

Abstract
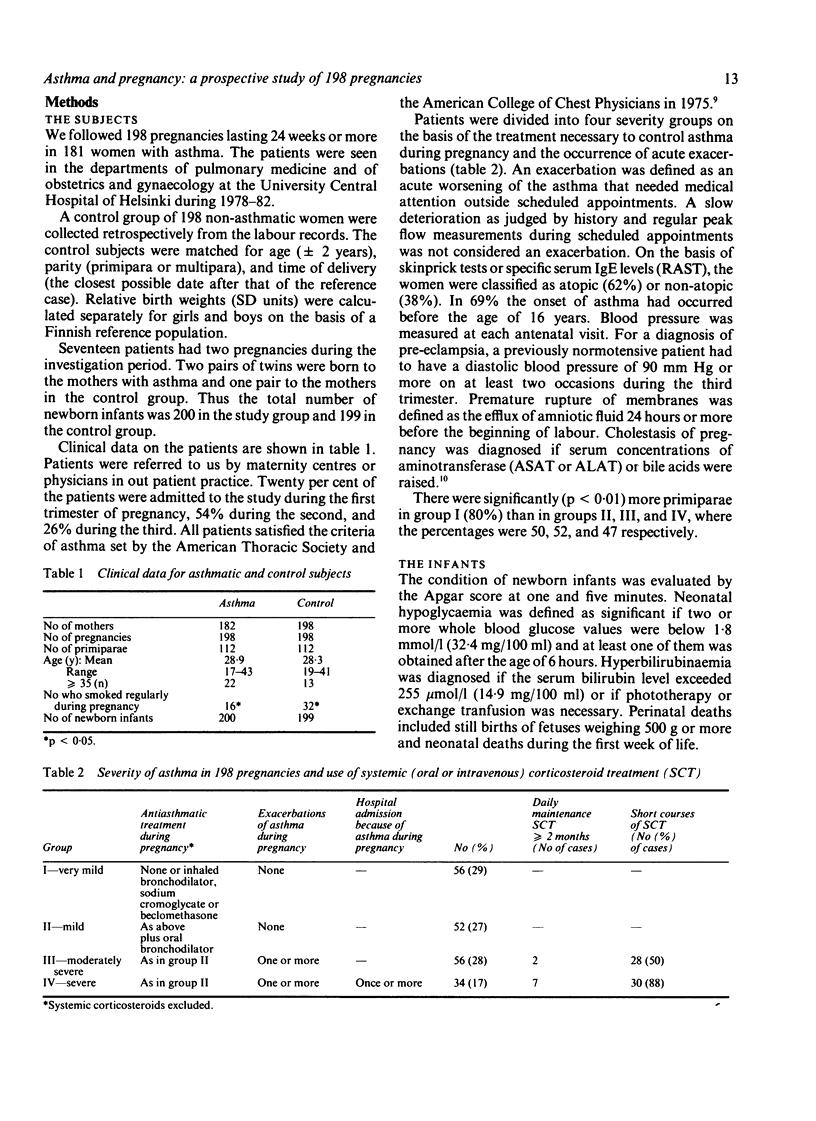
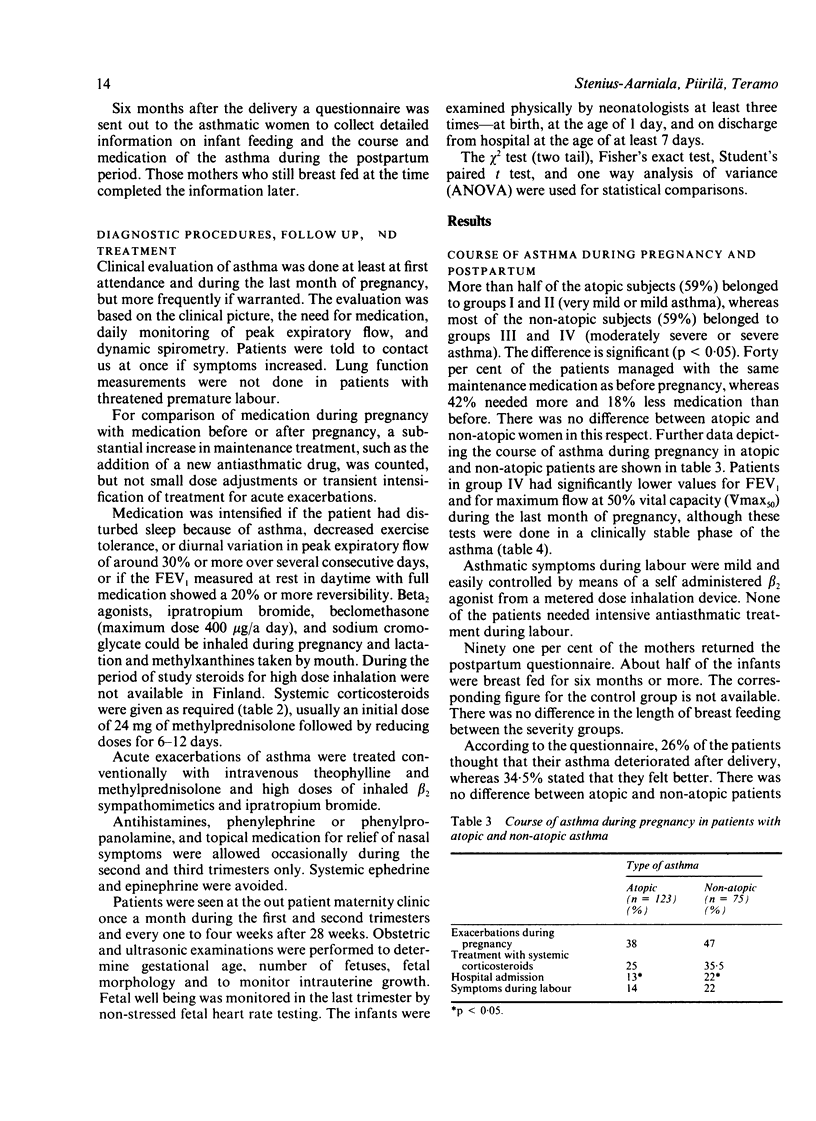
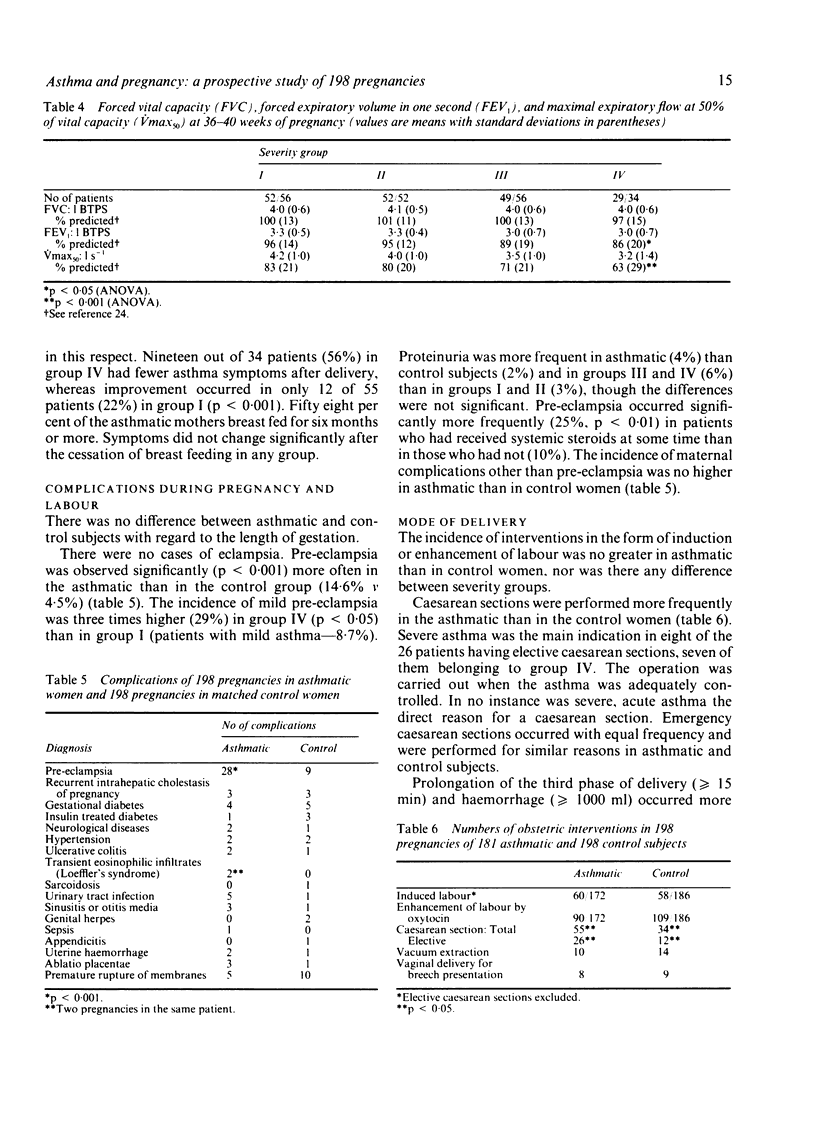
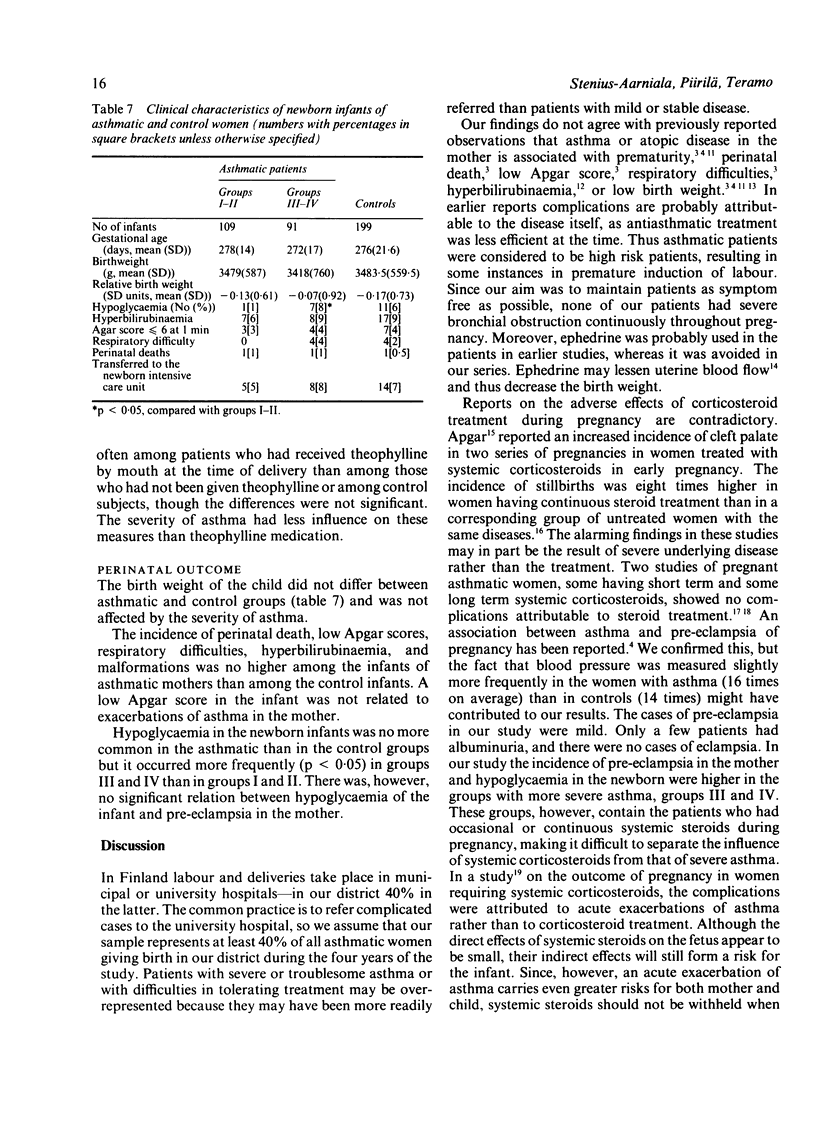
A study was designed to investigate whether asthma, when carefully managed, is associated with an increased risk of complications in connection with pregnancy. One hundred and eighty one asthmatic women were monitored during 198 pregnancies. Antiasthmatic treatment consisted of inhaled beta 2 adrenergic drugs, beclomethasone, sodium cromoglycate, oral theophylline, and systemic corticosteroids as needed. Postpartum information on asthmatic symptoms and infant feeding was collected by means of a questionnaire. A control group of 198 non-asthmatic pregnant women was matched for age and parity. Atopic women had less severe asthma than non-atopic women. During pregnancy 40% of the patients were managed with the same antiasthmatic medication as before pregnancy; 18% needed less and 42% more medication. Pre-eclampsia occurred more often in asthmatic than control subjects, especially in patients with severe asthma. Hypoglycaemia occurred more often in infants of mothers with severe asthma than in infants of mothers with less severe disease. Theophylline medication at term did not influence labour or delivery. Asthma caused no emergencies during labour. Among the asthmatic subjects 28% of babies were delivered by caesarean section compared with 17% in the control group. There was no difference between asthmatic and control subjects with regard to length of gestation, birth weight, incidence of perinatal deaths, low Apgar scores, neonatal respiratory difficulties, hyperbilirubinaemia, or malformations. It is concluded that severe asthma or systemic corticosteroid treatment (or both) during pregnancy seems to increase the incidence of mild pre-eclampsia in the mother and hypoglycaemia in the infant. The findings suggest that careful supervision of asthma during pregnancy and labour by obstetricians and chest physicians working in close collaboration should prevent most of the serious obstetric and neonatal complications of asthma in pregnancy reported by previous authors.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Apgar V. The drug problem in pregnancy. Clin Obstet Gynecol. 1966 Sep;9(3):623–630. doi: 10.1097/00003081-196609000-00004. [DOI] [PubMed] [Google Scholar]
- Bahna S. L., Bjerkedal T. The course and outcome of pregnancy in women with bronchial asthma. Acta Allergol. 1972 Dec;27(5):397–406. doi: 10.1111/j.1398-9995.1972.tb01439.x. [DOI] [PubMed] [Google Scholar]
- Chung K. F., Barnes P. J. Treatment of asthma. Br Med J (Clin Res Ed) 1987 Jan 10;294(6564):103–105. doi: 10.1136/bmj.294.6564.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dombrowski M. P., Bottoms S. F., Boike G. M., Wald J. Incidence of preeclampsia among asthmatic patients lower with theophylline. Am J Obstet Gynecol. 1986 Aug;155(2):265–267. doi: 10.1016/0002-9378(86)90804-5. [DOI] [PubMed] [Google Scholar]
- Fitzsimons R., Greenberger P. A., Patterson R. Outcome of pregnancy in women requiring corticosteroids for severe asthma. J Allergy Clin Immunol. 1986 Aug;78(2):349–353. doi: 10.1016/s0091-6749(86)80088-4. [DOI] [PubMed] [Google Scholar]
- Gluck J. C., Gluck P. The effects of pregnancy on asthma: a prospective study. Ann Allergy. 1976 Sep;37(3):164–168. [PubMed] [Google Scholar]
- Gordon M., Niswander K. R., Berendes H., Kantor A. G. Fetal morbidity following potentially anoxigenic obstetric conditions. VII. Bronchial asthma. Am J Obstet Gynecol. 1970 Feb 1;106(3):421–429. doi: 10.1016/0002-9378(70)90371-6. [DOI] [PubMed] [Google Scholar]
- Greenberger P. A., Patterson R. Beclomethasone diproprionate for severe asthma during pregnancy. Ann Intern Med. 1983 Apr;98(4):478–480. doi: 10.7326/0003-4819-98-4-478. [DOI] [PubMed] [Google Scholar]
- HIDDLESTONE H. J. BRONCHIAL ASTHMA AND PREGNANCY. N Z Med J. 1964 Aug;63:521–523. [PubMed] [Google Scholar]
- Laatikainen T., Ikonen E. Serum bile acids in cholestasis of pregnancy. Obstet Gynecol. 1977 Sep;50(3):313–318. [PubMed] [Google Scholar]
- Ralston D. H., Shnider S. M., DeLorimier A. A. Effects of equipotent ephedrine, metaraminol, mephentermine, and methoxamine on uterine blood flow in the pregnant ewe. Anesthesiology. 1974 Apr;40(4):354–370. doi: 10.1097/00000542-197404000-00009. [DOI] [PubMed] [Google Scholar]
- Schatz M., Patterson R., Zeitz S., O'Rourke J., Melam H. Corticosteroid therapy for the pregnant asthmatic patient. JAMA. 1975 Aug 18;233(7):804–807. [PubMed] [Google Scholar]
- Sims C. D., Chamberlain G. V., de Swiet M. Lung function tests in bronchial asthma during and after pregnancy. Br J Obstet Gynaecol. 1976 Jun;83(6):434–437. doi: 10.1111/j.1471-0528.1976.tb00860.x. [DOI] [PubMed] [Google Scholar]
- Spector S. L. The treatment of the asthmatic mother during pregnancy and lactation. Ann Allergy. 1983 Aug;51(2 Pt 1):173–178. [PubMed] [Google Scholar]
- Viljanen A. A., Halttunen P. K., Kreus K. E., Viljanen B. C. Spirometric studies in non-smoking, healthy adults. Scand J Clin Lab Invest Suppl. 1982;159:5–20. [PubMed] [Google Scholar]
- Walsh S. D., Clark F. R. Pregnancy in patients on long-term corticosteroid therapy. Scott Med J. 1967 Sep;12(9):302–306. doi: 10.1177/003693306701200902. [DOI] [PubMed] [Google Scholar]
- Warrell D. W., Taylor R. Outcome for the foetus of mothers receiving prednisolone during pregnancy. Lancet. 1968 Jan 20;1(7534):117–118. doi: 10.1016/s0140-6736(68)92723-2. [DOI] [PubMed] [Google Scholar]