

Abstract
Introduction:
The negative impact of inhaled antiasthmatic drugs (IAD) on oral health is reflected primarily in the increased incidence of caries in asthmatic children compared to healthy children. It is believed that one of the causes of the increased incidence of caries in asthmatic children is from bronchodilator effect in reduced secretion of saliva. Decreased salivation favors bacterial colonization and studies have shown that the concentration of Streptococcus mutans, a bacterium that has the primary role in the development of caries, is higher in asthmatic than in healthy children.
Material and methods:
The study sample consisted of 200 patients, age from 7-14 years, divided into two groups: control group (n1 = 100) consisted of healthy children and the experimental group consisted of children suffering from asthma (n2 = 100). In both groups of respondents are identified the DMFT values, the concentration of Streptococcus mutans, the amount of stimulated saliva and plaque index value.
Results:
It was found that there are significant differences in the values of plaque index, salivary index and streptococcus mutans between the control and experimental groups (p> 0.05 for each of the examined variables). Those in the control group had significantly higher DMFT index than subjects in the experimental group (p = 0.004).
Conclusion:
IAD does not cause reduced saliva production and thus do not represent a factor favoring increased concentration of Streptococcus mutans.
Keywords: Asthma, Streptococcus mutans, caries
1. INTRODUCTION
The negative impact of inhaled antiasthmatic drugs (IAD) on oral health is reflected primarily in the increased incidence of caries with asthmatic children compared to healthy children, as confirmed by various studies (1, 2, 3). It is believed that one of the causes of the increased incidence of caries in asthmatic children is a bronchodilator effect on reduced secretion of saliva (4, 5).
Decreased salivation and therefore deficit of its antibacterial components favors bacterial colonization and studies have shown that the concentration of Streptococcus mutans, a bacterium that has the primary role in the development of caries, is higher in asthmatic than in healthy children (5, 6). Both studies demonstrated a positive correlation between increased concentration of Streptococcus mutans and dental caries. Today, Streptococcus mutans is considered the main etiological microbiological factor in terms of caries, together with Lactobacillus and other bacteria participating in further progression of the disease. Why Streptococcus mutans seems predominant microbiological factors in pathogenesis of dental caries is its virulence factors that enable it to colonize and survive in biofilm or dental plaque that covers the tooth surface. These virulence factors are: surface-like proteins are adhesins, acid production and tolerance to the same, production of glucosyltransferase, mutacin and intracellular and extracellular polysaccharides that enhance adherence of them (7). Mutacins are bacteriocins, specific to S. mutans that negatively affect the growth of neighboring organisms. Glucosyltransferase is an enzyme essential to the cell wall and polymerization processes of Streptococcus mutans. The presence of antibodies to this antigen (protein) in the future may be of therapeutic interest (8).
Defensive role of saliva, lies not only in the mechanical cleaning of hard dental tissue, but larger problem in reduced secretion of saliva is reduced biosynthesis of biologically active components such as total protein, amylase, hexosamine, lysozyme, secretory IgA and salivary peroxidase, which represent important antibacterial components (9).
Research on caries in persons with deficient sIgA due to any reason have shown some correlation between the deficit in the secretion of sIgA and caries (10). Gregory et al. have found that levels of IgA2 in parotid saliva and serum IgG antibodies of the Streptococcus mutans antigen significantly increased in people resistant to caries than in caries sensitive individuals (11). This research supports the concept of immune regulation of caries present (natural) antibodies induced salivary antigens of S. mutans (12). The specificity of caries as an infection is that microorganisms in the beginning of the disease do not penetrate the enamel, but are found in large amounts on the surface of the enamel and act as pathogens. It is believed that salivary IgA is first line of host defense against pathogenic microorganisms that inhabit the surface coated external secretions. Salivary IgA bonds alien structures regroup them and inactivate toxic antigens. The main function of the secretory IgA antibody is to limit the adherence of microorganisms (their binding to the surface), as well as penetration of foreign antigens to the mucosa. Animal experiments showed that secretory IgA antibodies against Streptococcus mutans help to reduce the colonization of bacteria and caries prevalence (13, 14). Camling and colleagues in the research started from the fact that if the saliva antibodies against Streptococcus mutans are effective protection against decay, then the children with higher levels of these antibodies should have a smaller number of carious teeth. However they did not confirm their results (15). Following their logic, one might assume that children with reduced salivary flow and consequent quantitative changes in the quantity of saliva and thus the antibody should have a greater concentration of bacteria and more decayed teeth.
2. GOALS
-
■
Evaluate the level of oral hygiene in the experimental and control groups.
-
■
Determine the prevalence of dental caries in the experimental and control groups.
-
■
Perform salivary test to measure the amount of stimulated saliva per time unit in the experimental and control groups.
-
■
Determine the concentration of Streptococcus mutans in saliva samples in the experimental and control groups.
3. MATERIAL AND METHODS
Retrospective–prospective study included 100 children with asthma, of both sexes, aged 7 to 15 years, who are treated at the Clinic for children’s diseases Tuzla. Basic criteria for inclusion in the study are that all children are treated with antiasthmatic drugs for at least two years and they are children with persistent asthma which requires long-term therapy. A secondary source of data, for children suffering from asthma is medical records of the Department of Pulmonology and Outpatient Clinic for children’s diseases in Tuzla. The control group is composed of 100 healthy children who do not suffer from asthma or other systemic disease and that by age, sex and socioeconomic status correspond to the study group. A secondary source of data for the control group will be class diaries of Elementary School Banovici pupils. Subjects in both groups are chosen randomly.
By clinical examination is determined the dental status of each child by registration the number of carious and extracted teeth and teeth with filling of any kind.
By clinical examination, is also determined the level of oral hygiene by plaque index according Silness and Loe (16).
The amount of stimulated saliva is determined in the manner that to the child was previously given to chew paraffin block for one minute, until it gets tender, after which from the child that was previously informed on the procedure, the paraffin is taken out of the mouth and the child will swallow saliva. After that, paraffin is once again placed into the mouth and continues to chew the next 5 minutes. During chewing, the child does not swallow the saliva, but the whole saliva is collected during chewing and measured. The collected saliva, which is collected in plastic cups taken with a test tube and the amount of saliva is measured according to the gradations (it is not measured the saliva foam located on the surface of the container). The results are expressed by a milliliter of saliva secreted per minute, so that the total amount of collected saliva is divided with the number of minutes during which from the respondent was collected saliva.
The concentration of Streptococcus mutans will be determined using the Strip mutans test (the “Dentocult SM”), by the manufacturer Orion Diagnostic.
4. STATISTICAL ANALYSIS
For the experimental and control group are analyzed the following parameters:
-
■
Plaque index;
-
■
Streptococcus mutans level;
-
■
Salivary index;
-
■
DMFT INDEX (with an analysis of the components D, M, F).
In accordance with the objectives and hypotheses set research, data is analyzed by the following statistical methods:
For each parameter descriptive statistics is calculated which includes measures of central tendency (mean, median and mode), measures of dispersion (standard deviation, interquartile range), measures of asymmetry (curvature with standard error). Results are presented in tables and bar charts.
Before hypothesis testing will be performed normality distribution testing by Kolmogorov-Smirnov test.
5. RESULTS
Results of descriptive statistics for the parameters D, M, F, DMFT for the control and experimental groups:
-
■
DMFT index for the control group was 7.46 (± 4.08). On average, respondents had a 6.46 (± 4.44) decayed, 0.24 (± 0.74) extracted and 0.78 (± 1.24) teeth with fillings.
-
■
DMFT Index for the experimental group was 5.99 (± 3.62). On average, respondents had a 4.65 (± 3.93) decayed, 0.15 (± 0.6) of extracted and 1.19 (± 1.76) teeth with filling (Figure 1).
Figure 1.
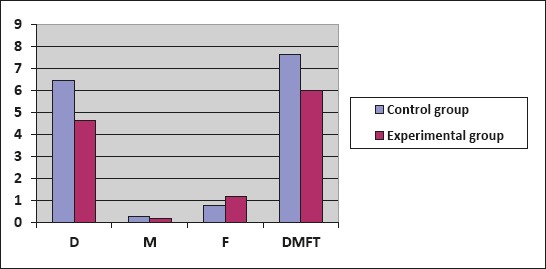
Overview of D, M, F and DMFT percentage value for the control and experimental group
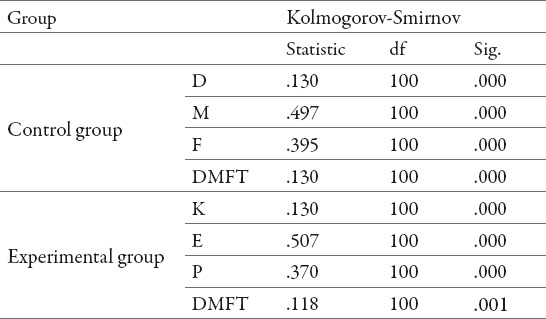
Testing of normal distribution D, M, F, DMFT is performed by Kolmogorov-Smirnov test. All studied variables showed a significant deviation from the normal distribution, the level of significance p = 0.000, except for DMFT index for the experimental group, p = 0.001. (Table 1.)
Table 1.
D, M, F, DMFT–results of normality distribution
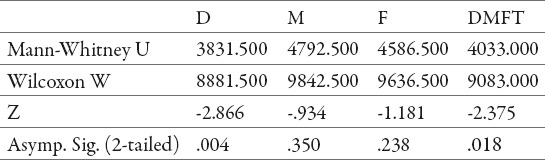
Significance of differences testing between the control and experimental groups for DMFT index and its components D, M and F is carried by the nonparametric Mann-Whitney test for independent samples (Table 2)
Table 2.
Results of the Mann-Whitney of the differences between the control and experimental groups for DMFT index and its components D, M and F
On the basis of the Mann-Whitney test it can be seen that:
-
■
There are no significant differences in the values of the M component (p = 0.350) and F component (p = 0.238) between the control and experimental groups.
-
■
There is a significant difference in the number of decayed (component D) teeth between the control and experimental groups (p = 0.004). Those in the control group had significantly more carious teeth than subjects in the experimental group. The average number of decayed teeth in the control group was 6.46 and in the experimental 4.65.
-
■
There is a significant difference in the DMFT values between the control and experimental groups (p = 0.004). Those in the control group had significantly higher DMFT index than subjects in the experimental group. The average DMFT values in the control group was 7.46 and in the experimental 5.99.
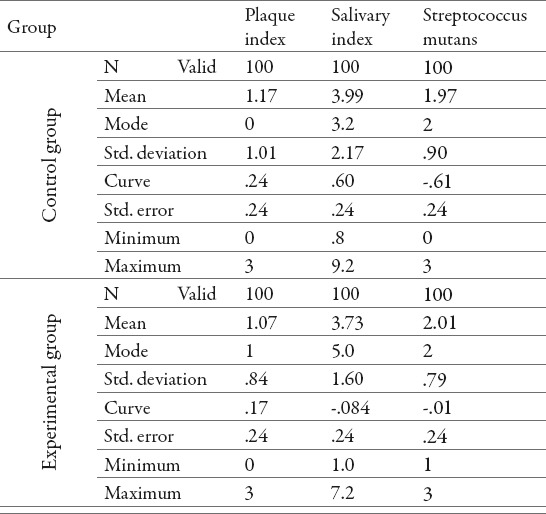
Results of descriptive statistics for plaque index, salivary index and mutans streptococcus level:
-
■
In the control group, subjects usually have very good oral hygiene (Mode for plaque index = 0), while the level of mutans streptococcus’s usually shows high values (Mode = 2). The average value of salivary index was 3.2 (± 2.17). All values show a positive curvature, except Streptococcus mutans levels, which shows a negative asymmetric distribution.
-
■
In the experimental group, respondents usually have good oral hygiene (Mode of plaque index = 1) while Streptococcus mutans level usually shows high values (Mode = 2). The average value of salivary index was 3.73 (± 1.60). Plaque index shows a positive curvature, while Streptococcus mutans levels and salivary index have a negative asymmetric distribution (Table 3).
Table 3.
Descriptive statistics for plaque index, the level of mutans streptococcus and salivary index for the control and experimental group
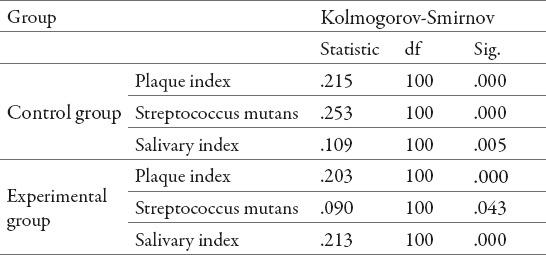
Testing of distribution normality of all the variables is performed by the Kolmogorov-Smirnov test. All variables tested showed a significant deviation from the normal distribution (level of significance of p = 0.000), except for the index of salivary control group (p = 0.005) and the experimental group (p = 0.043) (Table 4).
Table 4.
Testing of distribution of normality for plaque index, gingival index, salivary index and the level of Streptococcus mutans
Testing the significance of differences between the control and experimental groups for plaque index, the level of Streptococcus mutans and salivary index, due to the deviation from the normal distribution, for each of the individual variables was performed with nonparametric Mann-Whitney test for independent samples (Table 5).
Table 5.
Results of the Mann-Whitney comparison of the difference between the control and experimental groups: plaque index, Streptococcus mutans levels and salivary index.
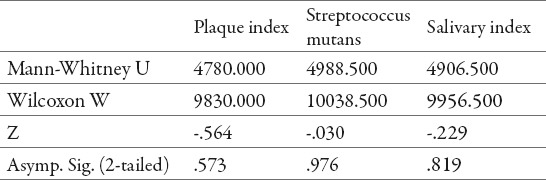
Based on the results of the Mann-Whitney test it is determined that there were no significant differences in the values of plaque index, salivary index and streptococcus mutans level between the control and experimental groups (p> 0.05 for each of the examined variables).
6. DISCUSSION
In the control group 26% of respondents have low and very low (score 1 and 0) Streptococci mutans levels, and 74% of respondents have high and very high levels (score 2 and 3).
In the experimental group, 31% of respondents have a low Streptococcus mutans levels (score 1) and 69% of respondents have high and very high levels (score 2 and 3).
Based on the Mann-Whitney test results it is revealed that there was no statistically significant difference in the Streptococcus mutans level between the control and experimental groups (p> 0.05). Due to the fact that in this study has not been proven statistically significant reduction in salivary index, therefore no reduced biosynthesis of biologically active components such as total protein, amylase, hexosamine, lysozyme, secretory IgA and salivary peroxidase could caused the increased concentration of Streptococcus mutans at subjects suffering from asthma. But both in the control and experimental group is demonstrated high level of Streptococcus mutans without statistically significant differences.
Streptococcus mutans streptococci are considered the predominant pathogens in pathogenesis of dental caries and in individuals with high concentrations of these bacteria should be an increased risk of caries. This is the case only in young children, where early colonization of tooth surfaces with this pathogen is an indicator of later high DMFT index of primary teeth. (17). But it became clear that when older children are concerned caries risk cannot be assumed on the basis of colonization of tooth surfaces with Streptococcus mutans (18, 19, 20).
This opinion is confirmed by our research, because the obtained results on this issue are contradictory. The majority of respondents, both from the control and experimental group have low values of plaque index and the high level of Streptococcus mutans on the one hand, and on the other hand, many respondents have decayed teeth and have high concentrations of Streptococcus mutans, which once again points to the multifactorial etiology of dental caries. Streptococcus mutans intracellular polysaccharides produced from glucose (21) contributing to their virulence because it can be stored and are then fermented in conditions of deficiency of exogenous origin of polysaccharide (22). This fact could explain the high concentration of Streptococcus mutans in patients with plaque index 0 or 1.
7. CONCLUSION
Due to the fact that inhalation antiasthmatic drugs belong to the group of medicines with xerostomic action, asthma is one of the chronic systemic diseases that increase the risk of caries and threaten oral health. But treatment with IAD is in most cases intermittent and apparently has no negative cumulative effect which would cause permanent change in salivary glands and thus disrupting the balance of oral micro flora that would favored growth of Streptococcus mutans and thus increased the incidence of caries in these children.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Shashikiran ND, Reddy VVS, Krishnam RP. Effect of antiasthmatic medication on dental disease: Dental caries and periodontal disease. J Indian Soc Pedod Prev Dent. 2007 doi: 10.4103/0970-4388.33450. [DOI] [PubMed] [Google Scholar]
- 2.Shulman JD, Taylor SE, Nunn ME. The association between asthma and dental caries in children and adolescents: A population-based case-control study. Caries Res. 2001;35(4):240–246. doi: 10.1159/000047464. [DOI] [PubMed] [Google Scholar]
- 3.Wogelius P, Poulsen S, Sorensen HT. Use of asthma-drugs and risk of dental caries among 5 to 7 year old Danish children: a cohort study. Community Dent Health. 2004;21(3):207–211. [PubMed] [Google Scholar]
- 4.Lenander-Lumikari M, Laurikainen K, Kuusisto P. Stimulated salivary flow rate and composition in asthmatic and non-asthmatic adults. Archives of Oral Biology. 1998;43:151–156. doi: 10.1016/s0003-9969(97)00110-6. [DOI] [PubMed] [Google Scholar]
- 5.Hegde PP, Ashok Kumar BR, Ankola VA. Dental caries experience and salivary levels of Streptococcus mutans and Lactobacilli in 13-15 years old children of Belgaum city, Arnataka. J Indian Soc Pedod Prev Dent. 2005;23(1):23–26. doi: 10.4103/0970-4388.16022. [DOI] [PubMed] [Google Scholar]
- 6.Khalilzadeh S, Jamshid S, Farzaneh S. Dental Caries-Associated Microorganisms in Asthmatic Children. Tanaffos. 2007;6(4):42–46. [Google Scholar]
- 7.Kuramitsu HK. Virulence factors of mutans streptococci: role of molecular genetics. Crit Rev Oral Biol and Med. 1993;4:159–176. doi: 10.1177/10454411930040020201. [DOI] [PubMed] [Google Scholar]
- 8.Gregory RL, Gfell LE, Malmstrom HS. Differences in secretory IgA and serum antibodies to Streptococcus mutans isolated from caries -resistant and caries -susceptible subjects. Adv Exp Med Biol. 1995;37(1B):1149–1152. [PubMed] [Google Scholar]
- 9.Ryberg M, Moller C, Ericson T. Saliva composition and caries development in asthmatic patients treated with β2 adrenoceptor agonists: A 4 year follow up study. Scand J Dent Res. 1991;99:212–218. doi: 10.1111/j.1600-0722.1991.tb01887.x. [DOI] [PubMed] [Google Scholar]
- 10.Marcotte H, Lavoie MC. Oral Microbial Ecology and the Role of Salivary Immunoglobulin A. Microbiol Mol Biol Rev. 1998;62(1):71–109. doi: 10.1128/mmbr.62.1.71-109.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gregory RL, Kindle JC, Hobbs LC, Filler SJ, Malmstrom HS. Function of anti-Streptococcus mutans antibodies: inhibition of virulence factors and enzyme neutralization. Oral Microbiol Immunol. 1990;5:181–188. doi: 10.1111/j.1399-302x.1990.tb00643.x. [DOI] [PubMed] [Google Scholar]
- 12.Gregory RL, Hobbs LC, Kindle JC, VanTo T, Malmstrom HS. Immunodominant antigens of Streptococcus mutans in dental caries- resistant subjects. Hum Antibodies Hybridomas. 1990;1(3):132–136. [PubMed] [Google Scholar]
- 13.Michalek SM, Childers NK. Development and outlook for a caries vaccinee. Crit Rev Oral Biol Med. 1990;1:37–54. doi: 10.1177/10454411900010010401. [DOI] [PubMed] [Google Scholar]
- 14.Marcotte H, Lavoie MC. Oral Microbial Ecology and the Role of Salivary Immunoglobulin A. Microbiol Mol Biol Rev. 1998;62(1):71–109. doi: 10.1128/mmbr.62.1.71-109.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Camling E, Gahnberg L, Krasse B. The relationship between IgA antibodes to Streptococcus mutans antigen in human saliva and breast milk and the numbers of indigenous oral S. mutans. Arch Oral Biol. 1987;32:21–25. doi: 10.1016/0003-9969(87)90149-x. [DOI] [PubMed] [Google Scholar]
- 16.Silness J, Loe H. Periodontal disease in pregnancy, correlation between oral hygiene and periodontal condition. Acta Odont Scand. 1964;22:121. doi: 10.3109/00016356408993968. [DOI] [PubMed] [Google Scholar]
- 17.Alaluusua S, Renkonen OV. Streptococcus mutans establishment and dental caries experience in children from 2 to 4 years old. Scand J Dent Res. 1983 Dec;91(6):453–457. doi: 10.1111/j.1600-0722.1983.tb00845.x. [DOI] [PubMed] [Google Scholar]
- 18.Stecksén-Blicks C. Salivary counts of lactobacilli and Streptococcus mutans in caries prediction. Scand J Dent Res. 1985 Jun;93(3):204–212. doi: 10.1111/j.1600-0722.1985.tb01946.x. [DOI] [PubMed] [Google Scholar]
- 19.Alanen P, Hurskainen K, Isokangas P, Pietilä I, Levänen J, Saarni UM, Tiekso J. Clinician’s ability to identify caries risk subjects. Community Dent Oral Epidemiol. 1994 Apr;22(2):86–89. doi: 10.1111/j.1600-0528.1994.tb01578.x. [DOI] [PubMed] [Google Scholar]
- 20.Hausen H. Caries prediction - state of the art. Community Dent Oral Epidemiol. 1997 Feb;25(1):87–96. doi: 10.1111/j.1600-0528.1997.tb00904.x. [DOI] [PubMed] [Google Scholar]
- 21.Kuramitsu HK. Virulence factors of mutans streptococci: role of molecular genetics. Crit Rev Oral Biol and Med. 1993;4:159–176. doi: 10.1177/10454411930040020201. [DOI] [PubMed] [Google Scholar]
- 22.Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev. 1986;50:353–380. doi: 10.1128/mr.50.4.353-380.1986. [DOI] [PMC free article] [PubMed] [Google Scholar]