

Abstract
Purpose/Introduction:
Osteoporosis is a multifactorial and slowly emerging global health problem. The lifetime risk of dying from hip fracture is same as that from breast cancer. One out of three women between age group of 50-60 years in India suffers from osteoporosis. Indian women have an early age of onset of osteoporosis as compared to western counterparts. There is need for early diagnosis, identification of high-risk groups and prevention and treatment of osteoporosis in the Indian context. The aim of this study was to review the literature published in last decade and compare the research in India with that in rest of the world.
Materials and Methods:
Research articles with key words menopausal, osteoporosis and bone mineral density were searched in Pubmed from January 2004 to December 2013. Articles were categorized according to year, place and objective of the studies.
Results:
In India more articles were published in year 2010-11 (53.3%), while outside the country a uniform distribution of studies was observed throughout the last decade. Objective of research was screening and diagnosis (36.7%) and risk factor identification (40%) in most of the Indian studies as compared to rest of the world. Research publications on prevention and treatment of osteoporosis are less in India (20%).
Conclusion:
Research focusing on diagnosis, prognosis, prevention and treatment are needed in India.
Keywords: Bone mineral density, India, menopause, osteoporosis
INTRODUCTION
Osteoporosis is one of the emerging health issues worldwide. It is a silent disease and causes fractures of bones. Due to an increase in longevity of life in India, osteoporotic fractures are becoming a major cause of morbidity and mortality, which is similar to the western part of the world. It is estimated that currently India has more than 36 million population affected by osteoporosis.[1]
After menopausal in women the process of osteoporosis is accelerated due to deficiency of estrogen. Estrogen helps in the positive calcium metabolism and osteogenesis. Menopause accelerates the bone loss to 2-5% per year, which may continue till 10 years.[2] Prevalence of osteoporosis increases with age in women and not in men. It is reported that 42.5% women and 24.6% men above the age of 50 years suffer from osteoporosis in India.[3] In India peak bone mineral density (BMD) at hip, forearm and spine is significantly lower than corresponding western counterparts.[4] Osteoporosis is becoming a public health problem in India with lower normative index of BMD as compared to western countries. The purpose of this study was to evaluate the objective of clinical studies on osteoporosis in menopausal women in India and compare them with the rest of the world.
MATERIALS AND METHODS
This was an observational study, which includes research articles indexed in Pubmed from January 2004 to December 2013 with key words menopausal, osteoporosis and bone mineral density. The articles were searched using the clinical queries option of Pubmed. Review articles and case reports were excluded from the study by giving command NOT review and NOT case reports. Articles were categorized according to the year of publication, place of study and objectives of the studies. Descriptive statistics was used to calculate simple proportions and percentages out of total number of studies.
RESULTS
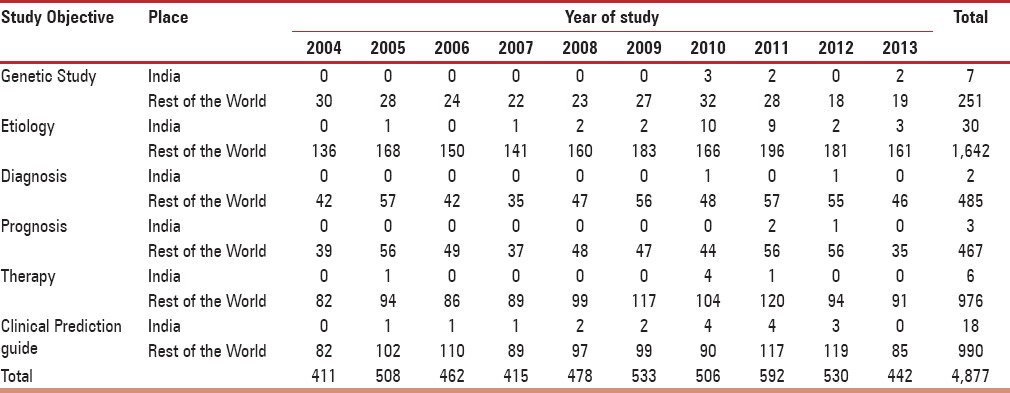
Total 4,877 studies were analyzed; 66 studies were from India and 4,811 were from outside India. Majority of the research occurred during year 2010-11 in India, but there is a uniform distribution of published research in rest of the world [Figure 1]. Analysis according to the objective of the study is depicted in Figure 2. Etiological and clinical prediction studies are more common in India as compared to diagnostic, prognostic and therapeutic studies. Etiological, clinical prediction and therapeutic studies are more observed in rest of the world. Year-wise and objective-wise comparison between India and rest of the world is depicted in Table 1.
Figure 1.
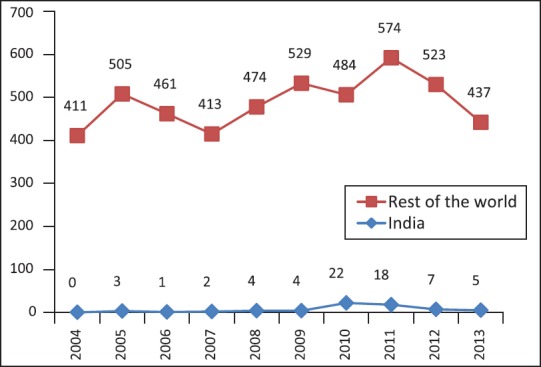
Year-wise distribution of articles from India and rest of the world
Figure 2.
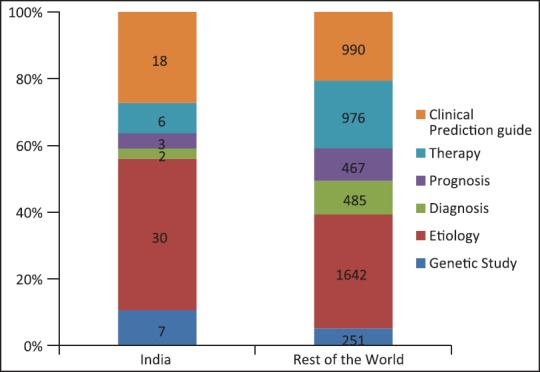
Comparison of objective of the study between India and Rest of the World
Table 1.
Year-wise and objective wise distribution of articles from India and rest of the world
DISCUSSION
Osteoporosis in menopausal women is becoming a major public health problem in India and still Indian research in this field is far behind. This health issue in India is different from the rest of the world as normative index of Indian women is lower as compared to their western counterparts.[2,4] This emphasizes the need for early screening of osteoporosis and early identification of high-risk groups so that early initiation of treatment can be achieved.
Various genetic conditions are known to predispose to osteoporosis. Vitamin D receptor (VDR) gene polymorphism and risk of osteoporosis was found in postmenopausal women of northwest India.[5] Possession of this haplotype exacerbates the risk of osteoporosis by 2.8 times. Association of apolipoprotein E (APOE) genotypes with BMD and risk of osteoporosis have also been reported from India.[6] This study focused on postmenopausal women only; no Indian study included women irrespective of menopausal, which will add more knowledge about genetic predisposition to osteoporosis. Estrogen receptor alpha (ESR1) gene polymorphisms was the most important factor, which is discussed in Indian context as estrogen is an essential hormone for absorption of calcium and bone metabolism. The case control study showed the ESR1 gene is associated with low bone mass and low estradiol levels in all study subjects and increased the risk of osteoporosis later in life.[7] Outside India, various polymorphisms were found, which can also be studied in India for early prediction of osteoporosis. Some well-known polymorphisms that are recently studied outside India are CYP19 gene, ESR2 AluI gene, DBP gene and osteoprotegerin (OPG) gene.[8,9,10,11]
Certain risk factors accentuate pre-existing osteoporosis hence special attention is needed for these people. Comparative study of Indian women with Iranian women showed that duration of menopause greater than 5 years, menarche age (more than 14 years), menopause age (before 45 years) and parity more than 3 are the major risk factors to osteoporosis which were observed in both the population.[12] Influence of years since menopause was studied in a south Indian population, and it was found that the risk of bone resorption is greater in early than late years of menopause.[13] The decreased bone resorption risk in late postmenopausal women might be due to increased FSH levels. Nutritional status and dietary calcium intake directly related to bone mineral density have been found in India.[14] Indian women are also frequently deficient in vitamin D, which is essential for positive bone metabolism.[15] Major source of vitamin D is exposure to sun. Considering Indian geographic location, Indians can get more Vitamin D synthesized if they are exposed to sun between 11 AM and 2 PM.[16] Lower socio-economic status, grand multiparity, duration of breastfeeding and corticosteroid therapy were other important factors that were also reported as risk factors for osteoporosis among studies published from outside India.[17,18,19]
DEXA (Dual Energy X-Ray Absorptiometry) scan is the most acceptable modality worldwide for the diagnosis and quantification of osteoporosis. In India, it is expensive and not widely available. Hence population screening of all high-risk women is not possible in India. Several bone markers can give clue of bone density and can be utilized for screening of osteoporosis and it can also be utilized to monitor the success in treatment. Various bone markers studied outside India are insulin-like growth factor 1 (IGF-1), osteoprotegerin (OPG), leptin, osteocalcin (OC), and urinary excretion of N-terminal telopeptide of type I collagen (NTx). The serum level of IGF-1 had significant, positive correlation with lean mass. Measurement of serum IGF-1 in young women may help in the early identification of those at risk for developing low bone mass and osteoporosis.[20] Baseline measurements of resorption markers are useful before the commencement of anti-resorptive treatment and can be checked 3-6 months later to monitor response and adherence to treatment.[21] There is no published Indian study on bone markers, which can be used to monitor effect of treatment on osteoporosis.
Prognosis of the disease depends on how early the condition is diagnosed and treatment initiated. As pathophysiology of osteoporosis is multifactorial, management part includes various factors like modification of lifestyle, diet, exposure to sun, exercise and drug treatment. Moderate to intense exercises, in water or on the ground and passive mechanical vibration can prevent and treat postmenopausal osteoporosis. This has reported to be beneficial for bone microarchitecture, improving bone density and bone strength.[22,23] Activities aimed to develop muscle strength, body balance and proprioception are also important.[22] A good general nutritional status and adequate dietary protein, calcium, vitamin D, fruits and vegetables have a positive influence on bone health while on the other hand high cholesterol and alcohol in diet increases the risk of osteoporosis.[24,25]
Though there are limited studies in India, the Indian Menopausal Society has developed guidelines for the management of postmenopausal osteoporosis.[26] It divides women according to years (less than 5 years and more) since menopause. Menopause of less than 5 years with no risk factors requires only primary preventive measures such as improved nutrition, lifestyle modification, adequate vitamin D and calcium, and exercise. Menopause since more than 5 years and osteoporosis diagnosed by DEXA scan requires active medical treatment with Bisphosphonates, Raloxifene and Strontium ranelate.
CONCLUSION
Considering all the above observations, Indian research for diagnostic, prognostic and therapeutic aspect of osteoporosis in menopausal women is needed to better understand and combat this emerging health problem in India.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Gupta A. Osteoporosis in India--the nutritional hypothesis. Natl Med J India. 1996;9:268–74. [PubMed] [Google Scholar]
- 2.Malhotra N, Mithal A. Osteoporosis in Indians. Indian J Med Res. 2008;127:263–8. [PubMed] [Google Scholar]
- 3.Marwaha RK, Tandon N, Garg MK, Kanwar R, Narang A, Sastry A, et al. Bone health in healthy Indian population aged 50 years and above. Osteoporos Int. 2011;22:2829–36. doi: 10.1007/s00198-010-1507-8. [DOI] [PubMed] [Google Scholar]
- 4.New Delhi: ICMR: Published by Director General; 2010. Population based reference standards of Peak Bone Mineral Density of Indian males and females – an ICMR multi-center task force study; pp. 1–24. [Google Scholar]
- 5.Singh M, Singh P, Singh S, Juneja PK, Kaur T. Vitamin D receptor (VDR) gene polymorphism influences the risk of osteoporosis in postmenopausal women of Northwest India. Arch Osteoporos. 2013;8:147. doi: 10.1007/s11657-013-0147-y. [DOI] [PubMed] [Google Scholar]
- 6.Singh M, Singh P, Singh S, Juneja PK, Kaur T. A susceptible haplotype within APOE gene influences BMD and intensifies the osteoporosis risk in postmenopausal women of Northwest India. Maturitas. 2010;67:239–44. doi: 10.1016/j.maturitas.2010.06.017. [DOI] [PubMed] [Google Scholar]
- 7.Jeedigunta Y, Bhoomi Reddy PR, Kolla VK, Munshi A, Ananthapur V, Narasimulu G, et al. Association of estrogen receptor alpha gene polymorphisms with BMD and their effect on estradiol levels in pre- and postmenopausal women in south Indian population from Andhra Pradesh. Clin Chim Acta. 2010;411:597–600. doi: 10.1016/j.cca.2010.01.026. [DOI] [PubMed] [Google Scholar]
- 8.Koudu Y, Onouchi T, Hosoi T, Horiuchi T. Association of CYP19 gene polymorphism with vertebral fractures in Japanese postmenopausal women. Biochem Genet. 2012;50:389–96. doi: 10.1007/s10528-011-9483-z. [DOI] [PubMed] [Google Scholar]
- 9.Currò M, Marini H, Alibrandi A, Ferlazzo N, Condello S, Polito F, et al. The ESR2 AluI gene polymorphism is associated with bone mineral density in postmenopausal women. J Steroid Biochem Mol Biol. 2011;127:413–7. doi: 10.1016/j.jsbmb.2011.05.008. [DOI] [PubMed] [Google Scholar]
- 10.Chupeerach C, Tungtrongchitr A, Phonrat B, Schweigert FJ, Tungtrongchitr R, Preutthipan S. Association of Thr420Lys polymorphism in DBP gene with fat-soluble vitamins and low radial bone mineral density in postmenopausal Thai women. Biomark Med. 2012;6:103–8. doi: 10.2217/bmm.11.88. [DOI] [PubMed] [Google Scholar]
- 11.Feng G, Meng L, Wang H, Lu Y, Jia J, Zhang Y, et al. Single-nucleotide polymorphism of the osteoprotegerin gene and its association with bone mineral density in Chinese postmenopausal women. J Pediatr Endocrinol Metab. 2012;25:1141–4. doi: 10.1515/jpem-2012-0274. [DOI] [PubMed] [Google Scholar]
- 12.Keramat A, Patwardhan B, Larijani B, Chopra A, Mithal A, Chakravarty D, et al. The assessment of osteoporosis risk factors in Iranian women compared with Indian women. BMC Musculoskelet Disord. 2008;9:28. doi: 10.1186/1471-2474-9-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Suresh M, Naidu DM. Influence of years since menopause on bone mineral metabolism in South Indian women. Indian J Med Sci. 2006;60:190–8. [PubMed] [Google Scholar]
- 14.Shatrugna V, Kulkarni B, Kumar PA, Rani KU, Balakrishna N. Bone status of Indian women from a low-income group and its relationship to the nutritional status. Osteoporos Int. 2005;16:1827–35. doi: 10.1007/s00198-005-1933-1. [DOI] [PubMed] [Google Scholar]
- 15.Harinarayan CV, Sachan A, Reddy PA, Satish KM, Prasad UV, Srivani P. Vitamin D status and bone mineral density in women of reproductive and postmenopausal age groups: A cross-sectional study from south India. J Assoc Physicians India. 2011;59:698–704. [PubMed] [Google Scholar]
- 16.Harinarayan CV, Holick MF, Prasad UV, Vani PS, Himabindu G. Vitamin D status and sun exposure in India. Dermatoendocrinol. 2013;5:130–41. doi: 10.4161/derm.23873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Demirtas O, Demirtas G, Hursitoglu BS, Terzi H, Sekerci Z, Ok N. Is grand multiparity a risk factor for osteoporosis in postmenopausal women of lower socioeconomic status? Eur Rev Med Pharmacol Sci. 2014;18:2709–14. [PubMed] [Google Scholar]
- 18.Bolzetta F, Veronese N, De Rui M, Berton L, Carraro S, Pizzato S, et al. Duration of breastfeeding as a risk factor for vertebral fractures. Bone. 2014;68:41–5. doi: 10.1016/j.bone.2014.08.001. [DOI] [PubMed] [Google Scholar]
- 19.Villa P, Moruzzi MC, Lassandro AP, Leoni F, Di Nardo F, De Waure C, et al. for Lazio-GISMO group. Glucocorticoid therapy as a significant risk factor for osteoporosis and fractures in an Italian postmenopausal population. Gynecol Endocrinol. 2013;29:678–82. doi: 10.3109/09513590.2013.788631. [DOI] [PubMed] [Google Scholar]
- 20.Liu JM, Zhao HY, Ning G, Chen Y, Zhang LZ, Sun LH, et al. IGF-1 as an early marker for low bone mass or osteoporosis in premenopausal and postmenopausal women. J Bone Miner Metab. 2008;26:159–64. doi: 10.1007/s00774-007-0799-z. [DOI] [PubMed] [Google Scholar]
- 21.Wheater G, Elshahaly M, Tuck SP, Datta HK, van Laar JM. The clinical utility of bone marker measurements in osteoporosis. J Transl Med. 2013;11:201. doi: 10.1186/1479-5876-11-201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Moreira LD, Oliveira ML, Lirani-Galvão AP, Marin-Mio RV, Santos RN, Lazaretti-Castro M. Physical exercise and osteoporosis: Effects of different types of exercises on bone and physical function of ostmenopausal women. Arq Bras Endocrinol Metabol. 2014;58:514–22. doi: 10.1590/0004-2730000003374. [DOI] [PubMed] [Google Scholar]
- 23.Murtezani A, Nevzati A, Ibraimi Z, Sllamniku S, Meka VS, Abazi N. The effect of land versus aquatic exercise program on bone mineral density and physical function in postmenopausal women with osteoporosis: A randomized controlled trial. Ortop Traumatol Rehabil. 2014;16:319–25. doi: 10.5604/15093492.1112533. [DOI] [PubMed] [Google Scholar]
- 24.Levis S, Lagari VS. The role of diet in osteoporosis prevention and management. Curr Osteoporos Rep. 2012;10:296–302. doi: 10.1007/s11914-012-0119-y. [DOI] [PubMed] [Google Scholar]
- 25.You L, Sheng ZY, Tang CL, Chen L, Pan L, Chen JY. High cholesterol diet increases osteoporosis risk via inhibiting bone formation in rats. Acta Pharmacol Sin. 2011;32:1498–504. doi: 10.1038/aps.2011.135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Meeta, Harinarayan CV, Marwah R, Sahay R, Kalra S, Babhulkar S. Clinical practice guidelines on postmenopausal osteoporosis: An executive summary and recommendations. J Midlife Health. 2013;4:107–26. doi: 10.4103/0976-7800.115293. [DOI] [PMC free article] [PubMed] [Google Scholar]