

Abstract
Objective
Exposure to secondhand smoke (SHS) from burning tobacco products causes disease and premature death among non-smoking adults and children. The objective of this study was to determine the nature, extent and demographic correlates of SHS exposure among adults in low- and middle-income countries with a high burden of tobacco use.
Methods
Data were obtained from the Global Adult Tobacco Survey (GATS), a nationally representative household survey of individuals 15 years of age or older. Interviews were conducted during 2008–2010 in Bangladesh, Brazil, China, Egypt, India, Mexico, the Philippines, Poland, Russia, Thailand, Turkey, Ukraine, Uruguay and Vietnam. Descriptive statistics were used to determine the prevalence and correlates of SHS exposure in homes, workplaces, government buildings, restaurants, public transportation and healthcare facilities.
Results
Exposure to SHS in the home ranged from 17.3% (Mexico) to 73.1% (Vietnam). Among those who work in an indoor area outside the home, SHS exposure in the workplace ranged from 16.5% (Uruguay) to 63.3% (China). Exposure to SHS ranged from 6.9% (Uruguay) to 72.7% (Egypt) in government buildings, 4.4% (Uruguay) to 88.5% (China) in restaurants, 5.4% (Uruguay) to 79.6% (Egypt) on public transportation, and 3.8% (Uruguay) to 49.2% (Egypt) in healthcare facilities.
Conclusions
A large proportion of adults living in low-and middle-income countries are exposed to SHS in their homes, workplaces, and other public places. Countries can enact and enforce legislation requiring 100% smoke-free public places and workplaces, and can also conduct educational initiatives to reduce SHS exposure in homes.
Introduction
Secondhand smoke (SHS) is the combination of smoke emitted from the burning end of a cigarette or other smoked tobacco products and the smoke exhaled from the lungs of smokers.1,2 SHS is involuntarily inhaled by non-smokers, can linger in the air for hours after smoked tobacco products have been extinguished, and contains at least 250 chemicals which are known to be toxic to humans.3 The International Agency for Research on Cancer, the WHO and the US Surgeon General have all concluded that exposure to SHS causes disease and premature death among non-smokers.2,4
Article 8 of the WHO Framework Convention on Tobacco Control (FCTC) calls on ratifying nations to adopt measures that provide universal protection from SHS.5 As a result, governments worldwide are increasingly implementing smoke-free laws that prohibit smoking in all indoor public places and workplaces, including restaurants and bars.5 In 2004, an estimated 40% of children, 33% of non-smoking men, and 35% of non-smoking women worldwide were exposed to SHS.6 This exposure is estimated to have caused a total of 602 300 deaths and 10.9 million lost disability-adjusted life years (DALYs).6
Few studies have examined cross-country variations in population-level SHS exposure.7–10 Data from the 1999–2005 Global Youth Tobacco Survey, which was comprised of students aged 13 years to 15 years old from 132 different countries, found that nearly 56% of respondents were exposed to SHS in any public place, with prevalence ranging from 46.3% in the African and eastern Mediterranean regions to 84.8% in the European region.7 Similar variation was observed with regard to SHS exposure in the home, with prevalence ranging from 30.4% in the African region to 78.0% in the European region. Data from the 2005–2009 Global Health Professions Student Survey also show cross-country variations in SHS exposure in both public places and the home among medical, dental and nursing students from nearly 50 countries.8–10 However, the extent of SHS exposure among the general population of adults, particularly in low- and middle-income countries, is less certain.
For the first time, the Global Adult Tobacco Survey (GATS) provides nationally representative and comparable estimates of SHS exposure among adults in low- and middle-income countries. A better understanding of the nature and extent of SHS exposure can help inform the development and/or refinement of national smoke-free policies. The present study utilises GATS data to assess the self-reported prevalence of SHS exposure in homes, workplaces, government buildings, restaurants, public transportation and healthcare facilities among nationally representative samples of adults from Bangladesh, Brazil, China, Egypt, India, Mexico, Poland, the Philippines, Russia, Thailand, Turkey, Ukraine, Uruguay and Vietnam.
Methods
GATS
GATS is a nationally representative household survey designed to monitor key tobacco control indicators.11 During 2008–2010, GATS was conducted in each of the following 14 countries: Bangladesh (2009; sample size (n)=9629), Brazil (2008; n=39 425), China (2010; n=13 354), Egypt (2009; n=20 924), India (2009–2010; n=69 296), Mexico (2009; n=13 617), the Philippines (2009; n=9701), Poland (2009–2010; n=7840), Russia (2009; n=11 406), Thailand (2009; n=20 566), Turkey (2008; n=9030), Ukraine (2010; n=8158), Uruguay (2009; n=5581), and Vietnam (2010; n=9925).
The target population of GATS includes all non-institutionalised men and women 15 years of age or older who consider the country to be their primary place of residence. In each country, a multistage cluster sample design was employed, with households selected proportional to population size. At each address in the sample, field interviewers administered the household questionnaire using an electronic data collection device to determine household eligibility and to identify a list of all household members. Once the roster of eligible household members was identified, one person was randomly selected to complete the individual questionnaire, which asks questions about background characteristics, tobacco smoking, smokeless tobacco use, cessation, SHS exposure, tobacco purchase patterns and price, exposure to pro- and antitobacco media, and knowledge, attitudes and perceptions about tobacco. Interviews were conducted privately. In countries where culturally appropriate (ie, Bangladesh, Egypt, and India), same-sex interviews were conducted. Overall response rates for GATS ranged from 65.1% in Poland to 97.7% in Russia.12
Measures
SHS exposure in the home
Exposure to SHS in the home was assessed among all respondents within each country using the question, ‘How often does anyone smoke inside your home? Would you say daily, weekly, monthly, less than monthly, or never?’ Respondents who indicated ‘daily’, ‘weekly’, or ‘monthly’ were classified as exposed to SHS in the home.
SHS exposure in the workplace
Exposure to SHS in the workplace was assessed among respondents within each country who reported working outside the home, either indoors or both indoors and outdoors, using the question, ‘During the past 30 days, did anyone smoke in indoor areas where you work?’ Respondents who indicated ‘yes’ were classified as exposed to SHS in the workplace.
SHS exposure in other public places
GATS questionnaire contains separate questions on SHS exposure in four public places: government buildings, healthcare facilities, public transportation and restaurants. Respondents were first asked whether they had visited each location in the past 30 days. Among those who indicated ‘yes’, exposure to SHS was assessed using the following questions, ‘Did anyone smoke inside of any (government buildings or government offices/healthcare facilities/public transportation/restaurants) that you (visited/used) during the past 30 days?’ Respondents who indicated ‘yes’ were classified as exposed to SHS in each public place. In China, exposure in healthcare facilities was assessed separately for three different facility types, including ‘private or village clinic’, ‘township or community health services centre’, and ‘any other healthcare facility’. Respondents who indicated ‘yes’ to any one of these three questions were classified as exposed to SHS in a healthcare facility.
Respondent characteristics
Smoking status was determined using the question, ‘Do you currently smoke tobacco on a daily basis, less than daily, or not at all?’ Respondents who indicated ‘not at all’ were classified as non-smokers, while those who indicated ‘daily’ or ‘less than daily’ were classified as smokers. Sociodemographic characteristics assessed within each country included sex (male or female) and age (15–24, 25–64 and ≥65 years).
Data analysis
All estimates and 95% CIs were calculated on weighted data using SPSS V.18, which estimated variances while accounting for the clustered sample design. For each country, prevalence of SHS exposure was calculated overall and among non-smokers by age and sex when sample size permitted. Differences in response estimates were considered statistically significant if 95% CIs did not overlap. Estimates were not presented when the sample size for any subpopulation was less than 25 cases.
Results
SHS exposure in the home
Among all respondents, exposure to SHS in the home was 54.9% in Bangladesh, 27.9% in Brazil, 67.3% in China, 62.5% in Egypt, 40.0% in India, 17.3% in Mexico, 54.4% in the Philippines, 44.2% in Poland, 34.7% in Russia, 33.2% in Thailand, 56.3% in Turkey, 23.5% in Ukraine, 34.0% in Uruguay, and 73.1% in Vietnam (data not shown). By sex, home SHS exposure ranged between 17.2% (Mexico) and 77.2% (Vietnam) among males, and between 17.4% (Mexico) and 69.2% (Vietnam) among females. In six out of the 14 countries, SHS exposure in the home was significantly greater among males than females (Bangladesh, Brazil, Philippines, Thailand, Uruguay and Vietnam). Exposure generally decreased with increasing age, with both males and females ≥65 years of age showing the lowest prevalence (table 1).
Table 1. Percent of adults exposed to secondhand smoke in the home, overall and among non-smokers by sex and age—Global Adult Tobacco Use Survey (GATS).
| % (95% CI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| GATS | Males (age in years) | Females (age in years) | |||||||
|
|
|
||||||||
| Country | Year | 15–24 | 25–64 | ≥65 | Overall | 15–24 | 25–64 | ≥65 | Overall |
| All respondents | |||||||||
| Bangladesh | 2009 | 55.4 (50.3 to 60.4) | 59.4 (56.4 to 62.3) | 58.6 (50.6 to 66.1) | 58.2 (55.4 to 61.0) | 50.3 (46.0 to 54.6) | 52.7 (50.1 to 55.3) | 47.2 (39.6 to 55.0) | 51.7 (49.3 to 54.0) |
| Brazil | 2008 | 32.6 (30.7 to 34.6) | 27.7 (26.6 to 28.8) | 27.8 (25.4 to 30.4) | 28.9 (28.0 to 29.9) | 30.4 (28.6 to 32.3) | 26.2 (25.3 to 27.2) | 25.2 (23.2 to 27.3) | 27.0 (26.2 to 27.9) |
| China | 2010 | 74.1 (67.6 to 79.7) | 70.7 (67.1 to 74.0) | 61.0 (55.0 to 66.7) | 70.5 (67.0 to 73.9) | 64.6 (57.6 to 71.0) | 64.4 (61.7 to 67.1) | 58.7 (53.0 to 64.1) | 63.9 (60.6 to 67.0) |
| Egypt | 2009 | 63.4 (60.4 to 66.4) | 60.7 (59.1 to 62.2) | 56.3 (51.4 to 61.0) | 61.3 (59.8 to 62.8) | 66.7 (64.1 to 69.3) | 63.4 (61.8 to 65.0) | 50.1 (45.7 to 54.6) | 63.8 (62.3 to 65.3) |
| India | 2009/10 | 40.8 (38.3 to 43.3) | 40.6 (38.9 to 42.3) | 41.2 (38.2 to 44.2) | 40.7 (39.0 to 42.3) | 39.2 (36.9 to 41.6) | 39.5 (37.8 to 41.1) | 38.2 (34.8 to 41.7) | 39.3 (37.7 to 40.9) |
| Mexico | 2009 | 17.9 (14.7 to 21.7) | 17.1 (14.8 to 19.7) | 15.6 (12.1 to 19.9) | 17.2 (15.0 to 19.7) | 19.9 (17.2 to 22.8) | 16.9 (14.8 to 19.2) | 13.4 (10.4 to 17.1) | 17.4 (15.6 to 19.4) |
| Philippines | 2009 | 57.1 (53.2 to 60.9) | 58.7 (56.2 to 61.1) | 56.2 (49.3 to 62.8) | 58.1 (55.8 to 60.3) | 49.1 (44.8 to 53.3) | 50.9 (48.4 to 53.5) | 54.0 (47.9 to 60.1) | 50.6 (48.4 to 52.8) |
| Poland | 2009/10 | 46.7 (41.0 to 52.4) | 46.3 (43.7 to 48.9) | 34.9 (29.9 to 40.2) | 44.9 (42.6 to 47.3) | 47.8 (42.3 to 53.5) | 45.9 (43.6 to 48.2) | 32.2 (28.4 to 36.3) | 43.6 (41.6 to 45.6) |
| Russia | 2009 | 35.6 (31.9 to 39.5) | 37.4 (34.8 to 40.0) | 34.2 (29.1 to 39.8) | 36.7 (34.5 to 38.9) | 37.5 (32.9 to 42.2) | 35.1 (32.4 to 37.8) | 22.7 (18.6 to 27.3) | 33.0 (30.7 to 35.3) |
| Thailand | 2009 | 41.3 (35.5 to 47.2) | 36.3 (34.1 to 38.5) | 36.4 (33.0 to 40.0) | 37.3 (35.1 to 39.6) | 33.5 (28.8 to 38.6) | 28.0 (26.3 to 29.8) | 29.5 (25.9 to 33.4) | 29.2 (27.4 to 31.1) |
| Turkey | 2008 | 68.7 (63.6 to 73.5) | 54.3 (51.9 to 56.7) | 36.9 (31.7 to 42.3) | 56.1 (53.8 to 58.4) | 65.0 (60.8 to 69.1) | 56.4 (53.9 to 58.8) | 37.7 (32.5 to 43.1) | 56.5 (54.3 to 58.7) |
| Ukraine | 2010 | 27.4 (22.8 to 32.4) | 26.5 (24.5 to 28.5) | 16.8 (13.6 to 20.6) | 25.4 (23.7 to 27.2) | 27.4 (22.1 to 33.5) | 23.7 (21.7 to 26.0) | 12.3 (10.1 to 14.8) | 21.9 (20.2 to 23.8) |
| Uruguay | 2009 | 49.8 (43.9 to 55.6) | 35.2 (32.0 to 38.5) | 22.6 (17.8 to 28.2) | 36.8 (34.0 to 39.6) | 42.0 (35.7 to 48.5) | 32.6 (29.7 to 35.7) | 18.7 (15.5 to 22.4) | 31.4 (29.1 to 33.9) |
| Vietnam | 2010 | 77.2 (73.1 to 80.9) | 78.4 (76.5 to 80.2) | 66.3 (60.7 to 71.5) | 77.2 (75.5 to 78.9) | 74.6 (70.9 to 78.0) | 68.6 (66.6 to 70.5) | 60.3 (55.7 to 64.7) | 69.2 (67.4 to 71.0) |
| Non-smokers | |||||||||
| Bangladesh | 2009 | 52.9 (47.0 to 57.8) | 36.5 (32.7 to 40.5) | 44.2 (34.9 to 54.0) | 43.8 (40.2 to 47.3) | 50.1 (45.8 to 54.5) | 52.0 (49.3 to 54.6) | 43.5 (35.7 to 51.7) | 50.9 (48.5 to 53.3) |
| Brazil | 2008 | 28.0 (26.1 to 30.1) | 15.5 (14.5 to 16.5) | 18.0 (15.6 to 20.6) | 19.1 (18.2 to 20.1) | 27.7 (25.8 to 29.6) | 18.3 (17.4 to 19.3) | 19.6 (17.6 to 21.7) | 20.7 (19.8 to 21.5) |
| China | 2010 | 64.1 (56.2 to 71.3) | 42.1 (36.3 to 48.2) | 37.9 (30.8 to 45.6) | 48.4 (43.3 to 53.6) | 64.5 (57.4 to 70.9) | 63.9 (61.1 to 66.5) | 56.0 (50.5 to 61.4) | 63.2 (59.9 to 66.4) |
| Egypt | 2009 | 57.5 (53.9 to 61.0) | 40.7 (38.4 to 43.1) | 39.7 (34.0 to 45.6) | 47.7 (45.5 to 49.8) | 66.6 (64.0 to 69.2) | 63.2 (61.5 to 64.7) | 49.5 (45.0 to 54.0) | 63.6 (62.1 to 65.1) |
| India | 2009/10 | 38.5 (36.0 to 41.2) | 26.5 (24.9 to 28.2) | 26.3 (23.1 to 29.7) | 30.8 (29.1 to 32.5) | 39.2 (36.8 to 41.5) | 37.8 (36.2 to 39.5) | 33.5 (30.1 to 37.2) | 37.9 (36.4 to 39.5) |
| Mexico | 2009 | 16.1 (13.0 to 19.7) | 12.4 (10.3 to 14.8) | 10.8 (7.6 to 15.2) | 13.3 (11.3 to 15.5) | 18.2 (15.7 to 21.1) | 13.8 (12.0 to 15.9) | 11.3 (8.3 to 15.2) | 14.8 (13.2 to 16.5) |
| Philippines | 2009 | 46.9 (41.8 to 52.0) | 35.2 (32.0 to 38.5) | 40.0 (32.2 to 48.5) | 39.6 (36.7 to 42.5) | 49.0 (44.7 to 53.3) | 47.4 (44.7 to 50.0) | 45.7 (39.0 to 52.5) | 47.8 (45.4 to 50.1) |
| Poland | 2009/10 | 34.6 (28.5 to 41.3) | 22.4 (20.0 to 25.2) | 21.6 (17.1 to 27.0) | 24.9 (22.6 to 27.3) | 40.9 (34.9 to 47.1) | 28.2 (25.8 to 30.7) | 28.5 (24.7 to 32.7) | 30.4 (28.3 to 32.6) |
| Russia | 2009 | 20.3 (15.9 to 25.5) | 12.6 (10.4 to 15.2) | 15.0 (10.6 to 20.7) | 14.8 (12.9 to 17.0) | 29.1 (23.8 to 35.0) | 24.7 (22.2 to 27.3) | 20.7 (16.6 to 25.4) | 24.3 (22.1 to 26.6) |
| Thailand | 2009 | 30.6 (23.4 to 39.1) | 16.8 (14.9 to 18.9) | 20.6 (17.2 to 24.5) | 20.5 (18.0 to 23.2) | 32.9 (28.1 to 38.0) | 26.8 (25.0 to 28.6) | 26.2 (22.7 to 30.0) | 27.9 (26.1 to 29.8) |
| Turkey | 2008 | 60.6 (53.7 to 67.2) | 34.1 (31.0 to 37.3) | 29.0 (23.5 to 35.2) | 40.4 (37.2 to 43.6) | 62.2 (57.6 to 66.6) | 50.6 (47.8 to 53.3) | 36.3 (31.2 to 41.7) | 51.7 (49.2 to 54.1) |
| Ukraine | 2010 | 15.7 (11.0 to 21.8) | 6.6 (5.2 to 8.4) | 7.4 (4.9 to 11.1) | 8.8 (7.2 to 10.7) | 18.8 (14.2 to 24.5) | 19.0 (17.2 to 21.0) | 12.3 (10.1 to 14.8) | 17.4 (15.9 to 18.9) |
| Uruguay | 2009 | 45.0 (37.7 to 52.5) | 20.5 (17.2 to 24.3) | 13.5 (9.3 to 19.0) | 25.0 (21.9 to 28.3) | 37.9 (30.8 to 45.7) | 21.2 (18.4 to 24.4) | 16.1 (13.1 to 19.6) | 23.0 (20.6 to 25.6) |
| Vietnam | 2010 | 73.7 (68.6 to 78.3) | 61.2 (57.8 to 64.5) | 52.9 (45.6 to 60.1) | 65.2 (62.3 to 67.9) | 74.5 (70.9 to 77.9) | 68.1 (66.0 to 70.0) | 59.2 (54.5 to 63.7) | 68.8 (67.0 to 70.6) |
Among non-smokers, SHS exposure in the home was 48.4% in Bangladesh, 20.0% in Brazil, 58.3% in China, 57.4% in Egypt, 34.7% in India, 14.1% in Mexico, 44.8% in the Philippines, 28.0% in Poland, 21.5% in Russia, 25.3% in Thailand, 47.5% in Turkey, 14.6% in Ukraine, 23.9% in Uruguay and 67.6% in Vietnam (figure 1). By sex, non-smokers' exposure to SHS in the home ranged between 8.8% (Ukraine) and 65.2% (Vietnam) among males, and between 14.8% (Mexico) and 68.8% (Vietnam) among females. With the exception of Brazil, Mexico, Uruguay and Vietnam, non-smokers' exposure to SHS in the home was significantly greater among females than males. Among both males and females, home SHS exposure generally decreased with increasing age (table 1).
Figure 1.
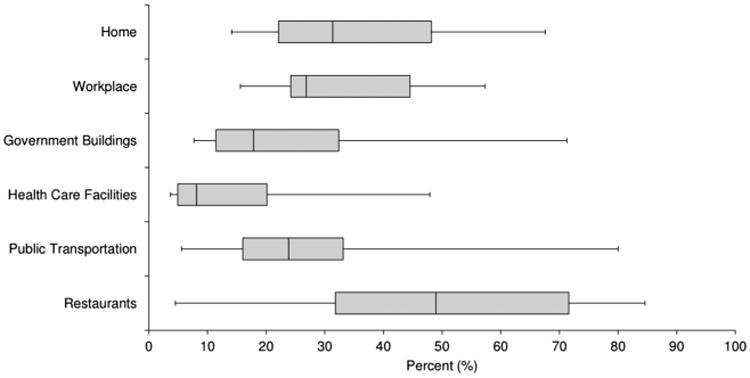
Box and whisker plots of the percentage of non-smokers exposed to secondhand smoke in 14 countries,† by location of exposure—Global Adult Tobacco Survey. †: Bangladesh, Brazil, China, Egypt, India, Mexico, Philippines, Poland, Russia, Thailand, Turkey, Ukraine, Uruguay, Vietnam. Note: Lower, middle, and upper ends of boxes represent 25%, 50% and 75% percentiles, respectively. Whiskers represent minimum and maximum country for each location.
SHS exposure in the workplace
Among all respondents who work in an indoor area outside the home, exposure to SHS in the workplace was 62.2% in Bangladesh, 23.3% in Brazil, 63.3% in China, 59.9% in Egypt, 29.9% in India, 18.6% in Mexico, 32.6% in the Philippines, 33.6% in Poland, 34.9% in Russia, 27.2% in Thailand, 37.3% in Turkey, 33.1% in Ukraine, 16.5% in Uruguay and 55.9% in Vietnam (data not shown). By sex, workplace SHS exposure ranged between 21.4% (Uruguay) and 71.1% (China) among males, and between 11.8% (Uruguay) and 53.6% (Egypt) among females. In every country, workplace SHS exposure was greater among males than females. The only statistically significant differences by age were among men in China and Russia, where workers aged 25–64 years had higher levels of exposure than other age groups (table 2).
Table 2. Percent of adults exposed to secondhand smoke in the workplace overall and among non-smokers,* by sex and age—Global Adult Tobacco Use Survey (GATS).
| % (95% CI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| GATS | Males (age in years) | Females (age in years) | |||||||
|
|
|
||||||||
| Country | Year | 15–24 | 25–64 | ≥65 | Overall | 15–24 | 25–64 | ≥65 | Overall |
| All respondents | |||||||||
| Bangladesh | 2009 | 64.6 (56.3 to 72.0) | 67.9 (63.2 to 72.3) | 61.8 (42.9 to 77.7) | 66.8 (62.4 to 70.9) | 23.6 (12.9 to 39.1) | 34.1 (26.2 to 42.9) | Not calculated† | 30.6 (23.7 to 38.6) |
| Brazil | 2008 | 25.4 (22.3 to 28.7) | 27.0 (25.4 to 28.7) | 37.1 (28.7 to 46.4) | 26.9 (25.4 to 28.4) | 16.9 (14.3 to 19.9) | 20.3 (19.0 to 21.7) | 22.9 (14.7 to 34.0) | 19.7 (18.5 to 20.9) |
| China | 2010 | 51.2 (42.3 to 60.0) | 79.3 (75.7 to 82.4) | 49.6 (27.1 to 72.2) | 71.1 (66.3 to 75.4) | 48.9 (41.7 to 56.1) | 55.3 (48.1 to 62.3) | 26.2 (10.2 to 52.8) | 53.2 (47.7 to 58.6) |
| Egypt | 2009 | 61.0 (54.4 to 67.2) | 62.0 (59.2 to 64.6) | 57.4 (36.7 to 75.8) | 61.7 (59.0 to 64.4) | 55.9 (45.0 to 66.3) | 53.0 (48.9 to 57.0) | Not calculated† | 53.6 (49.5 to 57.6) |
| India | 2009/10 | 31.2 (27.2 to 35.5) | 32.6 (30.6 to 34.7) | 29.3 (22.0 to 37.9) | 32.2 (30.3 to 34.2) | 13.9 (9.9 to 19.2) | 20.6 (17.3 to 24.3) | 39.3 (17.6 to 66.3) | 19.4 (16.4 to 22.7) |
| Mexico | 2009 | 27.5 (21.7 to 34.2) | 20.4 (17.3 to 24.0) | 25.0 (14.1 to 40.4) | 22.2 (19.7 to 24.9) | 14.1 (9.3 to 20.6) | 13.6 (10.7 to 17.1) | Not calculated† | 13.7 (11.1 to 16.7) |
| Philippines | 2009 | 36.6 (28.6 to 45.4) | 38.9 (34.9 to 43.0) | Not Calculated† | 38.8 (35.1 to 42.7) | 24.7 (18.1 to 32.8) | 25.7 (22.2 to 29.6) | 51.5 (31.7 to 70.8) | 26.2 (22.9 to 29.8) |
| Poland | 2009/10 | 43.6 (34.5 to 53.2) | 40.9 (37.8 to 44.0) | Not Calculated† | 41.3 (38.4 to 44.3) | 24.6 (16.2 to 35.5) | 25.1 (22.0 to 28.4) | Not calculated† | 24.9 (22.0 to 28.1) |
| Russia | 2009 | 38.7 (33.5 to 44.2) | 48.2 (44.7 to 51.7) | 27.9 (15.8 to 44.3) | 45.7 (42.5 to 48.9) | 25.4 (20.3 to 31.2) | 25.9 (23.0 to 29.2) | 18.8 (6.7 to 42.8) | 25.7 (22.9 to 28.8) |
| Thailand | 2009 | 40.6 (29.3 to 53.1) | 33.2 (30.1 to 36.4) | 42.9 (27.9 to 59.4) | 34.9 (31.2 to 38.8) | 15.3 (9.8 to 23.0) | 19.8 (17.4 to 22.3) | 13.9 (6.1 to 28.7) | 18.9 (16.8 to 21.2) |
| Turkey | 2008 | 42.7 (34.6 to 51.3) | 39.7 (36.4 to 43.1) | 27.5 (13.8 to 47.3) | 40.1 (36.9 to 43.5) | 32.7 (21.8 to 45.8) | 26.7 (21.9 to 32.2) | Not calculated† | 28.1 (23.4 to 33.4) |
| Ukraine | 2010 | 44.8 (36.1 to 53.7) | 43.3 (40.0 to 46.7) | 40.3 (24.8 to 58.0) | 43.5 (40.3 to 46.7) | 26.4 (17.4 to 37.8) | 22.3 (19.3 to 25.7) | Not calculated† | 22.9 (19.9 to 26.2) |
| Uruguay | 2009 | 20.3 (12.7 to 30.7) | 22.0 (18.1 to 26.5) | 10.4 (3.4 to 27.8) | 21.4 (17.7 to 25.5) | 16.0 (8.7 to to 27.7) | 11.5 (8.8 to 14.9) | 2.4 (0.5 to 9.5) | 11.8 (9.2 to 14.9) |
| Vietnam | 2010 | 65.9 (55.8 to 74.7) | 69.6 (65.7 to 73.3) | Not Calculated† | 68.7 (64.9 to 72.2) | 34.5 (26.4 to 43.6) | 44.1 (39.8 to 48.5) | Not calculated† | 41.4 (37.2 to 45.7) |
| GATS non-smokers | |||||||||
| Bangladesh | 2009 | 62.1 (52.0 to 71.3) | 60.2 (54.2 to 65.9) | 59.5 (38.1 to 77.8) | 60.8 (55.4 to 66.0) | 23.1 (12.5 to 38.7) | 32.8 (25.0 to 41.8) | Not calculated† | 29.6 (22.7 to 37.6) |
| Brazil | 2008 | 24.4 (21.2 to 28.0) | 24.8 (23.2 to 26.6) | 36.2 (27.4 to 46.0) | 25.0 (23.5 to 26.6) | 15.8 (13.2 to 18.9) | 19.3 (17.9 to 20.8) | 24.0 (15.1 to 35.8) | 18.7 (17.4 to 20.0) |
| China | 2010 | 39.3 (29.0 to 50.8) | 70.3 (64.6 to 75.4) | 26.6 (8.8 to 57.7) | 57.5 (51.2 to 63.5) | 49.0 (41.8 to 56.2) | 55.3 (47.6 to 62.6) | 26.2 (10.2 to 52.8) | 53.2 (47.4 to 58.8) |
| Egypt | 2009 | 58.6 (50.3 to 66.4) | 59.4 (55.9 to 62.7) | Not Calculated† | 59.2 (55.9 to 62.3) | 55.9 (45.0 to 66.3) | 52.7 (48.6 to 56.8) | Not calculated† | 53.4 (49.3 to 57.5) |
| India | 2009/10 | 29.0 (25.1 to 33.3) | 27.8 (25.8 to 29.9) | 24.5 (17.1 to 33.8) | 28.1 (26.2 to 30.0) | 13.5 (9.5 to 18.8) | 20.3 (16.9 to 24.0) | 36.3 (13.4 to 67.7) | 18.9 (15.9 to 22.2) |
| Mexico | 2009 | 20.1 (13.6 to 28.7) | 18.7 (15.6 to 22.3) | 27.0 (15.0 to 43.7) | 19.3 (16.7 to 22.2) | 14.1 (9.1 to 21.2) | 13.0 (10.2 to 16.4) | Not calculated† | 13.1 (10.6 to 16.2) |
| Philippines | 2009 | 26.9 (18.4 to 37.5) | 32.1 (27.2 to 37.5) | Not Calculated† | 31.7 (27.2 to 36.6) | 25.1 (18.3 to 33.4) | 25.1 (21.5 to 29.1) | 47.9 (25.0 to 71.7) | 25.7 (22.3 to 29.4) |
| Poland | 2009/10 | 39.2 (28.5 to 51.1) | 32.6 (29.0 to 36.5) | Not Calculated† | 33.8 (30.3 to 37.5) | 19.9 (11.3 to 32.7) | 19.5 (16.7 to 22.8) | Not calculated† | 19.5 (16.8 to 22.5) |
| Russia | 2009 | 27.9 (21.4 to 35.6) | 37.2 (32.7 to 42.0) | 17.1 (7.7 to 33.8) | 34.0 (30.1 to 38.2) | 23.7 (17.9 to 30.8) | 23.5 (20.4 to 26.8) | 18.8 (6.7 to 42.8) | 23.4 (20.5 to 26.7) |
| Thailand | 2009 | 40.1 (25.2 to 57.1) | 28.1 (24.5 to 31.9) | 35.3 (19.0 to 55.9) | 30.8 (26.0 to 36.1) | 15.4 (9.8 to 23.2) | 19.7 (17.3 to 22.3) | 14.9 (6.5 to 30.6) | 18.9 (16.8 to 21.2) |
| Turkey | 2008 | 36.0 (26.0 to 47.4) | 34.9 (30.7 to 39.3) | Not Calculated† | 35.0 (31.0 to 39.2) | 25.1 (13.7 to 41.5) | 21.9 (17.2 to 27.5) | Not calculated† | 22.9 (18.1 to 28.5) |
| Ukraine | 2010 | 38.4 (24.5 to 54.5) | 33.8 (29.4 to 38.5) | 37.3 (19.6 to 59.1) | 34.5 (30.1 to 39.3) | 22.9 (14.3 to 34.5) | 21.1 (18.0 to 24.5) | Not calculated† | 21.4 (18.4 to 24.7) |
| Uruguay | 2009 | 20.0 (11.9 to 31.6) | 20.2 (15.7 to 25.6) | 12.5 (3.9 to 33.6) | 19.9 (15.7 to 24.9) | 15.0 (7.0 to 29.4) | 11.8 (8.6 to 16.0) | 1.7 (0.2 to 11.8) | 11.9 (8.9 to 15.7) |
| Vietnam | 2010 | 65.6 (53.2 to 76.2) | 61.7 (55.6 to 67.4) | Not Calculated† | 62.8 (57.1 to 68.1) | 34.5 (26.4 to 43.6) | 44.0 (39.7 to 48.4) | Not calculated† | 41.3 (37.1 to 45.6) |
Among respondents who reported working in an indoor area outside the home.
Sample size less than 25.
Among non-smokers, SHS exposure in the workplace was 54.6% in Bangladesh, 21.7% in Brazil, 54.9% in China, 57.3% in Egypt, 26.1% in India, 16.4% in Mexico, 28.0% in the Philippines, 26.8% in Poland, 26.9% in Russia, 23.6% in Thailand, 31.1% in Turkey, 26.0% in Ukraine, 15.6% in Uruguay and 49.0% in Vietnam (figure 1). By sex, non-smokers' exposure to SHS in the workplace ranged between 19.3% (Mexico) and 62.8% (Vietnam) among males, and between 11.9% (Uruguay) and 53.4% (Egypt) among females. In every country, except for China, Egypt, the Philippines and Urguay, workplace SHS exposure among non-smokers was greater among males than females. The only statistically significant differences by age were among men in Brazil and China. In Brazil, men aged ≥65 years had higher levels of exposure than those aged 25–64 years. In China, men aged 25–64 years had higher levels of exposure than those aged 15–24 years and ≥65 years (table 2).
SHS exposure in other public places
Overall SHS exposure in government buildings was 43.3% in Bangladesh, 18.0% in Brazil, 58.4% in China, 72.7% in Egypt, 26.2% in India, 17.0% in Mexico, 25.5% in the Philippines, 10.0% in Poland, 17.0% in Russia, 13.0% in Thailand, 11.3% in Turkey, 10.1% in Ukraine, 6.9% in Uruguay and 38.7% in Vietnam (data not shown). By sex, SHS exposure in government buildings ranged between 8.0% (Uruguay) and 75.8% (Egypt) among males, and between 5.8% (Uruguay) and 66.6% (Egypt) among females (table 3). In seven of the 14 countries, exposure to SHS in government buildings was significantly higher among males than females (Bangladesh, Egypt, India, Russia, Turkey, Ukraine, and Vietnam). Among non-smokers, SHS exposure in government buildings ranged from 7.7% (Uruguay) to 71.3% (Egypt) (figure 1).
Table 3. Percent of adults exposed to secondhand smoke in government buildings, healthcare facilities, public transportation, and restaurants overall and among non-smokers, by sex—Global Adult Tobacco Use Survey (GATS).
| % (95% CI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| GATS | Government buildings | Health care facilities | Public transportation | Restaurants | |||||
|
|
|
|
|
||||||
| Year | Country | Males | Females | Males | Females | Males | Females | Males | Females |
| All respondents | |||||||||
| Bangladesh | 2009 | 49.2 (44.8 to 53.7) | 25.2 (18.8 to 33.0) | 31.7 (26.5 to 37.5) | 17.0 (14.2 to 20.3) | 56.9 (53.9 to 59.7) | 47.8 (43.8 to 51.8) | 84.6 (82.4 to 86.7) | 32.8 (25.8 to 40.6) |
| Brazil | 2008 | 18.4 (16.9 to 19.9) | 17.7 (16.3 to 19.2) | 9.6 (8.7 to 10.6) | 10.4 (9.7 to 11.1) | 9.8 (9.0 to 10.7) | 9.2 (8.5 to 10.0) | 32.1 (30.6 to 33.6) | 31.3 (29.8 to 32.8) |
| China | 2010 | 62.6 (55.0 to 69.5) | 50.7 (40.6 to 60.8) | 41.2 (34.7 to 48.1)* | 35.2 (31.0 to 39.6)* | 36.4 (30.1 to 43.1) | 31.5 (26.3 to 37.2) | 91.8 (89.7 to 93.5) | 83.3 (80.1 to 86.2) |
| Egypt | 2009 | 75.8 (73.5 to 77.9) | 66.6 (63.8 to 69.4) | 53.8 (50.9 to 56.7) | 46.4 (44.3 to 48.6) | 80.3 (78.7 to 81.9) | 78.7 (77.1 to 80.2) | 75.6 (73.2 to 77.8) | 62.1 (57.4 to 66.7) |
| India | 2009/10 | 29.4 (27.7 to 31.1) | 18.0 (16.1 to 20.0) | 18.9 (17.3 to 20.5) | 14.6 (13.3 to 16.1) | 36.4 (34.6 to 38.3) | 30.0 (28.1 to 31.9) | 51.1 (49.0 to 53.1) | 32.7 (29.3 to 36.2) |
| Mexico | 2009 | 17.7 (14.8 to 21.1) | 16.0 (12.6 to 20.2) | 5.2 (3.8 to 7.0) | 3.7 (2.8 to 4.9) | 25.4 (23.0 to 27.9) | 23.2 (20.2 to 26.4) | 30.9 (27.4 to 34.7) | 28.1 (25.0 to 31.4) |
| Philippines | 2009 | 27.9 (25.3 to 30.7) | 23.1 (20.6 to 25.9) | 8.0 (6.4 to 10.0) | 7.3 (6.0 to 8.9) | 61.1 (58.6 to 63.5) | 49.7 (47.3 to 52.1) | 38.4 (35.3–41.5) | 28.6 (25.9 to 31.4) |
| Poland | 2009/10 | 10.7 (9.1 to 12.7) | 9.3 (7.6 to 11.5) | 4.3 (3.3 to 5.7) | 4.8 (3.7 to 6.2) | 10.7 (9.0 to 12.7) | 6.6 (5.3 to 8.2) | 52.5 (48.4 to 56.5) | 51.5 (47.1 to 55.9) |
| Russia | 2009 | 21.2 (18.9 to 23.8) | 13.8 (12.0 to 15.8) | 12.1 (9.8 to 14.8) | 9.1 (7.4 to 11.2) | 24.5 (21.9 to 27.2) | 25.1 (22.5 to 28.0) | 78.3 (74.0 to 82.1) | 78.8 (74.0 to 82.9) |
| Thailand | 2009 | 14.4 (12.4 to 16.7) | 11.4 (9.3 to 13.9) | 5.8 (4.6 to 7.2) | 4.2 (3.5 to 5.0) | 22.2 (19.5 to 25.0) | 21.3 (18.7 to 24.1) | 38.7 (35.8 to 41.6) | 29.6 (26.9 to 32.5) |
| Turkey | 2008 | 13.0 (11.2 to 15.1) | 7.8 (5.6 to 10.7) | 6.6 (5.3 to 8.2) | 5.5 (4.5 to 6.7) | 18.7 (16.5 to 21.1) | 14.1 (12.3 to 16.0) | 57.7 (54.8 to 60.5) | 52.3 (48.1 to 56.5) |
| Ukraine | 2010 | 12.9 (10.9 to 15.3) | 8.1 (6.5 to 10.1) | 9.2 (7.0 to 12.2) | 5.3 (4.0 to 7.0) | 17.9 (15.8 to 20.2) | 17.2 (15.3 to 19.3) | 65.7 (61.9 to 69.2) | 62.3 (57.2 to 67.1) |
| Uruguay | 2009 | 8.0 (6.3 to 10.0) | 5.8 (4.2 to 8.0) | 4.2 (2.6 to 6.7) | 3.5 (2.6 to 4.8) | 5.7 (4.4 to 7.4) | 5.2 (4.0 to 6.8) | 4.7 (2.9 to 7.3) | 4.2 (2.6 to 6.7) |
| Vietnam | 2010 | 45.4 (42.0 to 48.8) | 28.4 (25.0 to 32.1) | 29.9 (26.1 to 34.0) | 19.6 (17.1 to 22.4) | 38.8 (34.4 to 43.4) | 29.6 (26.1 to 33.4) | 90.9 (89.0 to 92.4) | 75.2 (72.0 to 78.2) |
| Non-smokers | |||||||||
| Bangladesh | 2009 | 46.2 (40.4 to 52.1) | 224.7 (18.3 to 32.5) | 33.9 (27.6 to 40.8) | 16.9 (14.0 to 20.2) | 58.0 (54.4 to 61.5) | 47.6 (43.5 to 51.7) | 81.7 (78.3 to 84.6) | 32.4 (25.4 to 40.2) |
| Brazil | 2008 | 18.8 (17.2 to 20.5) | 117.8 (16.3 to 19.5) | 9.6 (8.6 to 10.7) | 10.4 (9.7 to 11.2) | 10.4 (9.5 to 11.4) | 9.8 (9.0 to 10.6) | 32.0 (30.5 to 33.7) | 31.2 (29.6 to 32.8) |
| China | 2010 | 60.8 (52.0 to 68.9) | 50.9 (40.7 to 61.1) | 32.3 (26.7 to 38.5)* | 35.2 (30.9 to 39.6)* | 32.2 (25.5 to 39.6) | 31.5 (26.3 to 37.3) | 86.7 (83.1 to 89.7) | 83.1 (79.8 to 85.9) |
| Egypt | 2009 | 75.1 (72.1 to 77.8) | 66.5 (63.7 to 69.3) | 52.0 (48.1 to 55.8) | 46.3 (44.2 to 48.5) | 81.7 (79.7 to 83.5) | 78.7 (77.0 to 80.2) | 72.4 (69.3 to 75.2) | 61.9 (57.2 to 66.5) |
| India | 2009/10 | 28.3 (26.5 to 30.2) | 17.7 (15.8 to 19.7) | 17.6 (16.0 to 19.3) | 14.3 (12.9 to 15.7) | 35.1 (33.2 to 37.0) | 29.6 (27.7 to 31.6) | 49.2 (47.1 to 51.4) | 32.3 (28.9 to 35.9) |
| Mexico | 2009 | 19.2 (15.9 to 23.0) | 15.6 (12.1 to 19.8) | 4.8 (3.4 to 6.8) | 3.7 (2.7 to 4.9) | 24.7 (22.1 to 27.4) | 23.2 (20.3 to 26.4) | 32.8 (28.7 to 37.1) | 28.1 (25.1 to 31.4) |
| Philippines | 2009 | 28.2 (24.8 to 31.9) | 23.2 (20.6 to 26.0) | 8.9 (6.7 to 11.7) | 7.2 (5.9 to 8.8) | 60.6 (57.5 to 63.7) | 49.8 (47.3 to 52.2) | 35.5 (31.8 to 39.3) | 28.3 (25.5 to 31.2) |
| Poland | 2009/10 | 11.4 (9.4 to 13.8) | 8.6 (6.8 to 10.9) | 3.9 (2.8 to 5.5) | 4.4 (3.3 to 5.9) | 9.3 (7.4 to 11.8) | 6.1 (4.7 to 7.8) | 47.9 (42.7 to 53.1) | 47.4 (42.7 to 52.3) |
| Russia | 2009 | 21.4 (18.2 to 25.1) | 12.2 (10.4 to 14.3) | 11.0 (8.1 to 14.7) | 7.8 (6.2 to 9.9) | 23.3 (20.0 to 27.0) | 24.1 (21.4 to 27.1) | 74.2 (67.2 to 80.1) | 71.3 (65.2 to 76.8) |
| Thailand | 2009 | 14.0 (11.4 to 17.1) | 11.4 (9.2 to 13.9) | 5.9 (4.5 to 7.8) | 4.2 (3.5 to 5.0) | 22.1 (18.9 to 25.8) | 21.2 (18.6 to 24.1) | 36.3 (32.7 to 40.1) | 29.8 (27.0 to 32.7) |
| Turkey | 2008 | 13.7 (11.1 to 16.9) | 7.7 (5.3 to 11.2) | 6.8 (5.0 to 9.0) | 5.2 (4.2 to 6.5) | 17.9 (15.3 to 20.9) | 14.2 (12.3 to 16.3) | 51.6 (47.6 to 55.7) | 48.4 (43.3 to 53.5) |
| Ukraine | 2010 | 13.9 (11.3 to 17.1) | 7.3 (5.7 to 9.3) | 9.3 (6.5 to 13.1) | 4.5 (3.3 to 6.1) | 17.4 (14.8 to 20.3) | 16.8 (14.8 to 18.9) | 66.2 (60.8 to 71.3) | 57.0 (51.1 to 62.7) |
| Uruguay | 2009 | 8.7 (6.6 to 11.5) | 6.8 (4.8 to 9.6) | 3.4 (1.9 to 6.0) | 3.8 (2.7 to 5.4) | 6.2 (4.5 to 8.3) | 5.2 (3.8 to 7.1) | 5.1 (3.0 to 8.6) | 4.0 (2.4 to 6.8) |
| Vietnam | 2010 | 42.5 (37.9 to 47.3) | 28.1 (24.7 to 31.8) | 27.1 (22.7 to 32.0) | 19.5 (17.0 to 22.2) | 39.7 (33.6 to 46.1) | 29.5 (26.0 to 33.2) | 87.5 (84.4 to 90.1) | 75.3 (72.0 to 78.3) |
Comparable indicator constructed comprised of exposure in ‘private/village clinic’, ‘township hospital/community health service centre’, or ‘any other healthcare facilities’.
Note: Estimates were calculated among respondents who reported visiting each respective location within the past 30 days.
Overall SHS exposure in healthcare facilities was 23.8% in Bangladesh, 10.1% in Brazil, 37.9% in China, 49.2% in Egypt, 16.8% in India, 4.3% in Mexico, 7.6% in the Philippines, 4.6% in Poland, 10.2% in Russia, 4.8% in Thailand, 6.0% in Turkey, 6.6% in Ukraine, 3.8% in Uruguay and 23.6% in Vietnam (data not shown). By sex, SHS exposure in healthcare facilities ranged between 4.2% (Uruguay) and 53.8% (Egypt) among males, and between 3.5% (Uruguay) and 46.4% (Egypt) among females (table 3). Exposure to SHS in healthcare facilities was higher among males than females in Bangladesh, Egypt, India and Vietnam. Among non-smokers, SHS exposure in healthcare facilities ranged from 3.7% (Uruguay) to 47.9% (Egypt) (figure 1).
Overall SHS exposure on public transportation was 53.6% in Bangladesh, 9.5% in Brazil, 34.1% in China, 79.6% in Egypt, 33.9% in India, 24.2% in Mexico, 55.3% in the Philippines, 8.4% in Poland, 24.9% in Russia, 21.6% in Thailand, 16.5% in Turkey, 17.5% in Ukraine, 5.4% in Uruguay and 34.4% in Vietnam (data not shown). By sex, SHS exposure in public transportation ranged between 5.7% (Uruguay) and 80.3% (Egypt) among males, and between 5.2% (Uruguay) and 78.7% (Egypt) among females (table 3). Exposure to SHS on public transportation was higher among males than females in six of the 14 countries (Bangladesh, India, Philippines, Poland, Turkey and Vietnam). Among non-smokers, SHS exposure on public transportation ranged from 5.6% (Uruguay) to 80.0% (Egypt) (figure 1).
Overall SHS exposure in restaurants was 79.7% in Bangladesh, 31.7% in Brazil, 88.5% in China, 72.7% in Egypt, 47.8% in India, 29.6% in Mexico, 33.6% in the Philippines, 52.0% in Poland, 78.6% in Russia, 34.4% in Thailand, 55.9% in Turkey, 64.1% in Ukraine, 4.4% in Uruguay and 84.9% in Vietnam (data not shown). By sex, SHS exposure in restaurants ranged between 4.7% (Uruguay) and 91.8% (China) among males, and between 4.2% (Uruguay) and 83.3% (China) among females (table 3). Exposure to SHS in restaurants was higher among males than females in seven of the 14 countries (Bangladesh, China, Egypt, India, Philippines, Thailand and Vietnam). Among non-smokers, SHS exposure in restaurants ranged from 4.5% (Uruguay) to 84.6% (China) (figure 1).
Discussion
This study used data from GATS to assess self-reported exposure to SHS in homes, workplaces, government buildings, restaurants, public transportation and healthcare facilities among a nationally representative sample of adults in 14 low- and middle-income countries. The findings indicate that for the majority of the countries assessed, a large proportion of adults are exposed to SHS in their homes, workplaces and other public places. Variations in the prevalence of SHS exposure were also observed across age and sex in most countries. Since there is no risk-free level of SHS, implementing and enforcing comprehensive smoke-free policies in all workplaces and public places, including bars and restaurants, represents the only effective way to fully protect the population from the harmful effects of SHS exposure.2,4 With adequate planning and education, such policies are relatively easy to implement, and achieve high levels of compliance at minimal expense.4,5,13 Accompanying strategies can also be implemented to encourage the voluntary adoption of smoke-free home rules.
Studies suggest that comprehensive smoke-free laws reduce self-reported and objectively measured SHS exposure in the general population of non-smokers.14,15 Comprehensive smoke-free policies have been shown to substantially reduce SHS exposure among non-smoking bar and restaurant workers, as measured by air quality monitoring, self-report, and biomarkers, such as cotinine, a metabolite of nicotine that can be measured in blood, urine or saliva.13,16,17 However, data from Scotland indicate that decreases in SHS exposure among non-smoking adults and youth may be more pronounced in households without smokers, with non-smokers living with smokers experiencing non-significant decreases in exposure.14,15 Accordingly, voluntary smoke-free home rules can further reduce SHS in the general population and help to fully protect all non-smokers from the adverse health effects of SHS exposure. Smoke-free home rules have also been shown to help current smokers quit.4,13,21
The benefits of smoke-free policies have been well documented globally. Data from a growing number of countries and sub-national areas show that the implementation of smoke-free policies improves public health.13,18 More specifically, comprehensive smoke-free policies are associated with reductions in self-reported respiratory symptoms and improved lung function among non-smoking hospitality workers,13,18 as well as reductions in hospitalisations for heart attacks in the general population.19 Additionally, several studies suggest that the implementation of smoke-free policies helps facilitate smoking cessation and the adoption of voluntary smoke-free home rules.4,13,20 Moreover, studies in multiple countries indicate that smoke-free environments are popular among the general public and do not have an adverse economic impact on restaurants and bars.4,5,13,22
Notable progress has recently occurred in enacting smoke-free policies. In 2000, no country had a comprehensive smoke-free law in place that completely eliminated smoking in indoor workplaces and public places.5,13 However, in March 2004, Ireland became the first country to implement a law of this kind.5,13 In the intervening years, many other countries have adopted comprehensive smoke-free laws, driven by the growing evidence on the health risks posed by SHS, the successful experiences of other jurisdictions in implementing smoke-free laws, and the requirements of WHO Framework Convention on Tobacco Control.5,13 Between 2008 and 2010, 16 countries implemented nationwide comprehensive smoke-free legislation, bringing the total number of countries with such laws to 31 and increasing the number of individuals protected by such laws to 739 million, or 11% of the world's population.23 An additional 210 million people, or 3% of the world's population, were protected by comprehensive smoke-free legislation at the subnational level in 2010.23
The prevalence of SHS exposure in workplaces and public places in the present study was lowest in Uruguay, which was the only country with a national comprehensive smoke-free law prohibiting smoking in all workplaces and public places with no exemptions at the time of GATS assessment. This finding aligns with studies showing that comprehensive smoke-free policies lead to marked reductions in population SHS exposure.14,15 Between the time that GATS was conducted and January 2011, both Thailand (2010) and Turkey (2009) subsequently enacted national comprehensive smoke-free laws, while the remaining 11 countries had either no or partial smoke-free laws in place.23
Enhanced efforts by the global tobacco control community have the potential to reduce SHS exposure, particularly among subpopulations where the burden of SHS exposure is greatest.5 In the present study, non-smokers' exposure to SHS in the home was generally higher among females than males, while exposure in the workplace and other public places was higher among males. Moreover, exposure to SHS in the home generally decreased with increasing age among both sexes. These findings may be reflective of variations in the social acceptability of tobacco use across genders and/or the demographic structure of the workforce in each country.24
Based on evidence of the cost-effectiveness, feasibility and popularity of smoke-free laws, the WHO recommends several key measures for protecting workers and the public from SHS exposure. These measures include implementing 100% smoke-free environments with no exemptions, enacting legislation requiring all workplaces and public places to be 100% smoke-free, adequately enforcing smoke-free legislation, and implementing accompanying strategies to reduce SHS exposure in the home.5 In addition, efforts should be made to evaluate and monitor the effects of the aforementioned measures in order to maintain public support, establish best practices and identify factors that may undermine existing smoke-free policies.5
The findings in this report are subject to at least four limitations. First, estimates of SHS exposure were self-reported and not validated by biochemical tests. Research suggest that self-reported surveys of SHS exposure in the home and workplace yield lower estimates of exposure than measurements of serum cotinine, an objective biomarker of nicotine intake.25 Second, in some regions, social norms (eg, unacceptability of women smoking) might result in under-reporting of current smoking behaviours. Misclassification of current smoking status could introduce bias into estimates of SHS exposure calculated among non-smokers. However, the use of same-sex interviewers and private interview settings may have reduced the extent of such under-reporting in the present study. Third, because the employed population tends to be predominantly less than age 65 years, sample size was limited for persons aged 65 years and older for this measure; therefore, analysing or interpreting data on workplace SHS exposure among this subpopulation was not possible in some countries. Finally, slight variations in the number and type of questions used to determine SHS exposure in healthcare facilities in China might limit comparability with findings from the other 13 countries. However, aside from this difference, questions were comparable across the 14 countries included in the analysis.
Conclusion
Findings from GATS suggest that a large proportion of adults who live in the low- and middle-income countries that were analysed in this report are exposed to SHS in their homes, workplaces and other public places. While progress has been made in implementing smoke-free policies, many individuals remain exposed to SHS in these environments. Accordingly, all countries can enact and enforce legislation requiring 100% smoke-free public places and workplaces, and also conduct educational initiatives to reduce SHS exposure in homes. Creating smoke-free environments and educating the public about the dangers of SHS could ultimately have complementary effects on tobacco control efforts by reducing the social acceptability of tobacco use around non-smokers. In addition, ongoing surveillance among both non-smokers and the general population is necessary to evaluate progress toward eliminating SHS exposure, to track the implementation and enforcement of legislation to reduce SHS exposure, and to gauge public support for smoke-free environments.
What this study adds.
Limited data are available on the extent of secondhand smoke (SHS) exposure in indoor environments in low- and middle-income countries with a high burden of tobacco use.
This study used nationally representative data from the Global Adult Tobacco Survey to assess the nature, extent and demographic correlates of SHS exposure among adults in 14 low- and middle-income countries.
The data suggest that a large proportion of adults in these countries are exposed to SHS in their homes, workplaces and other public places.
These findings can help inform the promotion, development and sustainability of smoke-free policies in these countries.
Acknowledgments
The authors gratefully acknowledge Linda Andes and Glenda Blutcher-Nelson from the CDC Office on Smoking and Health, as well as Antonella Cardone from the Global Smoke-Free Partnership, for their assistance with this manuscript. We also thank the numerous members of GATS Collaborating Group for their expertise and contributions. For the full list of GATS collaborating group members, please see the appendix at the end of this article.
Funding Funding for the Global Adult Tobacco Survey (GATS) was provided by the Bloomberg Initiative to Reduce Tobacco Use, a programme of Bloomberg Philanthropies. GATS was cofunded by the Bill and Melinda Gates Foundation in China, by the Brazilian Ministry of Health in Brazil, and by the Ministry of Health and Family Welfare in India. Technical assistance was provided by the Centers for Disease Control and Prevention (CDC), WHO, the Johns Hopkins Bloomberg School of Public Health, and RTI International. Programme support was provided by the CDC Foundation. The authors had full access to all the data in the study and final responsibility to submit the report for publication.
Appendix Gats Collaborating Group
National Collaborating Agencies and Contacts
Bangladesh: (Agencies) Ministry of Health and Family Welfare (MoHFW), National Institute of Preventive & Social Medicine (NIPSOM), Bangladesh Bureau of Statistics, National Institute of Population Research & Training (NIPORT); (Contacts) Md Amirul Hasan (NIPSOM). Brazil: (Agencies) Ministry of Health-Secretariat of Health Surveillance (SVS), Brazilian Institute of Geography & Statistics (IBGE), National Cancer Institute (INCA), The National Health Surveillance Agency (ANVISA); (Contacts) Deborah Carvalho Malta (MoH-SVS), Eduardo Pereira Nunes, Marcia Quintslr, Cimar Azeredo (IBGE), Liz Maria de Almeida (INCA), Humberto Martins (ANVISA). China: (Agencies) Ministry of Health (MoH), Chinese Centers for Disease Control (China CDC); (Contacts) Yang Gonghuan, Yang Yan, Xiao Lin, Li Qiang (China CDC). Egypt: (Agencies) Ministry of Health (MoH), Central Agency for Public Mobilization & Statistics (CAPMAS); (Contacts) Sahar Latif Labib (MoH), Awatef Hussein (CAPMAS). India: (Agencies) Ministry of Health & Family Welfare (MoHFW), Government of India, International Institute for Population Sciences (IIPS); (Contacts) Anuradha Vemuri, Jagdish Kaur (MoHFW), F Ram, Sulabha Parasuraman (IIPS). Mexico: (Agencies) Ministry of Health (MoH), National Institute of Public Health (INSP); (Contacts) Mauricio Hernandez Avila (MoH), Luz Miriam Reynales-Shigematsu (INSP). Philippines: (Agencies) Department of Health (DoH), National Statistics Office (NSO); (Contacts) Agnes Segarra (DoH), Glenn Barcenas, Benedicta Yabut (NSO). Poland: (Agencies) Ministry of Health (MoH), Maria Skłodowska-Curie Cancer Center Institute of Oncology, Medical University of Warsaw, Pentor Research International; (Contacts) Tadeusz Parchimowicz (MoH), Witold Zatonski, Krzysztof Przewozniak (CCI), Filip Raciborski (WMU), Krzysztof Siekierski (Pentor). Russian Federation: (Agencies) Ministry of Health & Social Development (MoHSD), Federal State Statistics of Russia (RosStat), Pulmonary Research Institute (PRI); (Contacts) Maria Shevireva, Natalya Kostenko (MoHSD), Vadim Nesterov, Tamara Chernisheva, Tatiana Konik (RosStat), Galina Sakharova (PRI). Thailand: (Agencies) Ministry of Public Health (MoPH), National Statistical Office (NSO), Tobacco Control Research & Knowledge Management Center (TRC) at Mahidol University; (Contacts) Sarunya Benjakul (MoPH), Lakkhana Termsirikulchai, Mondha Kengganpanich (TRC), Areerat Lohtongmongkol, Hataichanok Puckcharern, Chitrlada Touchchai (NSO). Turkey: (Agencies) Ministry of Health (MoH), Turkish Statistical Institute (TurkStat), Hacetteppe University (HU); (Contacts) Hüseyin İlter (MoH), Enver Tasti, Ramazan Celikkaya, Guzin Erdogan (Turkstat), Nazmi Bilir, Hilal Özcebe (HU). Ukraine: (Agencies) Ministry of Health (MoH), Kiev International Institute of Sociology (KIIS), School of Public Health, National University of Kyiv-Mohyla Academy (SPH); (Contacts) Alla Grygorenko, Konstantin Krasovsky (MoH), Natalia Kharchenko, Volodymyr Paniotto (KIIS), Tatiana Andreeva (SPH). Uruguay: (Agencies) Ministry of Health (MoH), National Statistics Institute (INE); (Contacts) Winston Abascal, Ana Lorenzo (MoH), Franco González Mora (INE). Vietnam: (Agencies) Ministry of Health (MoH), Viet Nam Standing Office on Smoking and Health (VINACOSH), General Statistics Office (GSO), Hanoi Medical University (HMU); (Contacts) PhanThi Hai (MoH), Nguyen The Quan (GSO), Hoang Van Minh (HMU), Kim Bao Giang (HMU).
International Collaborators
World Health Organization (WHO)-Tobacco Free Initiative: (Headquarters) Douglas Bettcher, Lubna Bhatti, Edouard Tursan d'Espaignet, Sameer Pujari, Ayda Yurekli; (AFRO) AE Ogwell Ouma, Nivo Ramanandraibe; (AMRO-PAHO) Adriana Blanco, Roberta de Betania Caixeta; (Brazil) Enrique Gil; (Mexico) Carlos Gamez; (Uruguay) Julio Vignolo; (EMRO) Fatimah El Awa, Heba Fouad; (Egypt) Randa Abou El Naga; (EURO) Kristina Mauer-Stender, Rula Khoury; (Poland) Anna Koziel; (Russian Federation) Luigi Migliorini, Oleg Storozhenko; (Turkey) Toker Ergüder; (Ukraine) Nataliya Korol; (SEARO) Dhirendra N Sinha; (Bangladesh) Sohel Choudhury, M Mostafa Zaman; (India) Vineet Munish Gill; (Thailand) Chai Kritiyapichatkul; (WPRO) Susan Mercado, James Rarick; (China) Sarah England; (Philippines) Marina Miguel-Baquilod; (Vietnam) Pham Thi Quynh Nga, Pham Huyen Khanh. US Centers for Disease Control and Prevention (CDC)-Office on Smoking and Health (OSH): Linda Andes, Samira Asma, Oksana Bilukha, Thomas R Frieden, Glenda Blutcher-Nelson, Peter Edwards, Jason Hsia, Deliana Kostova, Veronica Lea, Juliette Lee, Ronney Lindsey, Timothy McAfee, Sara Mirza, Jeremy Morton, Krishna Palipudi, Terry Pechacek, Dana Shelton, Sophia Song, Charles Warren, Luhua Zhao. CDC Foundation: William Parra, Brandon Talley, Connie Granoff, Michael Green. Johns Hopkins Bloomberg School of Public Health: Joanna Cohen, Rajeev Cherukupalli. RTI International: Jay Levinsohn, Steve Litavecz. Experts & Scientific Advisors: (Questionnaire Review Committee) Benjamin Apelberg, Marina Miguel-Baquilod, Ron Borland, Gary Giovino, Prakash C Gupta, Daniel Ferrante, Mostafa Mohammed; (Sample Review Committee) Michael Bowling, William Kalsbeek, Krishna Palipudi, TK Roy; (Scientific Advisors) Sonia Angell, Neeraj Bhalla, Frank Chaloupka, Prabhat Jha, Sir Richard Peto, Jonathan Samet, Gajalakshmi Vendhan, Witold Zatonski. Bloomberg Philanthropies—Bloomberg Initiative to Reduce Tobacco Use: Kelly Henning, Jennifer Ellis.
Footnotes
Contributors All authors contributed equally to this work. BAK and SAM designed the study, BAK wrote the manuscript, and BAK, SAM and SDB discussed the results and implications and commented on the manuscript at all stages.
Competing interests None.
Ethics approval Institutional review board approval was obtained separately in each of the 14 countries included.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from the Global Adult Tobacco Use Survey (GATS) are publicly available via the Global Tobacco Surveillance System (GTSS) website: http://www.cdc.gov/tobacco/global/gtss/index.htm.
References
- 1.U.S. Department of Health and Human Services. How tobacco smoke causes disease: the biology and behavioral basis for smoking-attributable disease: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2010. [PubMed] [Google Scholar]
- 2.World Health Organization/International Agency for Research on Cancer. Tobacco Smoke and Involuntary Smoking. IARC Monogr Eval Carcinog Risks Hum. 2004;83:1–1438. [PMC free article] [PubMed] [Google Scholar]
- 3.U.S. Department of Health and Human Services. Report on carcinogens. 11th. Washington, DC: United States Department of Health and Human Services, National Institutes of Health, National Institute of Environmental Health Sciences, National Toxicology Program; 2005. [Google Scholar]
- 4.U.S. Department of Health & Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention & Health Promotion, Office on Smoking and Health; 2006. [Google Scholar]
- 5.World Health Organization. WHO report on the global tobacco epidemic, 2009: implementing smoke-free environments. Geneva, Switzerland: World Health Organization Press; 2009. [Google Scholar]
- 6.Oberg M, Jaakkola MS, Woodward A, et al. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011;377:139–46. doi: 10.1016/S0140-6736(10)61388-8. [DOI] [PubMed] [Google Scholar]
- 7.The GTSS Collaborative Group. A cross country comparison of exposure to secondhand smoke among youth. Tob Control. 2006;15(Suppl 2):ii4–19. doi: 10.1136/tc.2006.015685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Warren CW, Sinha DN, Lee J, et al. Tobacco use, exposure to secondhand smoke, and training on cessation counseling among nursing students: cross-country data from the Global Health Professions Student Survey (GHPSS), 2005–2009. Int J Environ Res Public Health. 2009;6:2534–49. doi: 10.3390/ijerph6102534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Warren CW, Sinha DN, Lee J, et al. Tobacco use, exposure to secondhand smoke, and cessation counseling training of dental students around the world. J Den Educ. 2011;75:385–405. [PubMed] [Google Scholar]
- 10.Warren CW, Sinha DN, Lee J, et al. Tobacco use, exposure to secondhand smoke, and cessation counseling among medical students: cross-country data from the Global Health Professions Student Survey (GHPSS), 2005–2008. BMC Public Health. 2011;11:72. doi: 10.1186/1471-2458-11-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Warren CW, Asma S, Lee J, et al. GATS Collaborating Group; 2009. Global Tobacco Surveillance System: The GTSS Atlas. http://www.cdc.gov/tobacco/global/gtss/tobacco_atlas/pdfs/tobacco_atlas.pdf. [Google Scholar]
- 12.World Health Organization. Tobacco Free Initiative. Global Adult Tobacco Survey (GATS) http://www.who.int/tobacco/surveillance/survey/gats/en/index.html.
- 13.International Agency for Research on Cancer. Evaluating the effectiveness of smoke-free policies. Lyon, France: International Agency for Research on Cancer; 2009. [Google Scholar]
- 14.Haw SJ, Gruer L. Changes in exposure of adult non-smokers to secondhand smoke after implementation of smoke-free legislation in Scotland: national cross sectional survey. BMJ. 2007;335:549. doi: 10.1136/bmj.39315.670208.47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Akhtar PC, Currie DB, Currie CE, et al. Changes in child exposure to environmental tobacco smoke (CHETS) study after implementation of smoke-free legislation in Scotland: national cross sectional study. BMJ. 2007;335:545. doi: 10.1136/bmj.39311.550197.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fong GT, Hyland A, Borland R, et al. Reductions in tobacco smoke pollution and increases in support for smoke-free public places following the implementation of comprehensive smoke-free workplace legislation in the Republic of Ireland: findings from the ITC Ireland/UK Survey. Tob Control. 2006;15:51–8. doi: 10.1136/tc.2005.013649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Semple S, Maccalman L, Maji AA, et al. Bar workers' exposure to secondhand smoke: the effect of Scottish smoke-free legislation on occupational exposure. Ann Occup Hyg. 2007;51:571–80. doi: 10.1093/annhyg/mem044. [DOI] [PubMed] [Google Scholar]
- 18.Goodman PG, Haw S, Kabir A, et al. Are there health benefits associated with comprehensive smoke-free laws? Int J Public Health. 2009;54:367–78. doi: 10.1007/s00038-009-0089-8. [DOI] [PubMed] [Google Scholar]
- 19.Institute of Medicine. Secondhand smoke exposure and cardiovascular effects: making sense of the evidence. Washington, DC: National Academy of Sciences, Institute of Medicine; 2009. [Google Scholar]
- 20.Borland R, Yong HH, Cummings KM, et al. Determinants and consequences of smoke-free homes: findings from the International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15(Suppl 3):iii42–50. doi: 10.1136/tc.2005.012492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mills AL, Messer K, Gilpin EA, et al. The effect of smoke-free homes on adult smoking behavior: a review. Nicotine Tob Res. 2009;11:1131–41. doi: 10.1093/ntr/ntp122. [DOI] [PubMed] [Google Scholar]
- 22.Scollo M, Lal A, Hyland A, et al. Review of the quality of studies on the economic effects of smoke-free policies on the hospitality industry. Tob Control. 2003;12:13–20. doi: 10.1136/tc.12.1.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.World Health Organization. WHO report on the global tobacco epidemic, 2011: warning about the dangers of tobacco. Geneva, Switzerland: World Health Organization Press; 2011. http://www.who.int/tobacco/global_report/2011/en/ [Google Scholar]
- 24.Hitchman SC, Fong GT. Gender empowerment and female-to-male smoking prevalence ratios. Bull World Health Organ. 2011;89:195–202. doi: 10.2471/BLT.10.079905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Max W, Sung HY, Shi Y. Who is exposed to secondhand smoke? Self-reported and serum cotinine measured exposure in the U.S., 1999–2006. Int J Environ Res Public Health. 2009;6:1633–48. doi: 10.3390/ijerph6051633. [DOI] [PMC free article] [PubMed] [Google Scholar]