

Abstract
Background:
The reported association between vitamin D level and loss of Bone mineral densitometry measurements (BMD) has been controversial.
Objective:
The objectıve of the current study was to determine whether low vitamin D level and BMD are associated with depresive symptoms as burden in Arab women during the menopausal and postmenopausal period.
Design and Setting:
A cross-sectional descriptive study design was used at the Primary Health Care (PHC) Centers in Qatar.
Subjects:
A multi-stage sampling design was used and a representative sample of 1436 women aged 45-65 years were included during July 2012 and November 2013 and 1106 women agreed to participate (77.2%) and responded to the study.
Materials and Methods:
BMD (g/m2) was assessed at the BMD unit using a Lunar Prodigy DXA system (Lunar Corp., Madison, WI). The antero-posterior lumbar spine (L2-L4) and the mean of the proximal right and left femur were be measured by two technician and then reviewed by one radiologist. Data on body mass index (BMI), clinical biochemistry variables including serum 25-hydroxyvitamin D were collected. The Beck Depression Inventory (BDI) was administered for depression purposes.
Results:
Of the 1436 women living in urban and rural areas, 1106 women agreed to participate (77.0%) and responded to the study. The mean age and standard deviation of the subjects was 53.8 ± 3.2. The median age of natural menopausal in the present study was 49 years (mean and standard deviation 49.5 ± 3.1 and postmenopausal was 58.1 ± 3.3). There were statistically significant differences between menopausal stages with regards to ethnicity, education level, systolic and dialostic blood pressure, parity, sheesha smoking and depressive symptoms. Overall 30.4% of women were affected with osteopenia/osteoporosis in premenopausal and postmenopausal (24.4% vs 35.7%; P = 0.0442). Osteopenia in premenopausal and postmenopausal (18.7% vs 29.3%; P = 0.030) and Osteoporosis (9.9% vs 15.9%; P = 0.049) were significantly higher in post-menopausal women than in premenopausal women (P = 0.046). Similarly, vitamin D deficiency was more prevalent among postmenopausal women than menopausal women. Overall, only 15.1% of women had optimum vitamin D level and 15.5% had severe, 33.2% had moderate vitamin D insufficiency and 36.3% had mild vitamin D insufficiency in menopausal and post menopausal women (P = 0.021). The study revealed that vitamin D level, hemoglobin level, serum iron fasting plasma glucose, calcium, triglycerides, high density lipid (HDL) cholesterol, low density lipid (LDL) Cholesterol, alkaline phosphate and magnesium were considerably lower in postmenopausal compared to menopausal women (P < 0.001).
Conclusion:
The current study revealed that there was a strong association between vitamin D level and BMD in Arab women during the menopausal and post-menopausal period.
Keywords: Bone mineral density, depression, disease, menopausal, postmenopausal, physical activity, vitamin D
INTRODUCTION
Menopausal is the cessation of a woman's reproductive ability, the opposite of menarche. Menopausal is usually a natural change; it typically occurs in women in midlife, during their late 40s or early 50s, signaling the end of the fertile phase of a woman's life.[1] Menopausal is commonly defined by the state of the uterus and the absence of menstrual flow or “periods”, but it can instead be more accurately defined as the permanent cessation of the primary functions of the ovaries.[2] The transition from a potentially reproductive to a non-reproductive state is normally not sudden or abrupt, occurs over a number of years, and is a consequence of biological aging.[3,4,5,6,7]
Many women are likely to live more than 30 years after menopausal, spending about one-third of their lives in a state of estrogen deficiency.[2] Age at natural menopausal is an important research issue because of the suspected links between it and risk for certain diseases. Without intervention, more than 75% of these females will suffer the distressing sequelae of menopausal,[2,6,7,8,9] which include headache, irritability, fatigue, depression,[8,9] nervousness, poor concentration,[2] sexual dysfunction,[10] physical, psychological and psychiatric disorders,[5] major depressive disorders[11] and the more worrying effects of menopausal-related osteoporosis and ischemic heart disease (IHD).[12]
The role of vitamin D and its metabolites on bone health has been recognized for a long time.[6] Severe vitamin D deficiency causes overt osteomalacia in adults; mild to moderate vitamin D deficiency, also called vitamin D insufficiency, causes secondary hyperparathyroidism. Hence, vitamin D insufficiency might increase bone turnover and bone loss mainly from cortical sites.,[10] especially in postmenopausal women.[13]
However, there is no information available on bone mineral density (BMD), vitamin D and depression during menopausal and post-menopause in the State of Qatar. The reported association between Vitamın D, depression and loss of BMD has been controversial.[8,11,14] The objective of current study was conducted to determine whether the objectıve of current study was conducted to determine whether low vitamin D level and BMD are associated with depresive symptoms as burden in Arab women during the menopausal and post-menopausal period.
MATERIALS AND METHODS
Study design
This is a cross-sectional Primary Health Care (PHC) Centers based study conducted in the State of Qatar. The survey was conducted among Qatari national and Arab women aged 45-65 years old. Similar to other reported studies,[2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17] women were excluded with contraindications to estrogen use and, women who had a current unstable medical or social problem.[5]
Questionnaire and interview
Eligibility criteria
The entry criteria for the study were to be:
45-65 years of age;
Diagnosis of major depression according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV);
Moderate to severe depression according to the 21-item Beck Depression Inventory (BDI) [1-63] score;
No current use of homeopathic treatment for depression or antidepressants or anxiolytic drugs for three months prior to study entry;
Not taking psychotherapy for at least 3 months before screening;
No use of estrogens or other medications known to affect ovarian function for at least 3 months before screening;
Early transition to menopausal, defined by a change in cycle length of seven days or longer in either direction from the participant's own baseline for at least two cycles;
Postmenopausal stage defined by 12 months or more of amenorrhea; and
Capability and willingness to give informed consent and to comply with the study procedures.
Measures
Serum 25-hydroxyvitamin D (25OHD)
Trained phlebotomist collected venous blood sample, and serum separated and stored at −70°C until analysis. Serum 25-hydroxyvitamin D (25OHD), a vitamin D metabolite, was measured using a commercially available kit (DiaSorin Corporate Headquarter, Saluggia, Italy). The treated samples were then assayed using competitive binding radioimmunoassay (RIA) technique. Vitamin D deficiency which is defined as serum 25OHD and subjects were classified into four categories as described by Bener and El Ayoubi[14] and as recommended by Eyles et al.,[14] 1) severe vitamin D deficiency, 25OHD <10 ng/ml; 2) moderate deficiency, 25OHD 10-19 ng/ml; 3) mild deficiency, 25OHD 20-29 ng/ml; and normal/optimal level is between 30-80 ng/ml.
Bone mineral densitometry measurements
BMD (g/m2) was assessed at the BMD unit using a Lunar Prodigy DXA system (Lunar Corp., Madison, WI). The antero-posterior lumbar spine (L2-L4) and the mean of the proximal right and left femur (including total femur, neck, Ward's triangle and the trochanter) were be measured by two technologists and then reviewed by one radiologist using methods described.[5,10,11,12,13] Quality control of the DXA scanner included daily calibration and duplicate measures of a sample of the participants. The precision of the system, reported in a previous study, was found to be 1.6% for the spine and 1.2% for the total femur.[5,10,11,12,13] BMD was categorized according to the World Health Organization (WHO)[15] criteria based on the T-score. Values between −1.0 and −2.5 were classified as osteopenia, a T-score of −2.5 or below as osteoporosis, and a T-score of −1.0 and above as normal.[10,11,15]
The BDI-II was a 1996 revision of the BDI,[18] developed in response to the American Psychiatric Association's (APA) publication of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, which changed many of the diagnostic criteria for Major Depressive Disorder (MDD). The BDI is a widely-used, self-evaluation depression scale. The long form of the BDI, used in this study, comprises of 21 questions or items, each with four possible responses. Each response is assigned a score ranging from zero to three, indicating the severity of the symptom.[18] Items 1-13 assess symptoms that are psychological in nature, while items 14-21 assess more physical symptoms. The sum of all BDI item scores indicates the severity of depression. A score of 21 or above represents depression. Score between 1-10 these ups and downs are considered normal; scores between 11-16 considered mild mood disturbance; scores 17-20 considered borderline clinical depression; scores 21-30 is moderate depression; scores 31-40 is severe depression; finally, scores over 40 are determined extreme depression.
The data were collected through a validated questionnaire with the help of qualified nurses who were Arab nationals and could speak and write English and Arabic languages well and were aware of the Arabic culture and thus were able to engage and gain the trust of the study participants. Data collection took place from July 2012 to November 2013. The sample size was determined on a priori presumption that the prevalence rate of postpartum depression in Qatar would be more or less similar to rates found in other countries in the eastern Mediterranean, where the reported prevalence of postpartum depression to be 20%, with the 95% confidence interval (CI) for 2.5% error of estimation, a sample size of 1500 subjects would be required for this study. Of the 22 primary health care centers available, we have selected 12 health centers, of these, 10 were located in urban and two in semi-urban areas of Qatar. Finally, subjects were selected systematically 1-in-2 using a sampling procedure. Each participant was provided with brief information about the study and was assured of strict confidentiality. The survey instrument was initially tested for validation on 86 patients through face to face interview who visited the health centers. The Cronbach's alpha scores was 0.85 for Internet BDI scales respectively, confirming a high level of consistency among the different Likert items in both of these scales.
Statistical test
Data was analyzed using SPSS version 21. Sum of scores were calculated for BDI. Proportion with percentage was calculated for categorical variables and mean with standard deviation for continuous scale variables. Student-t test was used to ascertain the significance of differences between mean values of two continuous variables and confirmed by non-parametric Mann-Whitney test. The Chi-square and Fisher's exact tests (two-tailed) were performed to test for differences in proportions of categorical variables between two or more groups. Kruskal Wallis one-way analysis of variance (ANOVA) was employed for comparison of several group means. The Spearman's correlation coefficient was used to evaluate the strength of concordance between variables. The level P < 0.05 was considered as the cut-off value for significance.
RESULTS
Of the 1436 women living in urban and rural areas, 1106 women agreed to participate (77.0%) and responded to the study. The mean age and standard deviation (SD) of the subjects was 53.8 ± 3.2. The median age of natural menopausal in the present study was 49 years [mean and standard deviation 49.5 ± 3.1 and postmenopausal was 58.1 ± 3.3]. The rate of consanguineous marriages in the sample was found to be 33.3%. Figure 1 shows distribution of depression in menopausal and postmenopausal women, there were statistically significance differences between menopausal stages with regards to depression (P < 0.012).
Figure 1.
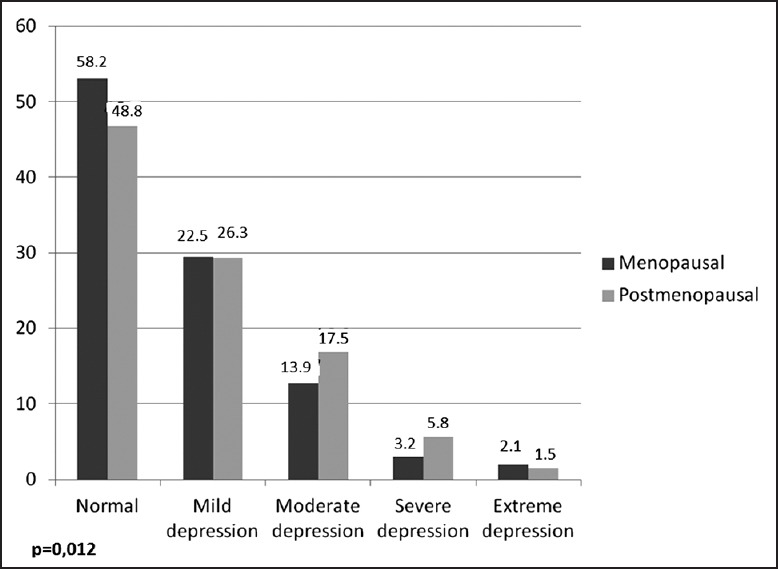
The distribution of depression in menopausal and post-menopausal women
Table 1 shows the socio-demographic characteristics of studied subject by menopausal and post-menopausal status. There were statistically significance differences between menopausal stages with regards to ethnicity, education level, Systolic and Dialostic Blood Pressure, parity, sheesha smoking and depressive symptoms.
Table 1.
The socio-demographics and lifestyle characters of studied subject by menopausal and postmenopausal
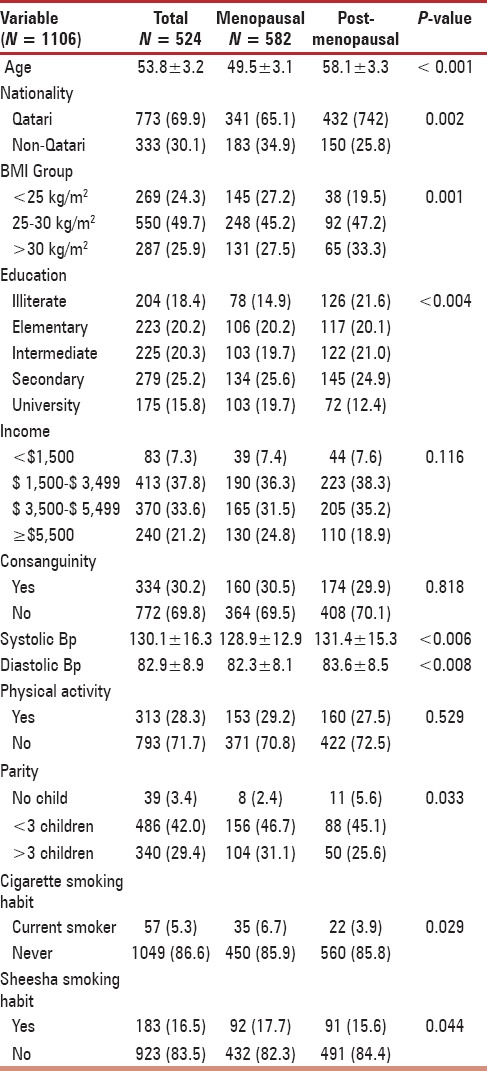
Table 2 presents osteopenia/osteoporosis profile and serum level of 25OHD in menopausal and postmenopausal women. Overall 23.9% of women were affected with osteopenia/osteoporosis in menopausal and postmenopausal (18.3% vs 29.6%; P < 0.0001). Osteopenia in menopausal and postmenopausal (18.7% vs 29.3%; P = 0.042) and Osteoporosis (6.9% vs 11.7%; P = 0.006) were significantly higher in post-menopausal women than in menopausal women. Similarly, vitamin D deficiency was more prevalent among postmenopausal women than menopausal women. Overall, only 15.1% of women had optimum vitamin D level and 15.5% had severe, 33.2% had moderate vitamin D insufficiency and 36.3% had mild vitamin D insufficiency in menopausal and post menopausal women (P = 0.021).
Table 2.
Osteopenia/Osteoporosis profile and serum level of 25OHD in menopausal and postmenopausal status. (N = 1106)
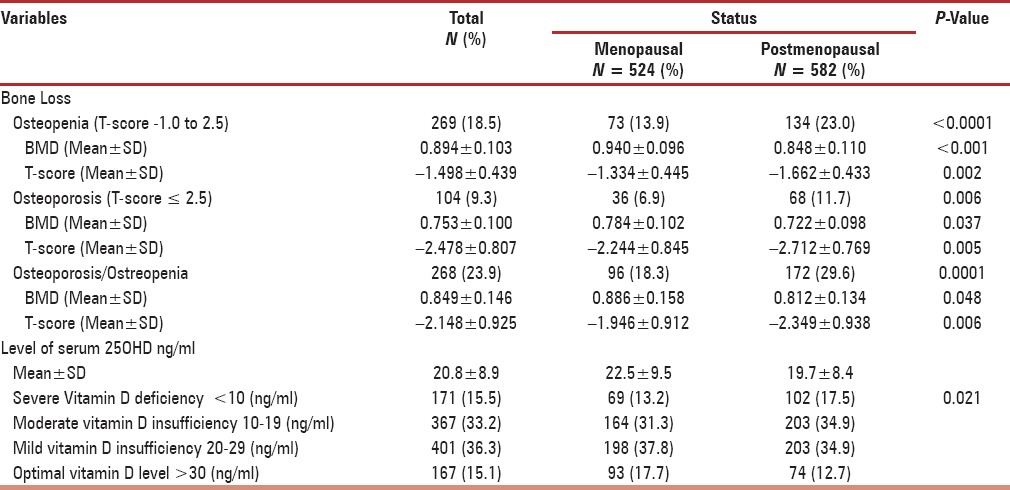
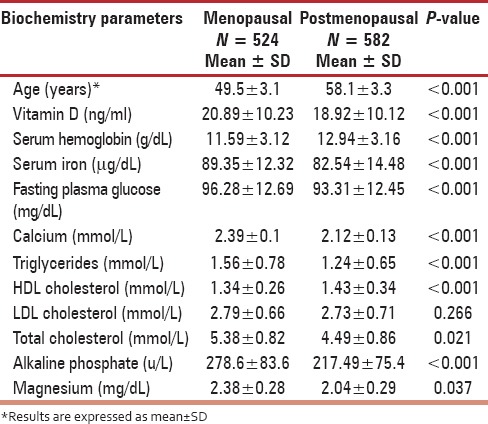
Table 3 shows biomarker values among menopausal and postmenopausal women. The study revealed that vitamin D level, hemoglobin level, serum iron fasting plasma glucose, calcium, triglycerides, HDL cholesterol, LDL Cholesterol, alkaline phosphate and magnesium were considerably lower in post-menopausal compared to menopausal women (P < 0.001).
Table 3.
Baseline serum and biochemical markers in menopausal and postmenopausal status. (N = 1106)
DISCUSSION
Menopausal is a biological process characterized by cessation of the menstrual cycle in women with a decline in age approximately between 40-60 years with the average age observed in the 52 years.[2] Symptoms experienced during menopausal and socio-demographic characteristics affect the quality of life in postmenopausal women. Hot flashes impact the daily activities of most postmenopausal women, especially those with more frequent/severe symptoms. Treatments that safely and effectively treat these symptoms could improve quality of life among postmenopausal women.[19] Menopausal is a unique experience. It is not a type of disease, but rather a stage in biological and physiological development. Menopausal produces very complex changes during this stage of life which include other changes such as psychological and social changes.[2] More recently study showed that due to postmenopausal depression predicted increased bone loss ın Finland.
Depression has been implicated as a possible risk factor for low BMD. However, there is still no solid evidence that could connect these two different illnesses. This research examined the association between depression and low BMD in menopausal and menopausal women. The loss of BMD with aging is a result of the complex interactions of hormonal, environmental, nutritional, and genetic factors. In recent years, psychological status has been identified as another factor possibly related to the loss of BMD.[8,11,14,16,17] In clinically depressed populations, significantly lower BMD has been found compared to nondepressed controls.[8,11,14,16,17] Lower BMD in depressed populations could be related to depression itself or to other behavioral disturbances that occur as a result of depression. Factors sometimes associated with depression such a s lower levels of physical activity, changes in body weight, lower calcium compliance, or use of antidepressant medications have been postulated as underlying causes of bone loss.[8,11,14,16,17]
There are precise recommendations regarding a sufficient Vitamin D intake in order to prevent, bone, loss in menopausal and postmenopausal women.[11,19,20] Considering the fact that Vitamin D deficiency and menopausal share risk factors beyond bone health such as cardiovascular, metabolic, cognitive and affective disorders, a sufficient Vitamin D status should be obtained in all peri- and postmenopausal women. This might be beneficial not only considering bone health but also regarding cognitive, affective, metabolic and cardiovascular health of women.[20] Furthermore, a number of studies revealed a positive association between serum 25OHD level and BMD.[11,19,20,21,22,23,24] This is confirmastive with the present study outcome.
The overall health and well-being of middle-aged women have become a major public health concern around the world. More than 80% of the women experience physical or psychological symptoms in the years when they approach menopausal, with various distress and disturbances in their lives, leading to a decrease in the quality of life.[2,3,5,6,7,8,9,10,11]
In Brazil,[4] the study was conducted to identify the prevalence of physical, psychological, and menopausal-related symptoms and their association with minor psychiatric disorders in menopausal and postmenopausal women, fatigue was the most frequent complaint in all groups. Low education level, memory loss, irritability, and the menopausal transition represent risk factors for positive findings in screening for minor psychiatric disorders. This is consistent with the current and previous reported studies.[3,5,6,7,8,9,10,11,20,22,23,24]
The study reported is consistent with the neighboring United Arab Emirates[2,3] and other developing countries.[4,5,6,7,8,9,10,14,15,16,17,18,21] However, the present study showed that climacteric symptoms in postmenopausal women in Qatari's women are less than in Western Women[4,5,6,7,8,9,10,14,15,16,17,18,21] and may be influenced by genetic factors, parity and previous use of oral contraceptives.
Limitations and strengths
There are several limitations of this study. First, the study is a cross-sectional design and the study sample was based on PHC Clinics visits. Second, the majority of the study sample was Arab women and of relatively high socioeconomic and education status; hence, the results are not generalizable to the population of all midlife women. Third, the information obtained for the biochemistry variables were based the medical records Furthermore, we were unable to evaluate the impact of these factors on change in quality of life over time. Despite these limitations, this study had a number of strengths. This study based on a large representative's sample and based on face-to-face ınterview.
CONCLUSION
The current study is consistent with previous findings of diminished low vitamin D correlated with BMD and depressive symptoms may be a risk factor for reduced BMD in perimanopausal or postmenopausal women.
CONTRIBUTORS
AB was involved in data collection, statistical analysis, interpretation of data and writing the manuscript. NMS was involved in data collection, interpretation of data, writing and editing the manuscript. All authors approved the final version.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors would like to thank the Hamad Medical Corporation for their support and ethical approval (HMC RC#8222/08).
REFERENCES
- 1.Harlow SD, Gass M, Hall JE, Lobo R, Maki P, Rebar RW, et al. STRAW + 10 Collaborative Group. Executive summary of the Stages of Reproductive Aging Workshop + 10: Addressing the unfinished agenda of staging reproductive aging. J Clin Endocrinol Metab. 2012;97:1159–68. doi: 10.1210/jc.2011-3362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bener A, Rizk DE, Shaheen H, Micallef R, Osman N, Dunn EV. Measurement-specific quality-of-life satisfaction during menopause in an Arabian Gulf country. Climacteric. 2000;3:43–9. doi: 10.3109/13697130009167598. [DOI] [PubMed] [Google Scholar]
- 3.Bener A, Rizk DE, Ezimokhai M, Hassan M, Micallef R, Sawaya M. Consangunity and the age of menopause in the United Arab Emirates. Int J Gynaecol Obstet. 1998;60:155–60. doi: 10.1016/s0020-7292(97)00250-6. [DOI] [PubMed] [Google Scholar]
- 4.Oppermann K, Fuchs SC, Donato G, Bastos CA, Spritzer PM. Physical, psychological, and menopause-related symptoms and minor psychiatric disorders in a community-based sample of Brazilian premenopausal, perimenopausal, and postmenopausal women. Menopause. 2012;19:355–60. doi: 10.1097/gme.0b013e31822ba026. [DOI] [PubMed] [Google Scholar]
- 5.Bener A, Falah A. A measurement-specific quality-of-life satisfaction during premenopause, perimenopause and postmenopause in an Arabian Qatari women. J Midlife Health. 2014;5:126–34. doi: 10.4103/0976-7800.141190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Parfitt AM, Gallagher JC, Heaney RP, Johnston CC, Neer R, Whedon GD. Vitamin D and bone health in the elderly. Am J Clin Nutr. 1982;36:1014–31. doi: 10.1093/ajcn/36.5.1014. [DOI] [PubMed] [Google Scholar]
- 7.Avis NE, Assmann SF, Kravitz HM, Ganz PA, Ory M. Quality of life in diverse groups of midlife women: Assessing the influence of menopause, health status and psychosocial and demographic factors. Qual Life Res. 2004;13:933–46. doi: 10.1023/B:QURE.0000025582.91310.9f. [DOI] [PubMed] [Google Scholar]
- 8.Cizza G, Ravn P, Chrousos GP, Gold PW. Depression: A major, unrecognized risk factor for osteoporosis? Trends Endocrinol Metab. 2001;12:198–203. doi: 10.1016/s1043-2760(01)00407-6. [DOI] [PubMed] [Google Scholar]
- 9.Sabia S, Fournier A, Mesrine S, Boutron-Ruault MC, Clavel-Chapelon F. Risk factors for onset of menopausal symptoms: Results from a large cohort study. Maturitas. 2008;60:108–21. doi: 10.1016/j.maturitas.2008.04.004. [DOI] [PubMed] [Google Scholar]
- 10.Hammoudeh M, Al Khayarin M, Zirie M, Bener A. Bone density measured by dual energy X-ray absorptiometry in Qatari women. Maturitas. 2005;52:319–27. doi: 10.1016/j.maturitas.2005.05.011. [DOI] [PubMed] [Google Scholar]
- 11.Bener A, El Ayoubi HR. The role of vitamin D deficiency and osteoporosis in breast cancer. Int J Rheum Dis. 2012;15:554–61. doi: 10.1111/1756-185x.12017. [DOI] [PubMed] [Google Scholar]
- 12.Oh SM, Kim HC, Ahn SV, Rhee Y, Suh I. Association between depression and bone mineral density in community-dwelling older men and women in Korea. Maturitas. 2012;71:142–6. doi: 10.1016/j.maturitas.2011.11.007. [DOI] [PubMed] [Google Scholar]
- 13.Hosseinpanah F, Rambod M, Hossein-nejad A, Larijani B, Azizi F. Association between vitamin D and bone mineral density in Iranian postmenopausal women. J Bone Miner Metab. 2008;26:86–92. doi: 10.1007/s00774-007-0791-7. [DOI] [PubMed] [Google Scholar]
- 14.Eyles DW, Burne TH, McGrath JJ. Vitamin D, effects on brain development, adult brain function and the links between low levels of vitamin D and neuropsychiatric disease. Front Neuroendocrinol. 2013;34:47–64. doi: 10.1016/j.yfrne.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 15.Geneva, Switzerland: World Health Organization; 1994. World Health Organization (WHO). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Report of a WHO study group. WHO Technical Report Series, Report No. 843. [PubMed] [Google Scholar]
- 16.Bosworth HB, Bastian LA, Kuchibhatla MN, Steffens DC, McBride CM, Skinner CS, et al. Depressive symptoms, menopausal status and climacteric symptoms in women at midlife. Psychosom Med. 2001;63:603–8. doi: 10.1097/00006842-200107000-00013. [DOI] [PubMed] [Google Scholar]
- 17.Wu Q, Magnus JH, Liu J, Bencaz AF, Hentz JG. Depression and low bone mineral density: A meta-analysis of epidemiologic studies. Osteoporos Int. 2009;20:1309–20. doi: 10.1007/s00198-009-0918-x. [DOI] [PubMed] [Google Scholar]
- 18.Beck AT, Steer RA, Ball R, Ranieri W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J Pers Assess. 1996;67:588–97. doi: 10.1207/s15327752jpa6703_13. [DOI] [PubMed] [Google Scholar]
- 19.Lerchbaum E. Vitamin D and menopause – a narrative review. Maturitas. 2014;79:3–7. doi: 10.1016/j.maturitas.2014.06.003. [DOI] [PubMed] [Google Scholar]
- 20.Lyles KW. Osteoporosis and depression: Shedding more light upon a complex relationship. J Am Geriatr Soc. 2001;49:827–8. doi: 10.1046/j.1532-5415.2001.49162.x. [DOI] [PubMed] [Google Scholar]
- 21.Malavolta N, Pratelli L, Frigato M, Mule R, Mascia ML, Gnudi S. The relationship of vitamin D status to bone mineral density in an Italian population of postmenopausal women. Osteoporos Int. 2005;16:1691–7. doi: 10.1007/s00198-005-1883-7. [DOI] [PubMed] [Google Scholar]
- 22.Collins D, Jasani C, Fogelman I, Swaminathan R. Vitamin D and bone mineral density. Osteoporos Int. 1998;8:110–4. doi: 10.1007/BF02672505. [DOI] [PubMed] [Google Scholar]
- 23.Bener A, Al-Hamaq AO, Saleh NM. Association between vitamin D insufficiency and adverse pregnancy outcome: Global comparisons. Int J Womens Health. 2013;5:523–31. doi: 10.2147/IJWH.S51403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sahota O, Masud T, San P, Hosking DJ. Vitamin D insufficiency increases bone turnover markers and enhances bone loss at the hip in patients with established vertebral osteoporosis. Clin Endocrinol (Oxf) 1999;51:217–21. doi: 10.1046/j.1365-2265.1999.00764.x. [DOI] [PubMed] [Google Scholar]