

Abstract
Background: Industrialization and urbanization had a devastating impact on public health and caused an increase in health related morbidity and mortality. In fact, asthma is a chronic condition which is considered as one of the significant challenges of public health. In this study, we investigated the association of air pollution and weather conditions with excess emergency ward admissions of asthmatic patients in Kermanshah hospitals.
Methods: This was an ecological study. The total number of hospital admissions to emergency wards from all related and major hospitals of Kermanshah was collected from September 2008 through August 2009. In addition, data on air pollution as well as meteorological data were collected from the Environmental Protection Agency and Meteorological Organization of Kermanshah. To determine the association between the number of hospitalization due to asthma with those parameters, Poisson regression was used.
Results: The results of Poisson regression revealed a significant association between carbon monoxide, ozone, nitrogen dioxide and temperature with emergency room visits due to asthma in Kermanshah. No associations were found for sulfur dioxide or for particulate matter.
Conclusion: This study provides further evidence for the significant effect of monoxide carbon on asthma; and it suggests that temperature may have a role in the exacerbation of asthma. However, due to the multi-factorial nature of asthma, other factors also play a major role in the development and exacerbation of this illness.
Keywords: Air Pollution, Asthma, Weather, Iran
Introduction
Asthma is a common respiratory disease whose prevalence has been increasing throughout the world in the recent years (1,2) .Factors associated with the incidence and exacerbation of asthma include genetic factors, respiratory tract infection, stress, poor nutrition, exposure to allergens such as pollen and mold spores, tobacco smoke, adverse weather conditions, air pollution and certain social factors (3-9). Among all factors, air pollution and adverse weather conditions play an important role in the development and exacerbation of asthma (10). Air pollutants contributing to asthma exacerbations include sulfur dioxide, carbon monoxide, nitrogen dioxide, ozone, smog and particulate (usually particles between 2.5 and 10 microns) (11).
In many epidemiological studies, the association between the number of hospital admissions of asthmatic patients with air pollution and climatic factors has been investigated. While the results of most of such studies indicated that air pollutants and air quality have a major role in exacerbation of asthma (12-15,16-18), other studies reported no significant association , (19-21) or even a negative association (22).
Studies have shown that in the developed countries of Europe and North America, due to the strict environmental regulations, air pollution as one of the important risk factors for asthma exacerbations, has been controlled in the recent years (23). However, due to the multi-factorial nature of asthma, it is still a major challenge in these countries (24,25).
In contrast, in developing countries, with rapid urbanization and lack of proper implementation of environmental legislation, air pollution is increasing rapidly (26-28). Iran, as a developing country, has been faced with air pollution in many of its large and industrial cities in the recent years. Studies also indicated that the prevalence of asthma in many cities of Iran is more than the world average and the trend in the prevalence of asthma is growing (29,30).Kermanshah, a city located in the west of Iran, is considered as one of the industrial cities of this country. According to WHO, Kermanshah has been considered as one of the ten most polluted cities in the world in 2011 (31). Since no studies have been done on the effect of air pollution on hospitalization of asthmatic patients in Kermanshah, the current study aimed to determine the association between air pollution levels and weather with excess emergency ward admissions of asthmatic patients in Kermanshah hospitals.
Methods
Study Area
Kermanshah is located in the West of Iran at 34° 18’ latitude North and 47° 4’ longitude East. It is located 1420 meters above the sea level; and its average, maximum and minimum annual temperature are 14.2, 38 and 3.2 ºC, respectively. The area of this city is 8547 square kilometers and its population, according to Census 2010, is already more than 980,786.
Data
This was an ecological study. Overall, there are 10 public and private hospitals in the urban area of Kermanshah. Of them, seven were included in the study, and the others (the Obstetrics and Gynecology and Psychiatric Hospitals) that were not related to the aim of this study were excluded. The total number of hospital admissions to emergency wards with the diagnosis of asthma from seven major hospitals (Imam Reza, Imam Hussain, Imam Khomeini, Bisotoun, Shohada, Artesh and Hazrat Masomeh) was collected from September 2008 through August 2009.
The daily number of asthmatic patients was gathered from all included hospitals (emergency wards), retrospectively. The patients diagnosed as suffering from "asthma" had been extracted by a trained health-care provider. The diagnosis made by the attending physician was classified according to the International Classification of Diseases, and code J44-46 (asthma, acute severe asthma and chronic obstructive asthma). From all admissions, only those who were residents of Kermanshah district were included.
For the study period, data on concentration levels of air pollutants was collected from the Environmental Protection Agency of Kermanshah. The daily concentrations of each pollutant were averaged from the available monitoring results of three fixed stations located in the urban district of Kermanshah. Pollutants measured by these stations were sulfur dioxide (SO2), nitrogen oxides, carbon monoxide (CO), particulate matter with less than 10 µm of aerodynamic diameter (PM10), and ozone (O3). For the purpose of this study, the mean hourly values of the above mentioned pollutants from 1:00 am to 12:00 pm were considered.
Based on the previous reports (19-21), major meteorological data (temperature, air pressure, relative humidity and rainfall) were obtained from Kermanshah Meteorological Organization. These data were all of the climatic factors measured by this Organization.
Statistical Analysis
Data processing and analysis were performed with SPSS 21 software. In order to measure the association between the daily number of emergency ward admissions with diagnosis of asthma with different air pollutants and climate parameters, we first investigated the possible collinearity between climate parameters and air pollutants by looking at the correlation between such factors using Pearson's bivariate correlation. Then, among the factors that had a high correlation with each other (correlation coefficient > 0.7), only one of them were included in the final model. According to Pearson's bivariate correlation NO and NOX had high collinearity with NO2 and CO, so they were removed in the multivariate model. Among NOX, NO and NO2, just NO2 was used inthe multivariate Poisson regression because of its higher importance in human health.
To determine the association between the number of hospital admissions with the diagnosis of asthma with air pollution and climate parameters, Poisson regression was used. In order to check the independent effect of each factor on the number of hospital admissions with the diagnosis of asthma, we used multivariable models.
Results
For the period of the study, 441 patients with the mean±SD age of 44.02±19.1 years who were diagnosed with asthma referred to Kermanshah hospitals. Among the total patients, women (56.1%; N = 248) and those who were in the adult age group (46.7%; N = 206) constituted the largest groups (Table 1). According to Fig. 1, the highest number of admissions of the asthmatic patients was in the winter and the month of December, and the lowest was in the summer and the month of August (p<0.05).
Table 1 . Number of Patients Admitted to Hospitals in Different Age Groups during 2008-2009 .
| Age | Frequency | Percent |
| 0-13 (Children) | 58 | 13.15 |
| 15-30 (Adolescents) | 87 | 19.7 |
| 30-65(Adults) | 206 | 46.7 |
| 65 < (Elderly) | 90 | 20.4 |
| Sex | ||
| Male | 193 | 43.8 |
| Female | 248 | 56.15 |
Fig. 1 .
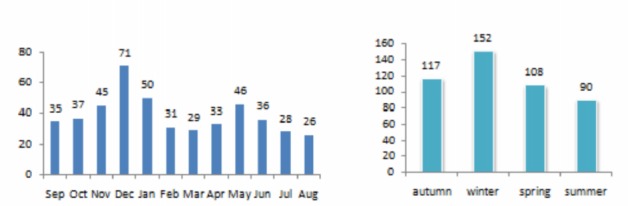
Number of Asthmatic Patients Attending to Hospitals in Different Months during 2008-2009
In December, the mean±SD values of climatic parameters, including ambient temperature, precipitation, humidity and pressure were obtained to be 2.0±4.5C0, 1.0±3.95mm, 872.1±3.29 and 62.9±16.5, respectively; and the values of air pollutants such as ozone, nitrogen monoxide, nitrogen dioxide, NOX, particulates, sulfur dioxide and carbon monoxide were calculated to be 3.48 ppb, 34.23 ppb, 15.97 ppb, 50.18 ppb, 77.21 ppb, 22.04 ppb, 2.09 ppm, respectively (Tables 2 and 3).
Table 2 . Descriptive Statistics of Air Pollutants in Different Months during 2008-2009 .
| Month | O3(ppb) | NO (ppb) | NO2(ppb) | NOx(ppb) | PM10(ug/m3) | SO2 (ppb) | CO (ppm) |
| Sep | 17.3±5.38* | 19.5±12.03 | 8.7±3.15 | 28.2±14.93 | 142.5±64.53 | 27.5±5.29 | 1.6±0.78 |
| Oct | 3.9±3.80 | 29.2±10.99 | 10.6±2.31 | 39.7±12.90 | 87.6±33.70 | 25.2±3.63 | 2.6±0.68 |
| Nov | 2.6±0.17 | 43.9±23.93 | 13.8±3.28 | 57.7±26.45 | 67.6±15.49 | 24.5±1.62 | 2.5±0.86 |
| Dec | 3.5±1.66 | 34.2±19.40 | 16.0±3.71 | 50.2±21.29 | 77.2±29.68 | 22.0±2.31 | 2.1±0.76 |
| Jan | 5.0±1.37 | 20.0±11.51 | 12.9±2.71 | 32.9±13.66 | 106.7±95.47 | 26.0±3.02 | 1.7±0.74 |
| Feb | 6.3±2.06 | 19.0±12.18 | 12.4±2.11 | 31.3±13.79 | 149.74±128.9 | 19.7±5.2 | 1.6±0.75 |
| Mar | 8.2±2.38 | 14.0±7.11 | 10.7±2.74 | 24.4±9.04 | 138.8±80.90 | 18.0±4.75 | 1.4±0.56 |
| Apr | 6.9±1.81 | 15.9±6.65 | 9.3±1.63 | 25.2±7.8 | 164.3±78.4 | 24.7±5.95 | 1.6±0.54 |
| May | 33.0±12.4 | 12.8±6.5 | 7.7±2.3 | 20.5±8.6 | 193.1±120.2 | 43.2±15.6 | 1.2±0.52 |
| Jun | 40.2±4.99 | 11.6±4.86 | 7.4±1.99 | 19.1±6.57 | 457.7±345.4 | 51.4±16.21 | 1.0±0.32 |
| Jul | 40.7±6.92 | 12.3±5.28 | 7.6±2.33 | 20.0±7.47 | 205.4±76.08 | 61.1±21.46 | 1.1±0.43 |
| Aug | 34.7±9.07 | 11.57±5.57 | 6.7±1.97 | 18.2±7.35 | 137.6±47.7 | 60.2±23.21 | 1.1±0.39 |
Mean±SD
Table 3 . Descriptive Statistics of Climatic Factors in Different Months during 2008-2009 .
| Month | Temperature | Rainfall | Pressure | Ave. Hum. |
| Sep | 19.8±2.09* | 0.0±0.00 | 870.9±2.53 | 28.5±8.07 |
| Oct | 10.8±3.4 | 3.3±7.4 | 872.5±1.88 | 64.8±15.11 |
| Nov | 5.0±3.6 | 1.89±6.76 | 872.3±2.30 | 61.2±13.27 |
| Dec | 2.0±4.5 | 1.0±3.95 | 872.1±3.29 | 62.9±16.5 |
| Jan | 5.4±3.09 | 2.2±5.96 | 869.9±2.63 | 68.0±10.87 |
| Feb | 7.9±3.51 | 0.5±1.08 | 868.6±3.17 | 58.0±11.2 |
| Mar | 10.09±1.79 | 1.9±3.6 | 866.5±2.9 | 60.4±11.24 |
| Apr | 16.9±2.67 | 0.2±0.89 | 869.1±1.56 | 53.3±11.8 |
| May | 23.9±2.1 | 0.1±0.03 | 867.2±1.6 | 27.9±6.1 |
| Jun | 28.19±1.14 | 0.0±0.02 | 862.9±2.26 | 20.6±4.8 |
| Jul | 28.1±2.7 | 0.0±0.05 | 863.5±3.3 | 19.1±5.1 |
| Aug | 24.1±2.5 | 0.4±2.08 | 866.8±2.15 | 27.1±13.5 |
Mean±SD
As mentioned above, the lowest rate of admission of asthmatic patients was in August; and in this month, the mean values of climate variables, ambient temperature, precipitation, barometric pressure and humidity were obtained to be 24.1±2.5 Cº, 0.4±2.08 mm, 866.8±2.15, 27.1±13.5, respectively. Also, the amount of air pollutants such as ozone, nitrogen monoxide, nitrogen dioxide, NOX, particulates, sulfur dioxide and carbon monoxide was 34.67ppb, 11.47ppb, 6.67ppb, 18.2ppb, 137.62g/m3μ, 60.17ppb, 1.14ppm, respectively(Table 2, 3).
Table 4 demonstrates the minimum, maximum, mean, standard deviation, and also the most critical days of pollutants and climatic factors that have been presented in 2008–2009. Accordingly, the maximum values of pollutants including NOX, NO, NO2 and CO occurred during the winter, and the highest levels of SO2 and PM10 and O3 concentration occurred in the summer.
Table 4 . Descriptive Statistics of Daily Values of Air Pollutants and Climatic Factor .
| Measured Daily Variable | Minimum | Maximum | Mean | Std. Deviation | The Day with Extreme Value |
| O3, ppb | .00 | 52.38 | 17.2 | 16.0 | 2009/August/12 |
| NO, ppb | 1.13 | 92.67 | 19.9 | 14.96 | 2009/January/4 |
| NO2, ppb | 2.00 | 23.54 | 10.2 | 3.7 | 2009/January/17 |
| NOx, ppb | 4.29 | 111.88 | 30.2 | 17.85 | 2009/January/4 |
| PM10, ug/m3 | .00 | 2758.60 | 162.6 | 223.14 | 2009/July/5 |
| SO2, ppb | 7.42 | 101.63 | 33.9 | 19.26 | 2009/July/23 |
| CO, ppm | 0.31 | 4.24 | 1.6 | 0.798 | 2008/December/6 |
| Tem,°C | -5.20 | 30.50 | 15.3 | 9.54 | 2009/August/17 |
| Rain, mm | .00 | 26.90 | 0.9 | 3.56 | 2008/October/26 |
| Pressure | 858.70 | 881.70 | 868.5 | 3.91 | 2009/January/14 |
| MinHum, % | 3.00 | 93.00 | 23.9 | 17.70 | 2009/January/21 |
| MaxHum, % | 21.00 | 100.00 | 67.1 | 27.57 | 2008/November/1 |
| AveHum, % | 12.50 | 97.00 | 45.6 | 21.52 | 2009/January/21 |
The results of univariate Poisson regression showed that carbon monoxide, nitrogen oxides (NO, NO2, NOX), humidity and temperature were significantly associated with the number of hospital admissions of asthmatic patients (p<0.05).
According to the multiple regression analysis, among the air pollutants and climatic parameters, temperature, ozone and carbon monoxide were significantly associated with the admission of asthmatic patients in Kermanshah hospitals (Table 5).
Table 5 . Univariate and Multiple Poisson Regression Models to Determine the Association between Air Pollutants and Weather Conditions, with the Number of Asthmatic Patients Admitted to Hospitals in Kermanshah .
| Parameter | Univariate Model β* ( 0.95 CI) | Multiple Model Β*( 0.95 CI) | |
| Air Pollutants | CO | 0.220 ( 0.122 – 0.325) | 0.165(0.009 – 0.322) |
| O3 | -0.001 (-0.01 – 0.0009) | 0.016(0.003 – 0.0276) | |
| NO** | 0.0119 (0.007- 0.017) | - | |
| NO2 | 0.054 (0.03 – 0.079) | 0.014(-0.024 – 0..054) | |
| NOx** | 0.011 (0.006 – 0.015) | - | |
| PM10 | 0.001 (-0.001 – 0.0003) | 0.0004 (-0.001 - 0.001) | |
| SO2 | -0.004 (-.009 - 0.001) | 0.0046 ( -0.007 – 0.016) | |
| Weather Conditions | Temperature | -0.021 (-0.031- -0.012) | -0.027(-.048 - -0.006) |
| Rain | 0.005 (-0.02 - 0.03) | 0.007(-0.02 - 0.032) | |
| Pressure | 0.049 (-0.024 - 0.073) | 0.023 (-0.01 - 0.055) | |
| Humidity | 0.006 (0.002 - 0.011) | 0.008 ( -0.003 – 0.02) | |
| Season | Spring | - | - |
| Summer | --0.191 (-0.544-0.148) | -0.35(-0.880-0.169) | |
| Autumn | 0.104(-0.23-0.469) | Omitted by software | |
| Winter | 0.518(0.169-0.879) | 0.549(0.086-0.90) |
In both univariate and multiple Poisson regression, no significant associations were found for sulfur dioxide or PM10 (p<0.05). The results of Poisson regression models showed the highest significant association between carbon monoxide and emergency room visits due to asthma with coefficient regression of 0.220 ( 0.122 – 0.325) and 0.165(0.009 – 0.322).
In addition, using the multivariate model, we found a positive association between the number of emergency ward admissions for asthmatic symptoms and cold season (winter).
Discussion
Based on the results of multivariate Poisson regression, among air pollutants, CO and O3 were significantly associated with the number of hospitalization of asthmatic patients in Kermanshah. In the studies performed in Washington, Taiwan, Korea and Australia both CO and O3 were associated with the increase in the number of patients with diagnosis of asthma (32-35).
However, such findings are not consistent with other reports (36-38).
According to the univariate model, carbon monoxide and nitrogen oxides, which include all of NO, NO2 and NOX, were associated with hospital admissions with diagnosis of asthma; and among these variables, the greatest influence was related to NO2. In fact, the toxic effect of NO2 on human health is about 4 times greater than NO (39). Our finding is in line with that of other similar reports (14,15,40-42).
In this study, in both single and multivariable models, no significant association was obtained between PM10 and the number of asthmatic patients admitted to hospitals in Kermanshah. In a study conducted by Lavin et al. in Canada, no significant association was found between the particles and the number of asthmatic patients admitted to hospital in all age groups, while carbon monoxide, NO2 and SO2 had the greatest impact on the rate of asthmatic patients’ admission to emergency departments (40).
Moreover, in other studies, there were no significant associations between particles and the rate of hospitalization of asthmatic and respiratory patients, but gaseous pollutants played an important role in the exacerbation of asthma (43-46).
However, in many studies, in addition to the gaseous pollutants, particulate matters were associated with a number of asthma admissions to the hospitals. For example, in 2011 a study was conducted in Italy showing that CO, SO2, NO2 and PM10, were associated with asthma hospitalization (14). Such findings were repeated in other studies showing an association between CO, NO2 and PM10 with the number of hospitalization of patients with asthma and respiratory diseases (15,41). In a study conducted in Barcelona, PM10 and NO2 were significantly associated with the number of asthma patients visiting EDs, while SO2 and O3 showed no significant association (42). In 2006, in Taiwan a significant positive association was found between NO2, CO and PM10 with the number of hospital admission of asthmatic children (12). In another study conducted in Athens in 2011, PM10, SO2 and ozone had a significant positive association with the number of emergency admissions of asthmatic patients (47).
In fact, in the recent years, just like other cities in western Iran, Kermanshah has been faced with a hazy weather resulting from successive droughts in the neighboring countries; and therefore, people are more aware of the effect of the particulate matter (PM10) on their health. For that reason, on such days, people go out less than other days; and this may contribute to the lack of effect of the particulate matter on the number of hospital admissions due to asthma in this study.
In this study, no significant positive association was found between SO2 levels and hospitalization of asthmatic patients. Other reports revealed different results; while some of such reports showed no association (12,42,45), others found a positive association (14,40,43,47).
Using univariate Poisson regression model, among climatic factors, temperature and humidity and winter were significantly associated with the number of hospital admissions of asthmatic patients in Kermanshah (p<0.05); and the most hospital admissions were in the winter with maximum humidity and minimum temperature. In a study conducted in China in 2006, the highest number of hospital admissions due to asthma was in the winter and the lowest was in the summer and early autumn (12).
In a study by T.Abe in 2008 (11) and Samoli, in 2011 (47), low temperature and cold weather were significantly associated with asthma exacerbations. In contrast, a study was conducted in 2011 by Tramuto et al. in which the severity of asthma in the summer was significantly more than the other seasons (14). In another study conducted in Australia by Jalaludin, it was found that the impact of air pollutants on asthma exacerbations was more in the warmer months than in the other months (35). In the present study, a significant association was found between the rate of hospital admission of asthmatic patients and levels of pollutants such as NO2, CO and O3. It should be noted that asthma is only one of the adverse effects of air pollution on public health.
Conclusion
This was an ecological study and did not take into consideration the behavioral characteristics of individuals, such as nutrition, physical activity, smoking and socioeconomic status which have significantly contributed to occurrence and exacerbation of asthma.
In fact, the government should reduce air pollution in the city of Kermanshah by taking more precise and serious actions in the form of short-term and long-term plans. Also, more serious environmental regulations should be implemented. As a short-term plan, it is recommended that urban air quality be monitored, and in the days that air pollution is higher than the permissible values, weather condition should be announced to all people specifically those with higher risk for respiratory diseases.
Acknowledgments
The present study was adopted from the final report of a research project approved by the Department of Research and Technology of Kermanshah University of Medical Sciences. The authors would like to thank Kermanshah Meteorological Organization, Kermanshah Department of Environment and hospital officials of Kermanshah for the material support.
Cite this article as: Khamutian R, Najafi F, Soltanian M, Shokoohizadeh MJ, Poorhaghighat S, Dargahi A, Sharafi K, Afshari A. The association between air pollution and weather conditions with increase in the number of admissions of asthmatic patients in emergency wards: a case study in Kermanshah. Med J Islam Repub Iran 2015 (7 July). Vol. 29:229.
References
- 1.Taylor BW. The identification of high risk asthmatic children using the emergency department asthma visit count. The Journal of emergency medicine. 1999;17(6):953–956. doi: 10.1016/s0736-4679(99)00122-5. [DOI] [PubMed] [Google Scholar]
- 2.Jalaludin B, Chey T, Holmwood M, Chipps J, Hanson R, Corbett S. et al. Admission rates as an indicator of the prevalence of severe asthma in the community. Australian and New Zealand journal of public health. 1998;22(2):214–219. doi: 10.1111/j.1467-842x.1998.tb01175.x. [DOI] [PubMed] [Google Scholar]
- 3.Sigurs N, BjarnAson R, Sigurbergsson F, Kjellman B. Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. American journal of respiratory and critical care medicine. 2000;161(5):1501–1507. doi: 10.1164/ajrccm.161.5.9906076. [DOI] [PubMed] [Google Scholar]
- 4.Cassol VE, Rizzato TM, Teche SP, Basso DF, Centenaro DF, Maldonado M. et al. Obesity and its relationship with asthma prevalence and severity in adolescents from southern Brazil. Journal of Asthma. 2006;43(1):57–60. doi: 10.1080/02770900500448597. [DOI] [PubMed] [Google Scholar]
- 5.Wickens K, Barry D, Friezema A, Rhodius R, Bone N, Purdie G. et al. Fast foods–are they a risk factor for asthma? Allergy. 2005;60(12):1537–1541. doi: 10.1111/j.1398-9995.2005.00945.x. [DOI] [PubMed] [Google Scholar]
- 6.Wong GW, Lai CK. Outdoor air pollution and asthma. Current opinion in pulmonary medicine. 2004;10(1):62–66. doi: 10.1097/00063198-200401000-00011. [DOI] [PubMed] [Google Scholar]
- 7.Lucas SR, Platts-Mills TA. Physical activity and exercise in asthma: relevance to etiology and treatment. Journal of Allergy and Clinical Immunology. 2005;115(5):928–934. doi: 10.1016/j.jaci.2005.01.033. [DOI] [PubMed] [Google Scholar]
- 8.Rosas I, McCartney HA, Payne RW, Calderon C, Lacey J, Chapela R. et al. Analysis of the relationships between environmental factors (aeroallergens, air pollution, and weather) and asthma emergency admissions to a hospital in Mexico City. Allergy. 1998;53(4):394–401. doi: 10.1111/j.1398-9995.1998.tb03911.x. [DOI] [PubMed] [Google Scholar]
- 9.Wilhelm M, Qian L, Ritz B. Outdoor air pollution, family and neighborhood environment, and asthma in LA FANS children. Health & place. 2009;15(1):25–36. doi: 10.1016/j.healthplace.2008.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Duhme H, Weiland SK, Keil U. Epidemiological analyses of the relationship between environmental pollution and asthma. Toxicology Letters. 1998;102:307–316. doi: 10.1016/s0378-4274(98)00322-1. [DOI] [PubMed] [Google Scholar]
- 11.Abe T, Tokuda Y, Ohde S, Ishimatsu S, Nakamura T, Birrer RB. The relationship of short-term air pollution and weather to ED visits for asthma in Japan. The American journal of emergency medicine. 2009;27(2):153–159. doi: 10.1016/j.ajem.2008.01.013. [DOI] [PubMed] [Google Scholar]
- 12.Sun HL, Chou MC, Lue KH. The relationship of air pollution to ED visits for asthma differ between children and adults. The American Journal of Emergency Medicine. 2006;24(6):709–713. doi: 10.1016/j.ajem.2006.03.006. [DOI] [PubMed] [Google Scholar]
- 13.Tsai SS, Cheng MH, Chiu HF, Wu TN, Yang CY. Air pollution and hospital admissions for asthma in a tropical city: Kaohsiung, Taiwan. Inhalation toxicology. 2006;18(8):549–554. doi: 10.1080/08958370600686176. [DOI] [PubMed] [Google Scholar]
- 14.Tramuto F, Cusimano R, Cerame G, Vultaggio M, Calamusa G, Maida CM. et al. Urban air pollution and emergency room admissions for respiratory symptoms: a case-crossover study in Palermo, Italy. Environmental Health. 2011;10(1):31. doi: 10.1186/1476-069X-10-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Delamater PL, Finley AO, Banerjee S. An analysis of asthma hospitalizations, air pollution, and weather conditions in Los Angeles County, California. Science of The Total Environment. 2012;425(0):110–118. doi: 10.1016/j.scitotenv.2012.02.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fusco D, Forastiere F, Michelozzi P, Spadea T, Ostro B, Arca M. et al. Air pollution and hospital admissions for respiratory conditions in Rome, Italy. European respiratory journal. 2001;17(6):1143–1150. doi: 10.1183/09031936.01.00005501. [DOI] [PubMed] [Google Scholar]
- 17.Hashimoto M, Fukuda T, Shimizu T, Watanabe S, Watanuki S, Eto Y. et al. Influence of climate factors on emergency visits for childhood asthma attack. Pediatrics international. 2004;46(1):48–52. doi: 10.1111/j.1442-200X.2004.01835.x. [DOI] [PubMed] [Google Scholar]
- 18.Strauss RH, McFadden JrER, Ingram JrRH, Jaeger JJ, Stearns DR. Enhancement of exercise-induced asthma by cold air. The New England journal of medicine. 1977;297(14):743. doi: 10.1056/NEJM197710062971402. [DOI] [PubMed] [Google Scholar]
- 19.Sahsuvaroglu T, Jerrett M, Sears MR, McConnell R, Finkelstein N, Arain A. et al. Spatial analysis of air pollution and childhood asthma in Hamilton, Canada: comparing exposure methods in sensitive subgroups. Environmental Health. 2009;8(1):14. doi: 10.1186/1476-069X-8-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kim SH, Son JY, Lee JT, Kim TB, Park HW, Lee JH. et al. Effect of air pollution on acute exacerbation of adult asthma in Seoul, Korea: A case-crossover study. Korean Journal of Medicine. 2010;78(4):450–456. [Google Scholar]
- 21.de Diego Damia A, CompteTorrero L. Effects of air pollution and weather conditions on asthma exacerbation. Respiration. 1999;66(1):52–58. doi: 10.1159/000029337. [DOI] [PubMed] [Google Scholar]
- 22.Garty BZ, Kosman E, Ganor E, Berger V, Garty L, Wietzen T. et al. Emergency Room Visits of Asthmatic Children, Relation to Air Pollution, Weather, and Airborne Allergens. Annals of Allergy, Asthma & Immunology. 1998;81(6):563–570. doi: 10.1016/S1081-1206(10)62707-X. [DOI] [PubMed] [Google Scholar]
- 23.Mayer H. Air pollution in cities. Atmospheric Environment. 1999;33(24):4029–4037. [Google Scholar]
- 24. uropean Community Respiratory Health Survey . Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community Respiratory Health Survey (ECRHS) 1996 doi: 10.1183/09031936.96.09040687. [DOI] [PubMed] [Google Scholar]
- 25.Chinn S, Burney P, Jarvis D, Luczynska C. Variation in bronchial responsiveness in the European community respiratory health survey (ECRHS) European Respiratory Journal. 1997;10(11):2495–2501. doi: 10.1183/09031936.97.10112495. [DOI] [PubMed] [Google Scholar]
- 26.Vasconcellos EA. Transport and environment in developing countries: Comparing air pollution and traffic accidents as policy priorities. Habitat International. 1997;21(1):79–89. [Google Scholar]
- 27. Khosh-Chashm K. The impact of urbanization on health in the countries of the Eastern Mediterranean region. City, 1998. 1960: p. 90.
- 28.Mage D, Ozolins G, Peterson P, Webster A, Orthofer R, Vandeweerd V. et al. Urban air pollution in megacities of the world. Atmospheric Environment. 1996;30(5):681–686. [Google Scholar]
- 29.Heidarnia MA, Entezari A, Moein M, Mehrabi Y, Pourpak Z. Prevalence of asthma symptom in Iran: a meta-analysis. Pejouhesh. 2007;31(3):217–225. [Google Scholar]
- 30.Mohammadzadeh I, Ghafari J, Savadkoohi RB, Tamaddoni A, Dooki MRE, Navaei RA. The Prevalence of Asthma, Allergic Rhinitis and Eczema in North of Iran. Iranian Journal of Pediatrics. 2008;18(2) [Google Scholar]
- 31. The Cities with the Worst Air Pollution in the World (2011) http://247wallst.com/2011/09/28/the-cities-with-the-worst-air-pollution-in-the-world/2/ Accessed 08 March 2013.
- 32.Sheppard L, Levy D, Norris G, Larson TV, Koenig JQ. Effects of Ambient Air Pollution on Nonelderly Asthma Hospital Admissions in Seattle, Washington, 1987-1994. Epidemiology. 1999;10(1):23–30. [PubMed] [Google Scholar]
- 33. Lien CH, Lin RS. Air pollution, weather, and associated risk factors related to asthma prevalence and attack rate. 2007. [DOI] [PubMed]
- 34.Xirasagar S, Lin HC, Liu TC. Seasonality in pediatric asthma admissions: the role of climate and environmental factors. European journal of pediatrics. 2006;165(11):747–752. doi: 10.1007/s00431-006-0164-6. [DOI] [PubMed] [Google Scholar]
- 35.Jalaludin B, Khalaj B, Sheppeard V, Morgan G. Air pollution and ED visits for asthma in Australian children: a case-crossover analysis. International archives of occupational and environmental health. 2008;81(8):967–974. doi: 10.1007/s00420-007-0290-0. [DOI] [PubMed] [Google Scholar]
- 36.Lipsett M, Hurley S, Ostro B. Air pollution and emergency room visits for asthma in Santa Clara County, California. Environmental Health Perspectives. 1997;105(2):216. doi: 10.1289/ehp.97105216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Schwartz J, Slater D, Larson TV, Pierson WE, Koenig JQ. Particulate air pollution and hospital emergency room visits for asthma in Seattle. American Journal of Respiratory and Critical Care Medicine. 1993;147(4):826–831. doi: 10.1164/ajrccm/147.4.826. [DOI] [PubMed] [Google Scholar]
- 38.Harre ES, Price PD, Ayrey RB, Toop LJ, Martin IR, Town GI. Respiratory effects of air pollution in chronic obstructive pulmonary disease: a three month prospective study. Thorax. 1997;52(12):1040–1044. doi: 10.1136/thx.52.12.1040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Amirbeygi H, Ahmadi A. Air pollution & pollutant control methods. Tehran: Andisheh Rafi. 2008.
- 40.Lavigne E, Villeneuve PJ, Cakmak S. Air pollution and emergency department visits for asthma in Windsor, Canada. Canadian Journal of Public Health. 2011;103(1):4–8. doi: 10.1007/BF03404060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Linn WS, Szlachcic Y, Gong JrH, Kinney PL, Berhane KT. Air pollution and daily hospital admissions in Metropolitan Los Angeles. Environmental Health Perspectives. 2000;108(5):427–434. doi: 10.1289/ehp.00108427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Castellsague J, Sunyer J, Saez M, Anto JM. Short-term association between air pollution and emergency room visits for asthma in Barcelona. Thorax. 1995;50(10):1051–1056. doi: 10.1136/thx.50.10.1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Makra L, Matyasovszky I, Bálint B. Association of allergic asthma emergency room visits with the main biological and chemical air pollutants. Science of The Total Environment. 2012;432(0):288–296. doi: 10.1016/j.scitotenv.2012.05.088. [DOI] [PubMed] [Google Scholar]
- 44.Katsouyanni K, Schwartz J, Spix C, Touloumi G, Zmirou D, Zanobetti A. et al. Short term effects of air pollution on health: A European approach using epidemiologic time series data: The APHEA protocol. Journal of Epidemiology and Community Health. 1996;50(SUPPL 1):S12–S18. doi: 10.1136/jech.50.suppl_1.s12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Fusco D, Forastiere F, Michelozzi P, Spadea T, Ostro B, Arca M. et al. Air pollution and hospital admissions for respiratory conditions in Rome, Italy. European Respiratory Journal. 2001;17(6):1143–1150. doi: 10.1183/09031936.01.00005501. [DOI] [PubMed] [Google Scholar]
- 46.Alves CA, Scotto MG, Freitas MDC. Air pollution and emergency admissions for cardiorespiratory diseases in lisbon (Portugal) Quimica Nova. 2010;33(2):337–344. [Google Scholar]
- 47.Samoli E, Nastos PT, Paliatsos AG, Katsouyanni K, Priftis KN. Acute effects of air pollution on pediatric asthma exacerbation: Evidence of association and effect modification. Environmental Research. 2011;111(3):418–424. doi: 10.1016/j.envres.2011.01.014. [DOI] [PubMed] [Google Scholar]