

Abstract
Risk of developing of emotional and behavioral mental health problems increases markedly during adolescence. Despite this increasing need, most adolescents, particularly ethnic minority youth, do not seek professional help. Informed by conceptual models of health behavior, the current study examined how cultural values are related to help-seeking among adolescents from two distinct racial/ethnic groups. In a prospective survey design, 169 10th and 11th grade Vietnamese American and European American youth reported on their mental health need, as measured by emotional/behavioral mental health symptoms and stressful life events, with participants reporting on their help-seeking behavior at 6-month follow-up assessments. Multinomial logistic regression analyses indicated that mental health need interacted with cultural values and ethnicity to predict help-seeking behavior. Specifically, associations between symptoms and stressful life events, and help-seeking behavior were smaller among Vietnamese American adolescents, and among adolescents with strong family obligation values. These results underscore the complex sociocultural factors influencing adolescents’ help-seeking behavior, which have important implications for engaging youth in needed mental health care.
Keywords: help-seeking, adolescents, ethnic minority, family obligation, cultural values
The risk of developing a range of mental health problems increases markedly during adolescence, a period defined by the World Health Organization as the second decade of life (World Health Organization, 2001). However, most youth with need do not receive professional help (Wilson, Rickwood, & Deane, 2007) due to a variety of reasons, such as low mental health literacy, and stigma and embarrassment (Gulliver, Griffiths, & Christensen, 2010). Adolescents also may be deterred from seeking help by their strong need for privacy, increased desire for autonomy and self-reliance, and a fragile self-identity (Cauce et al., 2002). When young people do seek help, they tend to reach out to members of their informal social network with whom they are close, such as family and peers (Gulliver et al., 2010; Wilson et al., 2007) rather than seeking help from more formal sources (e.g., counselors; family physician). Given the gap between mental health need and service use during adolescence and the vital importance of early intervention, understanding factors that influence young people’s help-seeking patterns is an important step toward reducing the burden of mental illness.
Two models used for understanding adolescents’ help-seeking behaviors are the Andersen Behavioral Model (ABM) and the Theory of Reasoned Action (TRA). Both are based on the fundamental assumption that humans are rational decision makers, but each emphasizes a different aspect of the help-seeking process (c.f., Andersen & Davidson, 2007; Fishbein & Ajzen, 1975). The ABM focuses on predisposing, enabling, and need characteristics that influence individual health behaviors (Andersen & Davidson, 2007). Predisposing characteristics (e.g. demographic factors) increase or decrease the likelihood of individuals using health services, whereas enabling characteristics (e.g. resources and access to care) provide the means for individuals to obtain care (Andersen, 1995). Need characteristics refer to individuals’ assessment of the severity of their illness and their need for health care. Since the ABM was first introduced, a number of studies have found gender (Doherty & Kartalova-O’Doherty, 2010; Neighbors et al., 2007), ethnicity (Abe-Kim et al., 2007; Williams et al., 2007, Wang et al., 2005), and perceived need (Fleury, Ngui, Bamvita, Grenier, & Caron, 2014; Katz, Kessler, Frank, Leaf, & Lin, 1997) to be important determinants of help-seeking.
Although generally found to be useful for understanding help-seeking behavior, one limitation of the ABM is that it does not directly provide for a description of the influences of cultural norms on help-seeking. The Theory of Reasoned Action (TRA) does provide such a perspective for integrating cultural influences on help-seeking (Park & Levine, 1999). According to the TRA, individuals’ attitudes and subjective norms about (help-seeking) behavior influence their intention to perform the behavior, which in turn influences actual behavior (Fishbein & Ajzen, 1975). Through its focus on norms regarding behaviors and attitudes, the TRA suggests a direct linkage between cultural beliefs and values, and an individual’s intentions and help-seeking behaviors. Indeed, variables such as acculturation (Le Meyer, Zane, Cho, & Takeuchi, 2009), stigma tolerance (Ting & Hwang, 2009), and interdependent self-construal (Shea & Yeh, 2008) have been found to play an important role in the seeking of professional services.
The growing interest on identifying predictors of help-seeking such as culture is important, given the persistent racial/ethnic disparities in use of mental health services that have been identified (Department of Health and Human Services, 2001). One group that continues to under-utilize mental health services but has received relatively little research attention is Vietnamese Americans (Luu, Leung, & Nash, 2009; Nguyen & Anderson, 2005). Vietnamese Americans were one of the primary Southeast Asian refugee groups that settled in the U.S. following the end of the Vietnam War in 1975 (Zhou & Bankston, 1998). Consequently, mental health need among Vietnamese American adolescents is closely intertwined with the experiences of their parents as refugees. Intergenerational conflict, negotiating cultural identities, and the pressure of academic achievement are salient stressors for Vietnamese American youth (Ho, 2010). Research on Vietnamese American mental health has focused on documenting the prevalence of mental health needs (e.g. Birman & Tran, 2008; Ngo, Tran, Gibbons, & Oliver, 2001; Tran, 1993) and attitudes around help-seeking (e.g. Luu et al., 2009; Nguyen & Anderson, 2005; Lien, 1993). However, few studies have examined actual mental health help-seeking in this group (e.g. Abe-Kim et al., 2007; Steel et al., 2004; Phan, 2000), and to the best of our knowledge, no research has examined the influences of cultural values on actual help-seeking behaviors of Vietnamese American adolescents, which may play a central role in help-seeking decisions.
More generally, one specific cultural factor that may influence help-seeking is attitudes and beliefs about emotional restraint. Although used by most cultural groups (e.g., Gross & Thompson, 2007), the degree to which self-control over emotions is valued by different groups varies. For instance, in interdependent cultural groups such as Vietnamese Americans, in part because group concerns are weighted relatively more strongly than individual concerns, individuals are socialized to exercise restraint over the expression of strong emotions, especially negative valence emotions (Friedlmeier, Corapci, & Cole, 2011; Louie, Oh, & Lau, 2013). Individuals seek to maintain the group harmony through emotional restraint, rather than actively exert influence on the environment to fit their needs through emotional expression (Markus & Kitayama, 1991; Tsai et al., 2006); this may include not burdening others by seeking help or comfort (Kim & Omizo, 2003). Considerable evidence indicates that Asian Americans who value interdependence are less likely to seek support from friends and family in the face of distressing life circumstances (Kim, Sherman, & Taylor, 2008; Taylor et al., 2004; Wang, Shih, Hu, Louie, & Lau, 2010). Professional help is seen as a last resort and not likely to be sought (Kim & Omizo, 2003; Shea & Yeh, 2008).
In contrast, in independent cultures that emphasize the value of the individual and one’s own self-interest, emotions and their expression take on relatively greater intrapersonal value (Matsumoto, Yoo, & Fontaine, 2008). Emphasis is placed on the ability to assert oneself and gain autonomy, and open expression of emotions is encouraged in most situations as a way to assert the importance of individual needs (Markus & Kitayama, 1991). Cross-cultural research has found that individuals from independent cultures value emotion expression more than individuals from interdependent cultures (Matsumoto et al., 2008), and emotion suppression is used less often among individuals holding independent values relative to those holding more interdependent values (Butler, Lee, & Gross, 2007). Together, these findings suggest that attitudes and beliefs about the importance of emotion restraint vary as a part of cultural norms, with interdependent and independent cultures operating as opposing ends of a continuum.
Family obligation is another value that is strongly socialized among interdependent cultural groups that may influence help-seeking. For instance, it has been found that adolescents from families recently immigrated to the U.S. (who tend to be interdependent culturally; Phinney, Ong & Madden, 2000) tend to place more emphasis on helping, respecting, and contributing to one’s family than European American youth (Fuligni, Tseng, & Lam, 1999; Telzer & Fuligni, 2009). Family obligation can include focusing on academic achievement as a means for the youth to honor and repay their parents’ sacrifices, providing the youth with a sense of having fulfilled their role within the family (Fuligni & Witkow, 2004). In regards to help-seeking, individuals with a strong sense of family obligation may be less likely to seek support or help for personal concerns, as this could be perceived as placing one’s own needs over those of the family, or burdening their family with their troubles (Telzer & Fuligni, 2009). Taylor and colleagues (2004) found that decreased support seeking among Asian Americans relative to European Americans was linked in part to concerns about burdening or stressing personal relationships. Similar to emotional restraint, family obligation appears to operate along a continuum, with interdependent groups having higher value orientation and independent groups having lower value orientation (Fuligni et al., 1999).
Although other cultural constructs may play a role in mental health help-seeking, the present study focused on emotional restraint and family obligation because of their developmental relevance. Adolescence is a period during which hormonal, neural, and cognitive systems underlying emotion regulation are maturing (Silk, Steinberg, & Morris, 2003), and thus adolescents’ beliefs about emotion expression may be a particularly important predictor of help-seeking during this period of developmental change. Similarly, adolescence is a period marked by increased autonomy from the family and involvement with peers, and thus attitudes and beliefs toward their family may be of particular relevance during this shifting social environment (Fuligni et al., 1999).
The goal of the present study was to examine factors that potentially influence the help-seeking behavior of Vietnamese American and European American adolescents, two groups with significantly different cultures (e.g. Phinney & Ong, 2002). We focused on the most intensive source of help (e.g., peers, adults, or formal providers) sought by adolescents for mental health related problems. Based on the structure of the Andersen Behavioral Model (ABM), we examined as predictors of help-seeking predisposing or demographic characteristics and perceived mental health need. We were interested specifically in ethnicity as a predisposing characteristic of help-seeking but also included gender as a control variable to account for help-seeking differences commonly found between male and female youths (e.g., Sen, 2004; Chandra & Minkovitz, 2006). In the current study, perceived mental health need was defined by severity of mental health symptoms and exposure to stressful life events in the family, peer, and academic domains. To reflect the larger influences of subjective norms as outlined in the TRA, we examined beliefs about emotional restraint and family obligation as two prominent cultural determinants of help-seeking patterns. Lastly, we explored whether race/ethnicity moderated the association between need and help-seeking and if so, could cultural characteristics explain such racial/ethnic differences? Through examination of cultural beliefs and values as predictors of help-seeking, the current study aimed to identify more culturally proximal explanations of potential racial/ethnic differences, which is important given the limitations in the use of race and ethnicity as an explanatory construct (Cokley, 2007; Helms, Jernigan, & Mascher, 2005). Further, whereas previous studies have treated ABM and TRA models as additive and tested only main effects of model-related variables on health-related behaviors (Poss, 2001), we theorized that these variables may interact and shape the effect of one another on help-seeking behavior.
We hypothesized that being (a) European American, and (b) having greater levels of emotional/behavioral symptoms and stressful life events would be associated with a higher likelihood of seeking help from formal sources versus not seeking help (from any source). Based on the logic of the Theory of Reasoned Action (TRA), we hypothesized that cultural values (norms and attitudes within the larger cultural context) would predict help-seeking behavior above and beyond effects of predisposing characteristics and individual need. Specifically, we predicted a negative effect of emotional restraint and family obligation values on help-seeking in general, and formal help-seeking in particular. Given the well-documented racial/ethnic disparity in mental health service utilization (e.g., Garland et al., 2005), we hypothesized that the relation between indicators of mental health need and help-seeking would vary by race/ethnicity, with a smaller positive relation between need and formal help-seeking among Vietnamese American adolescents than European American adolescents. We also hypothesized that family obligation and emotion restraint values would function as moderators, reducing the magnitude of the positive relation between need and help-seeking. Finally, we assessed whether the cultural variables might act as mediators in the association between race/ethnicity and help-seeking, hypothesizing that Vietnamese ethnicity would predict higher orientation toward family obligation and emotional restraint, which in turn would predict lower likelihood of seeking support.
Method
Participants and Procedures
The present sample was part of a larger study examining cultural variation in stress experiences, coping, and mental health among Vietnamese American and European American 10th and 11th grade students. The four schools from which the current sample was recruited were ethnically diverse, with over three-fourth of enrolled students from ethnic minority groups, serving mixed lower- and middle-income communities with the percent of students qualifying for a free or reduced cost lunch ranging from 15.2% to 73.1%. Two of the schools were designated as Title I eligible.
Recruitment and sampling included three stages during the 2011–2012 academic school year. First, research assistants made brief announcements in all 10th and 11th grade classrooms in a given department (e.g., Social Studies; Science) to describe the study and distribute consent packets. Students were asked to return the packets with a signed parental consent form if they were interested in participating in the study. Small incentives (e.g., key chains, stress balls, snacks) were provided to individual students who returned forms irrespective of whether they were interested in participating in the project or not and to classrooms with the highest return rates. Return rates for the consent packets ranged from 30.3% to 37.3% across the schools, and among those who returned consent packets 12.1% declined participation. In schools with smaller numbers of eligible students, targeted recruitment via email was used. Second, a stratified random sample was selected from among those who provided parental consent to maximize the gender and ethnicity balance in the Time 1 (T1) survey. This resulted in a sample of 427 students with a mean age of 15.6 years (SD = .61) who completed the T1 survey in small groups at the school. Among the T1 survey group, 42.2% were male and 70.5% were Vietnamese American, and 29.5% were European American.
Third, from among the 427 students who completed the survey, 209 participants were selected for the two follow-up assessments. Given the high percentage of female and Vietnamese American students in the original sample, researchers invited all male and European American students to participate in the follow-up assessments in order to balance gender and ethnicity distribution in the prospective sample. Among female and Vietnamese American students in the baseline survey, we stratified our sample across low and high scores on the life events checklist to participate in follow-up assessments. T2 and T3 surveys were completed 3 and 6 months after the initial assessment. Of the 209 students who were followed prospectively, 187 completed assessment at T2 (10.5% attrition from T1), and 169 completed assessment at T3 (9.6% attrition from T2). Students received $20 and $25 retail gift cards for participation in the first and each of the follow-up assessments, respectively. In the current study, the longitudinal sample of 169 students was used. Of these participants, 58.6% (n= 99) were Vietnamese American and 41.4% (n=70) were European American, and 46.2% (n=78) were male.
Measures
Emotional/Behavioral Symptoms
Emotional and behavioral symptoms were assessed using the Youth Self Report at T1 (YSR; Achenbach & Rescorla, 2001). The YSR measures internalizing and externalizing psychopathology, with 112 items covering a range of emotional and behavioral problems (as well as several positive distractor items). Adolescents rate each item on a 0 (“not true”), 1 (“somewhat or sometimes true”), or 2 (“very true or often true”) Likert scale for symptoms over the past three months. In the current study, we used the YSR Total Problems T-score as an indicator of total emotional/behavioral symptoms. The YSR has shown good reliability and discriminative validity across a wide range of cultural groups (e.g., Groot, Koot, & Verhulst, 1996), including adolescents of Vietnamese descent (Chiu & Ring, 1998). Internal consistency for the current sample was high (overall sample: α = .89; European Americans: α = .87; Vietnamese Americans: α = .89).
Stressful Life Events
Exposure to stressful life events as a source of mental health need was measured at T1, using a revised version of the Adolescent Life Events Questionnaire (ALEQ; Hankin & Abramson, 2002). This version of the ALEQ assesses the occurrence of 70 negative life events, including academic/achievement problems (e.g., “you didn’t make the honors roll when you wanted to”), friendship difficulties (e.g., “you had an argument with a close friend”), and family problems (e.g., “your parents put you down”). Counts of events in each of these three domains were used as an indicator of mental health need (Bird et al., 1996). The ALEQ has been found to be a reliable and valid measure, including among Asian adolescents (Cohen et al., 2013). For these scales, we did not compute internal consistency estimates. Life event scales often have been conceptualized as representing formative rather than reflective factors (e.g., Miller, 1989), which means that scale items are not indicators of a latent factor but rather are combined to create a formative factor. High correlations between items of a formative scale generally are not expected, and thus Cronbach’ alpha may be misleading as indicator of reliability (Bollen, 1989).
Family obligation values
At T1 the Adolescents’ Attitudes toward Family Obligation scale was used to measure the adolescents’ sense of family obligation (Fuligni et al., 1999). The measure assesses attitudes about the family associated with interdependent cultural contexts in several domains. The Current Assistance domain assesses the frequency with which adolescents assist their families with household tasks (e.g., “help take care of your brothers and sisters”). The Respect domain assesses the extent to which the adolescents respect and follow the wishes of family elders (e.g., “show great respect for your parents”). The Future Support domain assesses obligation to support the family in the future (e.g., “help your parents financially in the future”). In the present study the total score was used to measure family obligation (overall sample: α = .78; European Americans: α = .73; Vietnamese Americans: α = .78). The Family Obligation scale shows good reliability and validity with Asian American and European American adolescents (Fuligni et al., 1999).
Emotional restraint values
Emotional restraint was assessed at T1 using the 6-item Emotional Restraint scale. The Emotional Restraint (ER) scale was developed for the present study based on a literature review and on the Emotional Self-Control subscale of the Asian American Values Scale-Multidimensional (AAVS-M; Kim, Li, & Ng, 2005), which has demonstrated reliability and validity for both European American and Asian American samples (e.g., Park & Kim, 2008). In the ER scale, participants are asked to rate on a 6-point Likert scale how much they agree or disagree with a series of statements describing restraint in emotional expression (e.g., “Showing emotion is a sign of weakness”). A principal axis exploratory factor analysis indicated that a single factor underlay the six-item scale. The construct validity of the ER was assessed by assessing relations with avoidant coping, which is conceptually related to emotional restraint (Kashdan, Barrios, Forsyth, & Steger, 2006). We found significant positive relations between the ER scale and the Children’s Coping Strategies Checklist (Ayers, Sandier, West, & Roosa, 1996), for the overall sample (r = .53), European Americans (r = .61) and Vietnamese Americans (r = .45); all p <.001. Internal consistency estimates for the current sample were satisfactory, for the overall sample (α = .73), European Americans (α =.81), and Vietnamese Americans (α = .65).
Help-seeking behavior
Participants completed a modified version of the General Help-Seeking Questionnaire (GHSQ; Wilson, Deane, Ciarrochi, & Rickwood, 2007) at T3 (6-month follow-up)1. In the modified questionnaire, adolescents’ past year help-seeking behavior were assessed. Specifically, students were asked to endorse whether they have sought help from a list of potential support sources using a binary scale of “yes” or “no”. Potential support sources included a friend, significant other, parents, teacher, mental health professional (e.g., counselor, psychologist, and social worker), doctor, and religious/spiritual leader. Past research has shown that the GHSQ is reliable and valid for a range of youth, including adolescents of Asian descent (Moran, 2007). In the current study, an exploratory factor analysis identified three factors from the list of support sources: formal provider (medical or mental health professionals), adult (parent, teacher or spiritual leader), and peer (significant other or friend). Based on these results and our a priori focus on the relative intensity of these different sources of support, we constructed a 4-level multinomial outcome variable (GHSQ-4) reflecting the most intensive level of help sought: (1) no support sought, (2) peer support (i.e., sought support from peers but no one else), (3) adult support (i.e., sought help from adults but not formal professional help), and (4) formal support (regardless of whether adult or peer support was sought). Thus, each participant was categorized into 1 of the 4 levels of highest level of intensity support sought. This multinomial classification allowed us to make meaningful distinctions between types of help-seeking that vary in intensity.
Analyses
We used multinomial logistic regression to examine the effects of the ethnicity, mental health need, and cultural values on intensity of help-seeking (i.e., the GHSQ-4 help-seeking variable collected at T3). Three log odds ratios were computed from the GHSQ-4 with “no support” as the reference category. We hierarchically tested sets of predictors: (a) demographic variables (ethnicity, gender) as base control variables; (b) mental health need (i.e., emotional/behavioral symptoms, family, academic and peer stressful life events) at T1; and (c) cultural values (emotional restraint and family obligation values) at T1. To assess moderation effects we ran two separate models that included (d) interaction terms. The interaction models tested two sets of interaction terms: (a) ethnicity X emotional/behavioral symptoms and (b) ethnicity X peer stressful life events, ethnicity X family stressful life events, ethnicity X academic stressful life events. Given the conceptual challenges of assessing ethnic effects based on participants’ self-identification (Cokley, 2007; Helms et al., 2005), we assessed effects of the cultural variables as factors underlying potential racial/ethnic differences in help-seeking using two different approaches. First, ethnicity was replaced in separate sets of models with the two cultural values variables as potential moderators: (c1) emotion restraint X emotional/behavioral symptoms, (c2) family obligation X emotional/behavioral symptoms; and (d1a) emotion restraint X peer stressful life events, (d1b) emotion restraint X family stressful life events, (d1c) emotion restraint X academic stressful events, (d2a) family obligation X peer stressful events, (d2b) family obligation X family stressful events, (d2c) family obligation X academic stressful events.
A second approach used to identify cultural factors underlying potential racial/ethnic differences was tests of mediation, with family obligation and emotional restraint entered as potential mediators of the association between ethnicity and help sources. Given that there are no established statistical techniques for the treatment of indirect effects when the dependent variable is multinomial, we converted our dependent variable GHSQ-4 to two separate binomial variables in order to retain the entire sample: a) formal support vs. all other supports (i.e., adult, peer, and no support), and b) formal and adult support vs. peer and no support. Comparison of more intensive supports with lower supports ensured there is sufficient power to detect significant results in mediation. All mediation analyses were conducted using 5000 bootstrap samples to estimate the confidence intervals for the indirect effects of family obligation and emotional restraint (Preacher & Hayes, 2004).
All predictor variables were mean-centered prior to computing cross-products to reduce multi-collinearity (Jaccard, Wan, & Turrisi, 1990). To compare the fit of the different models in the hierarchical multinomial logistic regression, we used two model-selection statistics. The first was Akaike’s Information Criterion (AIC) (Akaike, 1987). A model with a lower AIC is considered more plausible than one with a higher AIC. The second model-selection statistic was the chi-square difference (likelihood ratio) test (Bentler & Bonett, 1980). A significant chi-square difference test suggests the constraints of the more restricted model may be too stringent. Listwise deletion of missing data was used in inferential analyses, with 3 (2%) to 5 (3%) participants dropped.
Results
Preliminary Analyses
Figure 1 presents the raw (i.e., not the highest level of support) percentages of students who sought help from a friend, significant other, parent, teacher, spiritual leader, doctor, mental health professional, or no one earlier during the academic year. In Table 1, these percentages were converted into the four mutually exclusive categories of the highest intensity of help sought: (1) no support, (2) peer support, (3) adult support, or (4) formal support. Across the total sample of 169 youths, (1) 11% reported seeking help from no one, (2) 30% reported peer support as the highest intensity of help sought, (3) 50% reported adult support was the highest intensity of help sought, and (4) 7% sought formal support.
Figure 1.
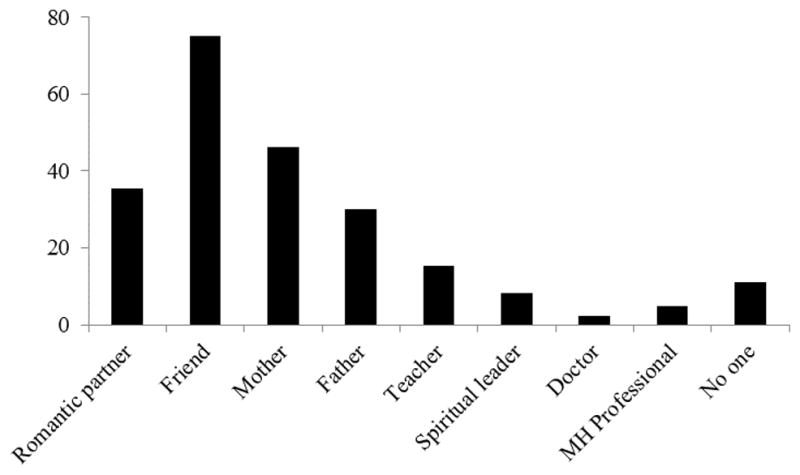
Frequency of help-seeking by sources of support.
Table 1.
Ethnic differences in mental health need, cultural values and help seeking
| Variables | European American | Vietnamese American | Analysis results | |||
|---|---|---|---|---|---|---|
| M (SD) | n (%) | M (SD) | n (%) | Significance test | Effect size | |
| Mental health need | ||||||
| Total problems | 57.26 (9.32) | 62.38 (10.23) | F(1,167)=11.07** | d = −0.52 | ||
| Family stress | 6.06 (4.03) | 9.04 (4.58) | F(1,166)=19.17*** | d =−0.69 | ||
| Academic stress | 3.61 (1.79) | 4.69 (2.07) | F(1,167)=12.27** | d =−0.55 | ||
| Peer stress | .84 (1.27) | 1.39 (1.58) | F(1,167)=5.86* | d =−0.38 | ||
|
| ||||||
| Cultural values | ||||||
| Family obligation | 3.07 (.56) | 3.45 (.52) | F(1,166)=19.62*** | d =−0.69 | ||
| Emotional restraint | 20.54 (5.71) | 21.70 (4.79) | F(1,167)=2.03 | d = −0.22 | ||
|
| ||||||
| Highest intensity of support sought | χ2(3) = 12.06** | φc = 0.27 | ||||
| None | 7 (10.1%) | 12 (12.4%) | ||||
| Peer | 12 (17.4%) | 39 (40.2%) | ||||
| Adult | 43 (62.3%) | 42 (43.3%) | ||||
| Formal | 7 (10.1%) | 4 (4.1%) | ||||
Note:
p <.05,
p <.01,
p <.001.
Cohen’s d and Cramer’s V are used to measure effect size of ANOVA and chi-square results, respectively.
Vietnamese American students had significantly higher levels of mental health need compared to European Americans; i.e., they reported significantly higher levels of emotional/behavioral symptoms, and significantly more stressful life events in all three stressful life event domains (family, peer, academic) relative to European Americans (see Table 1). Vietnamese American students reported significantly higher levels of family obligation than European Americans but the two groups did not differ significantly in regards to emotion restraint values.
Predictors of Help-seeking Behavior
In the first step of the multinomial logistic regression analyses, we entered the demographic and background variables into the model, with help-seeking behavior as the dependent variable. The demographic factors accounted for 6% of variability in the dependent variable (pseudo R2 = .06). The likelihood ratio test indicated that inclusion of the demographic characteristics significantly improved the model fit relative to the null model, χ2(6) = 23.54, p <.001. Next, we examined the extent to which mental health need incrementally predicted help-seeking, beyond effects of the demographic variables. The second model accounted for 16% of variability in help-seeking sources (pseudo R2 = .16). The likelihood ratio test indicated that the mental health need variables significantly increased model fit, χ2(12) = 37.09, p <.001. In the third step of the model, we assessed the incremental value of the cultural values. This model accounted for 18% variability in help-seeking sources (pseudo R2 = .18) but this third model did not provide a significantly improved fit relative to the previous model. Model statistics are shown in Table 2.
Table 2.
Summary of main effects from hierarchical multinomial logistic regression models for help seeking sources
| Individual Factor Statistics | Overall Model Statistics | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Highest intensity of support sought: | No Help vs. Formal | No Help vs. Adult | No Help vs. Peer | Fit index | ||||||||
|
|
||||||||||||
| Predictors | b | SE | OR | b | SE | OR | b | SE | OR | Pseudo R2 | AIC | Likelihood ratio test |
| Demographic variables | 0.06 | 370.70 | χ2 [6]= 23.54*** | |||||||||
| Gender | 3.01** | 1.15 | 20.37** | 1.62* | 0.63 | 5.03* | 1.58* | 0.66 | 4.83* | |||
| Ethnicity | −3.23** | 1.17 | .04** | −1.02 | 0.66 | 0.36 | 0.36 | 0.70 | 1.44 | |||
| Mental health need | 0.16 | 357.61 | χ2 [12]= 37.09*** | |||||||||
| Emotional/behavioral symptoms | −0.01 | 0.06 | 0.99 | 0.01 | 0.03 | 1.01 | 0.04 | 0.03 | 1.04 | |||
| Family stress | 0.03 | 0.15 | 1.03 | 0.02 | 0.09 | 1.02 | −0.04 | 0.09 | 0.96 | |||
| Academic stress | 1.20** | 0.41 | 3.32** | −0.02 | 0.19 | 0.97 | 0.11 | 0.20 | 1.12 | |||
| Peer stress | 0.01 | 0.34 | 1.01 | 0.15 | 0.22 | 1.16 | −0.08 | 0.23 | 0.92 | |||
| Cultural values | 0.18 | 359.12 | χ2 [6]= 10.50 | |||||||||
| Family obligation | 0.84 | 0.91 | 2.32 | 0.95 | 0.51 | 2.59 | 0.49 | 0.53 | 1.63 | |||
| Emotional restraint | 0.05 | 0.10 | 1.05 | −0.10 | 0.05 | 0.91 | −0.05 | 0.06 | 0.95 | |||
Note:
p <.05,
p <.01,
p <.001.
Pseudo R2 is measured by McFadden’s R2.
Table 2 also reports the effects of individual factors (e.g., ethnicity, within the demographic variables) on the individual logits (e.g., no help vs. formal help). European American adolescents and adolescents with a higher number of academic stressful life events were more likely to seek help from formal sources. Females were more likely than males to seek support from formal providers, adults, and peers, supporting the inclusion of gender as a covariate in the models. Neither family obligation nor emotional restraint were significantly associated as main effects with help-seeking behaviors.
We next tested whether ethnicity moderated the effect of the mental health need indicators (with emotional/behavioral symptoms, and stressful life events evaluated in separate models) on help-seeking behavior. As shown in Table 3, two interaction effects were significant in these analyses. First, ethnicity interacted with emotional/behavioral symptoms to predict formal help-seeking. As YSR Total Problems increased from low to high levels, the probability that European American but not Vietnamese American adolescents sought formal help increased substantially (see Figure 2a). Second, the ethnicity by family stressful life events interaction predicted formal help-seeking, with the pattern of the interaction similar to that of the Ethnicity X Emotional/behavioral Symptoms interaction: As the number of family stressful life events increased from low to high levels, European American but not Vietnamese American youth were more likely to seek help from a medical or mental health professional (see Figure 2b).
Table 3.
Summary of interaction effects from hierarchical multinomial logistic regression models for help seeking sources
| Individual Factor Statistics | Overall Model Statistics | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Highest intensity of support sought: | No Help vs. Formal | No Help vs. Adult | No Help vs. Peer | Fit index | ||||||||
| Predictors | b | SE | OR | b | SE | OR | b | SE | OR | Pseudo R2 | AIC | Likelihood ratio test |
| Model 1 | 0.22 | 351.06 | χ2^ [3]= 14.07** | |||||||||
| Eth x Emo/beh symptoms | −0.55* | 0.23 | 0.58* | 0.05 | 0.06 | 1.05 | −0.02 | 0.07 | 0.98 | |||
| Model 2 | 0.25 | 351.87 | χ2^ [9]= 25.25** | |||||||||
| Eth x Family stress | −.85* | 0.42 | 0.43* | 0.19 | 0.21 | 1.21 | −0.23 | 0.23 | 0.79 | |||
| Eth x Academic stress | −0.55 | 1.00 | 0.58 | −0.09 | 0.46 | 0.92 | −0.29 | 0.51 | 0.75 | |||
| Eth x Peer stress | −0.05 | 1.30 | 0.95 | −1.47 | 0.99 | 0.23 | 0.14 | 1.16 | 1.16 | |||
| Model 3 | 0.19 | 368.62 | χ2^ [6]= 2.50 | |||||||||
| Fam Obligation x Emo/beh symptoms | −0.04 | 0.09 | 0.96 | 0.01 | 0.05 | 1.01 | <.01 | 0.05 | 1.00 | |||
| Emo Restraint x Emo/beh symptoms | <.01 | 0.01 | 1.00 | <.01 | <.01 | 1.00 | <.01 | <.01 | 1.00 | |||
| Model 4 | 0.25 | 369.82 | χ2^ [18]= 25.30 | |||||||||
| Fam Obligation x Family stress | −0.76* | 0.34 | 0.47* | −0.06 | 0.15 | 0.94 | −0.16 | 0.16 | 0.85 | |||
| Fam Obligation x Academic stress | 1.28 | 0.82 | 3.58 | −0.17 | 0.36 | 0.84 | −0.03 | 0.36 | 0.97 | |||
| Fam Obligation x Peer stress | −2.40 | 1.24 | 0.09 | −0.36 | 0.59 | 0.70 | −0.28 | 0.61 | 0.76 | |||
| Emo Restraint x Family stress | 0.05 | 0.04 | 1.05 | −0.01 | 0.02 | 0.99 | −0.02 | 0.02 | 0.98 | |||
| Emo Restraint x Academic stress | −0.25 | 0.14 | 0.78 | <.01 | 0.05 | 1.00 | −0.03 | 0.05 | 0.97 | |||
| Emo Restraint x Peer stress | −0.07 | 0.11 | 0.93 | −0.08 | 0.06 | 0.92 | −0.05 | 0.06 | 0.95 | |||
Note:
p <.05,
p <.01,
p <.001.
Pseudo R2 is measured by McFadden’s R.2
Likelihood ratio test conducted against AIC fit index of multivariate model with demographic variables, mental health need and cultural values.
Fam Obligation=Family Obligation scale. Emo Restraint=Emotional Restraint scale.
Figure 2.

Figure 2a. Probability of formal help-seeking as a function of total symptoms and race/ethnicity.
Note: Panels A, B and C depict simple effects of ethnicity at −1SD, mean, and +1SD total symptoms, respectively (European American is the reference group). −1SD: Diff = .15, SE = .06, p =.02; Mean: Diff = −.04, SE = .05, p = .43; +1SD: Diff = −.26, SE = .08, p = .001.
Figure 2b. Probability of formal help-seeking as s function of family stressful events and race/ethnicity.
Note: Panels A, B and C depict simple effects of ethnicity at −1SD, mean, and +1SD family stressful events, respectively (European American is the reference group). −1SD: Diff = .09, SE = .07, p = .21; Mean: Diff = −.03, SE = .05, p= .51; +1SD: Diff = −.22, SE = .08, p = .004.
Figure 2c. Probability of formal help-seeking as s function of family stressful events and family obligation.
Note: Panels A, B and C depict simple effects of family obligation at −1SD, mean, and +1SD family stress, respectively. −1SD: DiffModerate vs. low obligation =.007, SE=.005, p=.12; DiffHigh vs. low obligation =.05, SE = .02, p=.03, DiffHigh vs. moderate obligation = .04, SE = .02, p =.04; Mean: DiffModerate vs. low obligation = .003, SE = .009, p = .34; DiffHigh vs. average obligation =.03, SE = .02, p = .03; DiffHigh vs. low obligation = .04, SE = .02, p = .06; +1SD: DiffModerate vs. low obligation = .05, SE= .05, p = .28, DiffHigh vs. low obligation = −.06, SE = .07, p =.38, DiffHigh vs. average obligation =−.008, SE = .03, p =.76
When we replaced ethnicity with cultural values as moderator in the association between need and help-seeking, only one interaction term was significant across the two models (Models 3 and 4 in Table 3). Family obligation values moderated the effect of negative family stressful events on formal help-seeking versus no help. As shown in Figure 2c, as levels of family stress rose from low to high, the likelihood of seeking help from formal sources increased among adolescents with lower levels of family obligation (i.e., one standard deviation below the mean of family obligation scores). However, adolescents with high levels (i.e., one standard deviation above the mean) of family obligation values did not show increased formal help-seeking as a function of family stress.
We also assessed the extent to which potential cultural factors were responsible for racial/ethnic differences by conducting mediational analyses. However, controlling for gender and mental health need, neither family obligation nor emotional restraint measured at T1 were significant mediators in the link between ethnicity and each of the two help-seeking outcomes: a) formal vs. all other supports (Family Obligation: Indirect effect = .061, Bootstrapped SE = 1.13, 95% CI = −1.61 – 3.20; Emotional Restraint: Indirect effect = .012, Bootstrapped SE = .23, 95% CI = −.33 – .66), and b) formal and adult support vs. peer and no support (Family Obligation: Indirect effect = .25, Bootstrapped SE = .16, 95% CI = −.02 – .60; Emotional Restraint: Indirect effect = −.005, Bootstrapped SE = .062, 95% CI = −.17– .09).
Discussion
The central finding from our study is that, as has been found with a number of other Asian American groups (e.g., Cummings & Druss, 2011), there is a mental health help-seeking disparity for Vietnamese American versus European American adolescents. The probability of seeking formal help (e.g., from a counselor) versus no help was significantly lower for the Vietnamese American than European American adolescents (Table 2). Other of our results indicate that this reduced receipt of formal sources of mental health support was not due simply to a lower mental health need, as the Vietnamese American adolescents showed significantly higher mental health need across all four indicators of this construct (i.e., emotional and behavioral problems, and stressful life events); this suggests that other factors differentiating the groups are responsible for these effects. Past studies of mental health service usage disparity (e.g., Department of Health and Human Services, 2001) have found similar results on formal help seeking but our results also suggest that this disparity may not be as substantial in relation to other sources of mental health support. A key question is the extent to which these other, less formal sources of support are useful for addressing the adolescents’ mental health challenges.
From a public health perspective, as health needs increase service usage should increase, so as to most efficiently support population health (Boylan, 2007). We found that European American but not Vietnamese American adolescents followed this pattern: As the level of mental health need increased (as assessed by self-reports of emotional and behavioral problems, and family stressful life events) above the mean, the probability of European American but not Vietnamese American adolescents seeking formal mental health support increased (Figures 2a, 2b). Other of our results suggest some of the cultural factors that may underlie these results. Across the two ethnic groups, we found that there was a significant interaction between adolescents’ reports of family obligation, and the effects of family life events: As the frequency of family stressful life events increased above the mean, for adolescents low on family obligation but not for adolescents high on family obligation the probability of seeking formal mental health support increased. This suggests that their sense of family obligation may have prevented these adolescents from seeking help from formal sources. The fact that Vietnamese American adolescents were significantly higher on family obligation than European American adolescents suggests this family obligation may be one factor underlying the Vietnamese American and European American differences in response to increased mental health need. It is interesting to note, and supports the validity of this interpretation, that it was only family-related stressful life events and not peer- or academic-related stressful life events that showed this pattern.
The raw frequencies (i.e., not converted to logits) of sources also provide an interesting perspective. Whereas approximately 17% of European American adolescents had peers as their highest intensity of support sought versus 61% had adults as the highest intensity support, for Vietnamese American adolescents about 39% had peers as their highest level of support versus 43% had adults as the highest level of support (see Table 1). One way of conceptualizing this result is that Vietnamese American adolescents are more likely to “stop” at the peer level of support than European American adolescents, but do not differ overall in help-seeking (i.e., the rates of No Help-seeking did not differ significantly between the two ethnic groups).
The fact that the only indicator of mental health need found to be a significant predictor of formal help seeking relative to not seeking any help was academic stressful events is consistent with previous studies that have found a strong link between academic problems and referral and entrance into formal mental health care (Guo, Kataoka, Bear, & Lau, 2014; Zwaanswijk, Verhaak, Bensing, Ende, & Verhulst, 2003). Interestingly, family stress was not a significant predictor of formal help-seeking despite the high levels of family-related stressful events reported by youth. This finding is somewhat at odds with previous research that highlighted the prominent effect of family conflict and parental burden on children’s mental health service use (e.g., Logan & King, 2001). However, it is important to note that family conflict and burden in those studies were based on parent report, whereas the current one relied on youth’s self-report. Given that adults are often the gatekeepers to providing consent and funding for youths to access mental health services, adolescents’ experience of family stress may not hold the same predictive power as parents’ recognition of family stress.
Neither family obligation nor emotional restraint values were significant main effect predictors of help-seeking. Although these findings are inconsistent with our hypothesis of main effects of cultural values, it is in line with the emerging body of research on the complex nature of help-seeking processes. Cauce and colleagues (2002) point out that there is a dynamic interaction between characteristics of the larger social environment and individual mental health problems and concerns. Indeed, there were significant interaction effects identified in our study. First, ethnicity moderated the positive association between indicators of mental health need and formal help-seeking. As stressful life events or symptoms increased, European Americans’ likelihood of seeking help from medical or mental health professionals increased whereas Vietnamese Americans’ likelihood remained low. Such patterns of behavior is of concern given that Vietnamese American youth reported consistently higher level of need relative to European Americans. Once believed to be the model minority with few adjustment problems, Asian American youth such as Vietnamese Americans have been identified as a vulnerable group with high level of unmet mental health need (e.g., Guo et al., 2014; Ting & Hwang, 2009). This finding highlights a common concern in mental health disparities, that need alone does not explain help-seeking for particular cultural groups. Specifically, for ethnic minority and immigrant youth, indices of need are less strongly related to receipt of care than for European American and U.S.-born families (Gudiño, Martinez, & Lau, 2012).
To better understand what underlies the help-seeking behaviors in these two ethnic groups, we examined how cultural values were related to help-seeking. Contrary to our hypothesis, family obligation and emotional restraint orientations did not mediate the association between race/ethnicity and help-seeking. European and Vietnamese American youth may have differed along other cultural values that in turn affected help-seeking, such as stigma tolerance (Ting & Hwang, 2009) and beliefs about mental illness (Nguyen & Anderson, 2005). Future studies may wish to explore the explanatory power of these variables for adolescents.
Although cultural characteristics did not explain ethnic differences in help-seeking, they were involved in the link between mental health need and help-seeking. In particular, family obligation attenuated the effect of family stress on formal help-seeking. The few studies on family obligation thus far have found a positive link to educational and emotional well-being (Fuligni & Pedersen, 2002; Fuligni, Yip, & Tseng, 2002). Our finding, however, suggests that such an internalized sense of duty to the family may have an indirect negative impact on well-being by deterring youths from seeking the formal mental health support they need, particularly when problems arise within the family. By isolating family obligation values as a more culturally proximal moderator, we moved closer to cultural explanations of group-based disparities. That is, we narrowed in on a particular attribute of Vietnamese-American group that may place adolescents at risk of unmet need.
Across these interactions, racial/ethnic differences in help-seeking behavior only emerged when symptoms or stress was high. This is understandable given that at low levels of need, youth are less likely to seek support regardless of their ethnicity or value orientation. More interestingly, racial/ethnic differences in help-seeking concentrated around formal support. Previous research point out that a number of cultural, affective, and cognitive barriers deter Asian Americans from seeking support from professionals, including misunderstanding of problem conception (Leong, Kim, & Gupta, 2011; Leong & Lau, 2001), distrust or stigma of mental health services (Gary, 2005; Lee et al., 2009), and lack of awareness for treatment options (Abe-Kim, Takeuchi, & Hwang, 2002). Our results lend support to the notion that formal and informal help-seeking may have distinct pathways as Vietnamese Americans did not shy away from general support relative to their European American peers, but relatively infrequently sought help from adults or formal providers.
These findings have several implications for outreach and intervention efforts. The mental health needs of adolescents are best served when available programs are congruent with their values and help-seeking preferences. For instance, family obligation appears to play an important role in youth entry into mental health services. As such, engagement and intervention efforts that acknowledge both the needs of the family and the individual may help adolescents and their parents strike a better balance between contributing to the family and attending to one’s personal concerns. Given that adolescents across racial/ethnic groups were more willing to ask for support from adult social network figures such as parents and teachers rather than formal providers, one approach to increase utilization of mental health care is for such gatekeepers to receive more comprehensive psychoeducation about mental health, and about treatment options and when and how to make referrals. Knowledge about the presentation and consequences of adolescent stress and symptoms can help parents and school staff better identify students in need of mental health services (Kelly, Jorm, & Wright, 2007). As conduits to care, these gatekeepers can help students navigate through the mental health system better if they have appropriate information about how to make referrals and follow-up about linkage to services. Psychoeducation may prove especially useful for improving problem detection and access to services for Asian Americans as referral rates have been notably low among this population relative to other racial/ethnic groups (Guo et al., 2014).
There are several limitations that should be considered when evaluating our results. First, although the study used a prospective design to measure factors that longitudinally predicted help-seeking behaviors, adolescents were asked to recall the help they had sought over the past school year; the length of this recall period may potentially have resulted in recall bias. Second, although the exploratory factor analysis identified clear factors of help-seeking support (peers, adults, formal providers), in each category there was more than one class of persons. It is possible that help-seeking behavior varies as a function of these sub-sources, and thus it may be useful for future studies to assess whether factors related to selection of, say, teachers versus parents differ. Although we found family obligation as a moderator of the link between family stress and help-seeking, there were no other interactions between cultural values and mental health need dimensions. It is possible that emotional restraint as a cultural value was not well captured by the newly developed measure, although it was validated against an accepted measure of a related construct. While the current study focused on adolescent mental health decision-making, formal help-seeking is likely influenced by both attitudes of the child and the surrounding caregivers. As such, more research is needed to disentangle the relative contribution that adolescents and adult gatekeepers make in the decision to seek formal mental health care. Finally, participants were categorized in regards to ethnicity based on self-identification, and thus results reflect their perceptions of their ethnicity (Cokley, 2007). Although self-perceptions are an important factor in such constructs, it may be useful for future studies to include other approaches to assessing ethnicity (e.g., Helms et al., 2005).
To summarize, our results indicate that mental health need alone does not explain adolescent mental health help-seeking, nor in our sample did it explain ethnic or cultural differences in help-seeking. Cultural factors such as family obligation may play an important role in adolescents’ decisions to seek formal help for mental health problems and indicate the dynamic interaction between adolescent distress and the sociocultural norms that influence youth. Consideration of family-based factors – both in terms of manifested stress and internalized beliefs and attitudes – seems particularly central to understanding pathways into care for adolescents.
Acknowledgments
This research is supported by grants from the National Institute of Mental Health to Bahr Weiss and the UCLA Asian American Studies Center to Anna Lau.
Footnotes
The original General Help-Seeking Questionnaire asks participants to rate their help-seeking intentions on a 7-point scale ranging from 1 “extremely unlikely” to 7 “extremely likely” for each source help source. The current study modified the original scale by measuring actual help-seeking behavior instead of intentions. As such, a binary scale of “yes” or “no” were used to assess whether particular help sources were sought.
Contributor Information
Sisi Guo, University of California, Los Angeles.
Hannah Nguyen, University of California, Los Angeles.
Bahr Weiss, Vanderbilt University.
Victoria Ngo, RAND Corporation.
Anna S. Lau, University of California, Los Angeles
References
- Abe-Kim J, Takeuchi DT, Hong S, Zane N, Sue S, Spencer MS, Alegría M. Use of mental health-related services among immigrant and US-born Asian Americans: results from the National Latino and Asian American Study. American Journal of Public Health. 2007;97(1):91–98. doi: 10.2105/AJPH.2006.098541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abe-Kim J, Takeuchi D, Hwang WC. Predictors of help-seeking for emotional distress among Chinese Americans: Family matters. Journal of Consulting and Clinical Psychology. 2002;70(5):1186–1190. http://dx.doi.org/10.1037/0022-006X.70.5.1186. [PubMed] [Google Scholar]
- Achenbach TM, Rescorla L. ASEBA School-Age Forms & Profiles. Burlington: Aseba; 2001. [Google Scholar]
- Akaike H. Factor analysis and AIC. Psychometrika. 1987;52(3):317–332. doi: 10.1007/BF0229435. [DOI] [Google Scholar]
- Andersen RM. Revisiting the behavioral model and access to medical care: Does it matter? Journal of Health and Social Behavior. 1995;36(1):1–10. 9. [PubMed] [Google Scholar]
- Andersen RM, Davidson PL. Improving access to care in America: Individual and contextual indicators. In: Anderson RM, Rice TH, Kominski GF, editors. Changing the US health care system: Key issues in health services policy and management. San Francisco: John Wiley & Sons, Inc; 2007. pp. 3–32. [Google Scholar]
- Ayers TS, Sandier IN, West SG, Roosa MW. A dispositional and situational assessment of children’s coping: testing alternative models of coping. Journal of Personality. 1996;64(4):923–958. doi: 10.1111/j.1467-6494.1996.tb00949.x. [DOI] [PubMed] [Google Scholar]
- Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychological bulletin. 1980;88(3):588. [Google Scholar]
- Bird HR, Andrews H, Schwab-Stone M, Goodman S, Dulcan M, Richters J, Gould MS. Global measures of impairment for epidemiologic and clinical use with children and adolescents. International Journal of Methods in Psychiatric Research. 1996;6(4):295–307. doi: 10.1002/(SICI)1234-988X(199612)6:4<295::AID-MPR173>3.3.CO;2-5. [DOI] [Google Scholar]
- Birman D, Tran N. Psychological distress and adjustment of Vietnamese refugees in the United States: Association with pre-and postmigration factors. American Journal of Orthopsychiatry. 2008;78(1):109. doi: 10.1037/0002-9432.78.1.109. [DOI] [PubMed] [Google Scholar]
- Bollen KA. Structural equations with latent variables. Hoboken, NJ: Wiley-Interscience; 1989. [Google Scholar]
- Boylan M. Theory and research in promoting public health. Thousand Oaks, CA: Sage Publications; 2007. [Google Scholar]
- Butler EA, Lee TL, Gross JJ. Emotion regulation and culture: Are the social consequences of emotion suppression culture-specific? Emotion. 2007;7(1):30–48. doi: 10.1037/1528-3542.7.1.30. [DOI] [PubMed] [Google Scholar]
- Cauce AM, Domenech-Rodríguez M, Paradise M, Cochran BN, Shea JM, Srebnik D, Baydar N. Cultural and contextual influences in mental health help-seeking: A focus on ethnic minority youth. Journal of Consulting and Clinical Psychology. 2002;70(1):44–55. doi: 10.1037/0022-006X.70.1.44. [DOI] [PubMed] [Google Scholar]
- Chandra A, Minkovitz CS. Stigma starts early: Gender differences in teen willingness to use mental health services. Journal of Adolescent Health. 2006;38(6):754–e1. doi: 10.1016/j.jadohealth.2005.08.011. [DOI] [PubMed] [Google Scholar]
- Chiu YW, Ring JM. Chinese and Vietnamese immigrant adolescents under pressure: Identifying stressors and interventions. Professional Psychology: Research and Practice. 1998;29(5):444–449. doi: 10.1037/0735-7028.29.5.444. [DOI] [Google Scholar]
- Cohen JR, Young JF, Hankin BL, Yao S, Zhu XZ, Abela JRZ. Personality predispositions in Chinese adolescents: The relation between self-criticism, dependency, and prospective internalizing symptoms. Journal of Social and Clinical Psychology. 2013;32(6):596–618. doi: 10.1521/jscp.2013.32.6.596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cokley K. Critical issues in the measurement of ethnic and racial identity: A referendum on the state of the field. Journal of Counseling Psychology. 2007;54(3):224–234. http://dx.doi.org/10.1037/0022-0167.54.3.224. [Google Scholar]
- Cummings JR, Druss BG. Racial/ethnic differences in mental health service use among adolescents with major depression. Journal of the American Academy of Child & Adolescent Psychiatry. 2011;50(2):160–170. doi: 10.1016/j.jaac.2010.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Department of Health and Human Services. Mental Health: Culture, race, and ethnicity - A supplement to mental health: A report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services; 2001. [PubMed] [Google Scholar]
- Doherty DT, Kartalova-O’Doherty Y. Gender and self-reported mental health problems: Predictors of help-seeking from a general practitioner. British journal of health psychology. 2010;15(1):213–228. doi: 10.1348/135910709X457423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Beliefs, attitude, intention, and behavior: An introduction to theory and research. Reading, MA: Addison-Wesley; 1975. [Google Scholar]
- Friedlmeier W, Corapci F, Cole PM. Emotion socialization in cross-cultural perspective. Social and Personality Psychology Compass. 2011;5(7):410–427. doi: 10.1111/j.1751-9004.2011.00362.x. [DOI] [Google Scholar]
- Fleury MJ, Ngui AN, Bamvita JM, Grenier G, Caron J. Predictors of healthcare service utilization for mental health reasons. International Journal of Environmental Research and Public Health. 2014;11(10):10559–10586. doi: 10.3390/ijerph111010559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuligni AJ, Pedersen S. Family obligation and the transition to young adulthood. Developmental Psychology. 2002;38(5):856–868. doi: 10.1037/0012-1649.38.5.856. [DOI] [PubMed] [Google Scholar]
- Fuligni AJ, Tseng V, Lam M. Attitudes toward family obligations among American adolescents with Asian, Latin American, and European backgrounds. Child Development. 1999;70(4):1030–1044. doi: 10.1111/1467-8624.00075. [DOI] [Google Scholar]
- Fuligni AJ, Witkow M. The postsecondary educational progress of youth from immigrant families. Journal of Research on Adolescence. 2004;14(2):159–183. doi: 10.1111/j.1532-7795.2004.01402002.x. [DOI] [Google Scholar]
- Fuligni AJ, Yip T, Tseng V. The impact of family obligation on the daily activities and psychological well-being of Chinese American adolescents. Child Development. 2002;73(1):302–314. doi: 10.1111/1467-8624.00407. [DOI] [PubMed] [Google Scholar]
- Garland AF, Lau AS, Yeh M, McCabe KM, Hough RL, Landsverk JA. Racial and ethnic differences in utilization of mental health services among high-risk youths. American Journal of Psychiatry. 2005;162(7):1336–1343. doi: 10.1176/appi.ajp.162.7.1336. [DOI] [PubMed] [Google Scholar]
- Gary FA. Stigma: barrier to mental health care among ethnic minorities. Issues in Mental Health Nursing. 2005;26(10):979–999. doi: 10.1080/01612840500280638. [DOI] [PubMed] [Google Scholar]
- de Groot A, Koot HM, Verhulst FC. Cross-cultural generalizability of the youth self-report and teacher’s report form cross-informant syndromes. Journal of Abnormal Child Psychology. 1996;24(5):651–664. doi: 10.1007/BF01670105. [DOI] [PubMed] [Google Scholar]
- Gross JJ, Thompson RA. Emotion regulation: Conceptual foundations. Handbook of emotion regulation. 2007;3:24. [Google Scholar]
- Gudiño OG, Martinez JI, Lau AS. Mental health service use by youths in contact with child welfare: racial disparities by problem type. Psychiatric Services. 2012;63(10):1004–1010. doi: 10.1176/appi.ps.201100427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. 2010;10(1):113. doi: 10.1186/1471-244X-10-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo S, Kataoka SH, Bear L, Lau AS. Differences in school-based referrals for mental health care: understanding racial/ethnic disparities between Asian American and Latino youth. School Mental Health. 2014;6(1):27–39. doi: 10.1007/s12310-013-9108-2. [DOI] [Google Scholar]
- Hankin BL, Abramson LY. Measuring cognitive vulnerability to depression in adolescence: reliability, validity, and gender differences. Journal of Clinical Child & Adolescent Psychology. 2002;31(4):491–504. doi: 10.1207/S15374424JCCP3104_8. [DOI] [PubMed] [Google Scholar]
- Helms JE, Jernigan M, Mascher J. The meaning of race in psychology and how to change it: A methodological perspective. American Psychologist. 2005;60(1):27–36. doi: 10.1037/0003-066X.60.1.27. [DOI] [PubMed] [Google Scholar]
- Ho J, Yeh M, McCabe K, Hough RL. Parental cultural affiliation and youth mental health service use. Journal of youth and adolescence. 2007;36(4):529–542. [Google Scholar]
- Ho J. Acculturation gaps in Vietnamese immigrant families: Impact on family relationships. International Journal of Intercultural Relations. 2010;34(1):22–33. doi: 10.1016/j.ijintrel.2009.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaccard J, Wan CK, Turrisi R. The Detection and interpretation of interaction effects between continuous variables in multiple regression. Multivariate Behavioral Research. 1990;25(4):467–478. doi: 10.1207/s15327906mbr2504_4. [DOI] [PubMed] [Google Scholar]
- Kashdan TB, Barrios V, Forsyth JP, Steger MF. Experiential avoidance as a generalized psychological vulnerability: Comparisons with coping and emotion regulation strategies. Behaviour Research and Therapy. 2006;44(9):1301–1320. doi: 10.1016/j.brat.2005.10.003. [DOI] [PubMed] [Google Scholar]
- Katz SJ, Kessler RC, Frank RG, Leaf P, Lin E. Mental health care use, morbidity, and socioeconomic status in the United States and Ontario. Inquiry. 1997:38–49. [PubMed] [Google Scholar]
- Kelly CM, Jorm AF, Wright A. Improving mental health literacy as a strategy to facilitate early intervention for mental disorders. The Medical Journal of Australia. 2007;187(7 Suppl):S26–30. doi: 10.5694/j.1326-5377.2007.tb01332.x. [DOI] [PubMed] [Google Scholar]
- Kim BK, Li LC, Ng GF. The Asian American Values Scale--Multidimensional: Development, reliability, and validity. Cultural Diversity and Ethnic Minority Psychology. 2005;11(3):187–201. doi: 10.1037/1099-9809.11.3.187. http://dx.doi.org/10.1037/1099-9809.11.3.187. [DOI] [PubMed] [Google Scholar]
- Kim BSK, Omizo MM. Asian cultural values, attitudes toward seeking professional psychological help, and willingness to see a counselor. The Counseling Psychologist. 2003;31(3):343–361. doi: 10.1177/0011000003031003008. [DOI] [Google Scholar]
- Kim HS, Sherman DK, Taylor SE. Culture and social support. American Psychologist. 2008;63(6):518–526. doi: 10.1037/0003-066X. [DOI] [PubMed] [Google Scholar]
- Le Meyer O, Zane N, Cho YI, Takeuchi DT. Use of specialty mental health services by Asian Americans with psychiatric disorders. Journal of Consulting and Clinical Psychology. 2009;77(5):1000–1005. doi: 10.1037/a0017065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee S, Juon HS, Martinez G, Hsu CE, Robinson ES, Bawa J, Ma GX. Model minority at risk: Expressed needs of mental health by Asian American young adults. Journal of Community Health. 2009;34(2):144–152. doi: 10.1007/s10900-008-9137-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leong FTL, Kim HHW, Gupta A. Attitudes toward professional counseling among Asian-American college students: Acculturation, conceptions of mental illness, and loss of face. Asian American Journal of Psychology. 2011;2(2):140–153. http://dx.doi.org/10.1037/a0024172. [Google Scholar]
- Leong FTL, Lau ASL. Barriers to providing effective mental health services to Asian Americans. Mental Health Services Research. 2001;3(4):201–214. doi: 10.1023/A:1013177014788. [DOI] [PubMed] [Google Scholar]
- Lien O. Attitudes of the Vietnamese community towards mental illness. Australasian Psychiatry. 1993;1(3):110–112. [Google Scholar]
- Logan DE, King CA. Parental facilitation of adolescent mental health service utilization: A conceptual and empirical review. Clinical Psychology: Science and Practice. 2001;8(3):319–333. doi: 10.1093/clipsy.8.3.319. [DOI] [Google Scholar]
- Louie JY, Oh BJ, Lau AS. Cultural differences in the links between parental control and children’s emotional expressivity. Cultural Diversity and Ethnic Minority Psychology. 2013;19(4):424–434. doi: 10.1037/a0032820. [DOI] [PubMed] [Google Scholar]
- Luu TD, Leung P, Nash SG. Help-seeking attitudes among Vietnamese Americans: The impact of acculturation, cultural barriers, and spiritual beliefs. Social Work in Mental Health. 2009;7(5):476–493. [Google Scholar]
- Markus HR, Kitayama S. Culture and the self: Implications for cognition, emotion, and motivation. Psychological Review. 1991;98(2):224–253. doi: 10.1037/0033-295X.98.2.224. [DOI] [Google Scholar]
- Matsumoto D, Yoo SH, Fontaine J. Mapping expressive differences around the world: The relationship between emotional display rules and individualism versus collectivism. Journal of Cross-Cultural Psychology. 2008;39(1):55–74. doi: 10.1177/0022022107311854. [DOI] [Google Scholar]
- Miller TW. Stressful life events. Madison, CT: International Universities Press; 1989. [Google Scholar]
- Moran P. Attachment style, ethnicity and help-seeking attitudes among adolescent pupils. British Journal of Guidance & Counselling. 2007;35(2):205–218. doi: 10.1080/03069880701256627. [DOI] [Google Scholar]
- Neighbors HW, Caldwell C, Williams DR, Nesse R, Taylor RJ, Bullard KM, Jackson JS. Race, ethnicity, and the use of services for mental disorders: results from the National Survey of American Life. Archives of General Psychiatry. 2007;64(4):485–494. doi: 10.1001/archpsyc.64.4.485. [DOI] [PubMed] [Google Scholar]
- Ngo D, Tran TV, Gibbons JL, Oliver JM. Acculturation, premigration traumatic experiences, and depression among Vietnamese Americans. Journal of Human Behavior in the Social Environment. 2001;3(3/4):225–242. [Google Scholar]
- Nguyen QCX, Anderson LP. Vietnamese Americans’ attitudes toward seeking mental health services: Relation to cultural variables. Journal of Community Psychology. 2005;33(2):213–231. doi: 10.1002/jcop.20039. [DOI] [Google Scholar]
- Park HS, Levine TR. The theory of reasoned action and self-construal: Evidence from three cultures. Communications Monographs. 1999;66(3):199–218. [Google Scholar]
- Park YS, Kim BSK. Asian and European American cultural values and communication styles among Asian American and European American college students. Cultural Diversity and Ethnic Minority Psychology. 2008;14(1):47–56. doi: 10.1037/1099-9809.14.1.47. http://dx.doi.org/10.1037/1099-9809.14.1.47. [DOI] [PubMed] [Google Scholar]
- Phan T. Investigating the use of services for Vietnamese with mental illness. Journal of Community Health. 2000;25(5):411–425. doi: 10.1023/a:1005184002101. [DOI] [PubMed] [Google Scholar]
- Phinney JS, Ong A, Madden T. Cultural values and intergenerational value discrepancies in immigrant and non-immigrant families. Child development. 2000;71(2):528–539. doi: 10.1111/1467-8624.00162. [DOI] [PubMed] [Google Scholar]
- Phinney JS, Ong AD. Adolescent-parent disagreements and life satisfaction in families from Vietnamese-and European-American backgrounds. International journal of behavioral development. 2002;26(6):556–561. [Google Scholar]
- Poss JE. Developing a new model for cross-cultural research: synthesizing the Health Belief Model and the Theory of Reasoned Action. ANS. Advances in Nursing Science. 2001;23(4):1–15. doi: 10.1097/00012272-200106000-00002. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers. 2004;36(4):717–731. doi: 10.3758/BF03206553. [DOI] [PubMed] [Google Scholar]
- Sen B. Adolescent propensity for depressed mood and help-seeking: race and gender differences. Journal of Mental Health Policy and Economics. 2004;7(3):133–145. [PubMed] [Google Scholar]
- Shea M, Yeh C. Asian American students’ cultural values, stigma, and relational self-construal: Correlates of attitudes toward professional help-seeking. Journal of Mental Health Counseling. 2008;30(2):157–172. [Google Scholar]
- Silk JS, Steinberg L, Morris AS. Adolescents’ emotion regulation in daily life: links to depressive symptoms and problem behavior. Child Development. 2003;74(6):1869–1880. doi: 10.1046/j.1467-8624.2003.00643.x. [DOI] [PubMed] [Google Scholar]
- Steel Z, Frommer N, Silove D. Part I—The mental health impacts of migration: The law and its effects: Failing to understand: Refugee determination and the traumatized applicant. International journal of law and psychiatry. 2004;27(6):511–528. doi: 10.1016/j.ijlp.2004.08.006. [DOI] [PubMed] [Google Scholar]
- Taylor SE, Sherman DK, Kim HS, Jarcho J, Takagi K, Dunagan MS. Culture and social support: Who seeks It and why? Journal of Personality and Social Psychology. 2004;87(3):354–362. doi: 10.1037/0022-3514.87.3.354. [DOI] [PubMed] [Google Scholar]
- Telzer EH, Fuligni AJ. Daily family assistance and the psychological well-being of adolescents from Latin American, Asian, and European backgrounds. Developmental Psychology. 2009;45(4):1177–1189. doi: 10.1037/a0014728. [DOI] [PubMed] [Google Scholar]
- Ting JY, Hwang WC. Cultural influences on help-seeking attitudes in Asian American students. American Journal of Orthopsychiatry. 2009;79(1):125–132. doi: 10.1037/a0015394. [DOI] [PubMed] [Google Scholar]
- Tran TV. Psychological traumas and depression in a sample of Vietnamese people in the United States. Health & social work. 1993;18(3):184–194. doi: 10.1093/hsw/18.3.184. [DOI] [PubMed] [Google Scholar]
- Tsai JL, Knutson B, Fung HH. Cultural variation in affect valuation. Journal of Personality and Social Psychology. 2006;90(2):288–307. doi: 10.1037/0022-3514.90.2.288. [DOI] [PubMed] [Google Scholar]
- Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC. Twelvemonth use of mental health services in the United States: results from the National Comorbidity Survey Replication. Archives of general psychiatry. 2005;62(6):629–640. doi: 10.1001/archpsyc.62.6.629. [DOI] [PubMed] [Google Scholar]
- Wang S, Shih JH, Hu AW, Louie JY, Lau AS. Cultural differences in daily support experiences. Cultural Diversity and Ethnic Minority Psychology. 2010;16(3):413–420. doi: 10.1037/a0019885. [DOI] [PubMed] [Google Scholar]
- Williams DR, Gonzalez HM, Neighbors H, Nesse R, Abelson JM, Sweetman J, Jackson JS. Prevalence and distribution of major depressive disorder in African Americans, Caribbean blacks, and non-Hispanic whites: results from the National Survey of American Life. Archives of General Psychiatry. 2007;64(3):305–315. doi: 10.1001/archpsyc.64.3.305. [DOI] [PubMed] [Google Scholar]
- Wilson CJ, Deane FP, Ciarrochi J, Rickwood D. Measuring help-seeking intentions: Properties of the General Help-Seeking Questionnaire. Canadian Journal of Counselling and Psychotherapy/Revue Canadienne de Counseling et de Psychothérapie. 2007;39(1) [Google Scholar]
- Wilson CJ, Rickwood D, Deane FP. Depressive symptoms and help-seeking intentions in young people. Clinical Psychologist. 2007;11(3):98–107. doi: 10.1080/13284200701870954. [DOI] [Google Scholar]
- World Health Organization. The second decade: improving adolescent health and development. Geneva: World Health Organization; 2001. [Google Scholar]
- Zhou M, Bankston CL., III . Growing up American: How Vietnamese children adapt to life in the United States. New York, NY: Russell Sage Foundation; 1998. [Google Scholar]
- Zwaanswijk M, Verhaak PFM, Bensing JM, van der Ende J, Verhulst FC. Help-seeking for emotional and behavioural problems in children and adolescents. European Child & Adolescent Psychiatry. 2003;12(4):153–161. doi: 10.1007/s00787-003-0322-6. [DOI] [PubMed] [Google Scholar]