

Abstract
Segmental absence of intestinal musculature (SAIM) is a rare cause of intestinal obstruction and/or perforation seen in neonates, and rarely in adults. We present a case of SAIM in a 48-year-old male, who presented with acute abdominal symptoms and was repeatedly explored because of recurrence of abdominal symptoms.
Keywords: Congenital defect, intestinal perforation, segmental absence of intestinal musculature, segmental muscular aplasia, small intestine
INTRODUCTION
Segmental absence of intestinal musculature (SAIM) was first reported as a new entity in 1947 by Emanuel et al. as a cause of intestinal obstruction.[1] The cases are now increasingly reported in the medical literature, so far more than 25 cases have been reported in the English literature with additional cases in European and Asian literature. The diagnosis is made after postoperative pathologic examination of the resected bowel.[2] Most of the cases are reported from neonatal age group. However, occasionally the cases have been reported in adults.[3,4] Beside small intestine, musculature defect has been reported in stomach[5] and colon.[6]
These cases of SAIM have been divided into primary and secondary groups. In primary group etiology is unknown, the onset of symptoms is acute and there is no pathologic finding in the remaining layers of the small intestine except for superimposed perforation or intussusception. In Secondary group there is longer history of intestinal symptoms and multiple surgical procedures. Histologically there may be ischemic necrosis of the remaining layers, fibrosis, calcification, chronic inflammation and presence of macrophages.[7] These findings indicate secondary destruction of muscle coat due to ischemia and/or infarction, interruption of blood supply or trauma. Most of the authors agree that this is a congenital defect and some believe ischemia to be only etiological factor in cases of perforation.[8] Here, we present a rare case of SAIM in an adult of 48 years.
CASE REPORT
A 48-year-old male, previously operated in some other hospital for pain in abdomen and vomiting for 2 days. Resection anastomosis of the bowel was done nearly 20 days back, and the surgical pathology report mentioned perforation peritonitis with the gangrenous bowel. He was admitted in our hospital for the complaints of abdominal distension and vomiting and treated conservatively. He was discharged from the hospital and was readmitted after a week for abdominal distension, pain and vomiting for 1-day. He had abdominal tenderness and guarding. His plain X-ray abdomen in standing position showed gas under the diaphragm. He was reoperated, and resection anastomosis of the bowel was done where perforation peritonitis was present.
In surgical pathology department, two pieces of small intestine together measuring 45 cm were received. The pieces were markedly congested with rough peritoneal surface and thin wall with a perforation of 1 cm. diameter in the mid part of one piece. Mucosa was blackish. Mesentery was congested. The sections near the perforation showed necrosis of mucosa with inflammatory cell infiltration, marked vascular congestion, sub-mucosal fibrosis and peritonitis [Figure 1a] with gangrenous changes. The section from the mesentery showed inflammation and a thrombosed artery [Figure 1b]. The sections taken from the normal looking parts of intestine revealed focal absence of muscularis propria [Figure 2].
Figure 1.
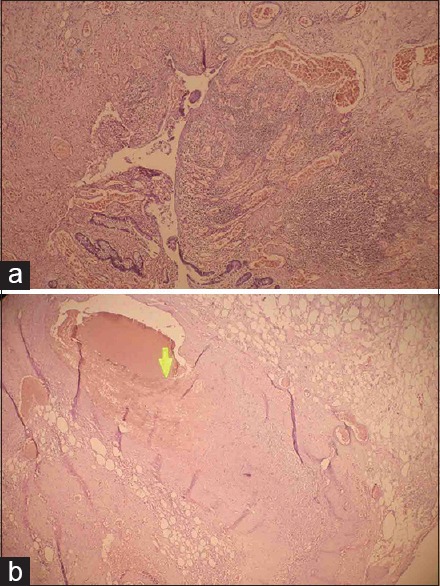
(a) Photomicrograph of small intestine showing focal ulceration of the mucosa with marked inflammatory cell infiltration and vascular congestion (H and E, ×40). (b) Photomicrograph of mesentery showing thrombus (arrow) in the mesenteric artery (H and E, ×40)
Figure 2.
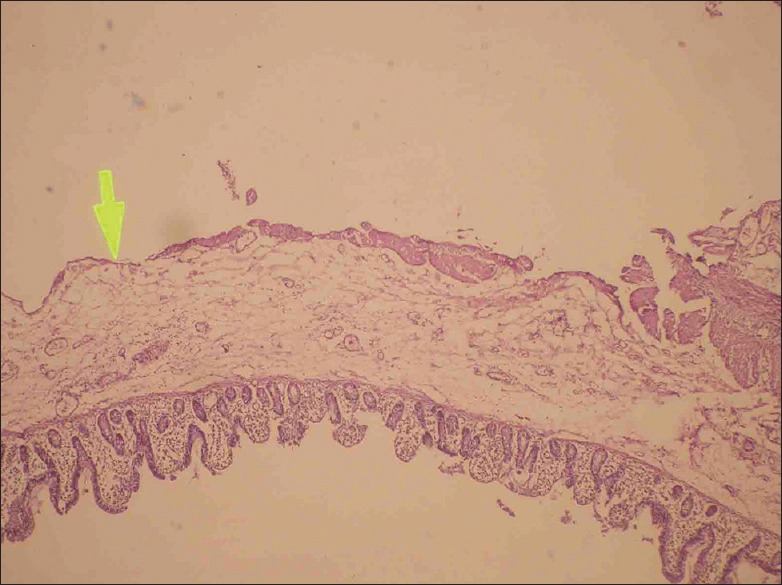
Photomicrograph of small intestine showing absence (arrow) of muscularis propria (H and E, ×40)
The patient subsequently developed abdominal fistula and was subjected to computed tomography angio based on the histopathology report of thrombosed artery. It revealed dilated small bowel loops in mid and left side of lower abdomen, proximal mesenteric artery was normal in caliber, distal superior mesenteric artery wall was irregularly thickened causing 60% narrowing of the lumen with thrombosis of few branched vessels [Figure 3]. The patient was advised re-exploration that he refused and left against medical advice.
Figure 3.
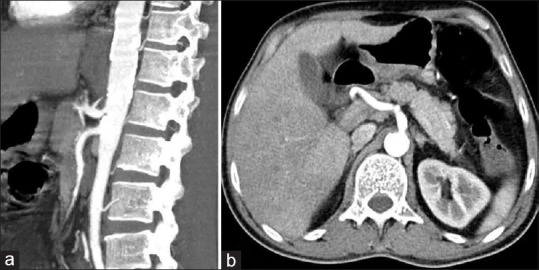
Photographs of computed tomography abdomen angiography sagittal (a) and axial (b): Calcified plaques in the abdominal aorta with focal narrowing of the celiac trunk at origin approximately 50% seen. There is normal caliber and flow in proximal superior mesenteric artery (SMA) with irregular slight thickening of SMA wall causing narrowing of SMA approximately 60%, mesenteric fat stranding in lower abdomen
DISCUSSION
Segmental absence of the intestinal musculature or segmental congenital defect of intestinal musculature is a rare clinical entity. Most of the patients are from neonatal age group and present as intestinal obstruction along with other associated congenital anomalies like patent ductus arteriosus, biliary atresia, intestinal atresia and ventricular septal defect.[2] The cases have presented with intestinal perforation, intussusception, and volvulus.[2] The present case is of Secondary group of SAIM in an adult. There was no association of any congenital anomaly in our case. The preoperative diagnosis is not possible in these cases, and the diagnosis is only possible on postoperative pathologic specimen provided the pathologists are aware of the condition.[2] However, it is suggested that transillumination of the intestinal wall may be helpful to identify the defect during the surgical procedure.[9] So in clinical set up of the cases of intestinal obstruction and/or perforation not only in neonates but also in higher age group, SAIMs may be one of the differential diagnosis if the patient has repeated recurrences of the symptoms as is seen in our case.
There have been several proposed theories of pathogenesis of SAIM such as:[4]
A normal embryogenesis leading to incomplete or dicontinuous myogenesis[3]
An ischaemic event during fetal life or postnatally leading to injury of mucosa or muscularis propria, and differences in regenerative capacity between mucosa and muscle, in which mucosa rather than muscle regenerates, resulting in exclusive absence of the musculature. A noteworthy fact is that animal studies have not yet been successful in producing such lesion. Ligation of the mesenteric vessel causes intestinal atresia involving all the three layers of intestinal wall[3,10]
Genetic and familial factors have been postulated in some cases, however, some investigators do not support this theory as there is not enough evidence[3,10]
Some authors believe that this malformation could be a relic of developmental diverticula in the embryonic small bowel. Others believe that it could also result from resorption of ileal muscle at the time of regression of omphalomesenteric duct, considering the frequency of proximity to the site of Meckel's diverticula.[10]
The present case is 48-year-old and did not have history of any other ailment. He was nondiabetic, nonhypertensive and developed intestinal perforation at the age of 48 years. The thrombosis in the vessels suggests that it may be a benign congenital anomaly and ischemia may be the cause of perforation as agreed upon by majority of the authors but still the etiology is controversial.
In summary, SAIM remain puzzling and challenging disease with variable clinical presentation not only in neonates but also in higher age group and adults and the pathologists as well as clinicians should be aware of the condition, especially, when repeated complications are developing in a patient of intestinal obstruction and/or perforation.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Emanuel B, Gault J, Sanson J. Neonatal intestinal obstruction due to absence of intestinal musculature: A new entity. J Pediatr Surg. 1967;2:332–5. doi: 10.1016/s0022-3468(67)80213-6. [DOI] [PubMed] [Google Scholar]
- 2.Davis JS, Ryan ML, Shields JM, Sola JE, Perez EA, Neville HL, et al. Segmental absence of intestinal musculature: An increasingly reported pathology. J Pediatr Surg. 2012;47:1566–71. doi: 10.1016/j.jpedsurg.2012.01.002. [DOI] [PubMed] [Google Scholar]
- 3.Tawfik O, Newell B, Lee KR. Segmental absence of intestinal musculature in an adult. Dig Dis Sci. 1998;43:397–9. doi: 10.1023/a:1018879011103. [DOI] [PubMed] [Google Scholar]
- 4.Aldalati O, Phelan C, Ibrahim H. Segmental absence of intestinal musculature (SAIM): A case report in an adult. BMJ Case Rep. 2009:2009. doi: 10.1136/bcr.01.2009.1425. pii: bcr01.2009.1425. doi: 10.1136/bcr.01.2009.1425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Herbut PA. Congenital defect in musculature of stomach with rupture in a newborn infant. Arch Pathol. 1943;36:91–4. [Google Scholar]
- 6.Procházka V, Svoboda T, Soucek O, Kala Z. Segmental absence of the muscularis propria layer in the colonic wall – A rare cause of colonic perforation during pregnancy. Rozhl Chir. 2010;89:679–81. [PubMed] [Google Scholar]
- 7.Husain AN, Hong HY, Gooneratne S, Muraskas J, Black PR. Segmental absence of small intestinal musculature. Pediatr Pathol. 1992;12:407–15. doi: 10.3109/15513819209023319. [DOI] [PubMed] [Google Scholar]
- 8.Dzieniecka M, Grzelak-Krzymianowska A, Kulig A. Segmental congenital defect of the intestinal musculature. Pol J Pathol. 2010;61:94–6. [PubMed] [Google Scholar]
- 9.Dhall JC, Khatri HL, Jaiswal TS, Sekhon GS. Congenital segmental absence of intestinal musculature: A rare cause of intestinal obstruction in a neonate. Am J Gastroenterol. 1978;70:401–3. [PubMed] [Google Scholar]
- 10.Darcha C, Orliaguet T, Levrel O, Pezet D, Lointier P, Chipponi J, et al. Segmental absence of colonic muscularis propria. Report of a case in an adult. Ann Pathol. 1997;17:31–3. [PubMed] [Google Scholar]