

Abstract
Aims:
A crossover double-blind, randomized study was designed to explore the efficacy of 2% mepivacaine with 1:100,000 adrenaline buccal infiltration and 4% articaine with 1:100,000 adrenaline buccal infiltration following 2% mepivacaine with 1:100,000 adrenaline inferior alveolar nerve block (IANB) for testing pulp anesthesia of mandibular first molar teeth in adult volunteers.
Materials and Methods:
A total of 23 healthy adult volunteers received two regimens with at least 1-week apart; one with 4% articaine buccal infiltration and 2% mepivacaine IANB (articaine regimen) and another with 2% mepivacaine buccal infiltration supplemented to 2% mepivacaine IANB (mepivacaine regimen). Pulp testing of first molar tooth was electronically measured twice at baseline, then at intervals of 2 min for the first 10 min, then every 5 min until 45 min postinjection. Anesthetic success was considered when two consecutive maximal stimulation on pulp testing readings without sensation were obtained within 10 min and continuously sustained for 45 min postinjection.
Results:
In total, the number of no sensations to maximum pulp testing for first molar teeth were significantly higher after articaine regimen than mepivacaine during 45 min postinjection (267 vs. 250 episodes, respectively, P < 0.001), however, both articaine and mepivacaine buccal infiltrations are equally effective in securing anesthetic success for first molar pulp anesthesia when supplemented to mepivacaine IANB injections (P > 0.05). Interestingly, volunteers in the articaine regimen provided faster onset and longer duration (means 2.78 min, 42.22 min, respectively) than mepivacaine regimen (means 4.26 min, 40.74 min, respectively) for first molar pulp anesthesia (P < 0.001).
Conclusions:
Supplementary mepivacaine and articaine buccal infiltrations produced similar successful first molar pulp anesthesia following mepivacaine IANB injections in volunteers. Articaine buccal infiltration produced faster onset and longer duration than mepivacaine buccal infiltration following mepivacaine IANB injections.
Keywords: Adrenaline, articaine, buccal infiltration, first molar pulp anesthesia, inferior alveolar nerve block, mepivacaine
INTRODUCTION
The ability of articaine infiltrations to secure pulp anesthesia in mandibular molars,[1] and the superiority of articaine infiltration over lidocaine[2,3] provided important new avenues for investigation. It has been theorized that supplementary injection of articaine buccal infiltration may add additional successful pulp anesthesia for mandibular teeth after an inferior alveolar nerve block (IANB) with the use of lidocaine.[4] The investigations over supplementary articaine buccal infiltration following lidocaine IANB injection provided significant differences for successful pulp anesthesia in lower mandibular teeth than when lidocaine injection administered alone.[5] The superiority of articaine buccal infiltration following lidocaine IANB injection was enormously remarkable for pain free treatment for mandibular teeth with irreversible pulpitis.[6] However, no trail in the literature has ever investigated the influence of articaine and mepivacaine buccal infiltration following 2% mepivacaine IANB. The aim of this study is to assess the depth of local anesthesia in healthy adult volunteers’ first molar teeth when buccal infiltration of 2% mepivacaine with adrenaline (1:100,000) and 4% articaine with adrenaline (1:100,000) were supplemented to 2% mepivacaine and adrenaline (1:100,000) local anesthetic solution.
MATERIALS AND METHODS
A crossover double-blind, randomized study design was employed. Official clearances and ethics were secured from Taibah University and the College of Dentistry in Al Madinah Al Munawwarah, Saudi Arabia. Inclusion criteria were considered for volunteers who were 17-60 years of age, with intact first molar teeth, American Society of Anesthesiologists (ASA) I patients (ASA, 1994). A study information sheet was available for every volunteer to read, understand and ask before they signed the consent form. Exclusion criteria were considered for individuals who were allergic to local anesthetics, with bilateral nonvital or missing lower first molar teeth, with bilateral composite or amalgam fillings of lower first molar teeth and individuals who were unable to complete the trail. Twenty-five volunteers, ranged in age between 17 and 60 years old, were invited to participate in this trial after reading the information study sheets and signing the related consent form. Two regimens were randomly administered with at least 1-week apart. Randomization was achieved by an independent researcher (KHA).
In one visit, patients received 1.8 mL mepivacaine 2% with adrenaline (1:100,000) IANB and 1.8 mL mepivacaine 2% with adrenaline (1:100,000) buccal infiltration (scandicaine 2% [2% mepivacaine with 1:00.000 epinephrine Septodont, France]). In another visit, patients received 1.8 mL mepivacaine 2% with adrenaline (1:100,000) IANB and 1.8 mL articaine 4% with adrenaline (1:100,000) buccal infiltration (Septanest SP. Articaine hydrochloride 4% with 1:00.000 epinephrine - Septodont, France). In mepivacaine IANB injections, the injection site was determined midway between the internal oblique ridge and the pterygomandibular raphe and the needle was advanced until an adequate bony contact is achieved (IANB: Direct or Halstead approach); then 1.8 mL mepivacaine 2% with adrenaline 1:100,000, was delivered slowly over 60 s after aspiration.[7] In both regimens, there was no deposition of anesthetic solution when the needle is advanced to the target site.[8] Articaine or mepivacaine buccal infiltrations (1.8 mL) were administered in the buccal mucosa of the mandibular first molar teeth over 60 s after aspiration. Both volunteers and the researcher testing anesthetic effectiveness (American Medical Association) were not aware to which local anesthetic buccal infiltration regimen, was administered. All injections were given by the same operator (GG). All IANB injections were given with standard aspirating dental cartridge syringes (USA: ATI) fitted with 27-gauge, 30 mm long needles (C-K Ject (27-gauge) 0.4 mm × 30 mm, Korea) while 27-gauge, 21 mm short needles (C-K Ject (27-gauge) 0.4 mm × 21 mm, Korea) were used for buccal infiltrations. The effectiveness of pulp anesthesia was assessed by stimulating the pulps of a mandibular first molar tooth at the tip of mesiobuccal cusp[9] on one side of the mouth with an electronic pulp tester (parkell products USA: Digitest pulp vitality tester: STOCK number D626D with maximum stimulation 64). Testing was undertaken at baseline twice, then at the following registration points: 2, 4, 6, 8, 10, 15, 20, 25, 30, 35, 40 and 45 min after injection. A control tooth on the other side of the mandible was also tested for validity at the following points: Baseline, 10 min, and 45 min after injection.[8] A successful measure was considered when no sensation, was reported, on maximal first molar pulp testing (64 reading). Anesthetic success criterion was considered when two consecutive maximal stimulation on pulp testing readings were obtained within 10 min and continuously sustained for 45 min postinjection. Onset and duration of first molar pulp anesthesia were recorded after both regimens.[7] Data were entered and analyzed in statistical software package SPSS version 20 (SPSS Inc., Chicago, IL).
RESULTS
A total of 25 healthy adult volunteers were recruited. Two volunteers were excluded due to faint following first local anesthetic IANB injection (one volunteer from mepivacaine regimen and one from articaine regimen) and were excluded consequently according to study protocol and official clearances. The final sample size included 23 volunteers aged between 17 and 60 years old (mean 29.9 years, standard deviation [SD] 10.77). Twelve volunteers received mepivacaine IANB and articaine buccal infiltration first. All volunteer participants received their IANB injections and buccal infiltrations on the right side of the mandible.
Frequency of pulp anesthesia: 64 reading versus time intervals
Figure 1 shows the percentage of episodes of no sensations to first molar teeth pulp testing on 64 reading (maximum stimulation) after mepivacaine IANB plus articaine buccal infiltration (267 episodes: Articaine regimen) and mepivacaine IANB plus mepivacaine buccal infiltration (250 episodes: Mepivacaine regimen). This difference was statistically significant (P < 0.001).
Figure 1.
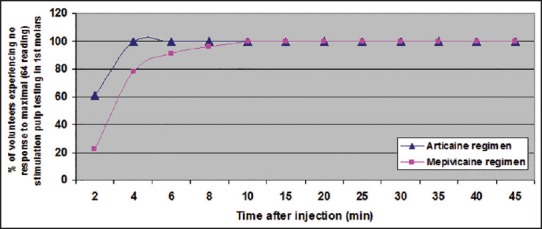
Percentage of 23 adult healthy volunteers recording first molar pulp anesthesia (1 × 64 stimulation without sensation) with time after mepivacaine inferior alveolar nerve block (IANB) plus articaine buccal infiltration (articaine regimen) and mepivacaine IANB plus mepivacaine buccal infiltration (mepivacaine regimen)
Anesthetic success
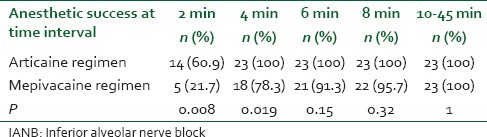
All (23 volunteers) secured anesthetic success for first molar tooth following pulp testing after articaine and mepivacaine regimens within 10 min and continuously sustained for 45 min postinjection (P = 1). Table 1 shows that the differences between articaine buccal infiltration supplemented to mepivacaine IANB (articaine regimen) and mepivacaine buccal infiltration supplemented to mepivacaine IANB (mepivacaine regimen) are statistically significant in regard to the number of episodes when there are no sensation on first molar pulp testing on 64 reading (maximum stimulation) at 2 min (60.9% vs. 21.7%, respectively, P = 0.008) and 4 min (100% vs.78.3%%, respectively, P = 0.019) but not at 6 min (100% vs. 91.3%, respectively, P = 0.15) or 8 min (100% vs. 95.7%, respectively, P = 0.32).
Table 1.
Number and percentages of anesthetic successes at time interval for first molar pulp anesthesia following articaine buccal infiltration supplemented to mepivacaine IANB injection (articaine regimen) and mepivacaine buccal infiltration supplemented to mepivacaine IANB injection (mepivacaine regimen) in 23 adult healthy volunteers
Onset and duration of first molar pulp anesthesia
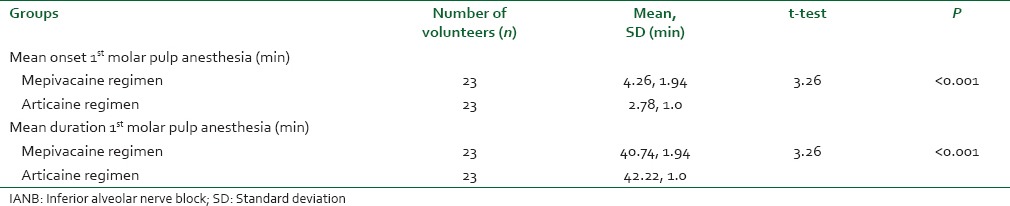
Table 2 reveals that the mean onset time of first molar pulp testing after articaine buccal infiltration supplemented to mepivacaine IANB (articaine regimen: mean 2.78 min, SD 1.0 min) was significantly faster than after mepivacaine buccal infiltration supplemented to mepivacaine IANB (mepivacaine regimen: 4.26 min, SD 1.94 min). Similarly, duration time of first molar pulp testing after articaine buccal infiltration supplemented to mepivacaine IANB (articaine regimen: Mean 42.22 min, SD 1.0 min) was significantly longer than after mepivacaine buccal infiltration supplemented to mepivacaine IANB (mepivacaine regimen: 40.74 min, SD 1.94 min).
Table 2.
Means onset and duration time (min) of first molar pulp anesthesia in 23 healthy adult volunteers after mepivacaine buccal infiltration supplemented to mepivacaine IANB (mepivacaine regimen) and articaine buccal infiltration supplemented to mepivacaine IANB (articaine regimen)
DISCUSSION
Mandibular teeth are rarely anesthetized by infiltration alone,[10] since poor drug penetration makes pulp anesthesia unpredictable in relation to IANB. It has been reported that articaine provides a marvelous level of successful dental local anesthesia in the maxillary and mandibular teeth.[3,11,12,13] Several articles in the literature have shown the efficacy of articaine and lidocaine, but the outcomes were equivocal.[14,15,16,17,18] Although more recent studies have shown that articaine buccal infiltration was satisfactory for first molar pulp anesthesia,[3,8] failures were, however, reported. A recent volunteer study has found that buccal infiltration was just as successful as IANB for first molar pulp anesthesia in 30 volunteers who received 1.7 mL local anesthetic solution with 4% articaine and 1:100,000 epinephrine for each injection regimen.[19] Similar results were also reported at same time[20] and previously.[7] Still, 100% successful pulp anesthesia has not been achieved. The regional IANB alone is not guaranteed to provide complete anesthesia in volunteers[5] and patients suffering from irreversible pulpitis.[21,22] One study investigated lidocaine infiltration anesthesia during different dental procedures to overcome failed IANB injections.[23] Nevertheless, a single-blind randomized cross over study has stated that buccal or lingual infiltration with lidocaine supplemental IANB with lidocaine does not provide better pulpal anesthesia than IANB injection with lidocaine alone,[4] however,[4] based on previous investigations believed that articaine buccal infiltration may play an important role in such success[2] following IANB injection, which has been confirmed consequently.[5] Still, there was a greater concern when 4% articaine is to be used. There was an increase in the number of patients who experienced paresthesia of the lower lip following articaine IANB and 10 cases of paresthesia out of 4,398,970 cartridges administered were reported in 1993 alone. Four cases out of 2,353,615 cartridges were also reported with paresthesia following 4% prilocaine use, but none following the administration of 3,062,613 cartridges of 2% lidocaine or 1,569,037 cartridges of mepivacaine, administered in the same year.[24] The incidence of paresthesia was more common after 4% articaine (10/569 cases) than 2% lidocaine injection (1/286 case) and that was why 4% articaine has been advised for infiltration use but not for IANB injection.[25] Concerns have not been expressed about articaine infiltration, and articaine was proved to be more successful than lidocaine, with no complications been recorded.[8] Mepivacaine local anesthetic drug frequently used in dentistry, one study involved children (50 patients: 7-13 years old) showed longer duration of soft tissue anesthesia in articaine than mepivacaine although no significant difference was noted during operative procedures in symmetric primary teeth based on Wong-Baker FACES pain rating scale.[26] In 18 volunteer adults,[27] one cross over double-blind randomized trial, compared six local anesthetic formulations namely; 2% lidocaine with 1:100,000 adrenaline, 4% articaine with 1:100,000 adrenaline, 4% articaine with 1:200,000 adrenaline, 4% prilocaine with 1:200,000 adrenaline, 3% mepivacaine without vasoconstrictor and 0.5% bupivacaine with 1:200,000 adrenaline for mandibular infiltration injections (six sessions per participant) of 0.9 mL of anesthetic into the buccal fold adjacent to the distal root of the mandibular first molar at the University of Pittsburgh, USA. Mepivacaine without vasoconstrictor and articaine with 1:100,000 adrenaline produced better pulp anesthesia (the maximum mean increase from baseline of electric pulp testing measurements) than other local anesthetic solutions (68.3% and 77.3%, respectively). The only significant difference was between articaine (1:100,000 adrenaline) and lidocaine (P = 0.029). Hence, the authors suggested that the mandibular infiltration with the tested dental anesthetics could produce only partial pulpal anesthesia, that unlikely to provide appropriate local anesthesia for most dental treatments.
The current study has formally considered the differences between articaine and mepivacaine with adrenaline buccal infiltration following IANB injection with 2% mepivacaine and adrenaline (1:100,000) as a potential valuable trail for pulp anesthesia in mandibular first molar teeth.
This study showed that the total number of episodes of no sensations to 64 reading pulp testing (maximum stimulation) for first molar teeth were significantly more successful following mepivacaine IANB with articaine buccal infiltration (267 episodes) of those received mepivacaine IANB with mepivacaine buccal penetration (250 episodes) during 45 min postinjection. Four percent articaine local anesthetic solution may be a key factor of such success due to the increased concentration compared to lidocaine (2%). The superiority of articaine buccal infiltration for first molar tooth pulp anesthesia has been reported.[3] Moreover, the increased liposolubility of articaine[25] may allow it to diffuse more easily into the tissues and provide more effective anesthesia during extraction of maxillary teeth.[13] Similarly, securing local anesthetic success may be by absorption through the mental foramen[10,28] quicker in articaine due to the higher concentration it has. However, it was reported previously that 2% articaine and 4% articaine (1:100,000) produced similar outcomes.[29,30]
Depth of local anesthesia can be assessed by electronic pulp testing, with the expectation that a negative response will equate with deep pulpal anesthesia.[31] In the current trial, electronic pulp testing was therefore employed for all volunteers to assess the depth of local anesthesia in first molar teeth. A variety of definitions of success has been employed in volunteer studies. In many, two consecutive 80 readings, or more, on pulp testing without sensation were considered as successful pulp anesthesia.[19,20,28,32,33,34,35,36,37,38] The current study, considered even a more stringent criterion. Only volunteers who achieved the maximal stimulation on first molar pulp testing (64 reading) without sensation within 10 min and continuously sustained for 45 min postinjection, were considered successful. This equates, to that considered by others.[10,35] The differences between the pulp testing device used in the current study (maximum stimulation 64 readings) and previous studies (maximum stimulation 80 readings), have not been investigated, future studies merit further investigations in this regard.
All 23 volunteers (100%) secured anesthetic success for first molar pulp anesthesia following articaine and mepivacaine regimens. However, the number of episodes of no sensation to first molar pulp testing (64 reading) were statistically significant in articaine regimen compared to mepivacaine regimen at 2 min (60.9% vs. 21.7%, respectively) and 4 min (100% vs. 78.3%%, respectively) but not at 6 min (100% vs. 91.3%, respectively) or 8 min [100% vs. 95.7%, respectively: Table 1].
About 4% solutions of prilocaine or articaine[39] may not be the only reason for the differences observed since 4% articaine was not superior to 2% articaine in one study.[29] The thiophene ring of articaine may be considered as additional co-factor for articaine's superiority[17] increasing its liposolubility.[25] This enables articaine to diffuse more easily into the tissues and produce more effective anesthesia.[13] Articaine is a unique local anesthetic drug, although it is classified as an amide; it contains an ester side chain. Articaine acts as an ester in its metabolism, and the half-life of articaine is approximately 4 times less than lidocaine and other amide local anesthetic drugs necessitate hepatic clearance.[25]
This may give the opportunity to “top up” the injection within the maximum allowed dose. One could say that more local anesthetic solution is required to achieve success if either the concentration or the strength is low. It was intriguing however to report, that the concentration of local anesthetic solution has no influence on successful anesthesia[29] and when different doses of bupivacaine were administered for supraclavicular block.[40]
The literature has lack of significant evidence regarding mepivacaine local anesthetic in comparison with articaine contemporaneous local anesthetic drug. A result of systematic review,[41] provided an additional conclusion to the superiority of articaine usage compared to lidocaine for first molar pulp teeth with similar adverse effects. One study stated that 4% articaine provided more success than 2% lidocaine did, but this did not achieve a statistical significance.[42] This study stated that articaine buccal injection resulted in speed of the anesthetic onset and longer duration of action compared to mepivacaine buccal injection. This result is in consistence with the findings of one study[43] that reported the clinical advantages of articaine infiltration including quicker onset of pulp anesthesia, longer duration of action, in addition to a greater diffusing property over lidocaine local anesthetic solution.
In the present study, the anesthetic effect for lower first molars peaked 4 min postinjection after articaine regimen (articaine buccal infiltration supplemented to mepivacaine IANB) and 10 min after mepivacaine regimen (mepivacaine buccal infiltration supplemented to mepivacaine IANB). Similar results were reported previously[5] that no sensation to maximum stimulation on pulp testing in first molar teeth peaked at 6 min when articaine infiltration supplemented to IANB injection but delayed to 25 min postinjection when lidocaine IANB injection was used alone. Robertson et al.[3] showed that no sensation to maximum stimulation on pulp testing in first molar teeth peaked between 10 and 20 min after infiltration of articaine buccally. Another study showed that no sensation to maximum stimulation on pulp testing in first molar teeth peaked between 12 and 20 min after infiltration of lidocaine buccally plus IANB injection.[4] Similar results were reported by Nist et al.[10] This study showed that the mean onset of first molar pulp anesthesia was significantly quicker in articaine regimen (2.78 min) compared with mepivacaine regimen (4.26 min). One study reported a slower onset of first molar pulp anesthesia (10.8 min) following lidocaine IANB injection. This was earlier after mepivacaine (8.2 min) and delayed to 11.0 min after the prilocaine.[32] Nevertheless, these results suggest that if mepivacaine IANB with articaine buccal infiltration is administered in the buccal mucosa of mandibular first molar tooth, no dental treatment should commence before at least 4 min. The corresponding figure should be extended at least 10 min if mepivacaine IANB with mepivacaine buccal infiltration is used. Similarly, this study showed that the mean duration of first molar pulp anesthesia was significantly longer in articaine regimen group (42.22 min) compared to mepivacaine regimen group (40.74 min). The current results are compatible with previous studies.[3,11,12] From the clinical point of view, buccal infiltrations of articaine following mepivacaine IANB injections are more effective than mepivacaine infiltration supplemented to mepivacaine IANB injection in securing pulp anesthesia for mandibular first molar teeth. Interestingly, both regimens achieved anesthetic success at 10 min until 45 min postinjections allowing a wide flexibility for selection of local anesthetic solutions.
Intraosseous (IO) anesthesia is the most ideal technique when the first IANB fails to achieve success. Few research studies showed that IANB plus IO anesthesia has produced complete first molar pulp anesthesia.[44,45,46] The current data show that using articaine or mepivacaine buccal infiltrations with IANB injections provided similar success of first molar pulp anesthesia at 10 min until 45 min postinjection and comparable to other repeated measures including IO anesthesia when administered with IANB injections.[34,47]
Infiltration anesthesia is a straightforward technique and does not necessitate the particular equipment essential for IO injection techniques. Moreover, articaine or mepivacaine infiltration, when supplemented to IANB, produces similar pulp anesthesia to that with IO anesthesia. The currently available data warrant further investigation in patients attending with irreversible pulpitis.
CONCLUSIONS
Supplementary mepivacaine and articaine buccal infiltrations produced similar anesthetic success for first molar pulp anesthesia following mepivacaine IANB injections in volunteers. Articaine buccal infiltration produced faster onset and longer duration than mepivacaine buccal infiltration following mepivacaine IANB injections.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Haas DA, Harper DG, Saso MA, Young ER. Lack of differential effect by Ultracaine (articaine) and Citanest (prilocaine) in infiltration anesthesia. J Can Dent Assoc. 1991;57:217–23. [PubMed] [Google Scholar]
- 2.Kanaa MD, Meechan JG, Corbett IP, Whitworth JM. Mandibular block or buccal infiltration for pulp anesthesia in molars? Int Endod J. 2006;39:740. [Google Scholar]
- 3.Robertson D, Nusstein J, Reader A, Beck M, McCartney M. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J Am Dent Assoc. 2007;138:1104–12. doi: 10.14219/jada.archive.2007.0324. [DOI] [PubMed] [Google Scholar]
- 4.Foster W, Drum M, Reader A, Beck M. Anesthetic efficacy of buccal and lingual infiltrations of lidocaine following an inferior alveolar nerve block in mandibular posterior teeth. Anesth Prog. 2007;54:163–9. doi: 10.2344/0003-3006(2007)54[163:AEOBAL]2.0.CO;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kanaa MD, Whitworth JM, Corbett IP, Meechan JG. Articaine buccal infiltration enhances the effectiveness of lidocaine inferior alveolar nerve block. Int Endod J. 2009;42:238–46. doi: 10.1111/j.1365-2591.2008.01507.x. [DOI] [PubMed] [Google Scholar]
- 6.Kanaa MD, Whitworth JM, Meechan JG. A prospective randomized trial of different supplementary local anesthetic techniques after failure of inferior alveolar nerve block in patients with irreversible pulpitis in mandibular teeth. J Endod. 2012;38:421–5. doi: 10.1016/j.joen.2011.12.006. [DOI] [PubMed] [Google Scholar]
- 7.Kanaa MD, Meechan JG, Corbett IP, Whitworth JM. Speed of injection influences efficacy of inferior alveolar nerve blocks: A double-blind randomized controlled trial in volunteers. J Endod. 2006;32:919–23. doi: 10.1016/j.joen.2006.04.004. [DOI] [PubMed] [Google Scholar]
- 8.Kanaa MD, Whitworth JM, Corbett IP, Meechan JG. Articaine and lidocaine mandibular buccal infiltration anesthesia: A prospective randomized double-blind cross-over study. J Endod. 2006;32:296–8. doi: 10.1016/j.joen.2005.09.016. [DOI] [PubMed] [Google Scholar]
- 9.Lin J, Chandler N, Purton D, Monteith B. Appropriate electrode placement site for electric pulp testing first molar teeth. J Endod. 2007;33:1296–8. doi: 10.1016/j.joen.2007.08.006. [DOI] [PubMed] [Google Scholar]
- 10.Nist RA, Reader A, Beck M, Meyers WJ. An evaluation of the incisive nerve block and combination inferior alveolar and incisive nerve blocks in mandibular anesthesia. J Endod. 1992;18:455–9. doi: 10.1016/S0099-2399(06)80849-6. [DOI] [PubMed] [Google Scholar]
- 11.Oliveira PC, Volpato MC, Ramacciato JC, Ranali J. Articaine and lignocaine efficiency in infiltration anesthesia: A pilot study. Br Dent J. 2004;197:45–6. doi: 10.1038/sj.bdj.4811422. [DOI] [PubMed] [Google Scholar]
- 12.Costa CG, Tortamano IP, Rocha RG, Francischone CE, Tortamano N. Onset and duration periods of articaine and lidocaine on maxillary infiltration. Quintessence Int. 2005;36:197–201. [PubMed] [Google Scholar]
- 13.Uckan S, Dayangac E, Araz K. Is permanent maxillary tooth removal without palatal injection possible? Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:733–5. doi: 10.1016/j.tripleo.2005.12.005. [DOI] [PubMed] [Google Scholar]
- 14.Vähätalo K, Antila H, Lehtinen R. Articaine and lidocaine for maxillary infiltration anesthesia. Anesth Prog. 1993;40:114–6. [PMC free article] [PubMed] [Google Scholar]
- 15.Malamed SF, Gagnon S, Leblanc D. A comparison between articaine HCl and lidocaine HCl in pediatric dental patients. Pediatr Dent. 2000;22:307–11. [PubMed] [Google Scholar]
- 16.Malamed SF, Gagnon S, Leblanc D. Efficacy of articaine: A new amide local anesthetic. J Am Dent Assoc. 2000;131:635–42. doi: 10.14219/jada.archive.2000.0237. [DOI] [PubMed] [Google Scholar]
- 17.Malamed SF, Gagnon S, Leblanc D. Articaine hydrochloride: A study of the safety of a new amide local anesthetic. J Am Dent Assoc. 2001;132:177–85. doi: 10.14219/jada.archive.2001.0152. [DOI] [PubMed] [Google Scholar]
- 18.Claffey E, Reader A, Nusstein J, Beck M, Weaver J. Anesthetic efficacy of articaine for inferior alveolar nerve blocks in patients with irreversible pulpitis. J Endod. 2004;30:568–71. doi: 10.1097/01.don.0000125317.21892.8f. [DOI] [PubMed] [Google Scholar]
- 19.Jung IY, Kim JH, Kim ES, Lee CY, Lee SJ. An evaluation of buccal infiltrations and inferior alveolar nerve blocks in pulpal anesthesia for mandibular first molars. J Endod. 2008;34:11–3. doi: 10.1016/j.joen.2007.09.006. [DOI] [PubMed] [Google Scholar]
- 20.Corbett IP, Kanaa MD, Whitworth JM, Meechan JG. Articaine infiltration for anesthesia of mandibular first molars. J Endod. 2008;34:514–8. doi: 10.1016/j.joen.2008.02.042. [DOI] [PubMed] [Google Scholar]
- 21.Nusstein J, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of the supplemental intraosseous injection of 2% lidocaine with 1:100,000 epinephrine in irreversible pulpitis. J Endod. 1998;24:487–91. doi: 10.1016/S0099-2399(98)80053-8. [DOI] [PubMed] [Google Scholar]
- 22.Reisman D, Reader A, Nist R, Beck M, Weaver J. Anesthetic efficacy of the supplemental intraosseous injection of 3% mepivacaine in irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:676–82. doi: 10.1016/s1079-2104(97)90372-3. [DOI] [PubMed] [Google Scholar]
- 23.Rood JP. The analgesia and innervation of mandibular teeth. Br Dent J. 1976;140:237–9. doi: 10.1038/sj.bdj.4803742. [DOI] [PubMed] [Google Scholar]
- 24.Haas DA, Lennon D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. J Can Dent Assoc. 1995;61:319–20, 323. [PubMed] [Google Scholar]
- 25.Becker DE, Reed KL. Essentials of local anesthetic pharmacology. Anesth Prog. 2006;53:98–108. doi: 10.2344/0003-3006(2006)53[98:EOLAP]2.0.CO;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Odabas ME, Cinar C, Deveci C, Alaçam A. Comparison of the anesthetic efficacy of articaine and mepivacaine in pediatric patients: A randomized, double-blind study. Pediatr Dent. 2012;34:42–5. [PubMed] [Google Scholar]
- 27.Abdulwahab M, Boynes S, Moore P, Seifikar S, Al-Jazzaf A, Alshuraidah A, et al. The efficacy of six local anesthetic formulations used for posterior mandibular buccal infiltration anesthesia. J Am Dent Assoc. 2009;140:1018–24. doi: 10.14219/jada.archive.2009.0313. [DOI] [PubMed] [Google Scholar]
- 28.Whitworth JM, Kanaa MD, Corbett IP, Meechan JG. Influence of injection speed on the effectiveness of incisive/mental nerve block: A randomized, controlled, double-blind study in adult volunteers. J Endod. 2007;33:1149–54. doi: 10.1016/j.joen.2007.07.016. [DOI] [PubMed] [Google Scholar]
- 29.Hintze A, Paessler L. Comparative investigations on the efficacy of articaine 4% (epinephrine 1:200,000) and articaine 2% (epinephrine 1:200,000) in local infiltration anesthesia in dentistry — A randomised double-blind study. Clin Oral Investig. 2006;10:145–50. doi: 10.1007/s00784-005-0025-0. [DOI] [PubMed] [Google Scholar]
- 30.Gazal G, Wamiq FM, Zafar MS, Samadani KH. Pain and anxiety management for pediatric dental procedures using various combinations of sedative drugs: A review. Saudi Pharm J. 2014. Available from: http://dx.doi.org/10.1016/j.jsps.2014.04.004 . [DOI] [PMC free article] [PubMed]
- 31.Dreven LJ, Reader A, Beck M, Meyers WJ, Weaver J. An evaluation of an electric pulp tester as a measure of analgesia in human vital teeth. J Endod. 1987;13:233–8. doi: 10.1016/s0099-2399(87)80097-3. [DOI] [PubMed] [Google Scholar]
- 32.McLean C, Reader A, Beck M, Meryers WJ. An evaluation of 4% prilocaine and 3% mepivacaine compared with 2% lidocaine (1:100,000 epinephrine) for inferior alveolar nerve block. J Endod. 1993;19:146–50. doi: 10.1016/s0099-2399(06)80510-8. [DOI] [PubMed] [Google Scholar]
- 33.Dagher FB, Yared GM, Machtou P. An evaluation of 2% lidocaine with different concentrations of epinephrine for inferior alveolar nerve block. J Endod. 1997;23:178–80. doi: 10.1016/S0099-2399(97)80271-3. [DOI] [PubMed] [Google Scholar]
- 34.Reitz J, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of a repeated intraosseous injection given 30 min following an inferior alveolar nerve block/intraosseous injection. Anesth Prog. 1998;45:143–9. [PMC free article] [PubMed] [Google Scholar]
- 35.Clark S, Reader A, Beck M, Meyers WJ. Anesthetic efficacy of the mylohyoid nerve block and combination inferior alveolar nerve block/mylohyoid nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87:557–63. doi: 10.1016/s1079-2104(99)70133-2. [DOI] [PubMed] [Google Scholar]
- 36.Yonchak T, Reader A, Beck M, Clark K, Meyers WJ. Anesthetic efficacy of infiltrations in mandibular anterior teeth. Anesth Prog. 2001;48:55–60. [PMC free article] [PubMed] [Google Scholar]
- 37.Gallatin E, Stabile P, Reader A, Nist R, Beck M. Anesthetic efficacy and heart rate effects of the intraosseous injection of 3% mepivacaine after an inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:83–7. doi: 10.1016/s1079-2104(00)80019-0. [DOI] [PubMed] [Google Scholar]
- 38.Berlin J, Nusstein J, Reader A, Beck M, Weaver J. Efficacy of articaine and lidocaine in a primary intraligamentary injection administered with a computer-controlled local anesthetic delivery system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:361–6. doi: 10.1016/j.tripleo.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 39.Haas DA, Harper DG, Saso MA, Young ER. Comparison of articaine and prilocaine anesthesia by infiltration in maxillary and mandibular arches. Anesth Prog. 1990;37:230–7. [PMC free article] [PubMed] [Google Scholar]
- 40.Gupta PK, Hopkins PM. Effect of concentration of local anaesthetic solution on the ED50 of bupivacaine for supraclavicular brachial plexus block. Br J Anaesth. 2013;111:293–6. doi: 10.1093/bja/aet033. [DOI] [PubMed] [Google Scholar]
- 41.Meechan JG. The use of the mandibular infiltration anesthetic technique in adults. J Am Dent Assoc. 2011;142 Suppl 3:19S–24. doi: 10.14219/jada.archive.2011.0343. [DOI] [PubMed] [Google Scholar]
- 42.Kambalimath DH, Dolas RS, Kambalimath HV, Agrawal SM. Efficacy of 4 % Articaine and 2 % Lidocaine: A clinical study. J Maxillofac Oral Surg. 2013;12:3–10. doi: 10.1007/s12663-012-0368-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hawkins JM, Moore PA. Local anesthesia: Advances in agents and techniques. Dent Clin North Am. 2002;46:719–32, ix. doi: 10.1016/s0011-8532(02)00020-4. [DOI] [PubMed] [Google Scholar]
- 44.Guglielmotti MB, Guerrero C, Cabrini RL. Chronodynamic evaluation of the stages of osseointegration in zirconium laminar implants. Acta Odontol Latinoam. 1997;10:11–23. [PubMed] [Google Scholar]
- 45.Gallatin J, Reader A, Nusstein J, Beck M, Weaver J. A comparison of two intraosseous anesthetic techniques in mandibular posterior teeth. J Am Dent Assoc. 2003;134:1476–84. doi: 10.14219/jada.archive.2003.0077. [DOI] [PubMed] [Google Scholar]
- 46.Stabile P, Reader A, Gallatin E, Beck M, Weaver J. Anesthetic efficacy and heart rate effects of the intraosseous injection of 1.5% etidocaine (1:200,000 epinephrine) after an inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:407–11. doi: 10.1016/s1079-2104(00)70120-x. [DOI] [PubMed] [Google Scholar]
- 47.Dunbar D, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of the intraosseous injection after an inferior alveolar nerve block. J Endod. 1996;22:481–6. doi: 10.1016/S0099-2399(96)80083-5. [DOI] [PubMed] [Google Scholar]