

Abstract
Objective:
To characterize demographic and clinical features in pregnant women presenting with acute headache, and to identify clinical features associated with secondary headache.
Methods:
We conducted a 5-year, single-center, retrospective study of consecutive pregnant women presenting to acute care with headache receiving neurologic consultation.
Results:
The 140 women had a mean age of 29 ± 6.4 years and often presented in the third trimester (56.4%). Diagnoses were divided into primary (65.0%) and secondary (35.0%) disorders. The most common primary headache disorder was migraine (91.2%) and secondary headache disorders were hypertensive disorders (51.0%). The groups were similar in demographics, gestational ages, and most headache features. In univariate analysis, secondary headaches were associated with a lack of headache history (36.7% vs 13.2%, p = 0.0012), seizures (12.2% vs 0.0%, p = 0.0015), elevated blood pressure (55.1% vs 8.8%, p < 0.0001), fever (8.2% vs 0.0%, p = 0.014), and an abnormal neurologic examination (34.7% vs 16.5%, p = 0.014). In multivariate logistic regression, elevated blood pressure (odds ratio [OR] 17.0, 95% confidence interval [CI] 4.2–56.0) and a lack of headache history (OR 4.9, 95% CI 1.7–14.5) had an increased association with secondary headache, while psychiatric comorbidity (OR 0.13, 95% CI 0.021–0.78) and phonophobia (OR 0.29, 95% CI 0.09–0.91) had a reduced association with secondary headache.
Conclusions:
Among pregnant women receiving inpatient neurologic consultation, more than one-third have secondary headache. Diagnostic vigilance should be heightened in the absence of a headache history and if seizures, hypertension, or fever are present. Attack features may not adequately distinguish primary vs secondary disorders, and low thresholds for neuroimaging and monitoring for preeclampsia are justified.
The most common primary headache disorders have a peak prevalence and incidence at a younger age and affect women disproportionately, particularly during childbearing years.1 The female predilection may be explained by the relationship of headache and sex hormones, particularly estrogen.2 Migraine is the most common disabling primary headache disorder, and, in pregnancy, retrospective and prospective studies consistently demonstrate that by the second trimester, migraine frequency typically improves, although attacks of migraine with aura and aura without headache may not reflect this pattern.3–10
Acute, severe headache in pregnancy is generally regarded as a “red flag” and a cause for further investigation, particularly when new onset.11–13 Various secondary headache disorders are more likely to occur during this time period,12 possibly related to hypercoagulability, hormonal factors, anesthesia for labor, and other mechanisms.
Acute headache in pregnancy is a common cause for urgent inpatient neurologic consultation and often results in diagnostic challenges. In pregnant women, a preceding headache history is frequent, and differentiating between a severe headache as a manifestation of preexisting migraine and a newly acquired, more ominous disorder may be difficult. Guidelines do not exist for diagnostic strategies in this patient population, developed algorithms are not validated,14,15 and clinical series describing demographics, symptomatology, and diagnoses of pregnant women evaluated for acute headache are scarce.16,17
We aimed to study a large number of pregnant women presenting with acute headache to the inpatient setting to better characterize demographics, comorbidities, symptoms, examination findings, rates, and risk factors of primary and secondary headache diagnoses.
METHODS
This study was conducted as a chart review of neurologic consultations for pregnant women aged 18 years and older presenting with acute headache to the emergency department, labor and delivery triage, or antepartum units of the Jack D. Weiler Hospital of Montefiore Medical Center in the Bronx, NY, an urban, tertiary referral center.
All neurology consultations requested by the obstetrical team for acute headache from July 1, 2009, through June 30, 2014, were reviewed in detail retrospectively. All consultations were performed by a team that comprised a neurology resident and a teaching service attending participating in this research.
Measures ascertained from the chart review included demographic variables such as age and ethnicity, pregnancy features including parity, gestational age, trimester, antepartum complications, and history of medical, neurologic, and obstetrical illnesses. Details related to headache history and acute headache symptoms were reviewed including pain location, laterality, duration, attack frequency, associated symptoms including nausea, vomiting, photophobia, phonophobia, triggers, aura, and aggravating and relieving factors. Elevated blood pressure was defined as a single measurement of the systolic blood pressure ≥140 mm Hg or a diastolic blood pressure ≥90 mm Hg. Fever was defined as a single temperature ≥100.4°F. Neurologic examination abnormalities were reviewed and further distinguished based on their relevancy to the acute headache syndrome with associated features. For example, numbness in the first 3 digits of the hand in a patient with carpal tunnel syndrome would be classified as an abnormal neurologic examination finding, but not one referable to the acute headache syndrome. However, sensory loss in a limb believed to be acutely numb in the context of the acute headache attack would be classified as both an abnormal finding in general and one referable to the acute headache syndrome. Diagnostic tests were also recorded, including neuroimaging and CSF analysis as performed. Past headache diagnoses and diagnosis of the acute attack with such background in clinical practice were reviewed and final diagnoses were assigned using the International Classification of Headache Disorders, 3rd edition (beta version) (ICHD-3 beta).18 For simplicity of diagnostic categories, probable migraine without aura and probable migraine with aura were classified as migraine with and without aura, but the presence of entirely new-onset headache and aura was distinguished. A few diagnoses in clinical practice did not fit into the ICHD-3 beta schema, which were noted in the results.
The data were compiled into a confidential Microsoft Excel database free of patient identifiers where descriptive statistics were generated. The statistical analysis was performed using SPSS Statistics, version 21 (IBM, Armonk, NY). Subgroup proportions were compared using χ2 or Fisher exact test depending on cell size, and subgroup means were compared using an unpaired t test. Using binomial logistic regression, we assessed the dichotomous outcome of secondary vs primary headache as the dependent variable with independent variables having a p value <0.20 in univariate analyses, excluding categorical variables where any cell size was <2. Statistical significance for all analyses was defined as a p value ≤0.05.
Standard protocol approvals, registrations, and patient consents.
Approval from Montefiore Medical Center's institutional review board was obtained before study initiation. Informed consent from patients was not required based on the retrospective review of medical records.
RESULTS
Clinical assessment.
Over the 5-year period, we evaluated 140 pregnant women presenting with acute headache. The women had a mean age of 29.4 (±6.4) years and were mostly African American (39.3%) or Hispanic (36.4%). On average, the patients had 3.8 (±2.6) pregnancies and 1.3 (±1.3) previous live births, with 15.0% primigravidas, 32.6% multiparas (≥2 viable pregnancies), and 2.8% grand multiparas (≥7 births). A history of headache was present in 78.6%. Any neurologic examination abnormalities were present in 30.7%, and 87.9% had neuroimaging. Diagnoses for acute attacks were broadly divided into primary headache (65.0%) and secondary headache (35.0%) (figure). Migraine was the most common diagnosis overall, consisting of 59.3% of the sample and 91.2% of primary headache. Within the primary headache group, 57.1% had migraine without aura, 37.4% had migraine with aura, 8.8% had chronic migraine, and 33.0% had status migrainosus. Within the secondary headache group, hypertensive disorders of pregnancy were the most frequently assigned diagnosis (51.0%), predominated by preeclampsia (38.8%). Three patients (6.1%) developed pneumocephalus immediately after spinal/epidural anesthesia19 and will be described in detail separately.
Figure. Final headache diagnoses in pregnant women.

Percentages within chart categories may summate to greater than 100% because some patients have multiple diagnoses. The denominator for all percentages is the size of the total sample (n = 140). “Other” category consists of single patients diagnosed with post–dural puncture headache, arteriovenous malformation, acute posttraumatic headache, metabolic disorder, sickle cell crisis, retropharyngeal abscess, and moyamoya syndrome with bihemispheric ischemic infarctions. The following diagnoses are not classified in the ICHD-3 beta: PRES, HELLP, pneumocephalus, sickle cell crisis, retropharyngeal abscess, and moyamoya syndrome. HELLP = hemolysis, elevated liver enzymes, and low platelet count; HTN = hypertension; ICHD-3 beta = International classification of headache disorders, 3rd edition (beta version); PRES = posterior reversible encephalopathy syndrome; RCVS = reversible cerebral vasoconstriction syndrome.
Patients, demographics, and pregnancy details.
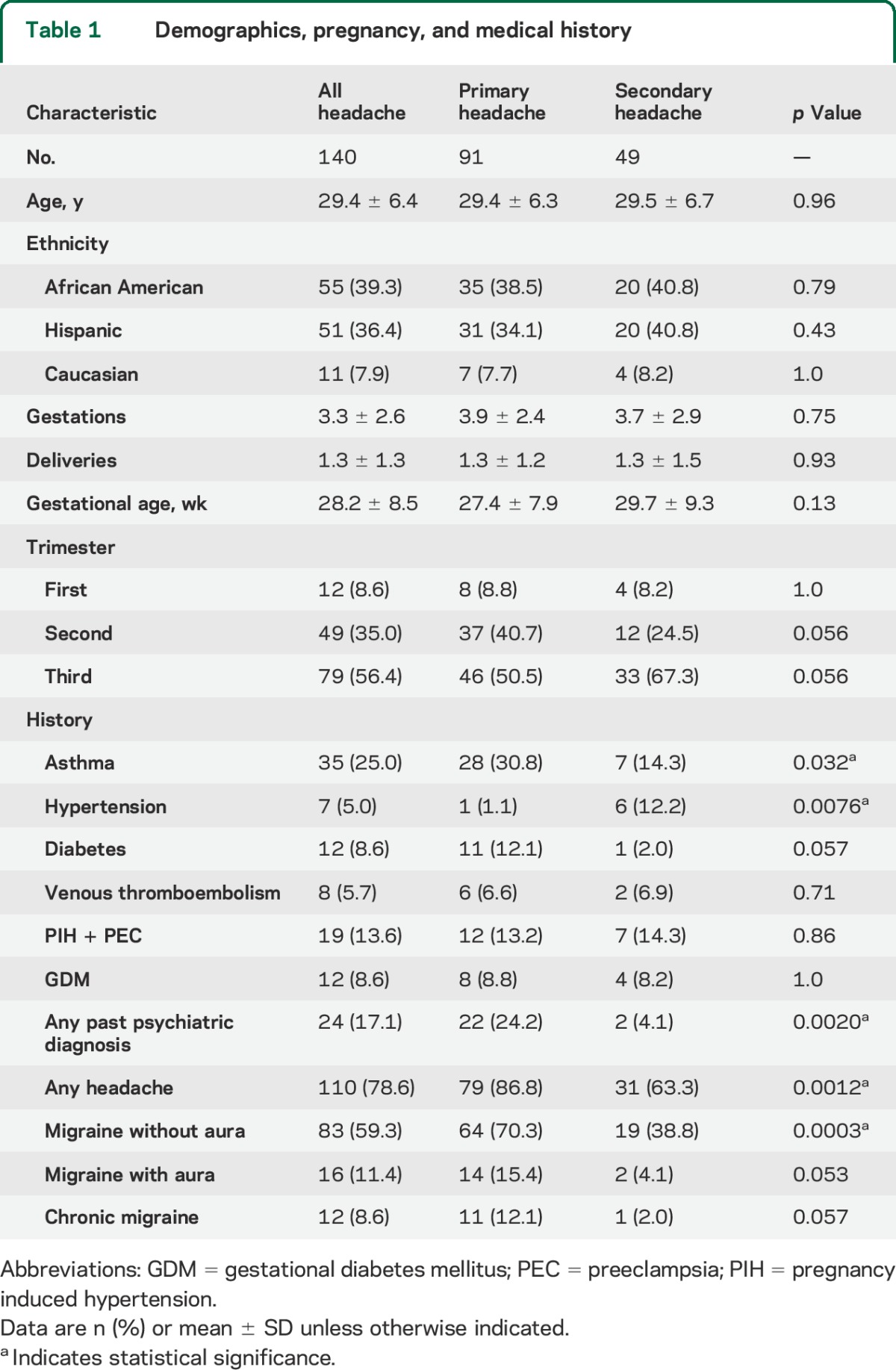
The primary and secondary headache groups did not differ by age, race, or number of prior pregnancies (table 1). A third trimester presentation was the most common (56.4%), particularly for patients with secondary headache (67.3%) vs primary headache (50.5%), but was not significant (p = 0.056). In 3 patients (2.1%), all with secondary headache, the headache presentation led to the discovery of the pregnancy. One patient at gestational week 4 had systemic lupus erythematosus with renal failure and hyperkalemia, the second patient at gestational week 24 had eclampsia with posterior reversible encephalopathy syndrome (PRES) and hemolysis with elevated liver enzymes and low platelet counts (HELLP), and the third patient at gestational week 28 had preeclampsia and HELLP with PRES and reversible cerebral vasoconstriction syndrome.
Table 1.
Demographics, pregnancy, and medical history
Medical history.
Asthma was the most common medical comorbidity overall and was more likely to be present in patients with primary headache (30.8% vs 14.3%, p = 0.032). Psychiatric diagnoses most commonly featured depression (7.9%), anxiety (4.3%), and bipolar disorder (3.6%), and as a group were more common with primary headache (24.2% vs 4.1%, p = 0.0020). Patients with secondary headache were more likely to have nongestational hypertension (12.2% vs 1.1%, p = 0.0076). Rates of prior venous thromboembolism, preeclampsia in a previous pregnancy, gestational hypertension, and diabetes in the current pregnancy were similarly present in primary and secondary headache groups.
Headache history.
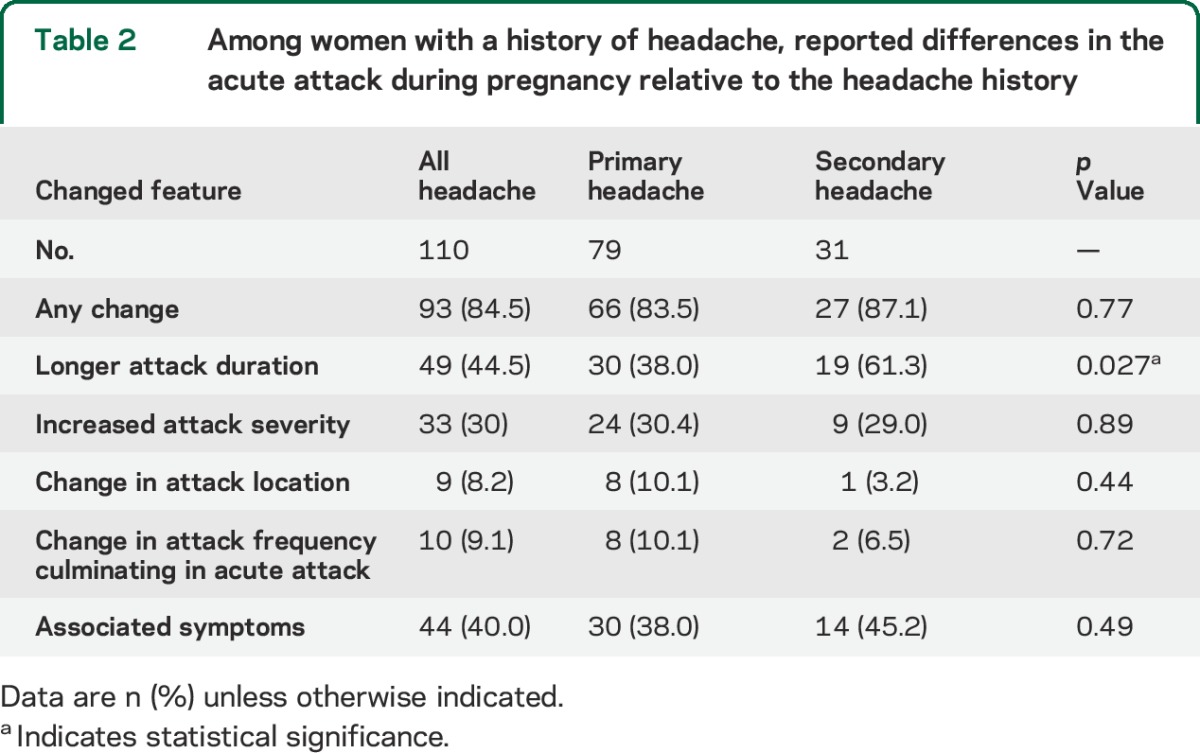
Diagnostic rates of past migraine without aura were 59.3%, migraine with aura 11.4%, and chronic migraine 8.6%. Any history of headache was more common in patients with primary headache (86.8% vs 63.3%, p = 0.0012). In those with a headache history, the patients reported that the acute attack differed from their previous pattern in most cases (84.5%, table 2). The most common difference was longer attack duration (44.5%), presence of associated symptoms including aura (40.0%), increase in severity (30.0%) or frequency (9.1%), or change in headache location (8.2%). In comparison to patients with primary headache, patients with secondary headache were more likely to report prolonged attack duration as their change from past headache (61.3% vs 38.0%, p = 0.027); other differences were not significant.
Table 2.
Among women with a history of headache, reported differences in the acute attack during pregnancy relative to the headache history
Acute headache attack features.
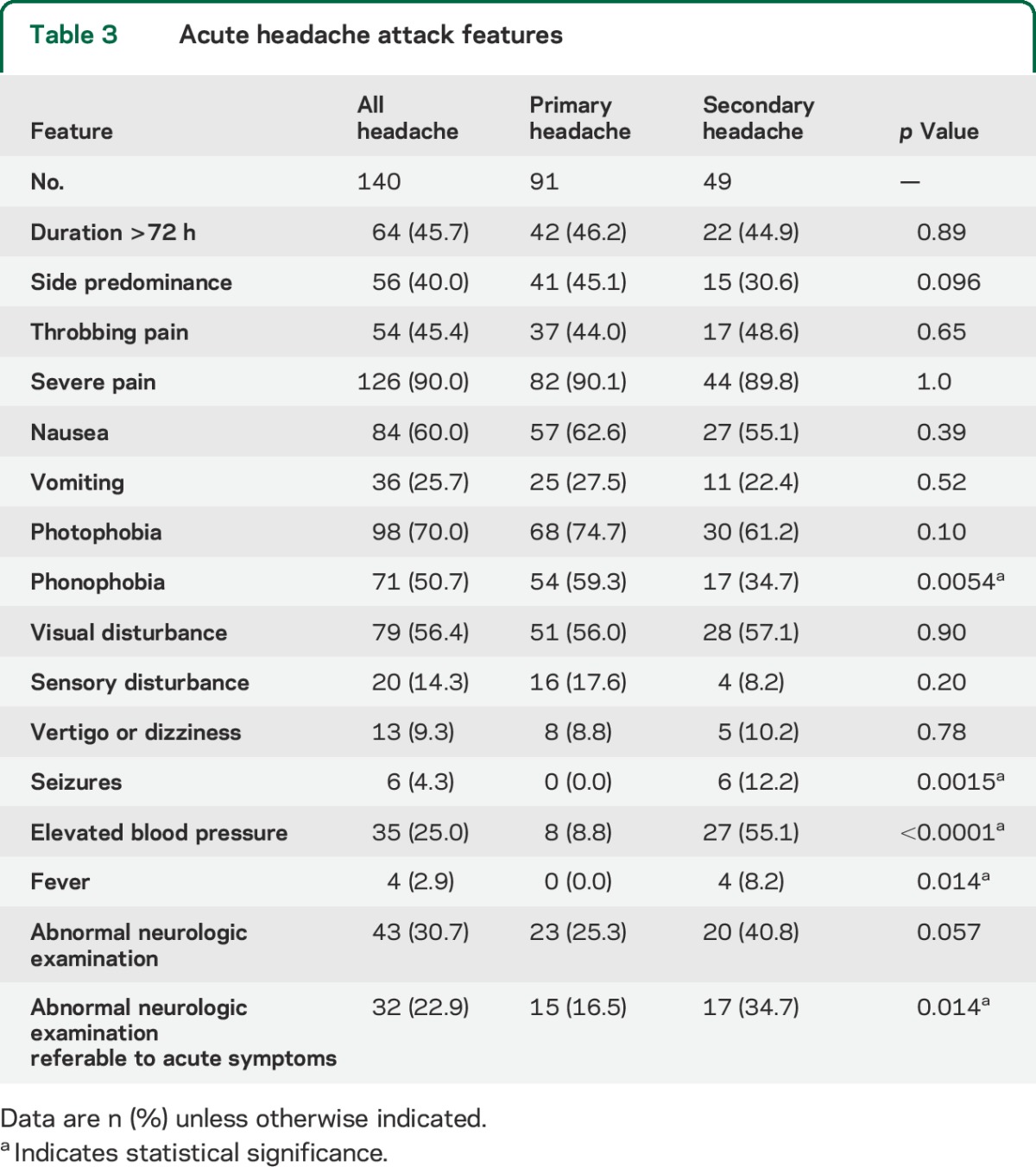
Acute headache duration frequently exceeded 72 hours (table 3), with a location featuring side predominance in 40.0% and throbbing pain in 45.4%, with no differences in patients who had primary or secondary headache. Patients with primary headache were more likely to have phonophobia (59.3% vs 34.7%, p = 0.005) but had similar rates of nausea, vomiting, and photophobia.
Table 3.
Acute headache attack features
Other acute neurologic symptoms.
Visual disturbance was the most common associated neurologic symptom (56.4%), followed by somatosensory disturbance (14.3%) and vertigo or dizziness (9.3%). Seizures were present in 12.2% of patients with secondary headache but none with primary headache (p = 0.0015).
Aura.
Aura was present in 39.6% of the primary headache group. Of those women with aura, 69.4% had no history of aura, and most (86.1%) had neuroimaging to assist in ruling out secondary headache. All but 2 patients (tension-type headache, chronic posttraumatic headache) had migraine with aura. Typical visual aura was present in 91.7%, sensory aura in 38.9%, and brainstem aura in 5.6%. Two patients reported transient, isolated hand clumsiness ipsilateral to their contemporaneous sensory aura. Pregnant women presenting with aura did not differ from those without aura in years of age (30.1 ± 6.7 vs 28.9 ± 6.2, p = 0.40), number of total pregnancies (4.4 ± 2.5 vs 3.5 ± 2.3, p = 0.071), gestational week of presentation (27.7 ± 8.7 vs 27.2 ± 7.5, p = 0.80), a third trimester presentation (52.8% vs 49.1%, p = 0.73), or lack of any headache history (16.7% vs 10.9%, p = 0.43).
Physical examination.
Patients with secondary headache more frequently featured elevated blood pressure (55.1% vs 8.8%, p < 0.0001) and fever (8.2% vs 0.0%, p = 0.014). An abnormal neurologic examination was more likely to be encountered in patients with secondary headache (40.8% vs 25.3%, p = 0.057), which became significant (34.7% vs 16.5%, p = 0.014) when only findings related to the acute symptomatic presentation were included.
Diagnostic tests.
Some form of neuroimaging was performed in 87.9% of the sample, including brain MRI (78.6%), magnetic resonance venography of the head (59.3%), magnetic resonance angiography of the head (53.6%), head CT (14.3%), magnetic resonance angiography of the neck (9.3%), and cervical spine MRI (2.1%). Lumbar puncture was performed in 3.6%. Of the 118 patients who had neuroimaging, 55.9% had normal studies, 26.3% had findings thought to be incidental or unrelated to the acute headache presentation, and 17.8% had abnormal findings that led to secondary headache diagnoses (figure). The most common incidental findings were a hypoplastic transverse venous sinus (n = 13), small subcortical white matter hyperintensities (n = 8), low-lying cerebellar tonsils <5 mm (n = 3), unruptured intracranial aneurysm (n = 2), infundibulum (n = 2), and enlarged pituitary gland without adenoma or hemorrhage (n = 2). In the group with hypertensive disorders of pregnancy, patients had no imaging (12.0%), normal imaging (36.0%), an incidental or unrelated imaging finding (28.0%), or imaging revealing PRES in isolation (20.0%) or PRES with reversible cerebral vasoconstriction syndrome (4.0%).
Variables independently associated with secondary headache.
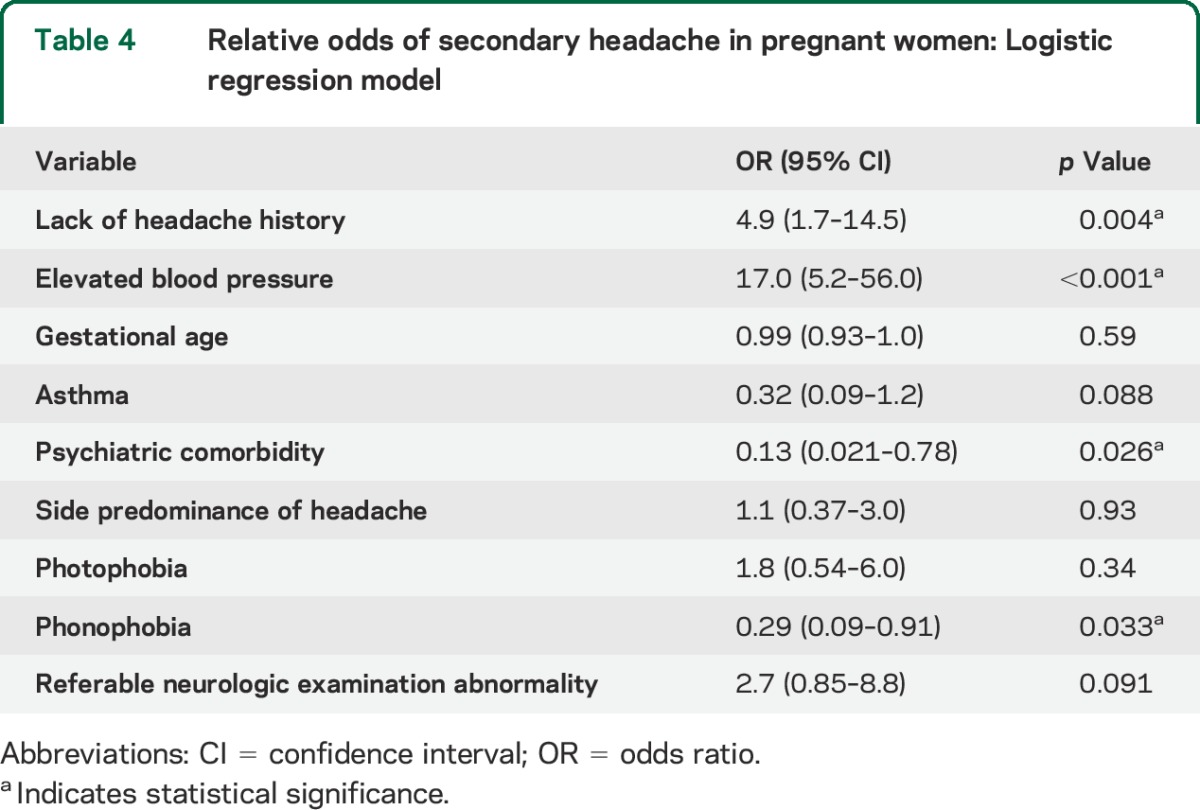
Using binomial logistic regression, we modeled the independent associations of select demographic and clinical variables (tables 1 and 3) with secondary headache (table 4). Secondary headaches were associated with blood pressure elevation and lack of a history of primary headaches. Primary headaches were more likely in persons with psychiatric comorbidity and phonophobia. A referable neurologic examination abnormality did not independently predict secondary headache. We did not assess for the independent effects of fever or seizures since none of the patients in the primary headache group had these potential associated factors.
Table 4.
Relative odds of secondary headache in pregnant women: Logistic regression model
DISCUSSION
We reviewed all neurologic consultations over a 5-year period for acute headache in a mostly African American and Hispanic population of pregnant women, yielding rates of primary headache at 65.0% and secondary headache at 35.0%. A third trimester presentation was typical. Pregnant women with secondary headache were more likely to lack a history of headaches and to present with seizures, high blood pressure, fever, and an abnormal neurologic examination, all established red flags in headache diagnosis.20 The presence of hypertension conferred the greatest independent association with secondary headache, likely driven by preeclampsia and related disorders. The lack of headache history also conferred a strong independent risk. A referable abnormal neurologic examination was more often present in patients with secondary headache but was not an independent risk factor, in part because of frequent sensory abnormalities occurring in migraine with aura. In addition, neurologic abnormalities are likely associated with elevated blood pressure and headache history, reducing their influence in the final model. The presence of a psychiatric diagnosis was independently associated with a primary headache diagnosis, which was expected given the established psychiatric comorbidity of migraine.1
Aside from a lack of phonophobia and a self-report of increased headache duration relative to past headache, secondary headache features did not differ from those of primary headache. A diverse set of headache diagnoses was captured, although migraine and preeclampsia were most frequently encountered. Because more than one-third had a secondary headache disorder, and nearly one-fifth of patients had abnormal neuroimaging that led to the diagnosis, a low threshold for neuroimaging may be justified. In addition, since the headache and related symptoms of preeclampsia and migraine may overlap, close follow-up with monitoring for signs of preeclampsia is also reasonable.
Our study can be compared to 2 other investigations of acute headache in pregnancy. Ramchandren et al.16 reviewed 63 pregnant women presenting to an emergency department with headache, two-thirds of whom received neurologic consultation and all had neuroimaging, yielding 26.9% with secondary headache. An abnormal neurologic examination was more common in patients with secondary headache, but this did not reach significance. Semere et al.17 reviewed 60 pregnant women mostly seen in acute care settings referred for neuroimaging during pregnancy, including 42 receiving neurologic consultation. The mean gestational age (27 weeks) and rate of third trimester presentation (53%) was similar to our study, and 14.3% of those with headache had secondary headache.
Melhado et al.3 conducted a large prospective study of 1,029 pregnant women in a variety of obstetrical settings, also utilizing International Headache Society classification.21 Although they did not focus on acute severe headache, a subgroup of 76 women experienced new-onset or a new type of headache in pregnancy, of whom 52.6% had secondary headache. As in our study, the most common diagnoses were migraine (34.2%) and headache attributed to hypertension (32.9%).
Nearly a quarter of the patients in our study did not have a history of headache, and the remainder of the patients reported a change in their preexisting headache pattern or symptomatology. These factors may have led our pregnant patients to seek care in the acute hospital setting. Even if previously diagnosed with migraine, patients who seek acute care in the emergency department may have more severe and prolonged headache attacks, diagnostic uncertainty, and a lack of access to headache care in the outpatient setting.22 Our patients may have had similar motivations for seeking acute care, and particularly for pregnant patients with headache, our study demonstrates that this is an important issue for resource utilization, as the overwhelming majority of patients were referred for urgent neuroimaging, particularly MRI, as CT is typically avoided because of radiation exposure.23 In addition, safe treatment of headache during pregnancy is an unmet need by established medical therapies,24,25 which may also yield a higher rate of presentation to the acute care setting.
Our study is also a reminder that screening for pregnancy with directed questioning or urine or serum testing26 is important for any woman of childbearing age presenting with acute headache, as the pregnancy status influences diagnostic and therapeutic approaches. The 3 patients presenting with undiagnosed headache in our study all had secondary headache diagnoses with elevated morbidity and mortality requiring immediate management.
The strengths of our study include the large sample size, high amount of clinical detail, utilization of the ICHD-3 beta for diagnosis, high rates of neuroimaging for diagnostic certainty, and the diverse diagnoses captured. Our sample may be representative of some urban hospital-based neurologic consultation clinical practice settings for acute headache in pregnancy in the United States. The main limitations are the retrospective review of records and a lack of generalizability to a general obstetrical or outpatient neurology practice setting. The high rates of African American and Hispanic women may have influenced rates of preeclampsia.27 Routine cases of primary headache easily treated with first line acute therapies or typical preeclampsia may not have been referred for neurologic consultation, leading to our sample including more atypical and severe clinical presentations. We also did not assess for regular prenatal care, which may be suboptimal in an underserved urban population and influence diagnostic rates in acute care. Prospective studies to better capture the general obstetrical population and pregnancy outcomes are indicated.
GLOSSARY
- CI
confidence interval
- HELLP
hemolysis, elevated liver enzymes, and low platelet count
- ICHD-3 beta
International Classification of Headache Disorders, 3rd edition (beta version)
- OR
odds ratio
- PRES
posterior reversible encephalopathy syndrome
AUTHOR CONTRIBUTIONS
Dr. Robbins conceived and designed the study, acquired, analyzed, and interpreted the data, conducted the statistical analysis, drafted, revised, and gave final approval to the manuscript. Dr. Farmakidis acquired, analyzed, and interpreted the data, revised and gave final approval to the manuscript. Drs. Dayal and Lipton interpreted the data, revised and gave final approval to the manuscript.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
M. Robbins serves on the editorial board for Headache, and is a section editor for Current Pain and Headache Reports. He has received royalties for educational activities with the American Headache Society, American College of Physicians, Prova Education, SUNY Downstate, and North Shore-LIJ Hofstra School of Medicine, and book royalties for Headache (Neurology in Practice series) from Wiley. C. Farmakidis and A. Dayal report no disclosures relevant to the manuscript. R. Lipton has received research support from the NIH (PO1 AG03949 [program director, project and core leader], RO1AG025119 [investigator], RO1AG022374-06A2 [investigator], RO1AG034119 [investigator], RO1AG12101 [investigator], K23AG030857 [mentor]), the National Headache Foundation, and the Migraine Research Foundation. He serves on the editorial board of Neurology®, has reviewed for the NIA and National Institute of Neurological Disorders and Stroke, holds stock options in eNeura Therapeutics; serves as a consultant, advisory board member, or has received honoraria from Allergan, the American Headache Society, Autonomic Technologies, Boehringer Ingelheim Pharmaceuticals, Boston Scientific, Bristol-Myers Squibb, CogniMed, CoLucid, Eli Lilly, Endo, eNeura Therapeutics, GlaxoSmithKline, Merck, Novartis, NuPathe, Pfizer, and Vedanta Research. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Robbins MS, Lipton RB. The epidemiology of primary headache disorders. Semin Neurol 2010;30:107–119. [DOI] [PubMed] [Google Scholar]
- 2.Zacur HA. Hormonal changes throughout life in women. Headache 2006;46(suppl 2):S49–S54. [DOI] [PubMed] [Google Scholar]
- 3.Melhado EM, Maciel JA, Jr, Guerreiro CA. Headache during gestation: evaluation of 1101 women. Can J Neurol Sci 2007;34:187–192. [DOI] [PubMed] [Google Scholar]
- 4.Granella F, Sances G, Zanferrari C, Costa A, Martignoni E, Manzoni GC. Migraine without aura and reproductive life events: a clinical epidemiological study in 1300 women. Headache 1993;33:385–389. [DOI] [PubMed] [Google Scholar]
- 5.Scharff L, Marcus DA, Turk DC. Headache during pregnancy and in the postpartum: a prospective study. Headache 1997;37:203–210. [DOI] [PubMed] [Google Scholar]
- 6.Marcus DA, Scharff L, Turk D. Longitudinal prospective study of headache during pregnancy and postpartum. Headache 1999;39:625–632. [DOI] [PubMed] [Google Scholar]
- 7.Granella F, Sances G, Pucci E, Nappi RE, Ghiotto N, Napp G. Migraine with aura and reproductive life events: a case control study. Cephalalgia 2000;20:701–707. [DOI] [PubMed] [Google Scholar]
- 8.Sances G, Granella F, Nappi RE, et al. Course of migraine during pregnancy and postpartum: a prospective study. Cephalalgia 2003;23:197–205. [DOI] [PubMed] [Google Scholar]
- 9.Manzoni GC, Farina S, Granella F, Alfieri M, Bisi M. Classic and common migraine suggestive clinical evidence of two separate entities. Funct Neurol 1986;1:112–122. [PubMed] [Google Scholar]
- 10.Russell MB, Rasmussen BK, Fenger K, Olesen J. Migraine without aura and migraine with aura are distinct clinical entities: a study of four hundred and eighty-four male and female migraineurs from the general population. Cephalalgia 1996;16:239–245. [DOI] [PubMed] [Google Scholar]
- 11.Lipton RB, Silberstein SD, Dodick D. Overview of diagnosis and classification. In: Silberstein SD, Lipton RB, Dodick D, editors. Wolff's Headache and Other Head Pain, 8th ed Oxford, UK: Oxford University Press; 2008:29–43. [Google Scholar]
- 12.Contag SA, Mertz HL, Bushnell CD. Migraine during pregnancy: is it more than a headache? Nat Rev Neurol 2009;5:449–456. [DOI] [PubMed] [Google Scholar]
- 13.De Luca GC, Bartleson JD. When and how to investigate the patient with headache. Semin Neurol 2010;30:131–144. [DOI] [PubMed] [Google Scholar]
- 14.Von Wald T, Walling AD. Headache during pregnancy. Obstet Gynecol Surv 2002;57:179–185. [DOI] [PubMed] [Google Scholar]
- 15.Martin SR, Foley MR. Approach to the pregnant patient with headache. Clin Obstet Gynecol 2005;48:2–11. [DOI] [PubMed] [Google Scholar]
- 16.Ramchandren S, Cross BJ, Liebeskind DS. Emergent headaches during pregnancy: correlation between neurologic examination and neuroimaging. AJNR Am J Neuroradiol 2007;28:1085–1087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Semere LG, McElrath TF, Klein AM. Neuroimaging in pregnancy: a review of clinical indications and obstetric outcomes. J Matern Fetal Neonatal Med 2013;26:1371–1379. [DOI] [PubMed] [Google Scholar]
- 18.Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013;33:629–808. [DOI] [PubMed] [Google Scholar]
- 19.Reddi S, Honchar V, Robbins MS. Peripartum pneumocephalus associated with epidural anesthesia for labor. Neurology 2014;82:P5.207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dodick DW. Pearls: headache. Semin Neurol 2010;30:74–81. [DOI] [PubMed] [Google Scholar]
- 21.Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004;24(suppl 1):9–160. [DOI] [PubMed] [Google Scholar]
- 22.Minen MT, Loder E, Friedman B. Factors associated with emergency department visits for migraine: an observational study. Headache 2014;54:1611–1618. [DOI] [PubMed] [Google Scholar]
- 23.ACOG Committee on Obstetric Practice. ACOG Committee Opinion. Number 299, September 2004 (replaces No. 158, September 1995). Guidelines for diagnostic imaging during pregnancy. Obstet Gynecol 2004;104:647–651. [DOI] [PubMed] [Google Scholar]
- 24.Lucas S. Medication use in the treatment of migraine during pregnancy and lactation. Curr Pain Headache Rep 2009;13:392–398. [DOI] [PubMed] [Google Scholar]
- 25.Govindappagari S, Grossman TB, Dayal AK, Grosberg BM, Vollbracht S, Robbins MS. Peripheral nerve blocks in the treatment of migraine in pregnancy. Obstet Gynecol 2014;124:1169–1174. [DOI] [PubMed] [Google Scholar]
- 26.Strote J, Chen G. Patient self assessment of pregnancy status in the emergency department. Emerg Med J 2006;23:554–557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Caughey AB, Stotland NE, Washington AE, Escobar GJ. Maternal ethnicity, paternal ethnicity, and parental ethnic discordance: predictors of preeclampsia. Obstet Gynecol 2005;106:156–161. [DOI] [PubMed] [Google Scholar]