

Abstract
Background
Demand-side strategies could contribute to achieving high and timely vaccine coverage in rural Africa, but require platforms to deliver either messages or conditional cash transfers (CCTs). We studied the feasibility of using short message system (SMS) reminders and mobile phone-based CCTs to reach parents in rural western Kenya.
Methods
In a Health and Demographic Surveillance System (HDSS), mothers with children aged 0–3 weeks old were approached to determine who had access to a mobile phone. SMS reminders were sent three days prior to and on the scheduled day of immunization for 1st (age 6 weeks) and 2nd doses (age 10 weeks) of DTP-HepB-Hib (Pentavalent) vaccine, using open-source Rapid SMS software. Approximately $2.00 USD was sent as cash using mPESA, a mobile money transfer platform (2/3 of mothers), or airtime (1/3 of mothers) via phone if the child was vaccinated within 4 weeks of the scheduled date. Follow-up surveys were done when children reached 14 weeks of age.
Results
We approached 77 mothers; 72 were enrolled into the study (26% owned a phone and 74% used someone else’s). Of the 63 children with known vaccination status at 14 weeks of age, 57 (90%) received pentavalent1 and 54 (86%) received pentavalent2 within 4 weeks of their scheduled date. Of the 61 mothers with follow-up surveys administered at 14 weeks of age, 55 (90%) reported having received SMS reminders. Of the 54 women who reported having received SMS reminders and answered the CCT questions on the survey, 45 (83%) reported receiving their CCT. Most (89%) of mothers in the mPESA group obtained their cash within 3 days of being sent their credit via mobile phone. All mothers stated they preferred CCTs as cash via mobile phone rather than airtime.
Conclusion
The data show that in rural western Kenya mobile phone-based strategies are a potentially useful platform to deliver reminders and cash transfers. Follow-up studies are needed that provide evidence for the effectiveness of these strategies in improving vaccine coverage and timeliness.
INTRODUCTION
Despite clear evidence that immunization is an efficient and cost-effective intervention for improving child survival [1], children in many parts of the world, including much of sub-Saharan Africa, are either unvaccinated or vaccinated late [2]. Much of the efforts to augment immunization over the past decade have appropriately focused on improvements in vaccine supply-side issues (e.g., cold chain, transportation, procurement, and staff training). As coverage improves, lingering deficits and barriers remain to achieving optimal immunization status, many of which cannot be overcome with more supply-side interventions. In particular, demand-side barriers, such as lack of knowledge, forgetfulness, prohibitive transport cost, and competing priorities come to play a more prominent role in hard-to-reach and impoverished populations with persistently low vaccine uptake.
The access and ownership of mobile phones in Africa is rapidly rising [3]. Aside from verbal communication, mobile phones are increasingly being used for health applications (mHealth) and mobile money services (mMoney) [4–8]. We believe some of these new applications of mobile phones could potentially be harnessed to administer interventions to achieve high, timely and sustainable immunization coverage. One application of mobile phones that has become widespread is sending short message service (SMS) reminders. SMSs have been successfully employed for various health applications, such as promoting adherence to drug treatments for chronic diseases[9–11], uptake of screening tests[12–15], immunization coverage[16–18], clinical appointment attendance[19,20], and training health workers in malaria treatment.[21]
mMoney, refers to the technology that facilitates cash transfers through mobile phones mMoney has been used for a range of activities including utility bill/retail payments, person-to-person cash transfers, payrolls, public transport, mobile banking, and international remittances[22]. In many developing countries, mMoney provides an opportunity to reach rural and/or low-income population who otherwise have limited or no access to formal financial institutions. In Kenya, the mPESA system has been a leader in offering mobile financial services, currently claiming 14 million users [23], approximately 30–35% of the total population (43 million) [24].
Economic incentives targeting both health care providers [25] and the general population have been used to improve health outcomes by encouraging use of various health services, including immunizations [26–28]. Individual incentives to improve immunization include food vouchers [29], grocery items [30], and cash transfers [27]. A specific type of incentive are conditional cash transfers (CCTs), which are the provision of money (or other valuable goods) upon completion of a particular health behavior [27,28,31,32]. Due to its growing reach, mPESA and other mMoney providers can potentially serve as a platform to provide paperless CCTs to improve immunization coverage.
While use of SMS reminders and mobile-phone based CCTs hold promise for improving immunization coverage and timeliness, rigorous evidence is needed before scaling up such interventions. Moreover, operational and technical logistics of such programs must be worked though before expanding them. We undertook a feasibility study of using automated SMS reminders and mobile-phone based CCTs for timely immunization among mothers in rural western Kenya.
METHODS
Study site
The study was conducted in the Kenya Medical Research Institute/Centers for Disease Control and Prevention’s Health (KEMRI/CDC) and Demographic surveillance system (HDSS) in rural Siaya District, western Kenya[33].Within the HDSS, this pilot study was conducted in 30 villages located within 5 km radius of the government operated Ting’ Wang’i health center. In the HDSS area, malaria is holoendemic[34,35] and HIV prevalence is high (17% in adults ≥18 years in 2008)[36]. The under-5 mortality rate was 212 per 1,000 live births in 2008[34]. As part of the HDSS, births and deaths are identified on an ongoing basis by village reporters (VRs), who are residents of each village [33]. Immunization status of children, collected by field workers during home visits done three times per year, is determined primarily by vaccination card, and if not available, by verbal report. Immunization coverage with the third dose of pentavalent vaccine was 54% by 24 weeks of age (scheduled to be given at 14 weeks) and 83% by ages 12–23 months in 2010. Vaccinations are also documented in Ting’ Wang’i health center by HDSS-employed health facility recorders. The Kenyan Expanded Program on Immunization (EPI) guidelines call for vaccination with the primary series at 6, 10 and 14 weeks of age and measles at 9 months of age [37].
Enrolment into the pilot study
We enrolled mothers of children 0–3 weeks of age, randomly distributed in a 2:1 mMoney:airtime ratio. This number was chosen, without statistical considerations, to enroll enough mothers in each group to encounter most of the main contingencies and problems that might occur with the process. For enrolment, VRs approached mothers of newborns at the time of the birth notification visit, as well as children up to 4 weeks of age in their villages. Mothers were informed that they would receive 150 Kenya shillings (~US$2.00 in 2011) in mMoney or equivalent in airtime if they brought their child in on time, defined as within 4 weeks, for their first and second pentavalent vaccines. The CCT amount was chosen as it was the standard transport reimbursement given for all studies conducted in the HDSS, representing the average cost of round-trip transportation to the clinic for HDSS residents. After consenting to participate, mothers were asked to provide a phone number of a mobile phone from which they could receive short message service (SMS) messages related to this study. We defined mobile phone access as owning a phone or readily being able to receive messages from a phone owned by someone living in their compound, a neighbor or a friend.
SMS reminders
We customized RapidSMS, a free and open source system designed to leverage SMS mobile phone technologies [38]. The system has the capability of sending and receiving multiple messages at once and could be used on basic mobile phones. At the time of enrollment, VRs sent a message to the RapidSMS server at KEMRI/CDC offices, located approximately 50 km from Ting’ Wang’i, using the following syntax: name, date of birth, phone number (Figure 1). At this point, the phone was automatically registered by the server, which was programmed to send the first SMS immunization reminder three days before the child reached six weeks of age based on the indicated date of birth in the enrollment SMS. The first reminder SMS read“[Baby’s name] is due for Pentavalent1 vaccination in three days (e.g., Wednesday) 13/7/2011 at Ting’ Wang’i. You will get Ksh. 150 by mPESA(or airtime) if baby is vaccinated on time.” On the day the baby was exactly six weeks old, the mother was sent a second SMS with a similar message that emphasized that vaccination was due on that day. If the child had come for vaccination at Ting’ Wang’i for the first dose, SMS reminders were next sent three days prior to and on the day that the second pentavalent dose was due. If the child did not get vaccinated at Ting’ Wang’i exactly at six weeks for the first vaccination, then the SMS reminders were reprogrammed to occur four weeks after first dose. Of note, if the first dose was not given at the designated vaccination clinic, Ting’ Wang’i, then the system was not aware that the first dose was given and no SMS reminders were sent for the second dose. All the SMS reminders were sent in the local language (Dholuo).
Figure 1.
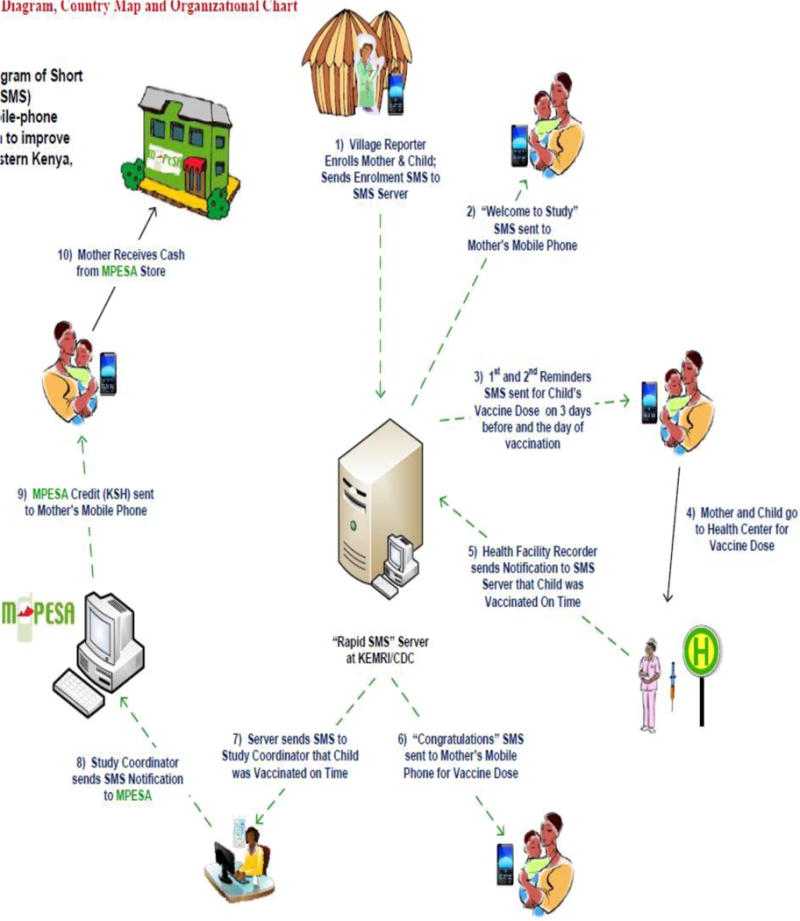
Flow diagram of short message service (SMS’s) for mobile phone-based intervention to improve immunization, Kenya 2011.
Immunizations and CCTs
A study-employed health facility recorder was based at Ting’ Wang’i to record immunization visits of enrolled children (Figure 1). Every Monday, the recorder was provided with a list of expected immunization visits by enrolled children for that week. When a child was brought in for immunization, the health facility recorder verified from the list that the child was a study participant and then notified the server via an SMS of the child’s visit. The server sent simultaneous SMSs to the participant’s phone, congratulating her on vaccinating her child on time, and to the study coordinator, notifying her that child was vaccinated on time. For children who were brought in for vaccination after 4 weeks, a SMS was sent by the server to the mother congratulating her on vaccinating her child, but indicated that it was not done within a timeframe that entitled her to receive the CCT.
Mothers were randomized to one of the two CCT groups, either mMoney or airtime. Any of the four mMoney systems registered in Kenya could be used for CCTs, based on the mother’s preference. For mothers who vaccinated their child on time, CCTs were sent to the mother’s registered mobile phone. For those randomized to get the CCT via mMoney, we sent a credit worth Ksh.150 to each participant’s registered mobile phone. Mothers could redeem the credit for cash at any of the many retail agents in the area. For those participants randomized to receive airtime, we directly transferred Ksh.150 worth of airtime credit that could be used instantly.
Follow-up visits
All enrolled mothers were followed-up at home 4 weeks after their second scheduled vaccination visit. A trained field worker administered a questionnaire to evaluate if the mother received the SMS reminders, if she brought her child in for immunization, and if she received the CCT. For those who answered in the negative to these questions, we inquired about the reasons. We also asked about which factors motivated the mother to bring the child in for vaccination and what factors they thought would motivate other mothers in their community to bring their children in for timely vaccination.
Data collection and analysis
Data was collected at enrollment, at the clinic and during the follow-up home visits using scannable questionnaires (Cardiff Software Inc, Vista, CA). We determined vaccination status of children through recording visits at Ting’ Wang’i health center and at the end of study follow-up visit. Scanned data were processed and stored in Microsoft Corporation SQL Server 2008 R2 ® database at the KEMRI/CDC data center. Frequencies of responses to questions were calculated using SAS, version 9.2 © 2002–2008 by SAS Institute Inc., Cary, NC, USA. No statistical analysis was done.
Ethical Review
The study protocol was reviewed and approved by institutional review boards of CDC (Atlanta, GA) and KEMRI (Nairobi, Kenya). Informed written consent for participation was obtained from participants.
RESULTS
Enrolment and vaccination status
Among 77 mothers of newborn children approached for enrollment, 72 (94%) were enrolled; only two mothers refused participation (Figure 2). The characteristics of enrolled mothers are shown in Table 1. Of the 72 enrolled mothers, 9 were lost to follow-up by the end of the study and their children’s vaccination status was not known. Of the 63 children with known vaccination status, 57 (90%) received pentavalent1 and 54 (86%) received pentavalent2 by 14 weeks of age (Figures 2 and 3). Fifty children (91%) who received pentavalent1 and 47 (75%) who received pentavalent2 were vaccinated at the designated referral clinic, Ting’ Wang’i health center.
Figure 2.
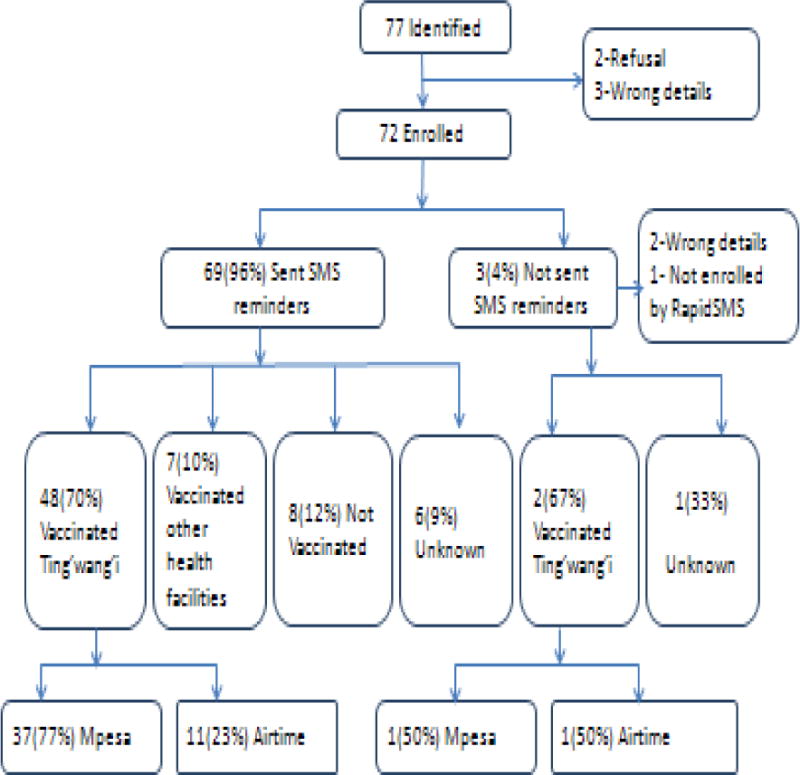
Pentavalent1 vaccination results.
Table 1.
Characteristics of enrolled participants by mobile phone ownership status, western Kenya, 2011
| Characteristic | Owns mobile phone (N=19) | Does not own mobile phone (N=53) | Totala | P value comparing those who own and don’t own phone | |||
|---|---|---|---|---|---|---|---|
|
| |||||||
| N | % | n | % | n | % | ||
| Infant age at enrolment | 0.494 | ||||||
| < 7 days | 6 | 31.6% | 11 | 20.8% | 17 | 23.6% | |
| 8–13 | 4 | 21.0% | 14 | 26.4% | 18 | 25.0% | |
| 14–20 | 3 | 15.8% | 16 | 30.2% | 19 | 26.4% | |
| 21–27 | 6 | 31.6% | 12 | 22.6% | 18 | 25.0% | |
| Maternal age (years) | 0.074 | ||||||
| <20 | 0 | 0.0% | 6 | 15.8% | 6 | 11.8% | |
| 20–29 | 6 | 46.1% | 23 | 60.5% | 29 | 56.9% | |
| >29 | 7 | 53.9% | 9 | 23.7% | 16 | 31.4% | |
| Maternal Education* | 0.369 | ||||||
| Some Primary | 8 | 66.7% | 16 | 43.2% | 24 | 50.0% | |
| Completed Primary | 3 | 25.0% | 16 | 43.2% | 19 | 38.8% | |
| Some Secondary | 1 | 8.3% | 5 | 13.5% | 6 | 12.2% | |
| Ability to read English | 0.746 | ||||||
| Not at all | 0 | 0% | 1 | 2.7% | 1 | 2.0% | |
| With difficulty | 7 | 58.3% | 18 | 48.65% | 25 | 51.0% | |
| Easily | 5 | 41.7% | 18 | 48.65% | 23 | 47.0% | |
| Ability to speak English | 0.238 | ||||||
| Not at all | 1 | 8.3% | 1 | 2.7% | 2 | 4.0% | |
| With difficulty | 8 | 66.7% | 17 | 46.0% | 25 | 51.1% | |
| Easily | 3 | 25.0% | 19 | 51.4% | 22 | 44.9% | |
| Ability to write English | 8.3% | 0.730 | |||||
| Not at all | 1 | 58.3% | 2 | 5.4% | 3 | 6.1% | |
| With difficulty | 7 | 33.3% | 18 | 48.7% | 25 | 51.0% | |
| Easily | 4 | 17 | 46.0% | 21 | 42.9% | ||
| # of people in houseb | 3.7 | 1.7 | 4.4 | 2.1 | 4.2 | 2.0 | 0.268 |
| SESc | 0.791 | ||||||
| Bottom 2 quintiles | 2 | 25.0% | 6 | 30.0% | 8 | 28.6% | |
| Upper 3 quintiles | 6 | 75.0% | 14 | 70.0% | 20 | 71.4% | |
Different denominators due to missing HDSS data
Mean and STD
Calculated using multiple components analysis from all households in HDSS area.
Figure 3.
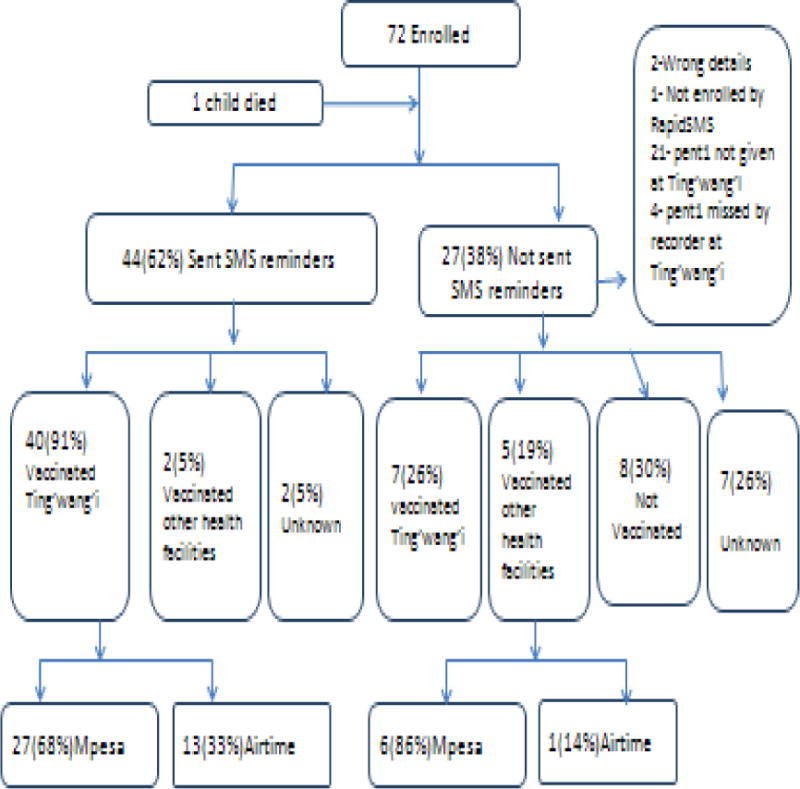
Pentavalent2 vaccination results.
The reasons reported by 8 mothers for not vaccinating their children were the following: forgot to take the child for vaccination, the vaccine was not available at Ting’ Wang’i, was away at the time when the child was due for vaccination, child died before the scheduled vaccination date, her church is against vaccination, was not informed of any SMS reminder by the neighbor whom the mobile phone belonged to, was taking care of a sick person when the child was due for vaccination, and was sick at the time the child was to due for vaccination [one (13%) mother for each reason].
Phone ownership
All 77 mothers approached for enrollment identified a mobile phone on which they thought they could receive SMSs. Of the 72 enrolled mothers, 19 (26%) had their own phones and 53 (74%) had access to someone else’s phone – 20 (38%) used their husbands’ phones, 20 (38%) used their neighbors’ phones, 12 (22%) used the phone of someone within their compound or household, and 1 (2%) used the village reporter’s phone.
SMS reminders
Of the 72 enrolled mothers, 69 (96%) were sent SMS reminders for their first routine EPI visit at 6 weeks of age; 2 of the children’s dates of birth were entered incorrectly in the enrollment SMS by the village reporter sent and 1 child did not have an enrollment SMS sent by the village reporter (Figure 2). Of the 72 enrolled mothers, 44 (61%) were sent SMS reminders for the second scheduled EPI vaccinations. Twenty-one mothers who did not visit Ting’ Wang’i for their children’s first EPI visit were not sent SMS reminders for their second EPI visit, as per the coding algorithm of the rapid SMS system. Of the 111 doses of pentavalent1 and pentavalent2 that were given, 57% were given on the scheduled day of vaccination and 88% were given within 3 days of the scheduled date (Figure 4).
Figure 4.
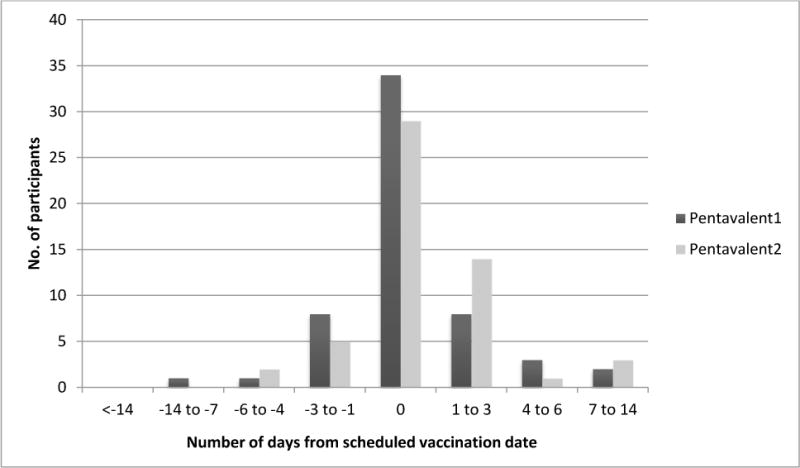
Time of vaccination of study participants in relationship to scheduled date, western Kenya, 2011
Of the 61 mothers with follow-up surveys administered, 55 (90%) reported having received SMS reminders. Three mothers reported that the SMS never appeared on the designated phone and three mothers who were using another person’s phone reported that the SMS’s were not conveyed to them. Among the 55 who received SMS reminders, the number who reported having received four, three, two and one SMS reminders was 22 (44%), 7 (13%), 18 (33%) and 8 (14%), respectively. Forty-nine (91%) mothers reported that the SMS reminders influenced their decision to come in for vaccination and 51 (94%) said the number of SMS reminders they received did not bother them.
CCTs
Among enrolled women, 48 (67%) were randomly assigned to the mMoney group and 24 (33%) to the airtime group (Figure 2). All participants in the mMoney group chose to use mPESA as their preferred mMoney network. Of the 54 women who reported having received SMS reminders and completed the follow-up interview, 45 (83%) reported receiving their CCT –6 in the mMoney group and 3 in the airtime group reported not having received it. Of the 47 mothers in the mMoney group, 37 (77%) completed the follow-up questionnaire. Of these, 23 (62%) received the cash on the same day the mPESA credit was sent to them, 10 (27%) within 3 days, and 4 (11%) more than a week later. Eight (22%) mothers traveled less than a half kilometer and 23 (62%) less than 2 kilometers to get their cash at the mPESA agent. Only 1 (3%) had to travel more than 5 km. Thirty-two (86%) of mothers in the mMoney group were already registered in mPESA and 35 (95%) had used mPESA previously.
All 54 mothers who completed the follow-up survey stated they would prefer mMoney payments over airtime. Thirty-three (61%) claimed mMoney was “worth more”, 16 (30%) said it was “better to have cash than airtime” and 5 (9%) said it was “easier.” All 54 mothers said they thought paying mothers would influence their decision to get their children vaccinated on time. However, when asked what factor most influenced their own decision to get their child vaccinated, 21(47%) said the SMS reminder, 16 (36%) said neither the SMS reminder nor the CCT, 2 (4%) said the CCT, 2 (4%) said both, and 3 (7%) said “other”. When asked “What is the least amount of payment that would encourage you to bring your child into vaccination?” 22 (40%) said at least 150 Ksh ($2.00), 20 (37%) said at least 200 Ksh ($2.66) and 12 (22%) said more than 200 Ksh.
Discussion
The results of our pilot study show evidence of the feasibility of setting up an integrated mobile phone-based system to remind and incentivize mothers to vaccinate their children in rural Kenya. The pilot study successfully achieved several of its objectives. We identified mothers of newborn infants and enrolled them before the date of their child’s first EPI visit. We trained village reporters, a group of women with minimal formal education, to register mothers using mobile phone technology. We set up an automated program to deliver SMS reminders at designated times to enrolled mothers. We successfully delivered CCTs to mothers using a paperless remuneration strategy with mPESA, which minimized the logistical challenges and potential for fraud inherent in delivering cash or tangible goods as CCTs. Lastly, the strategy was well-accepted by mothers, who expressed mostly positive impressions of their experience at the end of the study.
Despite moderate levels of mobile phone ownership among mothers, access to mobile phones within the participant’s immediate circle was high with every woman approached being able to identify someone’s phone to receive SMSs. Only a few women who were using someone else’s phone did not have the reminders delivered to them. We hypothesized that the CCT would foster ingenuity in the “local economy” so that mothers without phones would find ways to get messages and receive the small CCTs. This seemed to be borne out by our findings, although we did not inquire if mothers shared their CCTs with the owners of the phones.
The small sample size and lack of a comparison group prevents drawing conclusions about the effectiveness of SMS reminders and CCTs to improve vaccine coverage and timeliness. However, pentavalent2 coverage was 95% for the 42 participants who received SMS reminders and whose vaccination status could be ascertained. This is in contrast to 60% pentavalent2 coverage for the 20 individuals who did not receive SMS reminders and whose vaccine status was ascertained. Studies conducted in low-income, minority, populations in New York City found that SMS reminders improve coverage from 4–17%, depending on the vaccine[18]. Additionally, CCTs or other incentives, have increased vaccine coverage by 2.8–13.6% in other parts of the world [25–31,39].
The pilot study did identify several problems with the current system. Despite its automation, the system was still subject to human error. In several instances, VRs entered date of birth or mobile phone numbers incorrectly, which resulted in SMSs being sent at the wrong time or to the wrong phone. More training of the importance of entering correct data is needed. Second, the SMS reminder algorithm was programmed on the assumption that all participants would use the Ting’ Wang’i health facility for vaccination. If a mother brought her child to another clinic for pentavalent1, the system considered that child unvaccinated for pentavalent1 and did not send a SMS reminder for pentavalent2. This programming glitch should be addressed for future interventions. Third, in a few cases after a mother enrolled, her husband did not approve of the study or suspected that the vaccines being given were experimental. More extensive engagement of husbands in the community is important since this strategy extends beyond the traditional mother-child pair targeted for most immunization-related interventions. Fourth, we only designated one health facility where children’s vaccination status could be verified. The distance-decay effect posits that as one’s distance from a health facility increases, the likelihood of utilization decreases [40]. In this study, mothers who live the farthest from the designated clinic might have preferred bringing their child to a clinic closer to their home for vaccination, despite receipt of remuneration only at the designated facility.
Using the lessons learned in the pilot study in establishing a mobile phone-based system to send SMSs and deliver CCTs, we plan to investigate the impact of this intervention on timely vaccination in a larger randomized trial. Although there is a great deal of interest and excitement surrounding mHealth and CCT programs in Africa, there is insufficient evidence documenting their effectiveness [22,27]. Such evidence will serve as a basis of the investment, time and effort that will be necessary to introduce and, then, potentially scale-up these programs in Kenya and other countries in Africa.
Footnotes
The findings and conclusions are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
References
- 1.Andre FE, Booy R, Bock HL, Clemens J, Datta SK, John TJ, et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull World Health Organ. 2008;86(2):140–6. doi: 10.2471/BLT.07.040089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Clark A, Sanderson C. Timing of children’s vaccinations in 45 low-income and middle-income countries: an analysis of survey data. Lancet. 2009;373(9674):1543–9. doi: 10.1016/S0140-6736(09)60317-2. [DOI] [PubMed] [Google Scholar]
- 3.BBC News. Africa’s mobile phone industry ‘booming’. 2011 http://www.bbc.co.uk/news/world-africa-15659983. Date accessed: April 20, 2012.
- 4.Kamanga A, Moono P, Stresman G, Mharakurwa S, Shiff C. Rural health centres, communities and malaria case detection in Zambia using mobile telephones: a means to detect potential reservoirs of infection in unstable transmission conditions. Malar J. 2010;9:96. doi: 10.1186/1475-2875-9-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Meankaew P, Kaewkungwal J, Khamsiriwatchara A, Khunthong P, Singhasivanon P, Satimai W. Application of mobile-technology for disease and treatment monitoring of malaria in the “Better Border Healthcare Programme”. Malar J. 2010;9:237. doi: 10.1186/1475-2875-9-237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tamrat T, Kachnowski S. Special Delivery: An Analysis of mHealth in Maternal and Newborn Health Programs and Their Outcomes Around the World. Matern Child Health J. 2011 doi: 10.1007/s10995-011-0836-3. [DOI] [PubMed] [Google Scholar]
- 7.Onono M, Carraher N, Cohen R, Bukusi E, Turan J. Use of personal digital assistants for data collection in a multi-site AIDS stigma study in rural south Nyanza, Kenya. Afr Health Sci. 2011;11(3):464–73. [PMC free article] [PubMed] [Google Scholar]
- 8.Pop-Eleches C, Thirumurthy H, Habyarimana JP, Zivin JG, Goldstein MP, de Walque D, et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011;25(6):825–34. doi: 10.1097/QAD.0b013e32834380c1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lester RT, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–45. doi: 10.1016/S0140-6736(10)61997-6. [DOI] [PubMed] [Google Scholar]
- 10.Vervloet M, van Dijk L, Santen-Reestman J, van Vlijmen B, Bouvy ML, de Bakker DH. Improving medication adherence in diabetes type 2 patients through Real Time Medication Monitoring: a randomised controlled trial to evaluate the effect of monitoring patients’ medication use combined with short message service (SMS) reminders. BMC Health Serv Res. 2011;11:5. doi: 10.1186/1472-6963-11-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Strandbygaard U, Thomsen SF, Backer V. A daily SMS reminder increases adherence to asthma treatment: a three-month follow-up study. Respir Med. 2010;104(2):166–71. doi: 10.1016/j.rmed.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 12.Dokkum NF, Koekenbier RH, van den Broek IV, van Bergen JE, Brouwers EE, Fennema JS, et al. Keeping participants on board: increasing uptake by automated respondent reminders in an Internet-based Chlamydia Screening in the Netherlands. BMC Public Health. 2012;12(1):176. doi: 10.1186/1471-2458-12-176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.de Tolly K, Skinner D, Nembaware V, Benjamin P. Investigation into the use of short message services to expand uptake of human immunodeficiency virus testing, and whether content and dosage have impact. Telemed J E Health. 2012;18(1):18–23. doi: 10.1089/tmj.2011.0058. [DOI] [PubMed] [Google Scholar]
- 14.Lakkis NA, Atfeh AM, El-Zein YR, Mahmassani DM, Hamadeh GN. The effect of two types of sms-texts on the uptake of screening mammogram: a randomized controlled trial. Prev Med. 2011;53(4–5):325–7. doi: 10.1016/j.ypmed.2011.08.013. [DOI] [PubMed] [Google Scholar]
- 15.Khokhar A. Short text messages (SMS) as a reminder system for making working women from Delhi Breast Aware. Asian Pac J Cancer Prev. 2009;10(2):319–22. [PubMed] [Google Scholar]
- 16.Kharbanda EO, Stockwell MS, Fox HW, Andres R, Lara M, Rickert VI. Text message reminders to promote human papillomavirus vaccination. Vaccine. 2011;29(14):2537–41. doi: 10.1016/j.vaccine.2011.01.065. [DOI] [PubMed] [Google Scholar]
- 17.Stockwell MS, Kharbanda EO, Martinez RA, Lara M, Vawdrey D, Natarajan K, et al. Text4Health: impact of text message reminder-recalls for pediatric and adolescent immunizations. Am J Public Health. 2012;102(2):e15–21. doi: 10.2105/AJPH.2011.300331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Stockwell MS, Kharbanda EO, Martinez RA, Vargas CY, Vawdrey DK, Camargo S. Effect of a text messaging intervention on influenza vaccination in an urban, low-income pediatric and adolescent population: a randomized controlled trial. JAMA. 2012;307(16):1702–8. doi: 10.1001/jama.2012.502. [DOI] [PubMed] [Google Scholar]
- 19.Guy R, Hocking J, Wand H, Stott S, Ali H, Kaldor J. How effective are short message service reminders at increasing clinic attendance? A meta-analysis and systematic review. Health Serv Res. 2012;47(2):614–32. doi: 10.1111/j.1475-6773.2011.01342.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hasvold PE, Wootton R. Use of telephone and SMS reminders to improve attendance at hospital appointments: a systematic review. J Telemed Telecare. 2011;17(7):358–64. doi: 10.1258/jtt.2011.110707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zurovac D, Sudoi RK, Akhwale WS, Ndiritu M, Hamer DH, Rowe AK, et al. The effect of mobile phone text-message reminders on Kenyan health workers’ adherence to malaria treatment guidelines: a cluster randomised trial. Lancet. 2011;378(9793):795–803. doi: 10.1016/S0140-6736(11)60783-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gencer M. The Mobile Money Movement: Catalyst to Jumpstart Emerging Markets. Innovations. 2011:3–19. Winter. [Google Scholar]
- 23.Safaricom. M-PESA Customer and Agent Numbers. http://www.safaricom.co.ke/fileadmin/M-PESA/Documents/statistics/M-PESA_Statistics_-_2.pdf. Date accessed: February 20, 2012.
- 24.Central Intelligence Agency. The World Factbook: Kenya. https://www.cia.gov/library/publications/the-world-factbook/geos/ke.html. Date accessed: May 8, 2012.
- 25.Basinga P, Gertler PJ, Binagwaho A, Soucat AL, Sturdy J, Vermeersch CM. Effect on maternal and child health services in Rwanda of payment to primary health-care providers for performance: an impact evaluation. Lancet. 2011;377(9775):1421–8. doi: 10.1016/S0140-6736(11)60177-3. [DOI] [PubMed] [Google Scholar]
- 26.Arnold C, Conaway T, Greenslade M. Cash Transfers Evidence Paper. Department for International Development. 2011 Apr; http://webarchive.nationalarchives.gov.uk/+/http://www.dfid.gov.uk/Documents/publications1/cash-transfers-evidence-paper.pdf. Date accessed May 8, 2012.
- 27.Gaarder M, Glassman A, Todd J. Conditional cash transfers and health: unpacking the causal chain. Journal of Development Effectiveness. 2010;2(1):6–50. [Google Scholar]
- 28.Lagarde M, Haines A, Palmer N. Conditional cash transfers for improving uptake of health interventions in low- and middle-income countries: a systematic review. JAMA. 2007;298(16):1900–10. doi: 10.1001/jama.298.16.1900. [DOI] [PubMed] [Google Scholar]
- 29.Chandir S, Khan AJ, Hussain H, Usman HR, Khowaja S, Halsey NA, et al. Effect of food coupon incentives on timely completion of DTP immunization series in children from a low-income area in Karachi, Pakistan: a longitudinal intervention study. Vaccine. 2010;28(19):3473–8. doi: 10.1016/j.vaccine.2010.02.061. [DOI] [PubMed] [Google Scholar]
- 30.Banerjee AV, Duflo E, Glennerster R, Kothari D. Improving immunisation coverage in rural India: clustered randomised controlled evaluation of immunisation campaigns with and without incentives. BMJ. 2010;340:c2220. doi: 10.1136/bmj.c2220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Barham T, Maluccio J. (Health and Society Program Working Paper HS2008-01).Eradicating Diseases: The Effect of Conditional Cash Transfers on Vaccination Coverage in Nicaragua. 2008 doi: 10.1016/j.jhealeco.2008.12.010. http://www.colorado.edu/ibs/pubs/hs/hs2008-0001.pdf. [DOI] [PubMed]
- 32.Morris SS, Flores R, Olinto P, Medina JM. Monetary incentives in primary health care and effects on use and coverage of preventive health care interventions in rural Honduras: cluster randomised trial. Lancet. 2004;364(9450):2030–7. doi: 10.1016/S0140-6736(04)17515-6. [DOI] [PubMed] [Google Scholar]
- 33.Adazu K, Lindblade KA, Rosen DH, Odhiambo F, Ofware P, Kwach J, et al. Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. Am J Trop Med Hyg. 2005;73(6):1151–8. [PubMed] [Google Scholar]
- 34.Hamel MJ, Adazu K, Obor D, Sewe M, Vulule J, Williamson JM, et al. A reversal in reductions of child mortality in western Kenya, 2003–2009. Am J Trop Med Hyg. 2011;85(4):597–605. doi: 10.4269/ajtmh.2011.10-0678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Phillips-Howard PA, Nahlen BL, Wannemuehler KA, Kolczak MS, ter Kuile FO, Gimnig JE, et al. Impact of permethrin-treated bed nets on the incidence of sick child visits to peripheral health facilities. Am J Trop Med Hyg. 2003;68(4 Suppl):38–43. [PubMed] [Google Scholar]
- 36.Dalal W, Feikin D, Amolloh M, Ransom R, Burke H. Home-based HIV Counseling and Testing in rural and urban Kenyan communities. JAIDS. 2012 doi: 10.1097/QAI.0b013e318276bea0. In press. [DOI] [PubMed] [Google Scholar]
- 37.Republic of Kenya Ministry of Health. Division of Vaccines and Immunization (DVI) Multi Year Plan 2006–2010. http://www.sabin.org/files/uploads/pdfs/cMYP_Kenya.pdf. Date accessed: May 25, 2012.
- 38.RapidSMS. http://www.rapidsms.org. Date accessed: February 20, 2012.
- 39.Brenzel L, Barham T, Maluccio J. Beyond 80%: Are There New Ways of Increasing Vaccination Coverage? Evaluation of CCT Programs in Mexico and Nicaragua. http://paa2008princetonedu/downloadaspx?submissionId=806652007. Date accessed: May 15, 2012.
- 40.Stock R. Distance and the utilization of health facilities in rural Nigeria. Soc Sci Med. 1983;17(9):563–70. doi: 10.1016/0277-9536(83)90298-8. [DOI] [PubMed] [Google Scholar]