

Abstract
Objective:
The knowledge, attitude, practice (KAP) studies play an important role in promotion of oral health. The aim of this study was to assess oral health KAP in 12-year-old schoolchildren in Iran.
Materials and Methods:
In a cross-sectional study on 1554 students aged 12 years from the rural and urban areas of five provinces, KAP of subjects was assessed using a culturally adapted questionnaire. Data were analyzed using Chi-squared test, t-test, correlation coefficient, analysis of variance (ANOVA), and linear regression. Statistical significance was set at P < 0.05.
Results:
In general, the scores of students in knowledge, attitude, and practice were 74.1 ± 21.1%, 72.6 ± 21.1%, and 51.8 ± 12%, respectively. Urban students had significantly higher scores in KAP (P = 0.0001). Female students got higher scores in all the three dimensions, but the difference was significant only in brushing practice (P = 0.006). Students in Tehran (the capital city) had significantly higher scores in all fields (P = 0.0001). Parents’ education and mothers’ job had a significant relationship with KAP of children.
Conclusion:
The results of this study showed that 12-year-old schoolchildren in Iran had good knowledge and positive attitude. But oral health practice was not satisfactory.
Keywords: Attitude, Iran, knowledge, oral health, practice
INTRODUCTION
Recent studies show that the rate of dental caries is on the rise globally.[1] Many factors such as changing patterns of sugar consumption and lifestyle might be responsible for the increase in caries rates, especially in developing countries.[2,3,4]
In Iran, despite the high rate of dental caries in 12 years (52.3%),[5] socio-epidemiologic data about oral health behaviors are not available at a national level. Therefore, this study was undertaken to collect information about oral health knowledge, attitude, and practice (KAP) of 12 years in different regions of Iran.
MATERIALS AND METHODS
This study was a cross-sectional survey of 1691 students studying in sixth grade (12 years of age) in various schools of five provinces (seven urban and eight rural areas) of Iran. A stratified sampling procedure was performed per province and cluster (school). In each stratum, a number of schools were selected and in each school, a random sample proportional to the number of students per school was selected. To obtain a national representative sample, the capital of Iran (Tehran) and four provinces (Khorasan in the northeast, Isfahan in the center, Hormozgan in the south, and Kerman in the southeast) were selected.
A questionnaire that included 33 closed-ended questions was designed based on a systematic review of related articles and was translated and back-translated in the standard method from English to Persian. The final version was evaluated by pediatric dentists and epidemiologists. For assessment of face validity and reliability, a pilot study was carried out on 30 students of sixth grade with an interval of 3 weeks (the consistency rate was over 80%). For assessment of validity, Cronbach's alpha was calculated, which was at an acceptable level (0.88).
Finally, the Persian version was designed to include demographic data and issues in the field of KAP.
With coordination of the school principal and after student satisfaction was ensured, the questionnaires were completed by the children in school under the teachers’ supervision. The sample size was 1691 students, with a response rate of about 92% as the incorrectly filled 137 questionnaires were excluded from the analysis.
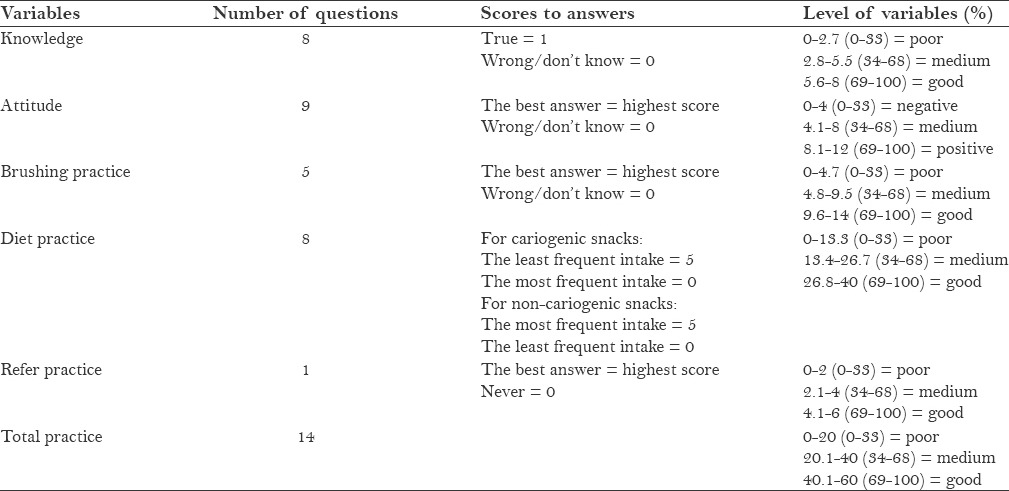
Oral health KAP was measured based on true answers to the questions related to each variable [Table 1].
Table 1.
The method of calculating the scores of knowledge, attitude, and practice on oral health
Data were analyzed with SPSS 21 using Chi-squared test, t-test, correlation coefficient, analysis of variance (ANOVA), and linear regression model. A P value of < 0.05 was considered significant.
RESULTS
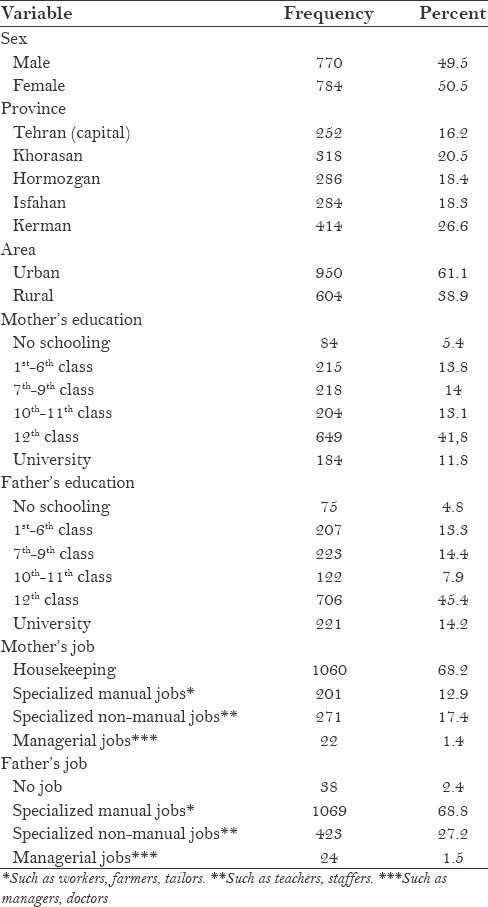
In this study, 1554 students were recruited, with 49.5% males and around 61% from urban areas [Table 2].
Table 2.
The basic demographic features of the subjects
The mean knowledge score was 74.1 ± 21.1%. Only 72 (4.7%) of students had poor knowledge [Figure 1].
Figure 1.
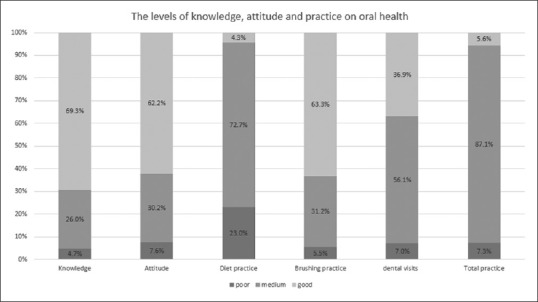
The levels of KAP on oral health in 12-year-olds
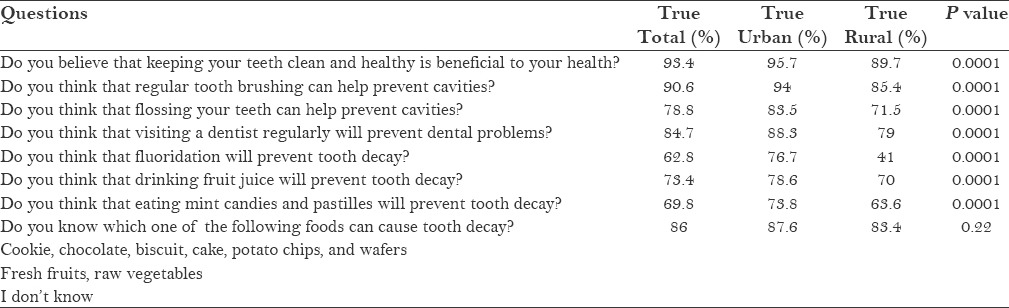
The results of the analysis of knowledge questions are presented in Table 3. These results show that some of the subjects were unaware that drinking fruit juice (26.6%) and eating candies and pastilles (30.2%) can cause dental caries.
Table 3.
The percent of the true responses to knowledge questions according to living in urban and rural regions
The mean score of attitude was 72.6 ± 21.1%. Only 116 (7.6%) of subjects had a negative attitude [Figure 1]. Approximately 91.8% of students believed that it was important for them to take care of their teeth. But 43.6% of them reported that they did not have a good feeling about dental visits.
Around 87% of students had medium practice [Figure 1]. The mean score of total practice was 51.8 ± 11.9%. Of the study sample, 94.9% had a toothbrush and 79.8% used it with toothpaste to brush. Unfortunately, 5.1% had no toothbrushes. Most of the students (48.7%) brushed their teeth once daily. Only 8.1% brushed their teeth at least twice daily. The results showed that 53.7% of the population visited a dentist when they had pain or a dental problem. Only 15.1% visited their dentists every 6 months for the control of oral and dental health.
Approximately 27.3% of students consumed sweet foods (chocolate/cake/biscuit/chips) and 43% of them drank soft drinks (sugared tea or coffee or milk/soda/syrup) several times a day. But the habit of having fresh fruit and raw vegetables several times a day was reported by 15% of subjects.
There was a significant association between knowledge and attitude and practice. Minimum correlation coefficients (r = 0.05) and (r = 0.11) were between attitude and knowledge with diet practice, respectively.
In general, the students in urban areas obtained higher scores in KAP (P = 0.0001). The mean scores in urban areas of different provinces were significantly lower than in Tehran, the capital of Iran. These scores were significantly lower in rural areas in Khorasan than in other provinces [Figure 2].
Figure 2.
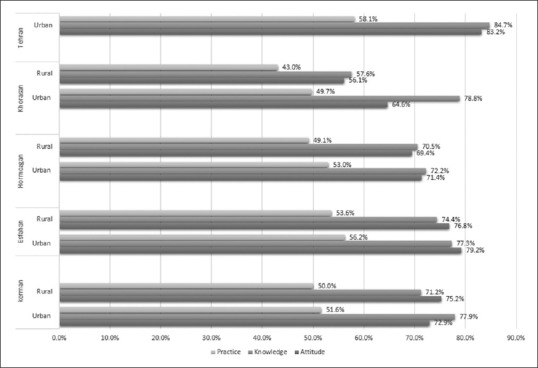
The mean of scores of oral health KAP in urban and rural areas of different provinces
Female students exhibited higher scores in all fields, but the difference was significant only in brushing practice (P = 0.006).
The results of multivariate analysis of practice of oral health are presented in Table 4. This analysis showed that children whose mothers had higher education obtained higher scores in all fields. Children whose fathers had higher education showed significantly better brushing, but the difference was not significant in relation to diet and referral practice.
Table 4.
Prediction of the total practice score in the multivariate regression model
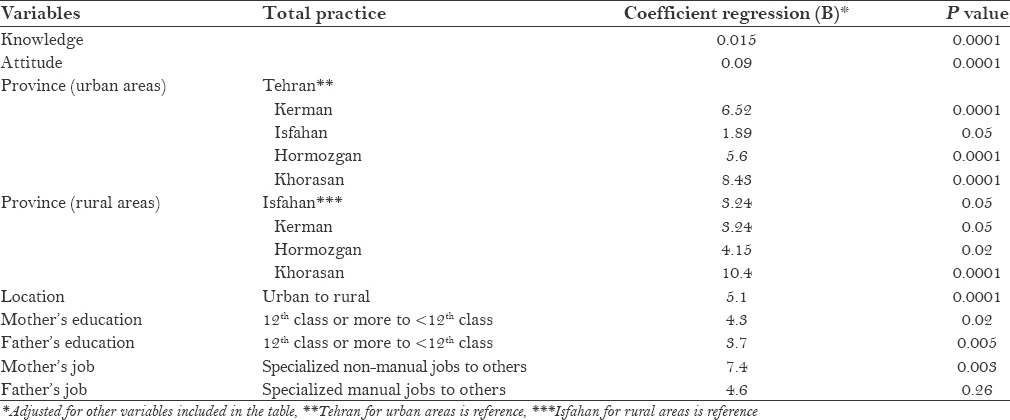
Children whose mothers were employed obtained significantly higher scores in comparison with the children of housewives. The fathers’ job did not have a significant association with the KAP of students.
DISCUSSION
In general, the results of this study indicate that the levels of knowledge and attitude were good, but the level of practice was not satisfactory, especially diet-related practice. Although it was found that awareness about the effect of excess sweets or soft drinks was high (86%), 43% of children consumed soft drinks and 27.3% ate sweet food several times a day. This can explain that oral health knowledge does not necessarily relate to better health behavior. Other studies have confirmed the finding that the association of KAP of oral health cannot be understood simply based on the KAP chain, and other factors such as socioeconomic factors, especially parents’ education level and region where the children live should also be considered.[2,6]
In this study, the KAP of urban students was significantly more than that of rural students. Studies conducted in rural areas show that the effect of knowledge on oral health was negligible.[3,6,7] This may be due to factors such as socioeconomic status and better coverage of the oral healthcare programs. Also, the effect of KAP on oral health is influenced by the province of residence.[3] In this study, Tehran (capital of Iran) exhibited the highest mean scores. Therefore, it seems the province health authorities should be encouraged to develop school-based educational programs including parents and teachers.
In the present study, we assessed the effect of parents’ jobs and education on KAP of children. The results showed that employed mothers had an effective role in increasing KAP in children, but there was no association with fathers’ job. However, there are no studies about the effect of parents’ job on KAP of children to compare the results of our study. Also, parents’ educational level had a significant relationship with KAP on oral health. This finding was similar to other studies.[6,8] It is natural that educated parents improve their children's oral health.
In this study, unfortunately, 5.1% had no toothbrushes, which was lower compared to a study in Iraq, in which 78.1% of children used a toothbrush and 16.6% reported using their fingers instead.[9] In our study, 8.1% of the students brushed their teeth at least twice daily. This finding was higher compared to the finding of a study conducted in Dehradun, India,[10] in which 4.1% of children brushed their teeth twice a day. However, both studies reported a very low percentage of people brushing their teeth twice a day, compared to other studies. Approximately 38.5% of 12-year-olds in Bangalore, India,[4] half of the children and adolescents in China and European countries,[3] 61% of children in Nairobi,[11] and 30% of 12-year-olds in Sudan brushed their teeth at least twice a day.[12] However, the low rate of the number of daily tooth brushing might be attributed to poor knowledge, which can lead to faulty practice.
In our study, 78.8% of children knew the effect of dental flossing was to prevent dental caries, which was higher compared to the rates in Udaipur, India (48.1%)[13] and in Jordan (40%);[14] however, despite the high knowledge, only 60.1% of students used dental floss.
The knowledge among the children in our study about the effect of fluoride on teeth (62.8%) was lower compared to that among the students (77%) in Jordan,[14] but was higher compared to that of children from China (37%)[15] and Udaipur in India (12.6%).[13]
In our sample, although 84.7% of the students were aware of the importance of regular dental visits, only 35.3% reported that they have visited a dentist during the last 6 or 12 months, 4.4% of students did not visit any dentist, and 53.7% visited a dentist if they had pain or a problem in their teeth or gums. This finding is in line with the results of a study in India, in which 67.8% were aware of the importance of regular dental visits and 35.1% had visited a dentist during the last 12 months.[4]
In our sample, 43.6% of participants reported that they did not have a good feeling about dental visits. In a study in India,[4] 46.1% of 12-year-olds feared dental visits, which was the main cause of irregular visits by these students. In Jordan, 28% of 14–15-year-olds reported that they feared dental visits.[14] Therefore, based on these studies and our study, it seems that an unpleasant feeling about or fear of dental visits is the main reason for irregular visits to dentists.
However, this study might have had certain limitations.First, the information was collected by a questionnaire, and the subjects might have overestimated positive practices and underestimated negative behaviors. Second, recall bias should be considered, probably occurring in relation to the past dental visits and diet history.
CONCLUSION
The results of this study show that 12-year-olds in Iran had good knowledge and positive attitude. But oral health behaviors were not satisfactory. The results also show that oral health behaviors are not totally explained by knowledge and attitude, and are influenced by parents’ educational level and region where the children live.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This work was supported by Kerman Oral and Dental Diseases Research Center, Kerman University of Medical Sciences, Kerman, Iran. Also, the authors would like to thank Dr. Sudabeh Lotfi, Dr. Razieh Sedaghat, Dr. Ashkan Faryad, and Dr. Siavash Faryad for their assistance in data collection.
REFERENCES
- 1.Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. 2009;22:3–8. [PubMed] [Google Scholar]
- 2.Suprabha BS, Rao A, Shenoy R, Khanal S. Utility of knowledge, attitude, and practice survey, and prevalence of dental caries among 11- to 13-year-old children in an urban community in India. Glob Health Action. 2013;6:20750. doi: 10.3402/gha.v6i0.20750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX. Oral health knowledge, attitudes and behaviour of children and adolescents in China. Int Dent J. 2003;53:289–98. doi: 10.1111/j.1875-595x.2003.tb00762.x. [DOI] [PubMed] [Google Scholar]
- 4.Harikiran AG, Pallavi SK, Hariprakash S, Ashutosh, Nagesh KS. Oral health-related KAP among 11- to 12-year-old school children in a government-aided missionary school of Bangalore city. Indian J Dent Res. 2008;19:236–42. doi: 10.4103/0970-9290.42957. [DOI] [PubMed] [Google Scholar]
- 5.Pakshir HR. Oral health in Iran. Int Dent J. 2004;54(Suppl 1):367–72. doi: 10.1111/j.1875-595x.2004.tb00013.x. [DOI] [PubMed] [Google Scholar]
- 6.Smyth E, Caamano F, Fernández-Riveiro P. Oral health knowledge, attitudes and practice in 12-year-old schoolchildren. Med Oral Patol Oral Cir Bucal. 2007;12:E614–20. [PubMed] [Google Scholar]
- 7.Mafuvadze BT, Mahachi L, Mafuvadze B. Dental caries and oral health practice among 12 year old school children from low socio-economic status background in Zimbabwe. Pan Afr Med J. 2013;14:164. doi: 10.11604/pamj.2013.14.164.2399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Petersen PE, Jiang H, Peng B, Tai BJ, Bian Z. Oral and general health behaviours among Chinese urban adolescents. Community Dent Oral Epidemiol. 2008;36:76–84. doi: 10.1111/j.1600-0528.2007.00375.x. [DOI] [PubMed] [Google Scholar]
- 9.Ahmed NA, AstrømAstrøm AN, Skaug N, Petersen PE. Dental caries prevalence and risk factors among 12-year old schoolchildren from Baghdad, Iraq: A post-war survey. Int Dent J. 2007;57:36–44. doi: 10.1111/j.1875-595x.2007.tb00116.x. [DOI] [PubMed] [Google Scholar]
- 10.Diwan S, Saxena V, Bansal S, Kandpal SD, Gupta N. Oral health: Knowledge and practices in rural community. Indian J Community Comm Health. 2011;22:29–33. [Google Scholar]
- 11.Gathecha G, Makokha A, Wanzala P, Omolo J, Smith P. Dental caries and oral health practices among 12 year old children in Nairobi West and Mathira West Districts, Kenya. Pan Afr Med J. 2012;12:42. [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 12.Nurelhuda NM, Trovik TA, Ali RW, Ahmed MF. Oral health status of 12-year-old school children in Khartoum state, the Sudan; a school-based survey. BMC Oral Health. 2009;9:15. doi: 10.1186/1472-6831-9-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sharda AJ, Shetty S, Ramesh N, Sharda J, Bhat N, Asawa K. Oral health awareness and attitude among 12-13 year old school children in Udaipur, India. Int J Dent Clin. 2011;3:16–9. [Google Scholar]
- 14.Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70:179–87. [PubMed] [Google Scholar]
- 15.Wong MC, Lo EC, Schwarz E, Zhang HG. Oral health status and oral health behaviors of Chinese children. J Dent Res. 2001;80:1459–65. doi: 10.1177/00220345010800051501. [DOI] [PubMed] [Google Scholar]