

Abstract
Background: Health literacy is the ability to obtain, read, understand and use healthcare information to make appropriate health decisions and follow instructions for treatment. The aim of this study was to identify the effect of various factors on health literacy in patients with diabetes.
Methods: 407 patients with diabetes older than 15 years of age were identified from the Diabetes Clinic affiliated to the Institute of Endocrinology and Metabolism (IEM) of Iran University of Medical Sciences. We assessed patients' health literacy using the Persian version of Test of Functional Health Literacy in Adults (TOFHLA) questionnaire.
Results: Mean age of the patients was 55.8 ± 11.3 years, and 61.7% the participants were female.. Overall, 18.2% of the patients had adequate health literacy skills, 11.8% had marginal and 70.0% inadequate health literacy skills. Male participants performed better than females (p< 0.01) and older patients had lower health literacy score than younger patients (p< 0.001). Furthermore, patients with higher educational and occupational levels had higher functional health literacy score than those with lower levels (p< 0.001).
Conclusion: Health literacy score in Iranian patients with diabetes seems inadequate. Therefrom effective interventions should be designed and implemented for this group of patients to improve diabetes outcomes.
Keywords: Health literacy, Diabetes, Influencing Factors
Introduction
Health literacy is defined as "the degree to which individuals have the capacity to obtain, process, and understand basic health information needed to make appropriate health decisions (1). Health literacy consists of reading, writing, cultural and conceptual knowledge, the ability to apply numbers and decision making as needed to manage health situation (2-3). Recent studies found that health literacy is an important predictor of health behaviors, outcomes and self-care activities (4-9). It is noteworthy to add that there is a close relationship between poor health outcomes across chronic diseases and health literacy (10).
In 2014, the global prevalence of diabetes was estimated to be 9% among adults aged 18 and older (11). Based on a recent survey in Iran, the prevalence of diabetes has been estimated to be 11.3 % (12). Since diabetic patients need long-term care, health literacy can play an important role in the quality of the provided care. Those diabetic patients with a low literacy level had difficulty in understanding their conditions (13-14). Researchers have indicated that diabetic patients with low numeracy have higher BMI and cannot control their blood sugar properly. The most important factor is low self confidence in numeracy to control diabetes (15). Diabetic patients with inadequate health literacy are not able to read the information on drug boxes. Therefore, sight problems are increased among them (16). Illiterates pay significantly less attention to foot-caring and weight-control compared to the low-literates and literates (17).
Since little is known about health literacy in patients with diabetes in Iran, this study was conducted to identify the effect of various factors on health literacy in this group of patients in order to design better educational interventions.
Methods
Setting and Study Participants
The study was conducted in the Diabetes Clinic affiliated to Institute of Endocrinology and Metabolism (IEM) of Iran University of Medical Sciences. The study sample consisted of 407 consecutive diabetic patients who referred to the diabetes clinic. All patients were 15 years or older with type 1 or 2 diabetes. We excluded patients with vision or hearing problems. Ethical approval was granted by IEM Ethics Committee.
Measures
To measure health literacy, the Persian version of TOFHLA (Test of Functional Health Literacy in Adults) was used (18).
The first part of the questionnaire dealt with patients’ demographic information (age, gender, level of education, occupation, marital status). The other two parts assessed their ability in reading comprehension and numeracy skill.
The TOFHLA takes approximately 30 minutes to administer. The TOFHLA and S-TOFHLA are timed reading comprehension tests that use the modified cloze procedure, in which every 5th to 7th word in a passage is omitted and replaced with a blank space. The patient should select a word to fit into the blank spaces from the 4 multiple-choice options provided for each space. The TOFHLA is scored on a scale of 0 to 100.Patients are categorized as having adequate, marginal, and inadequate health literacy by two point scores of 59 and 74.
The questionnaire measures reading comprehension ability and consists of three passages and 50 questions. All participants had 20 minutes to fill out the blanks with appropriate answers. The first part of the reading passage was about instructions for preparing upper gastrointestinal tract radiograph series. The second and third parts of reading passages were about patients’ rights and responsibilities in insurance and hospital consent forms, respectively. The part of numeracy skill consists of some description about medication, the results of laboratory tests and appointment. After 10 minutes, the participants answered 17 questions based on cue cards. All the individuals signed an informed consent.
Statistical Analyses
Data were entered into SPSS (version 17). Chi square, ANOVA, and student t-test were used to compare mean values. P values less than 0.05 were considered as statistically significant.
Results
Four hundred seven patients with the Mean±SD age of 55.85 ±11.3 years, ranging from 18 to 82 years were identified by the diabetes clinic as potentially eligible for the study. Among them, 251 (61.7%) were female, and 85.9% were married. There was a significant difference in educational level among genders (Table 1). Females had lower educational level compared to males (p<0.001), and 53.1% of them were housekeepers. There was a significant relationship between occupational status and educational level (p<0.001) (Table 2). Health literacy score means were 47.1 and 38.9 out of 100 in male and female participants, respectively. Patients with higher educational level and employed patients had higher health literacy score (p< 0.001). Tukey’s post hoc test revealed that employed patients had high health literacy compared to housekeepers (p< 0.001). Tukey’s post hoc test have shown that patients with low health literacy level were significantly less educated than others (p< 0.001).
Table 1 . Frequency of education status in diabetic patients based on gender .
| Education Status | Male N (%) | Female N (%) | Both N (%) | p |
| Illiterate | 14(9.0) | 49(19.9) | 63(15.7) | 0.003 |
| Incomplete school | 73(46.8) | 120(62.2) | 193(48) | |
| Diploma | 38(24.4) | 52(21.1) | 90(22.4) | |
| University | 31(19.9) | 25(10.2) | 56(13.9) | |
| Total | 156(100.0) | 246(100.0) | 402(100.0) |
Table 2 . Characteristics of patients stratified by two types of health literacy .
| Characteristics | Reading Comprehension Mean±sd | p | Numeracy Skill Mean±sd | p | Total score Mean±sd | p |
| Male | 17.9±16.8 | 0.07 | 29.2±14.0 | 0.001 | 47.1±27.9 | 0.006 |
| Female | 14.9±16.1 | 24.0±15.7 | 38.9±29.5 | |||
| Total | 16.05±16.43 | ------- | 26.0±15.3 | ------- | ------- | |
| Employed subjects | 24.4±18.0 | ‹0.001 | 33.2±14.3 | ‹0.001 | 57.6±29.2 | ‹0.001 |
| Unemployed subjects | 16.5±18.8 | 27.5±15.7 | 44.0±32.0 | |||
| House keeper | 12.3±14.9 | 21.9±16.0 | 34.2±28.1 | |||
| Others | 17.69±15.8 | 29.14±12.6 | 46.84±25.3 | |||
| Total | 15.94±16.42 | ------- | 25.9±15.3 | ------- | ------- | |
| Married | 15.9±16.1 | 0.6 | 26.3±14.8 | 0.1 | 42.2±28.2 | 0.6 |
| Single | 16.87±18.4 | 23.47±17.8 | 40.4±34.0 | |||
| Total | 16.02±16.44 | ------- | 25.93±15.3 | ------- | ------- | |
| Illiterate | 0.0±0.0 | ‹0.001 | 0.0±0.0 | ‹0.001 | 0.0±0.0 | ‹0.001 |
| Incomplete school | 10.45±12.0 | 26.2±1.2 | 36.65±20.4 | |||
| Diploma | 26.98±14.6 | 35.6±7.39 | 62.58±19.6 | |||
| University | 35.19±12.8 | 38.25±6.82 | 73.44±17.3 | |||
| Total | 16.0±16.43 | ------- | 25.9±15.3 | ------- | ------- |
of the patients, 70% had inadequate health literacy level and 18.2% and 11.8% of the patients had adequate and marginal literacy levels, respectively (Table 3). There was a correlation between the ability of reading comprehension and numeracy skill. (Pearson correlation coefficient=0.61, p<0.001)
Table 3 . Number of Patients Admitted to Hospitals in Different Age Groups during 2008-2009 .
| Characteristics | Inadequate N (%) | Marginal N (%) | Adequate N (%) | Total N (%) | p |
| Male | 106(67.9) | 14(9.0) | 36(23.1) | 156(100.0) | 0.07 |
| Female | 179(71.3) | 34(13.5) | 38(15.1) | 251(100.0) | |
| Employed subjects | 34(48.6) | 9(12.9) | 27(38.6) | 70(100.0) | ‹0.001 |
| Unemployed subjects | 8(66.7) | 1(8.3) | 3(25.0) | 12(100.0) | |
| House keeper | 169(78.2) | 24(11.1) | 23(10.6) | 216(100.0) | |
| Others | 70(68.6) | 13(12.7) | 19(18.6) | 102(100.0) | |
| Married | 249(71.6) | 39(11.2) | 60(17.2) | 348(100.0) | 0.2 |
| Single | 35(61.4) | 8(14.0) | 14(26.4) | 57(100.0) | |
| Illiterate | 63(100.0) | 0(0.0) | 0(0.0) | 63(100.0) | ‹0.001 |
| Incomplete school | 170(88.1) | 15(7.8) | 8(4.1) | 193(100.0) | |
| Diploma | 35(38.9) | 26(28.9) | 29(32.2) | 0(100.0) | |
| University | 14(25.0) | 6(10.7) | 36(64.3) | 56(100.0) |
In this study, health literacy was not associated with HbA1c. The peak of health literacy was observed among the patients with the age range of 18-29. As shown in Fig. 1, adequate health literacy is associated with lower ages.
Fig. 1 .
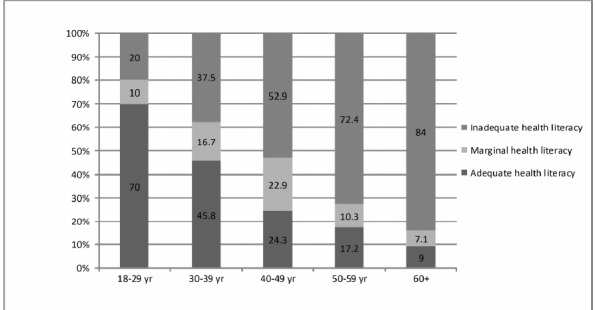
Distribution of Health Literacy in Age Groups
Discussion
In this study, 70% of diabetic patients had inadequate health literacy level, and 18.2% had adequate health literacy level. Nurss et al. have shown that among 131 African-American diabetic patients, 47% and 25% in new and old cases had adequate practical health literacy (19).
Based on a study conducted in Iranian population, 57% of the participants had inadequate health literacy compared to the general population (18). It seems that the diabetic patients have lower health knowledge. The level of health literacy was lower in female diabetic patients compared to the male. Also, level of health literacy was decreased with the increase in age. The peak was observed among the patients with the age range of 18-29.
In the present study, no association was found between health literacy level and HbA1c. Moreover, another study conducted on Iranian diabetic patients in 2007 found no significant difference in the level of HbA1C among the three groups of participants (17).
Trief et al. assessed the relationship between marital quality and HbA1c in diabetic patients using three questionnaires, Spanier Dyadic Adjustment Scale, Personal Assessment of Intimacy in Relationships Scale and HRQoL found no relationship between them (20).
Pala et al. used two generic quality of life instruments(SF-36 and WHOQOL-BREF) in diabetic patients, and HbA1c did not show any relationship with any of the domains of the instruments (21).
In the present study, there was a significant association between occu-pational status and health literacy level as all students had adequate health literacy level. However, the regression analyses did not show any significant difference in occupation groups "employed subjects, unemployed and housekeepers"
It is noteworthy to mention that house keepers and those with a high school diploma were at risk for diabetes outcomes more than others due to inadequate health literacy. It seems that providing appropriate education to patients with inadequate health literacy can be useful.
National Work Group on Literacy and Health in United States, addresses the failure of elementary schools to produce adults who are sufficiently literate to participate in health issues (22).
In health care services, physicians have the responsibility to provide enough education to the patients (23). It seems that non- written tools are useful in learning. Using some methods which include picture, video and computer software are effective.
Educational and training packages based on the patient’s literacy level and knowledge can improve outcomes of chronic diseases.
Our study had several limitations. First, our study participants were a sample of patients already enrolled from one hospital in diabetes clinic and may not be representative of all diabetic patients. Second, our sample was small to assess the HbA1c. Finally, the Test of Functional Health Literacy in Adults evaluates the ability of reading comprehension and numeracy skill although health literacy consists of many parts such as speaking and listening skill etc. (24-26).
In this study, health literacy in Iranian patients with diabetes was low, and the results revealed that some other factors were also involved. Previous studies revealed that diabetes education was effective in improving self-management, diabetes knowledge, and glycemic control of patients with inadequate and limited health literacy. Therefore, it seems that effective methods such as using visual equipment are useful.
Conclusion
Health literacy score in Iranian patients with diabetes seems low. Therefore, effective interventions should be designed and implemented for this group of patients to improve diabetes outcomes.
Acknowledgements
We would like to present our special thanks to all participants of this study. This study was supported by the Institute of Endocrinology and Metabolism (IEM) in Iran University of Medical Sciences.
Cite this article as: Mohammadi Z, TehraniBanihashemi A, Asgharifard H, Bahramian M, Baradaran HR, Khamseh ME.Health literacy and its influencing factors in Iranian diabetic patients.Med JIslam RepubIran 2015 (11 July). Vol. 29:230.
References
- 1. Ratzan SC, Parker RM. Introduction. In: National Library of Medicine Current Bibliographies in Medicine: Health Literacy. Selden CR, Zorn M, Ratzan SC, Parker RM, Editors. NLM Pub. No. CBM 2000-1. Bethesda, MD: National Institutes of Health, U.S. Department of Health and human Services.
- 2.Sihota S, Lennard L. Health literacy: being able to make the most of health. London: National Consumer Council. 2004:11. [Google Scholar]
- 3.Zarcadoolas C, Pleasant A, Greer DS. Understanding health literacy: an expanded model. Health PromotInt. 2005;20:195–203. doi: 10.1093/heapro/dah609. [DOI] [PubMed] [Google Scholar]
- 4.Waldrop-Valverde D, Osborn CY, Rodriguez A, Rothman RL, Kumar M, Jones DL. Numeracy skills explain racial differences in HIV medication management. AIDS Behav. 2010;14:799–806. doi: 10.1007/s10461-009-9604-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Osborn CY, Cavanaugh K, Wallston KA, White RO, Rothman RL. Diabetes numeracy: an overlooked factor in understanding racial disparities in glycemic control. Diabetes Care. 2009;32:1614–1619. doi: 10.2337/dc09-0425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Donelle L, Arocha JF, Hoffman-Goetz L. Health literacy and numeracy: key factors in cancer risk comprehension. Chronic Dis Can. 2008;29:1–8. [PubMed] [Google Scholar]
- 7.Apter AJ, Cheng J, Small D, Bennett IM, Albert C, Fein DG. et al. Asthma numeracy skill and health literacy. J Asthma. 2006;43:705–710. doi: 10.1080/02770900600925585. [DOI] [PubMed] [Google Scholar]
- 8.Huizinga MM, Carlisle AJ, Cavanaugh KL, Davis DL, Gregory RP, Schlundt DG. et al. Literacy, numeracy, and portion-size estimation skills. Am J Prev Med. 2009;36:324–328. doi: 10.1016/j.amepre.2008.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Huizinga MM, Beech BM, Cavanaugh KL, Elasy TA, Rothman RL. Low numeracy skills are associated with higher BMI. Obes (Silver Spring) 2008;16:1966–1968. doi: 10.1038/oby.2008.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kutner M, Greenberg E, Baer J. A First Look at the Literacy of America’s Adults in the 21st Century. Washington, DC, National Center for Education Statistics, U.S. Department of Education, 2005.
- 11. WHO. Global status report on noncommunicable diseases 2014. Geneva, World Health Organization, 2012.
- 12.Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, etal etal. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005-2011. Diabetes Res Clin Pract . 2014 Feb;103(2):319–27. doi: 10.1016/j.diabres.2013.12.034. [DOI] [PubMed] [Google Scholar]
- 13.Gazmararian JA, Williams MV, Peel J, Baker DW. Health literacy and knowledge of chronic disease. Patient Educ Couns. 2003;51:267–275. doi: 10.1016/s0738-3991(02)00239-2. [DOI] [PubMed] [Google Scholar]
- 14.Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional health literacy to patients’ knowledge of their chronic disease: a study of patients with hypertension and diabetes. Arch Intern Med. 1998;158:166–172. doi: 10.1001/archinte.158.2.166. [DOI] [PubMed] [Google Scholar]
- 15.Cavanaugh K, Huizinga MM, Wallston KA, Gebretsadik T, Shintani A, Davis D. et al. Association of numeracy and diabetes control. Ann Intern Med. 2008;148:737–746. doi: 10.7326/0003-4819-148-10-200805200-00006. [DOI] [PubMed] [Google Scholar]
- 16.Schillinger D, Piette J, Grumbach K, Wang F, Wilson C, Daher C. et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003 Jul 28;163(14):1745–6. doi: 10.1001/archinte.163.1.83. [DOI] [PubMed] [Google Scholar]
- 17.ShahabJahanlou A, AlishanKarami N. The Effect of Literacy Level on Health Related-Quality of Life, Self-Efficacy and Self-Management Behaviors in Diabetic Patients. Acta Medica Iranica. 2011;49(3):153–158. [PubMed] [Google Scholar]
- 18.TehraniBanihashemi S, Amirkhani M, Haghdoost A, Alavian S, Asgharifard H, Baradaran H. et al. Health Literacy and the Influencing Factors: A Study in Five Provinces of Iran. Strides Dev Med Educ. 2007;4(1):1–9. [Google Scholar]
- 19.Nurss JR, Baker D, Davis T, Parker R, Williams M. Difficulty in functional health literacy screening in Spanish-speaking adults. Journal of Reading. 1995;38:632–637. [Google Scholar]
- 20.Trief PM, Wade MJ, Britton KD, Weinstock RS. A prospective analysis of marital relationship factors and quality of life in diabetes. Diabetes Care. 2002;25(7):1154–8. doi: 10.2337/diacare.25.7.1154. [DOI] [PubMed] [Google Scholar]
- 21.Pala T, Eser E, Ozmen B, Aydemir O, Boyvoda S. The eterminants of quality of life including treatment satisfaction in patients with type two diabetes mellitus: are different generic Qol instruments sensitive to the same determinants? Turkish J Endocrinol Metab. 2004;8(3):91–9. [Google Scholar]
- 22.National Work Group on Literacy and Health. Communicating with patients who have limited literacy skillsReport of the National Work Group on Literacy and Health. J of FamPract. 1998;46(2):168–76. [PubMed] [Google Scholar]
- 23.American College of Physicians; Fifth Edition. Section on Physician and the Patient (p561) Ann Intern Med. 2005;142:560–582. [Google Scholar]
- 24.Coonrod BA, Betschart J, Harris MI. Frequency and determinants of diabetes education among adults in the US population. Diabetes Care. 1994;17:852–858. doi: 10.2337/diacare.17.8.852. [DOI] [PubMed] [Google Scholar]
- 25.Glasgow RE, Toobert D, Hampson SE. Participation in outpatient diabetes education programs: how many patients takepart and how representative are they? Diabetes Educ. 1991;17:376–380. doi: 10.1177/014572179101700509. [DOI] [PubMed] [Google Scholar]
- 26. Nielsen-Bohlman L, Panzer AM, Kindig DA, Eds. Washington, D.C. Institute of Medicine: Health Literacy: A Prescription to End Confusion, The National Academics Press, 2004. [PubMed]