

Abstract
Aim:
The aim was to determine the frequency and distribution of oral squamous cell carcinoma (OSCC) involving tongue among patients by studying biopsy specimens obtained from the archives of the Department of Oral and Maxillofacial Pathology, College of Dental Sciences, Davangere, Karnataka, India, during the past 13 years.
Methodology:
Data for the study were retrieved from the case records of patients. Analyzed clinical variables included age, sex, anatomical site, and histological diagnosis.
Results:
Of the 369 squamous cell carcinoma involving head and neck region, we found 52 biopsies reported exclusively involving tongue. Lateral border of the tongue was most commonly involved (43 cases, 82.7%), followed by base of tongue and posterior part of tongue. The patient were affected over a wide range of 27–80 years with mean age of 55.75 years and peak incidence was seen in the fourth and fifth decades of life, with the male: female ratio of 1.7:1.
Conclusion:
The prevalence rate of OSCC involving tongue showed a definite geographic variation when compared with a study done in other parts of the world.
KEY WORDS: Lateral border of tongue, oral squamous cell carcinoma, tongue carcinoma
The oral cavity has been frequently exposed to various carcinogenic agents, specifically tobacco, alcohol, betel nut, and human papillomavirus (HPV) and through the oral cavity, these agents are exposed to digestive and respiratory tract. Head and neck squamous cell carcinomas are a biologically heterogeneous group of cancers. They are a major source of cancer morbidity and mortality worldwide, especially in the Indian subcontinent. Oral squamous cell carcinoma (OSCC) comprises more than 90% of head and neck malignancies.[1] OSCC is an important source of morbidity and mortality worldwide with an incidence rate that varies widely by geographic location.[2]
According to the reports of the World Health Organization (WHO), oral cancer ranks sixth among all malignancies worldwide.[3] In spite of advances in treatment, there has been no considerable drop in the mortality rate. Cancers of the tongue as well as buccal mucosa have been noted to be quiet common in India, attributed to the local custom of chewing pan, betel leaf with tobacco.[4]
Despite the large number of studies on OSCC in the literature, details on the demographic profile of these lesions in different populations are limited, especially in the Indian population. Thus, the purpose of this retrospective study was to identify any trends in the number of cases or incidence rates at specific anatomic sites or within specific age or gender groups in the occurrence of OSCC of tongue in the south Indian sample population over a period of 13 years in Davangere and the surrounding districts of Karnataka, India.
Methodology
A retrospective study on OSCC was conducted on the basis of oral biopsy specimens retrieved from the archives of the Department of Oral and Maxillofacial Pathology, College of Dental Sciences, Davangere, India, available from the year January 2001 through December 2013. The age, sex, and anatomical site of all cases were compiled from the clinical data sent together with the biopsy records. Histopathology slides stained with hematoxylin and eosin were selected and re-evaluated according to the current concepts outlined by the WHO.[3]
Inclusion criteria involved the histological confirmation of OSCC. Lesions with histological findings that were not compatible with OSCC were excluded from the study. Some records that were sent with the biopsy material were inadequate and were omitted. The following variables were recorded:
Age
Sex
Anatomical site.
The following anatomical sites were defined as:
Anterior - Defined as the anterior segment of tongue from tip of tongue to anterior two-third of tongue (till sulcus terminalis)
Posterior - The posterior region was defined as the region posterior to sulcus terminals
Anterior-posterior segments - Defined as involving both the anterior and posterior segments
Right side of the tongue
Left side of the tongue
Lateral border of the tongue.
Data were subjected to descriptive statistical analyses with the SPSS version 16.0 statistical software package (SPSS Inc., Chicago, USA).
Results
Age and sex
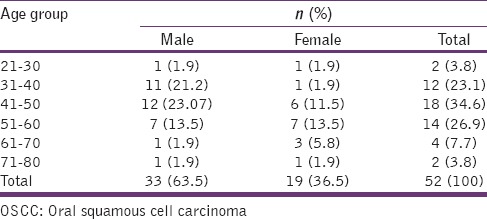
Thirty-three cases (63.5%) of tongue OSCC were observed in men and 19 cases (36.5%) were seen in women, with a male: female ratio of 1.7:1. The mean age in male was 47.3 years, (27–80) while in female it was 53.9 years (30–75). Overall mean age was 55.75 years (range: 27–80 years), with 18 cases (34.6%), 14 cases (26.9%), and 12 cases (23.1%) being diagnosed in the fourth, fifth, and third decades of life, respectively [Table 1].
Table 1.
Age Distribution of the patients with OSCC of the tongue
Prevalence and anatomical site
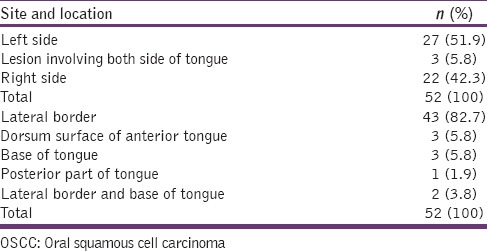
Among the 369 cases of OSCC, we found 52 cases (14.09%) were involving the tongue. Of the 52 tongue squamous cell carcinomas, 27 cases (51.9%) were involving the left side of the tongue, 22 cases (42.3%) were involving the right side, and 3 cases (5.8%) were involving both right and left side of the tongue. When anatomical sites were analyzed, the most commonly affected site was the lateral border the tongue (43 cases, 82.7%), followed by dorsum surface of anterior tongue and base of the tongue (3 cases each, 5.8%), while l case was observed in the posterior part of the tongue (1 case, 1.9%) [Table 2].
Table 2.
Site and location of OSCC of the tongue
Histological variation
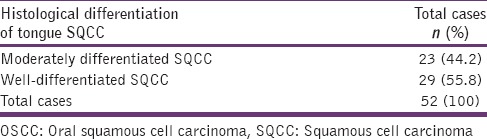
When histological grading of the squamous cell carcinoma was compared, we noticed that 29 cases (55.8%) were showing well-differentiated carcinoma and 23 cases (44.2%) were moderately differentiated squamous cell carcinoma [Table 3].
Table 3.
Site and location of OSCC of the tongue
Discussion
Considering that 95% of the head and neck cancers are squamous cell carcinomas, clinical behavior varies according to their location. The carcinoma of the tongue represents 25% to 50% of all cases of OSCC,[5] with the lateral borders and the anterior two-thirds being the most commonly affected locations.
Though the collective effects of tobacco and alcohol consumption may increase the risk of developing carcinoma[6,7] yet, few factors such as HPV, diet, and genetic factors also plays an important role in the development of carcinoma in patients without history of drinking and smoking.[6,7,8,9,10]
Epidemiology studies have shown that the sites of occurrence for oral cancer differ widely and tongue, lip, and floor of the mouth are the most frequent sites of lesions of OSCC in the oral cavity.[11,12]
Table 4 enumerates the worldwide epidemiological studies done on tongue squamous cell carcinoma.[13,14,15,16,17,18] Shenoi et al. found 18.31% cases involving tongue,[12] while Sharma et al.[13] found 3 cases (3.75%) involving tongue SQCC in his study. In our study, we found that 52 OSCC cases (14.09%) were involving tongue. This variation could be due to the variation in number of samples as well as different levels of tobacco and alcohol exposure, socioeconomics circumstances, etc.
Table 4.
Summary of studies and cases reporting OSCC involving tongue cited in English literature

Albuquerque et al.[14] found that the lateral borders of the tongue were the most frequent carcinoma locations in both groups (drinking and smoking persons as well as nondrinking and nonsmoking subjects). According to them, lateral border showed 59.7% and 40.3% in user and nonusers, respectively.[14] Falaki et al.[15] analyzed 158 cases of OSCC and found that the most common site of involvement was the tongue (66%) and lateral border of the tongue.[15] These results are similar to present study results as we also found a most frequent site to be the lateral border of tongue 82.7%.
Considering the histological grading of tongue OSCC, we found that well-differentiated SQCC accounted for 23 cases (44.2%), while moderately differentiated SQCC was seen in 29 cases (55.8%) and Agrawal et al.[18] found 10 cases (55.5%) of well-differentiated SQCC and 4 cases (22.2%) of moderately differentiated SQCC in his analysis.
Conclusion
Present study is to highlight the magnitude of OSCC involving the tongue. 14.09% of OSCC involves the tongue, and the lateral border of the tongue is more commonly involved. Men are affected more commonly, and the fourth decade is more commonly involved. Prevalence rate of tongue OSCC is different among the different populations globally, which could be due to the different level of tobacco and alcohol exposure, diet, socioeconomic status. Early detection and prevention of oral cancer helps in improving the quality and quantity of life of the patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Lawoyin JO, Lawoyin DO, Aderinokun G. Intra –oral squamous cell carcinoma in lbadan: A review of 90 cases. Afr J Med Sci. 1997;26:187–8. [PubMed] [Google Scholar]
- 2.Howell RE, Wright BA, Dewar R. Trends in the oral cancer in nova Scotia from 1983 to 1997. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:205–12. doi: 10.1067/moe.2003.49. [DOI] [PubMed] [Google Scholar]
- 3.Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics 1999. CA Cancer J Clin. 1999;49:8–31. doi: 10.3322/canjclin.49.1.8. [DOI] [PubMed] [Google Scholar]
- 4.Thomas G, Hashibe M, Jacob BJ. Risk factors for multiple oral premalignant lesions. Int J Cancer. 2003;107:285–91. doi: 10.1002/ijc.11383. [DOI] [PubMed] [Google Scholar]
- 5.Dantas DD, Ramos CC, Costa AL, Souza LB, Pinto LP. Clinicalpathological parameters in squamous cell carcinoma of the tongue. Braz Dent J. 2003;14:22–5. doi: 10.1590/s0103-64402003000100004. [DOI] [PubMed] [Google Scholar]
- 6.Dahlstrom KR, Little JA, Zafereo ME, Lung M, Wei Q, Sturgis EM. Squamous cell carcinoma of the head and neck in never smoker-never drinkers: A descriptive epidemiologic study. Head Neck. 2008;30:75–84. doi: 10.1002/hed.20664. [DOI] [PubMed] [Google Scholar]
- 7.Schmidt BL, Dierks EJ, Homer L, Potter B. Tobacco smoking history and presentation of oral squamous cell carcinoma. J Oral Maxillofac Surg. 2004;62:1055–8. doi: 10.1016/j.joms.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 8.Wight R, Paleri V, Arullendran P. Current theories for the development of nonsmoking and nondrinking laryngeal carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2003;11:73–7. doi: 10.1097/00020840-200304000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Goldenberg D, Lee J, Koch WM, Kim MM, Trink B, Sidransky D, et al. Habitual risk factors for head and neck cancer. Otolaryngol Head Neck Surg. 2004;131:986–93. doi: 10.1016/j.otohns.2004.02.035. [DOI] [PubMed] [Google Scholar]
- 10.Sturgis EM, Wei Q, Spitz MR. Descriptive epidemiology and risk factors for head and neck cancer. Semin Oncol. 2004;31:726–33. doi: 10.1053/j.seminoncol.2004.09.013. [DOI] [PubMed] [Google Scholar]
- 11.Barasch A, Morse DE, Krutchkoff DJ, Eisenberg E. Smoking, gender, and age a risk factors for site – specific intraoral squamous cell carcinoma. Cancer. 1994;73:509–13. doi: 10.1002/1097-0142(19940201)73:3<509::aid-cncr2820730303>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- 12.Shenoi R, Devrukhkar V, Chaudhuri, Sharma BK, Sapre Sb, Chikhale A. Demographic and clinical profile of oral squamous cell carcinoma patients: A retrospective study. Indian J Cancer. 2012;49:21–6. doi: 10.4103/0019-509X.98910. [DOI] [PubMed] [Google Scholar]
- 13.Sharma P, Saxena S, Aggarwal P. Trends in the epidemiology of oral squamous cell carcinoma in western UP: An institutional study. Indian J Dent Res. 2010;21:316–9. doi: 10.4103/0970-9290.70782. [DOI] [PubMed] [Google Scholar]
- 14.Albuquerque R, López-López J, Marí-Roig A, Jané-Salas E, Roselló-Llabrés X, Santos JR. Oral Tongue Squamous Cell Carcinoma (OTSCC): Alcohol and Tobacco Consumption versus Non-Consumption. A Study in a Portuguese Population. Braz Dent J. 2011;22:517–521. doi: 10.1590/s0103-64402011000600013. [DOI] [PubMed] [Google Scholar]
- 15.Falaki F, Dalirsani Z, Pakfetrat A, Falaki A, Saghravanian N, Nosratzehi T, Pazouki M. Clinical and histopathological analysis of oral Squamous cell carcinoma of young patients in Mashhad, Iran: A retrospective study and review of literatures Med Oral Patol Oral Cir Bucal. 2011 Jul 1;16:e473–7. doi: 10.4317/medoral.16.e473. [DOI] [PubMed] [Google Scholar]
- 16.Iype EM, Pandey M, Mathew A, Thomas G, Sebastian P, Nair MK. Oral cancer among patients under the age of 35 years. J postgrad Med. 2001;47:171–6. [PubMed] [Google Scholar]
- 17.Mehrotra R, Singh M, Kumar D, Pandey AN, Gupta RK, Sinha US. Age specific incidence rate and pathological spectrum of oral cancer in Allahabad. Ind J Med Sci. 2003;57:400–4. [PubMed] [Google Scholar]
- 18.Agarwal, AK, Sethi A, Sareen D, Dhingra S. Oral and oropharyngeal squamous cell carcinoma in our population: The clinic-pathological and morphological description of 153 cases. Int. J. Morphol. 2011;29:686–93. [Google Scholar]