

Abstract
Background
Heartland virus (HRTV) is a tick-borne phlebovirus recently described in Missouri that is associated with fever, leukopenia and thrombocytopenia. The virus has also been detected in Ambylommaamericanum ticks.
Methods and Results
Here we report the first fatal case of HRTV disease in an 80 year-old Tennessee resident. He was hospitalized with fever, confusion, leukopenia, and thrombocytopenia and developed multi-organ failure and hemorrhage. A tick-borne illness was suspected and testing for ehrlichiosis was negative. He died on hospital day 15 and autopsy specimens were tested for various pathogens as part of an unexplained death evaluation. HRTV antigens were detected in post-mortem spleen and lymph nodes by immunohistochemistry, and HRTV was detected in pre-mortem blood by RT-PCR and by isolation in cell culture.
Conclusions
This case demonstrates that HRTV infection can cause severe disease and death and expands the geographic range of HRTV within the United States.
INTRODUCTION
Heartland virus (HRTV) is a recently described tick-borne phlebovirus [1]. Phleboviruses are single-stranded RNA viruses in the family Bunyaviridae. The original two cases of HRTV disease were initially reported in adult males from Missouri. Both case-patients presented with a non-specific febrile illness with leukopenia and thrombocytopenia and history of tick exposure. They were initially diagnosed with ehrlichiosis for which they received doxycycline. The case-patients required hospitalization for approximately 11 days before being discharged to home where they eventually recovered. Subsequent field work identified the virus in Ambylommaamericanum ticks collected on one of the original patient’s farms and at a nearby site [2]. An additional five non-fatal cases have been recently identified through active surveillance in Missouri [3].
HRTV is relatively closely related to but distinct from the severe fever and thrombocytopenia syndrome virus (SFTSV), a virus found in China [4]and neighboring countries [5, 6]. SFTSV infection also presents with fever, thrombocytopenia, and leukopenia, but may have severe manifestations including neurological disease and hemorrhage. Between 6–17% of SFTSV cases are fatal [4, 7, 8]. Most SFTSV deaths in China have occurred in patients >70 years old [9].
CASE REPORT
An 80-year-old man with a history of chronic obstructive pulmonary disease and heavy alcohol use presented in July 2013 to a local emergency department for weakness, frequent falls over the past week, altered mental status, and fevers. He also reported decreased appetite and an episode of passing dark stool. He lived on a farm in central Tennessee and was active outdoors. He had a history of multiple tick bites, and his wife found a tick on him two weeks prior to his illness onset.
On presentation, his temperature was 37.8 °C. Laboratory tests revealed hyponatremia of 129 mmol/L, elevated aspartate aminotransferase (AST) of 184 U/L, elevated alanine aminotransferase (ALT) of 124 U/L, leukopenia of 1.1×103 cells/μL, and thrombocytopenia of 59.0 × 103/μL. His hemoglobin (16.8 g/dL) and prothrombin time (13.7 seconds) were within normal limits. Computed tomography of the head and a chest radiograph showed no significant acute abnormalities. He was admitted to the hospital with suspected ehrlichiosis and doxycycline therapy was initiated.
On hospital day 2, the patient was transferred to a quaternary care center for persistent delirium and worsening tachypnea. Within hours, he was admitted to the medical intensive care unit for worsening hypoxia and hypotension and antibiotic coverage was broadened due to concern for sepsis. He was noted to be febrile with a temperature of 39.8°C and purpura were noted on exam. A lumbar puncture was unable to be performed due to persistent thrombocytopenia. His clinical laboratory findings during hospitalization included worsening thrombocytopenia (nadir of 24 × 103/μL on hospital day 8) for which he was given three units of apheresis platelets (figure 1), persistent leukopenia, decreasing hemoglobin (nadir of 8.7 g/dL on hospital day 14), increased creatine kinase (844 U/L on hospital day 2), increased AST and ALT (peaking on hospital day 4 to 626 and 166 U/L, respectively), elevated lactate dehydrogenase (LDH) (peaking on hospital day 5 at 1801 U/L) and elevated creatinine (peaking on day 12 to 4.1 mg/dL). Prothrombin time and fibrinogen levels remained within normal limits. The immature platelet fraction was elevated at 25.2% (normal range, 0.9–7.0%), indicating that thrombocytopenia was due to platelet consumption rather than decreased bone marrow production. The white blood cell count normalized on hospital day 10, and the platelet count began to rise reaching a peak of 116 × 103 when last measured on hospital day 15. Urinalysis showed proteinuria and microscopic hematuria. Blood cultures showed no bacterial growth. Serology was negative for spotted fever group Rickesttsia species and both serology and molecular testing for E. chaffeensis were negative.
Figure 1.

Liver function test and complete blood count data. Apheresis platelet transfusions are indicated by arrow heads. AST: aspartate aminotransferase; ALT: alanine aminotransferase; PLT: platelet count; WBC: white blood cell count; HGB: hemoglobin.
His hospital course was complicated by respiratory failure requiring mechanical ventilation and vasopressors, troponin leak without associated electrocardiogram changes, acute kidney injury, and upper gastrointestinal bleeding requiring cauterization of gastric ulcers. The patient was successfully extubated but remained delirious and unable to communicate. His family opted to transition to comfort measures, and he died on hospital day 15.
An autopsy revealed acute gastritis, gastric and duodenal mucosal ulcers, and focal transmural hemorrhage in the ascending colon. The spleen was soft and there was no lymphadenopathy. The bone marrow exhibited trilineage hematopoiesis with myeloid hyperplasia, and rare hemophagocytosis was seen in a mediastinal lymph node. Acute pyelonephritis and adrenal cortical atrophy were present. The liver showed macrovesicular steatosis and portal triaditis. The lungs were emphysematous and there was patchy cardiac fibrosis, coronary artery and aortic atherosclerosis, and a remote cerebral infarct and systemic amyloidosis. No vasculitis was identified. Blood and lung cultures obtained at the time of autopsy were negative. The Infectious Diseases Pathology Branch at Centers for Disease Control and Prevention (CDC) was consulted for further evaluation of this unexplained death.
METHODS
Immunohistochemistry
Tissues were fixed in 10% neutral-buffered formalin and processed for routine histological analysis. Immunohistochemistry (IHC) assays were performed using a polymer-based indirect immunoalkaline phosphatase detection system with colorimetric detection of antibody-polymer complex with Fast Red Chromogen (Biocare Medical, Concord, CA). IHC assays were performed for Ehrlichia, Anaplasma, spotted fever group Rickettsia and Leptospira species [10, 11]. Tissues were also evaluated with a polyclonal rabbit sera generated against the HRTV nucleocapsid protein as previously described [1].
RNA detection, characterization and isolation
RNA was extracted from pre-mortem blood and serum samples as well as fixed post-mortem spleen and lymph tissues. Quantitative real-time RT-PCR for the detection of HRTV RNA was performed at Arboviral Diseases Branch, CDC, Fort Collins, CO using previously described methods [2]. HRTV genomic sequencing was conducted using Next Generation Sequencing methodologies as previously described [12]. Sequences were confirmed through spot sequencing using traditional Sanger methods and previously published primers [2]. Maximum likelihood phylogenetic analyses were conducted using MEGA version 5 software [13], with 2000 replicates for bootstrap testing. The blood sample was additionally subjected to standard virus isolation methods. Briefly, 200μL of undiluted and 10−1 preparations of the blood sample were inoculated onto confluent Vero cells in a T25 flask. The flask was then incubated at 37°C and reviewed for cytopathic effect daily.
RESULTS
IHC assays for Ehrlichia, Anaplasma, spotted fever group Rickettsia and Leptospira species were negative. White pulp depletion and scattered immunoblasts were observed in the spleen suggestive of a viral infection (figure 2A). Given the clinical history and negative test results, HRTV was suspected. IHC for HRTV was performed and demonstrated positive immunostaining of scattered large hematopoietic cells within the spleen and mediastinal and mesenteric lymph nodes (figure 2B&C). No other organs stained positive, including bone marrow, liver, kidneys, adrenal glands and CNS.
Figure 2.
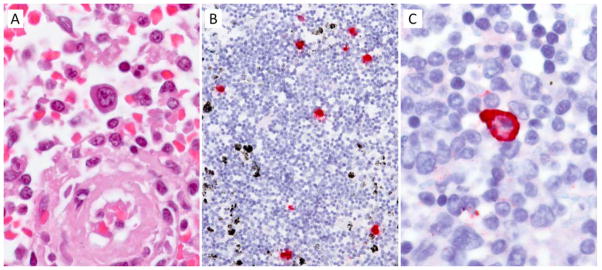
Pathological features of fatal HRTV case. Spleen demonstrating white pulp depletion and scattered immunoblasts (A). HRTV antigen detected in large hematopoietic cells of lymph node (B) and spleen (C) by immunohistochemistry using fast red chromogen. Original magnifications: 158X(A), 50X(B) and 158X(C)
The IHC finding was confirmed by detecting HRTV RNA in paraffin embedded tissues and from whole blood and serum (collected on hospital days 2 and 5, respectively) by RT-PCR and sequencing. In addition, an isolate was derived from the whole blood sample on day 16 post inoculation and was identified as HRTV by RT-PCR.
Full length phleboviral coding sequences representing all three segments of the phlebovirus genome, S, M and L (GenBank Accession #s: KJ740146, KJ740147, and KJ740148) were derived from the patient’s blood. Resultant analyses confirmed HRTV as the source of these sequences that share ~96.5% nucleotide sequence identity with other HRTV isolates in the 581 bp region of the non-structural protein (NSs) ORF of the S segment for which there is the broadest diversity of available data in GenBank. Phylogenetic analyses, including a diversity of phleboviruses as well as representative human and tick HRTV sequences [2], confirmed this identification (figure 3).
Figure 3.
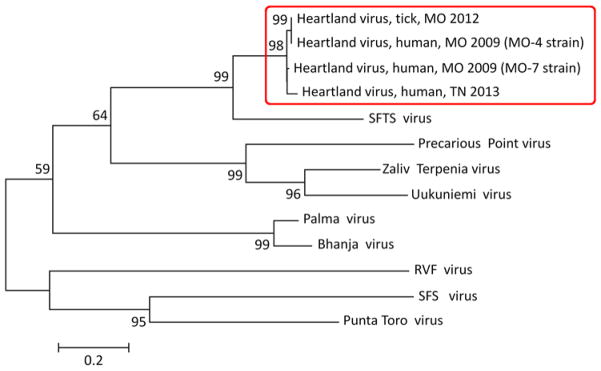
Phylogeny of phleboviruses including Heartland virus isolates. A maximum likelihood tree that was generated using MEGA version 5 software [8] with 2000 replicates for bootstrap testing is shown. The phylogeny was constructed from a 581 bp region of the NSs ORF of the phleboviral S segment for which there is the broadest diversity of available data in GenBank. Branch lengths are measured in the number of nucleotide substitutions per site.
DISCUSSION
This is the first reported case of fatal HRTV infection, which was revealed by autopsy of an 80 year-old man from central Tennessee with unexplained illness. Similar to the current case, the two index HRTV case-patients from Missouri were older male farmers who presented with fever, leukopenia and thrombocytopenia. However, the original two HRTV cases were younger (57 and 67 years), had higher platelet count nadirs at 34–37 × 103/μL, did not require transfusions, and both survived without hemorrhagic manifestations or multi-organ failure. HRTV antigen was detected by immunohistochemistry in a bone marrow biopsy collected from one of the first case-patients on hospital day 2, whereas the current patient had HRTV antigen detected at autopsy (hospital day 15) in lymph nodes and spleen, but notably not bone marrow, suggesting that antigen distribution may change over the disease course.
The elderly age, weakened immune system and co-morbidities of the current patient most likely predisposed to severity of HRTV infection and fatal outcome. The majority of SFTSV deaths in China have been in patients >70 years old [9], and occurred more frequently among patients who had CNS manifestations, hemorrhage and elevated liver enzymes [8]. Death has been associated independently with increasing age, decreased level of consciousness, elevated LDH levels (>1200 U/L) and elevated levels of creatine kinase (>800 U/L)[14]; all of which were present in the current HRTV case. Further, more severe SFTSV infections have been observed in patients with underlying chronic disease [7]. Disseminated intravascular coagulopathy has been described in some cases of SFTSV infection, but was not seen in this or in the previous HRTV cases.
The finding of viral antigen positive hematopoietic cells in lymph node and spleen with our cases is similar to that seen with a fatal SFTSV case from Japan [6]. However the SFTSV case also described necrotizing lymphadenopathy and extensive hemophagocytosis which were not seen in the current case. Antigen-positive hematopoietic cells have also been described in the spleen of mice experimentally infected with SFTSV[15].
This patient lived approximately 340 miles away from the closest case [3]and is the first HRTV case outside of Missouri, expanding the known geographic range of the virus. This is further supported by the percent nucleotide divergence (~4% in the compared region of the NSs ORF) of the presented strain from Tennessee when compared to previously described strains in Missouri. This divergence represents a level that is greater than that which has been previously described among human and A. americanum tick strains of HRTV (~2%). This suggests that the virus has been naturally circulating in Tennessee for some time and indicates that the known geographic range of HRTV expands beyond that of the first described cases and supports additional investigation in surrounding geographic areas.
The clinical differential for HRTV infection includes Ehrlichia, Anaplasma and Rickettsia rickettsii infection, viral disease and non-infectious entities such as thrombocytopenic thrombotic purpura or hematological neoplasms. The clinical course of HRTV appeared indistinguishable from severe infection with Ehrlichia chaffeensis, with the exception that the patients did not improve with doxycycline therapy [1]. HRTV infection should be considered in patients with fever, thrombocytopenia and leukopenia occurring in spring-summer months who report recent tick exposure, following exclusion of other tick-borne diseases. The reported HRTV patients were residents within the geographic range of the A. americanum tick, primarily the southeastern and eastern United States [16, 17]. A. americanum is a likely vector based on the detection of HRTV in these ticks [2]; however, formal studies on competency of A. americanum and other tick species to transmit HRTV are needed. Similar to reports from China, this case suggests that older adults or persons with co-morbidities might be at risk for more severe HRTV disease, but this needs to be validated with additional case finding and description. Finally, this case highlights the importance of autopsies for the detection and surveillance of emerging pathogens in unexplained deaths [18].
Currently, there is no treatment for HRTV disease. The best way to avoid HRTV is to prevent tick bites through using insect repellents, removing ticks promptly, applying pesticides, and reducing tick habitat. The CDC is currently working with state health departments to better define the epidemiology and clinical characteristics of HRTV disease, to validate how the virus is transmitted to persons (e.g., tick-borne), and to develop diagnostic assays for HRTV. Clinicians who have a suspect case of HRTV disease are encouraged to call their state health department to facilitate testing at CDC.
Acknowledgments
We thank Tim Jones, John Dunn, and Abelardo Moncayo (Tennessee Department of Health), Robert Hoffman (Vanderbilt University Medical Center), Marc Fischer and Daniel Pastula (Arboviral Diseases Branch, CDC), Laura McMullan (Viral Special Pathogens Branch, CDC), Clifton Drew, Jana Ritter, Wun-Ju Shieh, Brigid Batten and Pat Greer (Infectious Diseases Pathology Branch, CDC). All authors declare no competing interests. Funded by the Centers for Disease Control and Prevention.
Footnotes
DISCLAIMER:
The views expressed in this article are those of the authors and do not necessarily represent the official position of the CDC.
DISCLOSURES
MS has received consulting fees from Hospice Compassus. All other authors have no reported disclosures.
References
- 1.McMullan LK, Folk SM, Kelly AJ, et al. A new phlebovirus associated with severe febrile illness in Missouri. The New England journal of medicine. 2012;367(9):834–41. doi: 10.1056/NEJMoa1203378. [DOI] [PubMed] [Google Scholar]
- 2.Savage HM, Godsey MS, Jr, Lambert A, et al. First detection of heartland virus (Bunyaviridae: Phlebovirus) from field collected arthropods. The American journal of tropical medicine and hygiene. 2013;89(3):445–52. doi: 10.4269/ajtmh.13-0209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pastula DM, Turabelidze G, Yates KF, et al. Notes from the field: heartland virus disease - United States, 2012–2013. MMWR Morbidity and mortality weekly report. 2014;63(12):270–1. [PMC free article] [PubMed] [Google Scholar]
- 4.Yu XJ, Liang MF, Zhang SY, et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. The New England journal of medicine. 2011;364(16):1523–32. doi: 10.1056/NEJMoa1010095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim KH, Yi J, Kim G, et al. Severe Fever with thrombocytopenia syndrome, South Korea, 2012. Emerging infectious diseases. 2013;19(11) doi: 10.3201/eid1911.130792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Takahashi T, Maeda K, Suzuki T, et al. The First Identification and Retrospective Study of Severe Fever with Thrombocytopenia Syndrome in Japan. The Journal of infectious diseases. 2013 doi: 10.1093/infdis/jit603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Deng B, Zhou B, Zhang S, et al. Clinical Features and Factors Associated with Severity and Fatality among Patients with Severe Fever with Thrombocytopenia Syndrome Bunyavirus Infection in Northeast China. PloS one. 2013;8(11):e80802. doi: 10.1371/journal.pone.0080802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gai ZT, Zhang Y, Liang MF, et al. Clinical progress and risk factors for death in severe fever with thrombocytopenia syndrome patients. The Journal of infectious diseases. 2012;206(7):1095–102. doi: 10.1093/infdis/jis472. [DOI] [PubMed] [Google Scholar]
- 9.Ding F, Zhang W, Wang L, et al. Epidemiologic features of severe fever with thrombocytopenia syndrome in China, 2011–2012. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013;56(11):1682–3. doi: 10.1093/cid/cit100. [DOI] [PubMed] [Google Scholar]
- 10.Dawson JE, Paddock CD, Warner CK, et al. Tissue diagnosis of Ehrlichia chaffeensis in patients with fatal ehrlichiosis by use of immunohistochemistry, in situ hybridization, and polymerase chain reaction. The American journal of tropical medicine and hygiene. 2001;65(5):603–9. doi: 10.4269/ajtmh.2001.65.603. [DOI] [PubMed] [Google Scholar]
- 11.Paddock CD, Greer PW, Ferebee TL, et al. Hidden mortality attributable to Rocky Mountain spotted fever: immunohistochemical detection of fatal, serologically unconfirmed disease. The Journal of infectious diseases. 1999;179(6):1469–76. doi: 10.1086/314776. [DOI] [PubMed] [Google Scholar]
- 12.Huhtamo E, Lambert AJ, Costantino S, et al. Isolation and full genomic characterization of Batai virus from mosquitoes, Italy 2009. The Journal of general virology. 2013;94(Pt 6):1242–8. doi: 10.1099/vir.0.051359-0. [DOI] [PubMed] [Google Scholar]
- 13.Tamura K, Peterson D, Peterson N, Stecher G, Nei M, Kumar S. MEGA5: molecular evolutionary genetics analysis using maximum likelihood, evolutionary distance, and maximum parsimony methods. Molecular biology and evolution. 2011;28(10):2731–9. doi: 10.1093/molbev/msr121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liu W, Lu QB, Cui N, et al. Case-fatality ratio and effectiveness of ribavirin therapy among hospitalized patients in china who had severe fever with thrombocytopenia syndrome. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013;57(9):1292–9. doi: 10.1093/cid/cit530. [DOI] [PubMed] [Google Scholar]
- 15.Jin C, Liang M, Ning J, et al. Pathogenesis of emerging severe fever with thrombocytopenia syndrome virus in C57/BL6 mouse model. Proceedings of the National Academy of Sciences of the United States of America. 2012;109(25):10053–8. doi: 10.1073/pnas.1120246109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cortinas R, Spomer S. Lone star tick (Acari: Ixodidae) occurrence in Nebraska: historical and current perspectives. Journal of medical entomology. 2013;50(2):244–51. doi: 10.1603/me12207. [DOI] [PubMed] [Google Scholar]
- 17.Paddock CD, Yabsley MJ. Ecological havoc, the rise of white-tailed deer, and the emergence of Amblyomma americanum-associated zoonoses in the United States. Current topics in microbiology and immunology. 2007;315:289–324. doi: 10.1007/978-3-540-70962-6_12. [DOI] [PubMed] [Google Scholar]
- 18.Lynfield R, Nolte KB, Schmitz AM, Fischer M. Surveillance for Unexplained Infectious Disease-related Deaths. In: M’Ikanatha NM, Lynfield R, Van Beneden CA, de Valk H, editors. Infectious disease surveillance. 2. Chichester, West Sussex: Wiley-Blackwell; 2013. pp. 223–33. [Google Scholar]