. [DOI] [PubMed] [Google Scholar]
- 13.Miyazawa M, Torii T, Asano H, et al. Does a surgery for hepatocellular carcinoma with tumor thrombus highly occupying in the right atrium have significance? A case report and review of the literature. Hepatogastroenterology 2005; 52:212–216. [PubMed] [Google Scholar]
- 14.Uemura M, Sasaki Y, Yamada T, et al. Surgery for hepatocellular carcinoma with tumor thrombus extending into the right atrium: report of a successful resection without the use of cardiopulmonary bypass. Hepatogastroenterology 2004; 51:1259–1262. [PubMed] [Google Scholar]
- 15.Ohwada S, Takahashi T, Tsutsumi H, et al. Hepatocellular carcinoma with a tumour thrombus extending to the tricuspid valve: report of a successful en bloc resection. Hepatogastroenterology 2008; 55:903–906. [PubMed] [Google Scholar]
- 16.Miller DL, Katz NM, Pallas RS. Hepatoma presenting as a right atrial mass. Am Heart J 1987; 114:906–908. [DOI] [PubMed] [Google Scholar]
- 17.Fujisaki M, Kurihara E, Kikuchi K, et al. Hepatocellular carcinoma with tumor thrombus extending into the right atrium: report of a successful resection with the use of cardiopulmonary bypass. Surgery 1991; 109:214–219. [PubMed] [Google Scholar]
- 18.Inoue Y, Hayashi M, Katsumata T, et al. Hepatocellular carcinoma with right atrial tumor thrombus: report of a case. Surg Today 2011; 41:1122–1129. [DOI] [PubMed] [Google Scholar]
- 19.Masaki N, Hayashi S, Maruyama T, et al. Marked clinical improvement in patients with hepatocellular carcinoma by surgical removal of extended tumor mass in right atrium and pulmonary arteries. Cancer Chemother Pharmacol 1994; 33 suppl:S7–S11. [DOI] [PubMed] [Google Scholar]
- 20.Peng S, Zhao Y, Xu F, et al. An updated meta-analysis of randomized controlled trials assessing the effect of sorafenib in advanced hepatocellular carcinoma. PLoS One 2014; 9:e112530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Giuliani ME, Knox J, Dawson LA. Malignant intracardiac thrombus from hepatocellular carcinoma treated with external beam radiation therapy. J Palliat Med 2010; 13:1293–1295. [DOI] [PubMed] [Google Scholar]
- 22.Hasuike Y, Fukuchi N, Hayashi N, et al. Effectiveness of radiation therapy to the venous thrombosis between the inferior vena cava and right ventricle. Gan To Kagaku Ryoho 2006; 33:1804–1806. [PubMed] [Google Scholar]
- 23.Murakami M, Nagano H, Noda T, et al. A case of hepatocellular carcinoma with right atrium tumor thrombus treated with combined doxorubicin and interferon-beta/intra-arterial injection chemotherapy and hepatectomy. Gan To Kagaku Ryoho 2007; 34:2087–2089. [PubMed] [Google Scholar]
- 24.Monden K, Kobayashi S, Wada H, et al. A case of successful second look operation for hepatocellular carcinoma with right atrial tumor thrombus. Gan To Kagaku Ryoho 2011; 38:2472–2474. [PubMed] [Google Scholar]
- 25.Li AJ, Yuan H, Yin L, et al. Cavoatrial thrombectomy in hepatocellular carcinoma with tumor thrombus in the vena cava and atrium without the use of cardiopulmonary bypass. Ann Vasc Surg 2014; 28:1565.e1565–1565.e1568. [DOI] [PubMed] [Google Scholar]
- 26.Sengodan P, Grewal H, Gandhi S. Invasive hepatocellular carcinoma with recurrent pulmonary embolism: use of AngioVac cannula thrombectomy device for mechanical aspiration. J Invasive Cardiol 2014; 26:E100–E103. [PubMed] [Google Scholar]
- 27.Hayashida K, Okumura S, Kawase T. Right atrial obstruction due to cardiac extension of hepatocellular carcinoma. Asian Cardiovasc Thorac Ann 2014; 22:465–468. [DOI] [PubMed] [Google Scholar]
- 28.Sawada Y, Yoshikawa T, Fujii S, et al. Remarkable tumor lysis in a hepatocellular carcinoma patient immediately following glypican-3-derived peptide vaccination: an autopsy case. Hum Vaccin Immunother 2013; 9:1228–1233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kawakami M, Koda M, Mandai M, et al. Isolated metastases of hepatocellular carcinoma in the right atrium: case report and review of the literature. Oncol Lett 2013; 5:1505–1508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shivathirthan N, Shimoda M, Kosuge T, et al. Recurrent hepatocellular carcinoma with tumor thrombus in right atrium—report of a successful liver resection with tumor thrombectomy using total hepatic vascular exclusion without concomitant cardiopulmonary bypass. Hepatogastroenterology 2012; 59:872–874. [DOI] [PubMed] [Google Scholar]
- 31.Li SS, Jian LL, Gang PB, et al. Removal of hepatocellular carcinoma extending into the right atrium with extracorporeal circulation. Hepatogastroenterology 2012; 59:1591–1593. [DOI] [PubMed] [Google Scholar]
- 32.Sung AD, Cheng S, Moslehi J, et al. Hepatocellular carcinoma with intracavitary cardiac involvement: a case report and review of the literature. Am J Cardiol 2008; 102:643–645. [DOI] [PubMed] [Google Scholar]
- 33.Chang JY, Ka WS, Chao TY, et al. Hepatocellular carcinoma with intra-atrial tumor thrombi. A report of three cases responsive to thalidomide treatment and literature review. Oncology 2004; 67:320–326. [DOI] [PubMed] [Google Scholar]
- 34.Yogita S, Tashiro S, Harada M, et al. Hepatocellular carcinoma with extension into the right atrium: report of a successful liver resection by hepatic vascular exclusion using cardiopulmonary bypass. J Med Invest 2000; 47:155–160. [PubMed] [Google Scholar]
- 35.Wu CC, Hseih S, Ho WM, et al. Surgical treatment for recurrent hepatocellular carcinoma with tumor thrombi in right atrium: using cardiopulmonary bypass and deep hypothermic circulatory arrest. J Surg Oncol 2000; 74:227–231. [DOI] [PubMed] [Google Scholar]
- 36.Kashima Y, Miyazaki M, Ito H, et al. Effective hepatic artery chemoembolization for advanced hepatocellular carcinoma with extensive tumour thrombus through the hepatic vein. J Gastroenterol Hepatol 1999; 14:922–927. [DOI] [PubMed] [Google Scholar]
- 37.Noguchi H, Hirai K, Itano S, et al. Small hepatocellular carcinoma with intravascular tumor growth into the right atrium. J Gastroenterol 1994; 29:41–46. [DOI] [PubMed] [Google Scholar]
- 38.Dazai Y, Katoh T, Katoh I, et al. Effectiveness of chemoembolization therapy for metastatic right atrial tumor thrombus associated with hepatocellular carcinoma. Chest 1989; 96:434–436. [DOI] [PubMed] [Google Scholar]
- 39.Goto H, Kaneko Y, Utoh J, et al. Surgery of hepatoma with intracavitary cardiac extension. Heart Vessels 1986; 2:60–62. [DOI] [PubMed] [Google Scholar]
- 40.Ehrich DA, Widmann JJ, Berger RL, et al. Intracavitary cardiac extension of hepatoma. Ann Thorac Surg 1975; 19:206–211. [DOI] [PubMed] [Google Scholar]