

Abstract
Pain is defined as an “unpleasant sensory and emotional feeling which is associated with actual or potential injury of tissue or expressed in terms of such injury.” Tooth pain usually refers to pain around the teeth or jaws mainly as a result of a dental condition. Mostly, toothaches are caused by a carious cavity, a broken tooth, an exposed tooth root or gum disease. The toothache may sometimes be the result of radiating pain from structures in the vicinity of tooth and jaws (cardiac pain, ear, nose, throat pain, and sinusitis). Therefore, evaluation by both dentists and physicians are sometimes necessary to diagnose medical illnesses causing “toothache.” Cracked tooth syndrome is a major diagnostic challenge in clinical practice. Accurate diagnosis and appropriate treatment are complicated due to lack of awareness of this condition and its bizarre clinical features. Early diagnosis has been linked with successful restorative management and good prognosis. This article provides a detailed literature on the causes, classification, signs and symptoms, diagnosis, and treatment planning of cracked tooth syndrome.
Keywords: Cracked tooth syndrome, diagnosis, tooth pain
INTRODUCTION
Cracked tooth syndrome may be defined as a fracture plane of unknown depth, which originate from the crown, passes through the tooth structure and extends subgingivally, and may progress to connect with the pulp space and/or periodontal ligament.[1,2]
Gibbs in 1954, was the first to describe the clinical symptoms of incomplete fracture of posterior teeth involving the cusp and termed it as “cuspal fracture odontalgia.”[3] Cases of incomplete fracture with subsequent pulpitis were reported by Ritchey et al. in 1957.[4] Cameron in 1964 coined the term “cracked tooth syndrome.” Here, the signs and symptoms were not apparent, and the teeth showed painful response to cold or pressure applications and became necrotic, however, the pulp and periodontium were apparently healthy.[5]
Ellis defined, incomplete tooth fracture as a “fracture plane of unknown depth and direction passing through tooth structure, and may advance to connect with the pulp and/or periodontal ligament.”[6,7]
In the late 1970s, Maxwell and Braly advocated the use of the term incomplete tooth fracture.[8] According to Luebke, fractures are either complete or incomplete, although, other terms such as split-root syndrome, hairline fracture, hairline tooth fracture, enamel infraction, crown craze, craze lines, and tooth structure cracks are also known.[9]
CLASSIFICATION
Several classifications have been proposed based on: (a) The type or site of the crack, (b) the direction and degree of the crack, (c) the risk of symptoms, (d) pathological processes.
The American Association of Endodontists,[10] in a document titled “cracking the cracked tooth code” identified five types of cracked teeth [Table 1].
Table 1.
American Association of Endodontists classification of a cracked tooth

Craze lines are visible fractures and contained within the enamel. In posterior teeth, craze lines are usually seen to cross the marginal ridges and/or extend along buccal and lingual surfaces. Long vertical craze lines usually occur in anterior teeth [Figure 1a].
Figure 1.
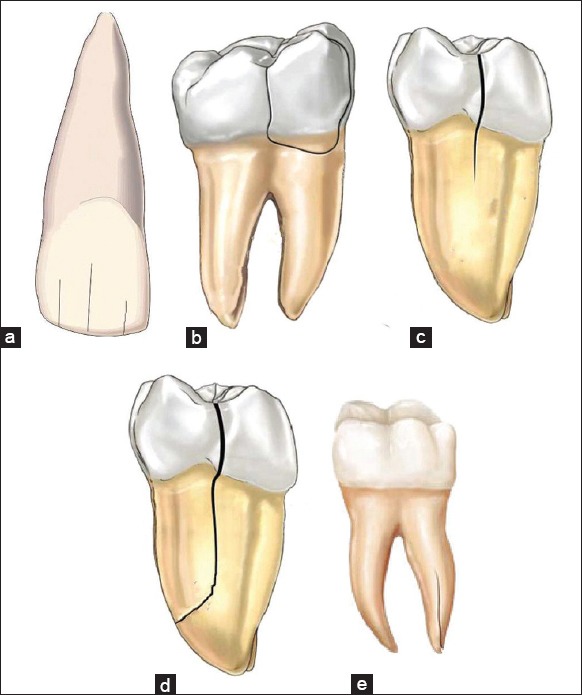
(a) Depicting visible fracture lines within the enamel suggestive of Craze lines; (b) Fractured cusp terminating in the cervical part of the tooth; (c) Cracked tooth extending from the occlusal tooth surface without separation of tooth fragments; (d) Separated tooth fragments suggestive of a split tooth; (e) Vertical root fracture
Fractured cusps begin at the crown of the tooth, extend into dentin, and the fracture ends in the cervical part of the tooth. They are usually seen in heavily restored teeth, causing unsupported cuspal enamel [Figure 1b].
A cracked tooth is indicative of a crack extending from the occlusal surface of the tooth apically without separation of the two fragments. The crack is generally located at the center of the tooth in a mesiodistal direction and may involve one or both marginal ridges [Figure 1c].
A split tooth is indicative of a crack extending through both marginal ridges usually in a mesiodistal direction splitting the tooth completely into two individual fragments. The crack is generally located at the center of the tooth and this entity occurs due to crack propagation [Figure 1d].
Vertical root fractures commence in the root generally in a bucco-lingual direction. The crack is generally complete though may be incomplete and involve only one surface. The crack may involve either the entire root or only a portion of the root [Figure 1e].
ETIOLOGY
Cracked tooth syndrome has a multi-factorial etiology. Geurtsen showed that “excessive forces applied to a healthy tooth or physiologic forces applied to a weakened tooth results in an incomplete fracture of the enamel or dentine.”[11]
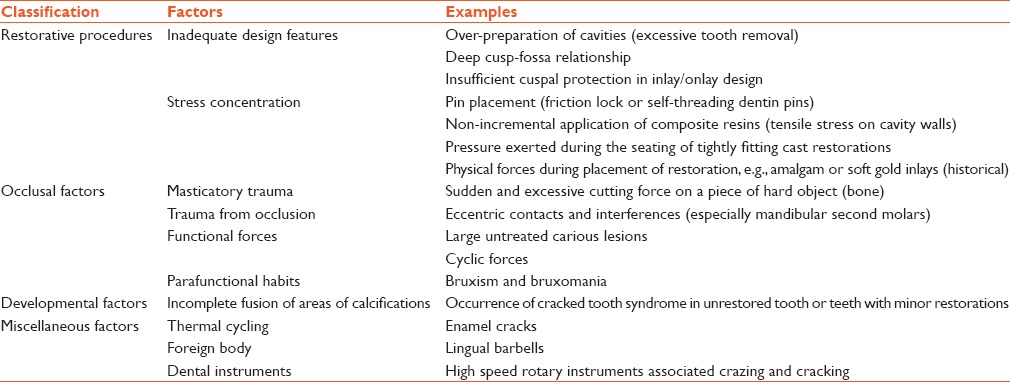
Lynch and McConnell[12] subdivided the etiology into 4 major categories-restorative procedures, occlusal factors, developmental factors, and miscellaneous factors [Table 2].
Table 2.
Etiological factors in cracked tooth syndrome
EPIDEMIOLOGY
The occurrence of cracked tooth syndrome is unknown, but an incidence rate of 34–74% has been documented.[5,13] It occurs frequently in individuals within the age range of 30–50 years,[14] with a female predilection.[2] Most commonly affected tooth is mandibular molar followed by maxillary premolar, maxillary molar, and mandibular premolar.[13] Mandibular first molars are the first permanent teeth to erupt into the dental arch, hence, they are more prone to dental caries and subsequent restorative intervention. Thus, they are more susceptible to fracture. The “wedging effect” upon lower first molar teeth from the prominent mesio-palatal cusp of maxillary first molar teeth may also be contributory.[11]
CLINICAL FEATURES
Cracked tooth syndrome presents with varied clinical signs and symptoms, according to the position and extent of the incomplete fracture.[11,15,16] History of the discomfort of several months and sharp pain when biting or when consuming cold food/beverages may be elicited.[17] “Rebound pain” - pain on the release of pressure upon intake of fibrous foods is a consistent feature.[18] Pain may be elicited by the consumption of sugar containing substances,[19] and also by the act of tooth grinding or during excursive mandibular movements.[20] Patients may or may not be able to locate the offending tooth (there are no proprioceptive fibers in the pulp chamber). The absence of heat-induced sensitivity may also be a feature. Chronic pulpitis with no clinical symptoms may be seen as a result of micro-leakage of bacterial by-products and toxins. Cracks with pulpal involvement may result in pulpal and periodontal symptoms.[21,22]
Brännström and Aström[23] proposed the physiological basis of pain on chewing. When the fractured portions of the tooth move independently of each other, it causes sudden movement of fluid present in the dentinal tubules. This causes activation of myelinated A-type fibers within the dental pulp and results in acute pain. Hypersensitivity to cold may occur due to the seepage of toxic irritants through the crack. This leakage of toxic irritants cause the release of neuropeptides, and a concomitant lowering in the pain threshold of unmyelinated C-type fibers within the dental pulp.[24] Other author states that the symptoms are caused by the alternating stretching and compressing of the odontoblast processes located within the crack.[25]
DIAGNOSIS
Because of the variable and bizarre clinical signs and symptoms, cracked tooth syndrome is a diagnostic challenge for even the most experienced dental operators.[26] The importance of an early diagnosis has been linked with successful restorative management and prognosis.[27] Wide variety of dental conditions may present with similar features and misdiagnosed as a cracked tooth syndrome, thus complicating the diagnosis. Such conditions include acute periodontal diseases, reversible pulpitis, dentinal hypersensitivity, galvanic pain associated with silver amalgam restorations, sensitivity following micro leakage from recently placed composite resin restorations, areas of hyper occlusion from dental restorations, occlusal trauma from parafunctional habits, orofacial pain arising from conditions such as trigeminal neuralgia and psychiatric disorders such as atypical facial pain.[2]
Dental history
A thorough and detailed dental history may help in eliciting certain distinct clues.[12] The patient may have a history of long-term dental treatment, multiple replacements of restorations, and occlusal adjustments. There may be a history of parafunctional habits (clenching or grinding, chewing on hard objects).[28] History of cold sensitivity and sharp pain on biting hard or tough foods which ceases when the pressure is released is an important indicator. Symptoms may vary according to the depth and orientation of the crack.[29]
Clinical examination
The application of a sharp straight probe to the margins of the heavily restored tooth (suspected to have an incomplete fracture) may evoke sharp pain, thus indicative of the presence of underlying crack. Sometimes exploratory excavation may be needed to obtain a visual diagnosis. Patient's consent is mandatory for excavation as it is not guaranteed that a fracture will be seen beneath the removed restoration. On removal of the existing restorations, fracture lines may be revealed. Clinical examination may also reveal the presence of wear facets on the occlusal tooth surfaces (identifies teeth in eccentric contact and at risk from damaging lateral forces), occurrence of localized periodontal defects (where cracks extend subgingivally) or the evocation of symptoms by sweat or thermal stimuli. The use of rubber dam enhances the probability of visualizing these cracks by isolating the tooth, emphasizing the crack with a distinct background, keeping the area saliva free, and reducing peripheral disruptions.
Periodontal probing
Cracked tooth and a split tooth may be differentiated by periodontal probing. The localized periodontal defect is the result of a fracture line extending below the gingiva. Isolated deep probing reveal the presence of a split tooth, indicating a poor prognosis.
Dye test
Special stains such as methylene blue or gentian violet are frequently used to highlight the cracks.[26] However, a long time (at least 2–5 days) is needed to be effective and may require placement of a provisional restoration. This may weaken the tooth integrity and further spread the crack. Another disadvantage is difficult esthetic restoration.
Bite tests
Pain on biting that ceases after the pressure has been withdrawn is a classical sign. Symptoms may be elicited when pressure is applied to an individual cusp.[3,30,31] This forms the basis of so-called “bite tests.” Here, the patient is asked to bite on various items such as a toothpick, cotton roll, rubber abrasive wheels such as burlew wheel, orange wooden stick[15,18,31] or the commercially available Tooth Slooth (Professional Results Inc., Laguna Niguel, CA, USA).[15]
Vitality tests
Vitality tests for individual teeth are usually positive.[19] Sometimes the affected teeth may show signs of hypersensitivity to cold thermal stimuli due to the presence of pulpal inflammation; a feature that may help to confirm a diagnosis of cracked tooth syndrome. Teeth affected by the condition may be seldom tender on apical percussion.
Radiographs
Diagnosis of cracked tooth syndrome by radiographs is usually questionable, as fractures propagate in a mesiodistal direction; parallel to the plane of the film.[12] Fractures occurring in a bucco-lingual direction is more readily noticed on radiographs. Radiographs may be helpful in assessing the status of the pulp and periodontium, and for excluding other dental pathology.[2]
Transillumination
Transillumination is an important aid in diagnosing the cracks, whether it is an incomplete crack (as in cracked tooth syndrome) or a complete vertical root fracture.[32] In transillumination, the tooth is cleaned and a fiber-optic or other light source is applied directly on the tooth. A crack will block the transmission of light, and structurally sound teeth (including those with craze lines) will transmit the light throughout the crown. Two main disadvantages of using transillumination without magnification are: (a) Transillumination dramatizes all cracks to the point that craze lines appear as structural cracks. (b) Subtle color changes are indistinguishable. Transillumination with a fiber-optic light and use of magnification will aid in visualization of a crack.[33]
Microscopic detection
Use of clinical microscope (×16) provides an ideal magnification level for the evaluation of enamel cracks, with a range from ×14 to ×18.[34]
Ultrasound is also capable of imaging cracks in the simulated tooth structure and can be used as a future diagnostic aid.[35]
Indirect diagnostic measures, such as the use of copper rings, acrylic provisional crowns, and stainless steel orthodontic bands, may also be used to detect cracked tooth syndrome.[15]
Another indirect diagnostic method is an unauthenticated technique by Banerji et al.[36] Composite resin is placed over the tooth without etching and bonding. The patient feels marked improvement in discomfort on biting, as the material acts as a splint.
MANAGEMENT
The treatment of a cracked tooth depends on the site, direction, size or the degree of the crack. Superficial cracks are easy and early to detect, and hence simple to manage. Minor cracks are often restored with a filling or a crown.
Deep cracks with pulp involvement require root canal treatment and a crown to protect the tooth.
In the worst case scenario, a cracked tooth cannot be repaired. This occurs when the crack extends into the root of the tooth beneath the bone. These cases require the removal of the tooth and replace with a dental implant or a dental bridge.
According to Clark and Caughman,[37] the prognosis of cracked teeth can be excellent, good, poor, and hopeless.
Excellent: (a) Cuspal fractures within the dentin that angle from the faciopulpal or linguopulpal line angle of a cusp to the cemento-enamel junction or slightly below. (b) Horizontal fracture of a cusp not involving the pulp
Good: A coronal vertical fracture that runs mesiodistally into the dentin but not into the pulp
Poor: A coronal vertical fracture that runs mesiodistally into the dentin and pulp, but is limited to the crown
Hopeless: A coronal vertical fracture that runs mesiodistally through the pulp and extends into the root.
CONCLUSION
Cracked tooth syndrome is a common and well-documented entity in the clinical practice. Patients usually present with a wide variety of signs and symptoms, thus making the diagnosis difficult and complicated. Detailed history and thorough clinical examination may help in establishing a correct diagnosis and hence that an appropriate treatment plan can be instituted.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Torabinejad M, Walton RE. Principles and Practice. 4th ed. Philadelphia: Saunders; 2008. Endodontics; pp. 110–5. [Google Scholar]
- 2.Türp JC, Gobetti JP. The cracked tooth syndrome: An elusive diagnosis. J Am Dent Assoc. 1996;127:1502–7. doi: 10.14219/jada.archive.1996.0060. [DOI] [PubMed] [Google Scholar]
- 3.Gibbs JW. Cuspal fracture odontalgia. Dent Dig. 1954;60:158–60. [Google Scholar]
- 4.Ritchey B, Mendenhall R, Orban B. Pulpitis resulting from incomplete tooth fracture. Oral Surg Oral Med Oral Pathol. 1957;10:665–70. doi: 10.1016/s0030-4220(57)80016-4. [DOI] [PubMed] [Google Scholar]
- 5.Cameron CE. Cracked-tooth syndrome. J Am Dent Assoc. 1964;68:405–11. doi: 10.14219/jada.archive.1964.0108. [DOI] [PubMed] [Google Scholar]
- 6.Brannstrom M. The hydrodynamic theory of dentinal pain: Sensation in preparations, caries, and the dentinal crack syndrome. J Endod. 1986;12:453–7. doi: 10.1016/S0099-2399(86)80198-4. [DOI] [PubMed] [Google Scholar]
- 7.Kahler B, Moule A, Stenzel D. Bacterial contamination of cracks in symptomatic vital teeth. Aust Endod J. 2000;26:115–8. doi: 10.1111/j.1747-4477.2000.tb00296.x. [DOI] [PubMed] [Google Scholar]
- 8.Maxwell EH, Braly BV. Incomplete tooth fracture. Prediction and prevention. CDA J. 1977;5:51–5. [PubMed] [Google Scholar]
- 9.Luebke RG. Vertical crown-root fractures in posterior teeth. Dent Clin North Am. 1984;28:883–94. [PubMed] [Google Scholar]
- 10.Chicago, IL: Fall/Winter; 1997. American Association of Endodontists. Endodontics: Colleagues for Excellence-Cracking the cracked tooth code. [Google Scholar]
- 11.Geurtsen W. The cracked-tooth syndrome: Clinical features and case reports. Int J Periodontics Restorative Dent. 1992;12:395–405. [PubMed] [Google Scholar]
- 12.Lynch CD, McConnell RJ. The cracked tooth syndrome. J Can Dent Assoc. 2002;68:470–5. [PubMed] [Google Scholar]
- 13.Hiatt WH. Incomplete crown-root fracture in pulpal-periodontal disease. J Periodontol. 1973;44:369–79. doi: 10.1902/jop.1973.44.6.369. [DOI] [PubMed] [Google Scholar]
- 14.Ellis SG, Macfarlane TV, McCord JF. Influence of patient age on the nature of tooth fracture. J Prosthet Dent. 1999;82:226–30. doi: 10.1016/s0022-3913(99)70161-7. [DOI] [PubMed] [Google Scholar]
- 15.Ehrmann EH, Tyas MJ. Cracked tooth syndrome: Diagnosis, treatment and correlation between symptoms and post-extraction findings. Aust Dent J. 1990;35:105–12. doi: 10.1111/j.1834-7819.1990.tb05872.x. [DOI] [PubMed] [Google Scholar]
- 16.Chong BS. Bilateral cracked teeth: A case report. Int Endod J. 1989;22:193–6. doi: 10.1111/j.1365-2591.1989.tb00924.x. [DOI] [PubMed] [Google Scholar]
- 17.Cameron CE. The cracked tooth syndrome: Additional findings. J Am Dent Assoc. 1976;93:971–5. doi: 10.14219/jada.archive.1976.0034. [DOI] [PubMed] [Google Scholar]
- 18.Stanley HR. The cracked tooth syndrome. J Am Acad Gold Foil Oper. 1968;11:36–47. [PubMed] [Google Scholar]
- 19.Trushkowsky R. Restoration of a cracked tooth with a bonded amalgam. Quintessence Int. 1991;22:397–400. [PubMed] [Google Scholar]
- 20.Griffin JD., Jr Efficient, conservative treatment of symptomatic cracked teeth. Compend Contin Educ Dent. 2006;27:93–102. [PubMed] [Google Scholar]
- 21.Brannstrom M. London: Wolfe Medical Publications Ltd; 1982. Dentin and Pulp in Restorative Dentistry; pp. 47–63. [Google Scholar]
- 22.Bergenholtz G. Pathogenic mechanisms in pulpal disease. J Endod. 1990;16:98–101. doi: 10.1016/S0099-2399(06)81571-2. [DOI] [PubMed] [Google Scholar]
- 23.Brännström M, Aström A. The hydrodynamics of the dentine; its possible relationship to dentinal pain. Int Dent J. 1972;22:219–27. [PubMed] [Google Scholar]
- 24.Davis R, Overton JD. Efficacy of bonded and nonbonded amalgam in the treatment of teeth with incomplete fractures. J Am Dent Assoc. 2000;131:469–78. doi: 10.14219/jada.archive.2000.0203. [DOI] [PubMed] [Google Scholar]
- 25.Dewberry JA. Vertical fractures of posterior teeth. In: Lieve FS, editor. Endodontic Therapy. 5th ed. St. Louis: Mosby; 1996. pp. 71–81. [Google Scholar]
- 26.Liu HH, Sidhu SK. Cracked teeth – treatment rationale and case management: Case reports. Quintessence Int. 1995;26:485–92. [PubMed] [Google Scholar]
- 27.Agar JR, Weller RN. Occlusal adjustment for initial treatment and prevention of the cracked tooth syndrome. J Prosthet Dent. 1988;60:145–7. doi: 10.1016/0022-3913(88)90303-4. [DOI] [PubMed] [Google Scholar]
- 28.Homewood CI. Cracked tooth syndrome – Incidence, clinical findings and treatment. Aust Dent J. 1998;43:217–22. [PubMed] [Google Scholar]
- 29.Geurtsen W, Schwarze T, Günay H. Diagnosis, therapy, and prevention of the cracked tooth syndrome. Quintessence Int. 2003;34:409–17. [PubMed] [Google Scholar]
- 30.Rosen H. Cracked tooth syndrome. J Prosthet Dent. 1982;47:36–43. doi: 10.1016/0022-3913(82)90239-6. [DOI] [PubMed] [Google Scholar]
- 31.Bales DJ. Pain and the cracked tooth. J Indiana Dent Assoc. 1975;54:15–8. [PubMed] [Google Scholar]
- 32.Liewehr FR. An inexpensive device for transillumination. J Endod. 2001;27:130–1. doi: 10.1097/00004770-200102000-00019. [DOI] [PubMed] [Google Scholar]
- 33.Lubisich EB, Hilton TJ, Ferracane J, Northwest Precedent. Cracked teeth: A review of the literature. J Esthet Restor Dent. 2010;22:158–67. doi: 10.1111/j.1708-8240.2010.00330.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Clark DJ, Sheets CG, Paquette JM. Definitive diagnosis of early enamel and dentin cracks based on microscopic evaluation. J Esthet Restor Dent. 2003;15:391–401. doi: 10.1111/j.1708-8240.2003.tb00963.x. [DOI] [PubMed] [Google Scholar]
- 35.Culjat MO, Singh RS, Brown ER, Neurgaonkar RR, Yoon DC, White SN. Ultrasound crack detection in a simulated human tooth. Dentomaxillofac Radiol. 2005;34:80–5. doi: 10.1259/dmfr/12901010. [DOI] [PubMed] [Google Scholar]
- 36.Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 1: Aetiology and diagnosis. Br Dent J. 2010;208:459–63. doi: 10.1038/sj.bdj.2010.449. [DOI] [PubMed] [Google Scholar]
- 37.Clark LL, Caughman WF. Restorative treatment for the cracked tooth. Oper Dent. 1984;9:136–42. [PubMed] [Google Scholar]