

Abstract
This article presents a narrative review of cystic lesions around the hip and primarily consists of 5 sections: Radiological examination, prevalence, pathogenesis, symptoms, and treatment. Cystic lesions around the hip are usually asymptomatic but may be observed incidentally on imaging examinations, such as computed tomography and magnetic resonance imaging. Some cysts may enlarge because of various pathological factors, such as trauma, osteoarthritis, rheumatoid arthritis, or total hip arthroplasty (THA), and may become symptomatic because of compression of surrounding structures, including the femoral, obturator, or sciatic nerves, external iliac or common femoral artery, femoral or external iliac vein, sigmoid colon, cecum, small bowel, ureters, and bladder. Treatment for symptomatic cystic lesions around the hip joint includes rest, nonsteroidal anti-inflammatory drug administration, needle aspiration, and surgical excision. Furthermore, when these cysts are associated with osteoarthritis, rheumatoid arthritis, and THA, primary or revision THA surgery will be necessary concurrent with cyst excision. Knowledge of the characteristic clinical appearance of cystic masses around the hip will be useful for determining specific diagnoses and treatments.
Keywords: Bursa, Cystic lesion, Ganglion cyst, Hip, Synovial cyst
Core tip: The purpose of the present paper is to review clinical features of cystic lesions around the hip joint. Ultrasound, computed tomography and magnetic resonance imaging are useful modalities for detection of cystic lesions, but it is difficult to distinguish pathological differences between ganglion cysts and synovial cysts, including bursae. Although cysts around the hip are usually asymptomatic, enlargement of these cysts may cause pain and/or compression of the surrounding structures, such as nerves and vessels. Treatment of these cysts depends on their size, the severity of symptoms, and the nature of the underlying disease.
INTRODUCTION
Cystic lesions may occur around any of the joints or tendon sheaths in the body. Common locations of the cyst include the wrist, hand, foot, ankle, and knee, because it could be much easier to identify cysts near the body surface. Development of cysts associated with the hip joint is a rare clinical problem, but they may be incidentally observed on clinical inspection or imaging examinations, such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI)[1]. Some researchers have examined the frequency of cysts in the hips of asymptomatic volunteers using MRI. Their results indicated that 5.8%-26.2% of asymptomatic hips had a cyst around the joint. In general, 15 synovial-lined bursae around the hip joint have been commonly imaged, particularly the iliopsoas bursa, which is the largest synovial bursa in the body and present bilaterally in 98% of adults[2]. In addition, herniation of the synovium into the surrounding tissue, displacement of the synovium in the embryonal stage, and degeneration of connective tissue in an adjacent joint or a tendon sheath have been suggested as possible etiological factors[3,4]. Histologically, there are 2 types of cysts around the joint or tendon: ganglion and synovial cysts. Ganglion cysts are generally believed to be the result of myxomatous degeneration of certain fibrous tissue structures and do not have a lining of synovial cells, whereas synovial cysts, including bursa, have a lining of synovial cells and sometimes directly communicate with the adjacent joint. Both ganglion and synovial cysts contain a similar gelatinous fluid that is highly viscous secondary to the presence of hyaluronic acid and other mucopolysaccharides or hemorrhage[3]. It is difficult to differentiate these cysts by clinical and radiological examinations or determine if the cysts communicate with the joint cavity. Accordingly, we primarily use the term “cyst or cystic lesion” when referring to bursae, synovial cysts, and ganglion cysts in this review because they have the same appearance radiologically. Cystic lesions around the hip are usually asymptomatic but may cause pain and compression of the surrounding nerves, veins, and arteries when they become enlarged. This narrative review article includes 5 main sections: Radiological examination, prevalence, pathogenesis, symptoms, and treatment for cystic lesions of the hip joint. For this review, we searched the key words “hip cyst” or “hip ganglion” or “hip bursa” using PubMed (National Library of Medicine, Bethesda, Maryland, United States) to obtain the articles published until December 2014. 1056 articles from the key word “hip cyst”, 134 from “hip ganglion”, and 239 from “hip bursa” were matched, respectively. All selected abstracts or articles were reviewed by the authors and articles without an English abstract that were not published in English were excluded. As a result searched with PubMed, total 151 articles were considered to be relevant for this review. Furthermore, we added the 140 related articles using the references of the articles, which is selected by PubMed, and finally 291 articles about cystic lesion around the hip were collected. The objective of the present article is to provide an overview of the clinical features of cystic lesions around the hip joint.
RADIOLOGICAL EXAMINATIONS
Conventional radiographs are useful for showing underlying hip joint disorders, such as osteoarthritis, rheumatoid arthritis, and acetabular dysplasia, but cannot detect cystic lesions[5-17]. Arthrography or cystography (bursography) can be used to demonstrate localization, size, and communication with the hip joint of cysts[9,12-15,18-33]. However, communication between cysts and the hip joint may not be demonstrated when the communication is very narrow or the root has a check valve mechanism[31]. Ultrasonography is a useful and noninvasive imaging modality for demonstrating the fluid-filled nature of a palpable mass. Cystic lesions can appear as hypoechoic areas on ultrasound examinations[12,15,16,34-47]. This modality may be used to guide needle aspirations and/or drug injections[34,48,49]. In contrast, ultrasonography does not show subtle sites of joint communication and has a limited ability to evaluate associated intra-articular abnormalities. CT scan is an excellent tool for assessing abnormalities of calcified tissues because of its high spatial resolution[8,9,11,12,16,19,25,26,35,50-58]. Cysts have lower attenuation than muscle and higher attenuation than fat. Rim enhancement may be observed after administration of intravenous contrast[26,59]. Similar to ultrasonography, CT can be used to guide needle aspiration of cysts[26,60]. MRI is superior to all other imaging modalities for investigating soft tissue abnormalities, particularly for demonstrating the exact location and extent of lesions around the cyst[6,9-11,16,17,27,37,40,41,52,56,61-75]. This technique offers superior soft tissue contrast and multiplanar capabilities and is noninvasive. Imaging can depict round or ovoid cystic masses with intermediate to low signal intensities on T1-weighted images and high signal on T2-weighed images. Detection of cystic lesions is much easier on fat-suppression T2-weighed or short tau inversion recovery images. MRI with intravenous administration of the contrast agent, Gd-DTPA, on T1-weighted imaging may show rim enhancement and is more useful for diagnosing synovial cysts because synovial proliferations exhibit rapid and marked increases in signal intensity[9,16,61,67,68,76]. However, after contrast agent injection, no enhancement of the cyst may be evident, even for synovial cysts[61]. In addition, MRI is very accurate in depicting associated joint disorders, such as acetabular labral tears and degenerative or inflammatory changes[4]. MR arthrography can show in detail the relationship of a lesion to a joint and the surrounding structures[77].
PREVALENCE
Most reports concerning cystic lesions around the hip joints have been single case reports, but O’Cooner[78] stated that the true incidence is probably higher than that indicated by infrequent cases in 1933. We found 3 reports on the prevalence of cysts in asymptomatic hips on MRI. In 1998, Cotten et al[79] first reported the MR appearance of the hip labrum in asymptomatic volunteers. They described that intralabral cysts were observed in 3 labra of 52 hips (5.8%). Recently, other studies have shown a high rate of cysts around the hip. Schmitz et al[80] described cystic lesions in 11 of 42 (26.2%) and 9 of 42 (21.4%) asymptomatic hips identified by 2 different radiologists. Register et al[81] reported that cysts were identified in 6 of 45 (13%) asymptomatic participants. These results indicate that detection of cysts around the hip joint is no longer an uncommon abnormal MRI finding and the increased sensitivity of MRI has enabled identification of these cysts.
PATHOGENESIS
There are pathologically some types of cystic lesions including ganglion cyst, synovial cyst, and bursa. Ganglion cysts histologically do not have a lining of synovial cells probably because of the result of myxomatous tissue degeneration[82]. While, synovial cysts have a lining of synovial cells because they may be caused by herniation of the synovium into the surrounding tissue or displacement of the synovium in the embryonal stage. However, the exact cause of these cysts is still unknown[12,26,61,83,84]. Bursae are fluid-filled sac lined by synovial membrane, which normally present and provide a cushion between bones and tendons and/or muscles. At least 15 synovial bursae have been described around the hip joint, including the trochanteric, iliopsoas, obturator, and ischial bursae[2,16,23,29,36,85-93] (Figure 1). The iliopsoas bursa is the largest synovial bursa in the body and is present bilaterally in 98% of adults[2] (Figure 2). This structure lies between the iliofemoral and pubofemoral ligaments, is adjacent to the thinnest and most vulnerable portion of the anterior capsule, and is the most problematic synovial bursa. In a cadaver study, Chandler found the communication between the iliopsoas bursa and the hip joint in only 14.25% (61 of 400) of adult cadavers and in as many as 40% of hips with osteoarthritis[11,14,56,94]. The iliopsoas bursitis was first reported by Fricke in 1834 according to Finder[95]. In 1887, Sprengel also reported a case of bursitis communicating with the hip joint, according to Gatch and Green[94]. Thus, it is believed that cysts that occur at the anterior of the hip could be inflammation and enlargement of the iliopsoas bursa itself or herniation of the anterior capsule caused by increased intra-articular pressure and an intrinsically weak capsule secondary to underlying inflammatory or degenerative joint disease[9,11,12,14,15,17,21-27,30,31,35,38-42,45,48,51,53,58,60,61,72,73,75,83,94,96-138]. On the other hand, a distended obturator bursa is believed to be formed by the protrusion of the posterior hip joint between the ischiofemoral capsular ligament and the zona orbicularis[85]. Trochanteric bursa is located at the lateral aspect of the greater trochanter of the femur[86-89]. An inflamed trochanteric bursa caused by various conditions is leading to pain in the lateral hip[70,139-159]. Anyways, it is difficult to distinguish isolated bursitis, pure articular synovial herniation without bursal involvement, or ganglion cysts on radiological or clinical examinations.
Figure 1.

A 58-year-old female with greater trochanteric bursitis. Coronal (A) and axial (B) T2-weighted magnetic resonance images of a cyst located at the characteristic position of the left greater trochanteric bursa (arrow). Arrowhead: Greater trochanter.
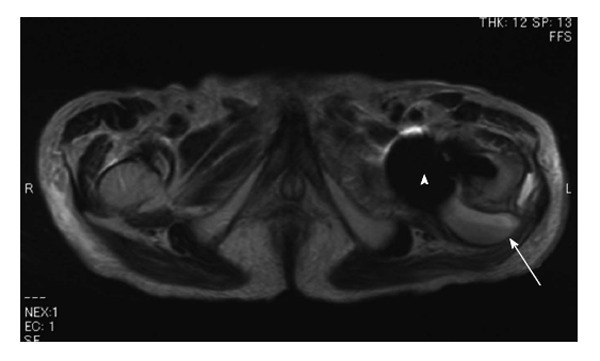
Figure 2.
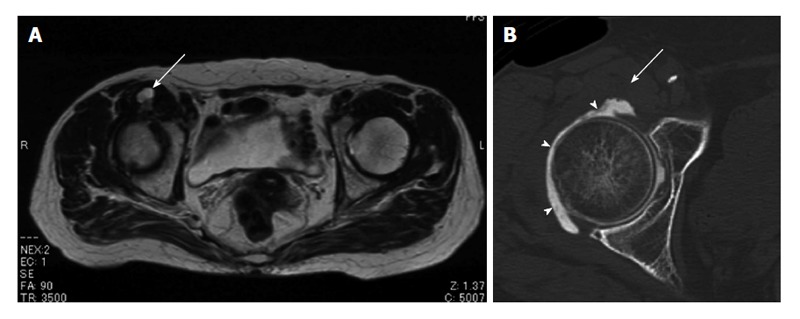
A 81-year-old female with femoral neuropathy caused by distended iliopsoas bursa. Axial T2-weighted magnetic resonance image shows a cystic lesion, which extends anteriorly into the iliopsoas muscle (A). Computed tomography arthrography demonstrates no communication between the cyst (arrow) and right hip joint (B). Arrowheads: Contrast material.
Cysts of the hip are usually accompanied by the following various hip disorders such as trauma, avascular necrosis of the femoral head, osteoarthritis, rheumatoid arthritis, and total hip arthroplasty (THA).
Surgical capsular release for hip contracture following a spinal injury
Anterior soft tissue release of the hip is a common procedure for contracture of this joint, particularly in patients with cerebral palsy or following spinal cord injury. There has been only 1 reported case of a cyst formation communicating with the hip joint after this procedure[66].
Avascular necrosis of the femoral head
Avascular necrosis of the femoral head is one of the pathogenesis of hip synovial cyst formation[17,27,62,112,160,161]. The necrosis and deformity of the femoral head lead to joint synovitis and result in osteoarthritis of the hip. Cohen et al[62] first reported iliopsoas bursitis associated with avascular necrosis of the femoral head in a 34-year-old female receiving steroid therapy for systemic lupus erythematosus. Yoon et al[27] reported a similar case involving femoral neuropathy. Plain radiographs show deformity of the femoral head and narrowing of the joint space, which results in osteoarthritis[27,56,62].
Trauma
Acute or chronic trauma and sports injuries have been mentioned as causative factors of cyst formation around the hip[5,12,26,94,97,162-165]. O’Conner[78] suggested that the trauma imparted to the iliopsoas bursa during vigorous hip flexion and extension was the most likely etiological mechanism[95].
Developmental dysplasia
Lin et al[10] reported a case of a 35-mo-old boy with a hip ganglion cyst secondary to a labral tear. He was treated with adductor tenotomy, closed reduction, and a hip spica for developmental dysplasia of the hip when he was 14-mo-old.
Labral tear
When cysts around the hip joint are adjacent to the joint capsule and/or the acetabular labrum on MRI, the cause of these cysts has been believed to be synovial fluid that is forced through the labral tear via a one-way valve mechanism[166]. This type of cyst is designated radiologically as a “paralabral or labral cyst[5,6,26,40,48,61-64,167]” (Figure 3). In 1989, Haller et al[5] first described the relationship between a cystic mass adjacent to the acetabulum and a labral tear. They illustrated that synovial tissue or fluid may extrude from the joint through the labral tear and lead to accumulation of fluid and cyst formation in the adjacent soft tissues as one factor in the pathogenesis of juxta-acetabular cysts. In 1994, Tirman et al[168] determined that a glenoid labral tear of the shoulder was associated with a cystic mass and termed the mass a “labral cyst”. The same group applied the term to similar cysts of the hip joint[6]. Schnarkowski et al[6] reported that of the 7 labral cysts, 5 were localized at the posterosuperior and 2 at the anterior. They described that the posterosuperior part of the labrum was the most vulnerable to mechanical stress and an easier site to detach by trauma, which could lead to cyst formation[169]. Furthermore, Magee et al[166] reported 10 patients who underwent surgery for labral cysts and had associated labral tears located in the area of the labral cyst. Seven of the tears occurred posteriorly and 3 occurred anteriorly. Recent reports of case series described that paralabral cysts were localized anterosuperiorly in 56% (10 of 18) of the patients, anteriorly in 22% (4 of 18), posterosuperiorly in 17% (3 of 18), anteroinferiorly in 6% (1 of 18), posteriorly in 0%, and posteroinferiorly in 0% on MR arthrographic analysis[77]. This result was consistent with the fact that most labral tears have occurred anterosuperiorly on evaluation by MR arthrography[170,171]. The labral cyst of the hip may be a predisposition to labral pathology. MR arthrography can increase the sensitivity and accuracy for detection of the associated labral tears. Recently, arthroscopic treatment for acetabular labral tear and paralabral cyst has been reported[63,172,173]. Tey et al[172] reported a case with acetabular labral tear and labral cyst caused by psoas impingement. In this case, the psoas tendon was released and the labral cyst was excised; reattachment of the labral tear was finally performed using a suture anchor. Kanauchi et al[173] also reported a combination treatment with arthroscopic labral repair and ultrasound-guided cyst aspiration for the acetabular paralabral cyst causing femoral nerve paresthesia. In contrast, Lee et al[63] described an arthroscopic treatment by cyst decompression and debridement of the degenerative labrum for labral cyst and tear. Thus, arthroscopic findings will be useful for further understanding of labral cysts.
Figure 3.
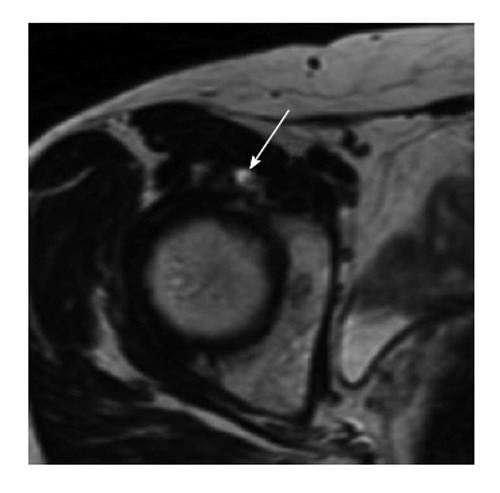
A 50-year-old female with a right hip pain. Axial T2-weighted magnetic resonance image shows a labral tear and paralabral cyst (arrow) at the anterior aspect of the right hip joint.
Osteoarthritis
Osteoarthritis is a degenerative joint disease, which causes joint pain and stiffness. More than 80% of all cases of idiopathic osteoarthritis of the hip joint may be because of subtle congenital or developmental defects, which increase joint incongruity and concentrate the dynamic load (Figure 4). Dynamic loads cause displacement of synovial fluid, which in turn may cause synovial cyst development[11,12,14,22,26,30,32,35,38,51,68,83,96,119,127,174-180].
Figure 4.
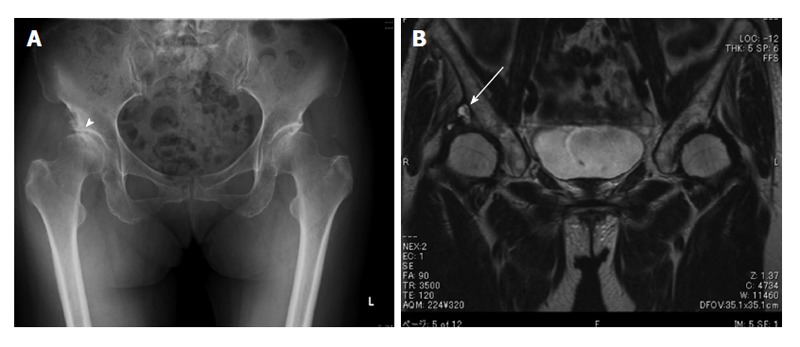
A 70-year-old female with a cystic lesion associated with osteoarthritis. Plain radiograph of the lower pelvis reveals the secondary osteoarthritis of right hip due to acetabular dysplasia (arrowhead) (A). Coronal T2-weighted magnetic resonance image shows a cystic mass (arrow) located superiorly, connected to the right hip joint (B).
Rapidly destructive arthrosis of the hip
Rapidly destructive hip disease (RDHD) is a rare entity that involves aggressive hip joint destruction within 6-12 mo of onset. Inflammatory arthritis is always caused by cartilage and bone destruction in such cases. Iliopsoas bursitis also has been seen in 2 reported RDHD cases[129,135].
Rheumatoid arthritis
Rheumatoid arthritis is an autoimmune disease that results in a chronic inflammatory response of the synovial joint capsule secondary to swelling due to excess synovial fluid and development of the synovium. The occurrence of synovial cyst of the hip in patients with rheumatoid arthritis has been reported[7,9,12,13,21,26,28,37,45,54,56,65,72,99-101,106,114,115,130,134,135,138,160,176,178,181-190].
Coventry et al[7] described 3 cases of rheumatoid synovial cysts of the hip. Two of 3 patients had edema of the extremities due to compression of the femoral vein caused by enlarged synovial cysts. They documented 3 theories regarding the etiology of rheumatoid synovial cyst formation. First, overproduction of synovial fluid in a rheumatoid cyst may increase the intra-articular pressure and distend the joint capsule. Second, the iliopsoas bursa, which is sometimes directly connected with the hip joint, may be involved in the rheumatoid process with formation of excessive quantities of fluid[12,24,33]. Third, necrosis of a subcutaneous periarticular rheumatoid nodule possibly could result in the formation of a juxta-articular cyst. However, the exact etiology of rheumatoid synovial cysts cannot be determined. Although some similar cases of rheumatoid cysts have been reported following Coventry’s cases[9,13,21,65], interestingly, all of the rheumatoid arthritis-associated cysts in the reported cases were localized anteriorly. This finding suggests that the iliopsoas bursa is involved in cyst formation associated with rheumatoid arthritis.
Juvenile idiopathic arthritis
Juvenile idiopathic arthritis (JIA) is an autoimmune arthritis in children less than 16 years of age. Iversen et al[41] described about the enlargement of the iliopsoas bursae communicated with the hips in a JIA patient.
Polymyalgia rheumatica
Polymyalgia rheumatica (PMR) is an inflammatory disorder that causes pain and stiffness in the neck, shoulder and pelvic girdle. Tani et al[128] reported a case of enlargement of iliopsoas bursa due to PMR.
Hip arthroplasty
In 1984, Kolmert et al[25] first reported 2 cases of cyst formation after THA. Moreover, some case reports have been published about cystic lesions after joint replacement[8,19,20,31,50,53,64,71,83,109,123,126,132,191-231]. Initially, these cysts were believed to be subclinical infections, but currently they are called “granulomatous pseudotumor” resulting from polyethylene, metal, or cement wear debris, which is phagocytosed by inflammatory cells and macrophages that cause a foreign body reaction[8,20,31,53,64,196,197,199-201,203-205,208,212,213,215,220-222] (Figure 5). On the other hand, some cysts may be distended iliopsoas bursitis as a tissue response to wear debris, but not newly formed granuloma[31,50,126,132,136,137,195,198,232].
Figure 5.
A 76-year-old male with a pseudotumor following cemented total hip arthroplasty, which was implanted 18 years earlier. Coronal short tau inversion recovery magnetic resonance image shows a cystic lesion (arrow) adjacent to the acetabular component (arrowhead).
In 2005, Willert et al[214] first described the development of an inflammatory synovial reaction as a novel complication associated with metal-on-metal (MoM)-bearing hip replacements[211,214]. A distinct histological pattern is observed and characterized by diffuse perivascular infiltrates of T and B lymphocytes, high endothelial venules, fibrin exudation, eosinophils, and necrosis. It is thought to be a variation of a type IV delayed hypersensitivity and has been termed an aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL). Adverse reactions to metal debris, including ALVAL and pseudotumor formation, should be considered as a diagnosis in any patient with unexplained groin pain or a mass following a MoM THA[137,203,216,217,223,224,233-238]. In general, patients with pseudotumors may be asymptomatic[193,207,208] or present with mild groin pain[20,196,201,213,220]. If the expansive lesions are intrapelvic, they may compress the adjacent structures, including the ureters[212], intestines[218], vessels[50,137,192,195,198,199,203,220,222,223], and nerves[8,19,53,64,210,216,217,224]. Compared with cystic lesions, solid lesions can more easily cause femoral palsy and revision THA[217]. Cystic lesions associated with THA can be one of the signals for implant failure or loosening.
Others
Gas-containing cysts of the hip have been reported infrequently. Gas may be seen on conventional plain radiography, linear tomography, or CT[239]. This gas may be difficult to differentiate from overlying bowel gas and other causes of gas within soft tissues[240]. Gas may be present inside distended iliopsoas bursae because of a gas-pumping mechanism, which may lead to a misdiagnosis. Silver et al[239] reported 3 cases of gas-containing ganglia arising from the hip joints with advanced osteoarthritis. Haller et al[5] also reported that gas was demonstrated in 4 cystic lesions around the hip joint associated with degenerative hip disease.
It should be noted that a cystic mass around the hip may not be a synovial or ganglion cyst but may originate from the adventitia of the common femoral artery or vein. The latter has been called “adventitial cystic disease”, which is an uncommon type of nonatherosclerotic peripheral vessel disease and is characterized by accumulation of a mucinous substance in the adventitia[241-244]. These substances cause symptoms of intermittent claudication or leg swelling because of obstruction of arteries or veins.
The differential diagnosis of a mass in the inguinal region includes various conditions, such as pigmented villonodular synovitis[245,246], synovial chondromatosis[93,108,247,248], arterial aneurisms, femoral hernias[249,250], inguinal lymphadenopathy, and abscess[25,33,40,60,70,90,120,140,142,145,149,151,153,154,156,181,229] (Figure 6). Careful clinical and radiological examinations will help confirm or exclude a diagnosis.
Figure 6.
A 93-year-old male with an infection after hemiarthroplasty for the left femoral neck fracture. Axial T2-weighted image reveals a cystic lesion with a fluid-fluid level (arrow) adjacent to the posterior aspect of the endoprosthesis (arrowhead).
SYMPTOMS
Cysts around the hip joint are often asymptomatic[10,11,54] (Figure 7). When cysts impinge upon nerves or vessels, they may become symptomatic.
Figure 7.

A 71-year-old female with the left femoral neck fracture. Coronal T2-weighted magnetic resonance image shows an asymptomatic multilocular cystic mass (arrow), which is communicated with the right hip joint.
Pain and/or swelling
Although pain is not a universal feature, it is frequently the earliest and may be the only cyst symptom, which may include bursitis[9-11,13-15,20,25,31,32,43,56,61,63,65,74,111,113,114,118,122,141,144,174,175,196,201,213,220,228,251-253]. An inguinal mass and groin or thigh pain usually comprise the clinical presentation in some patients. Akman et al[252] reported a case of a hip ganglion presenting with symptoms of right-sided groin pain. A larger mass caused nocturnal femoral pain[254]. Inguinal swelling also has been reported as another rare presentation of a hip cyst when the cysts grow anteriorly[43,116,118,255,256] or posteriorly[257]. A soft mass over the femoral triangle could be misdiagnosed as a femoral hernia[249,250].
Snapping
Iliopsoas bursitis is often associated with the snapping hip syndrome[24,29,48,49,121,143]. The snapping hip syndrome involves the iliopsoas tendon snapping over the iliopectineal eminence and the anterior hip capsule or a lesser trochanteric bony prominence. Harper et al[24] reported 2 cases with a painful audible snapping hip. In literature, the snapping was reproduced voluntarily by extending the flexed, abducted, and externally rotated hip, and iliopsoas bursography was a useful technique for diagnosis of this syndrome. Snapping could disappear by release of the tendinous portion in these cases[21,29,49,121].
Peripheral nerve compression
Femoral nerve: Approximately 20 cases about femoral nerve compression due to a cystic lesion around the hip joint have been described in literature[8,17,27,35,52,53,55,66,68,73,112,130,134,138,173,189,254,258-260]. The symptoms were described as radicular pain caused by compression of the femoral nerve and by hypoesthesia and/or paresthesia in the groin radiating down to the medial thigh, the anterior aspect of the knee, and the medial side of the lower leg and foot. Some patients complained of their inability to climb stairs and walking because of hip pain and muscle weakness. These symptoms mimic L2-4 radiculopathy with lumbar disorders, such as lumbar disc herniation and lumbar spinal canal stenosis[68,258]. Physical examination may reveal tenderness over the anterior hip, limited range of motion of the affected hip joint, sensory disturbance of the femoral nerve area, and atrophy of the thigh. The iliopsoas and quadriceps femoris muscle may be weak[27,35], accompanied by diminished patellar tendon reflexes[8,35,53]. The hip is held in flexion with some adduction and external rotation. Pain is elicited by hyperextending, abducting, or internally rotating the hip. On radiological examinations, radiography of the pelvis may show severe degenerative hip disease, which causes iliopsoas bursitis in some cases[17,27,35,68,112,130,134,189]. The cysts with femoral nerve compression are always located in the anterior hip and are mostly synovial cysts because of the relationship with the iliopsoas bursa (Figure 2). On the other hand, although rare, a few cases with femoral nerve compression caused by ganglion cyst have been reported[52,259]. Recently, a few reports have described wear debris from THA that produced a clinically detectable mass that could provoke delayed femoral nerve palsy[8,53,173,217,261], although some cases had solid pseudotumors but not cystic lesions.
Obturator nerve: Obturator neuropathy can be caused by various conditions, such as pelvic fracture, THA, or obturator hernia, but obturator nerve compression by a cyst is extremely rare. Only 4 cases have been reported[34,68,262,263]. In 2002, Campeas et al[262] first reported a case with obturator neuropathy caused by a ganglion cyst arising from the hip joint. In 2005, Yukata et al[34] presented a case with obturator neuropathy caused by a cyst associated with an anterior acetabular labral tear and its detailed MRI findings. Stuplich et al[68] also reported a case with combined femoral and obturator neuropathy caused by synovial cyst from moderate arthrosis of the hip. The main symptom of obturator nerve compression is pain in the right groin and anteromedial thigh[34]. The tenderness occurs over the adductor muscles, and Patrick’s sign (hip flexion, abduction, external rotation, extension position) may be positive and passive straight leg raising test is negative. The weakness of hip adductors due to pain and the absence of the adductor reflex could have been detected[68]. MRI of the pelvis has shown a cystic lesion at the medial aspect of the right acetabulum with its stalk continuing to the anterior labral tear[34] or extending into the obturator muscles toward the obturator nerve[68] (Figure 8). Further, the muscles of the obturator nerve area may show atrophy and increased signal intensity on T2-weighed images, which indicates denervation[34,263].
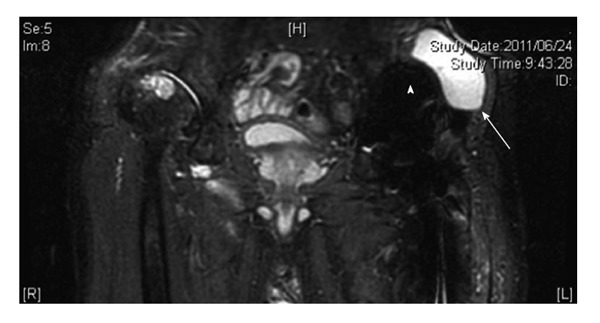
Figure 8.
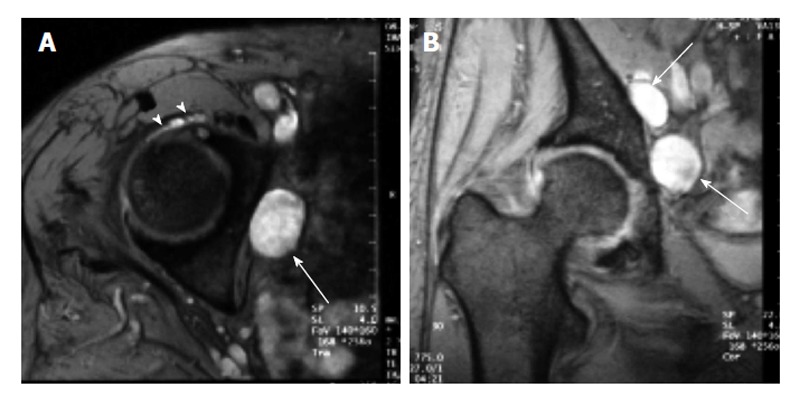
A 75-year-old female with obturator neuropathy. Axial (A) and coronal (B) short tau inversion recovery magnetic resonance images show that the location of the cystic masses (arrows) is consistent with the site of obturator nerve (Ref: [26]). The stalk of the cyst was connected to the anterior joint capsule (arrowheads).
Sciatic nerve: Sciatic neuropathy has been reported secondary to a cystic lesion around the hip joint[19,64,67,69,264-268]. In 1991, Juglard et al[264] first reported a case with sciatic nerve compression by a cystic lesion. In addition, some similar cases have been reported until 2014[67,69,265-267,269]. These patients presented with increasing buttock pain radiating downward to the posterior thigh and knee and the lateral aspect of the lower leg and sole, which is the so-called sciatica. The patient may have a paresthesia of the lateral calf and sole. Physical examination may reveal no sensory disturbance or muscle weakness of the lower leg, and the hip range of movement is full or mildly limited. Tenderness may be over the posterior hip. The straight leg raising test was negative in all reported cases, but the pain around the hip was elicited by hip rotations[67,69]. MRI clearly showed a cystic mass in the sciatic notch or extending posteriorly to the femur intertrochanteric lesion. Histological evaluation of these cysts demonstrated that the cyst wall was composed of variably dense fibroconnective tissue with no lining cells, which suggests a ganglion cyst[67,69,264,267,268], while the recent case reported by Salunke et al[265] was histologically diagnosed as a synovial cyst. Sciatic neuropathy as a late complication is sometimes caused by a cystic formation due to polyethylene or titanium wear debris after THA[19,64,206]. Fischer et al[19] first described a patient with sciatic neuropathy following compression caused by an intrapelvic synovial cyst that formed in response to wear debris. Crawford et al[206] reported 3 cases of compression of the sciatic nerve caused by polyethylene wear debris at the revision THA surgery. Recently, Mert et al[64] also reported that minor polyethylene wear at the edge of the liner and cracking of the titanium acetabular shell were observed at the revision THA. Histological examination showed that the resected cyst included foreign-body giant cells along with abundant titanium deposits and polyethylene particles. These cystic masses with sciatic neuropathy following THA appear to be synovial cysts connected with the joint space. We present MRI findings of an unpublished case of sciatic neuropathy due to a cystic lesion in which the patient had a 1-mo history of increasing pain in the left buttock and lower leg with an insidious onset (Figure 9).
Figure 9.
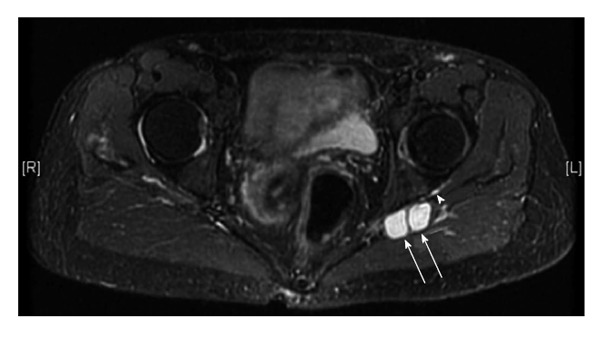
A 67-year-old female with a sciatica. Axial short tau inversion recovery magnetic resonance image demonstrates cysts at the posterior aspect of the left acetubulum (arrows). The stalk is connected to the posterior joint capsule (arrowhead).
Lateral cutaneous femoral nerve: Meralgia paraesthetica is numbness or pain in the outer thigh caused by entrapment of the lateral cutaneous femoral nerve. Only one case was reported as a compression neuropathy caused by a hip joint synovial cyst associated with rheumatoid arthritis[270].
Artery compression
Compression of the femoral artery causes leg ischemia. Byström et al[51] reported a 75-year-old female with a large cyst that was compressing the femoral artery. The symptoms were an intermittent, unpleasant sensation of coolness in the foot and hip pain. The cyst was communicating with a severely osteoarthritic hip joint. Beardsmore et al[271] and Stanek et al[272] also reported ganglion cysts arising from the hip joint or psoas sheath that compressed the artery and caused symptoms of intermittent claudication. Furthermore, Zack et al[57] presented an occlusion of the external iliac artery due to a giant synovial cyst that was produced by polyethylene wear debris after THA. In such cases, angiography can demonstrate occlusions of the external iliac or common femoral artery[57,263,264].
Vein compression
Compression of the femoral or iliac vein caused by a cyst of the hip joint results in leg swelling, which resembles that caused by deep vein thrombosis, and is called pseudothrombophlebitis. Previously, over 40 cases of vein compression due to a cystic lesion around the hip have been described in literature[12,21,23,50,56,73,83,101-103,107,110,115,125,131,133,137,138,176,179,188,190,192,196,198,209,220,222,230,232,254,273-289]. Radiography of the pelvis was useful for observing the presence of hip disorders because rheumatoid arthritis or osteoarthritis was present in approximately two-thirds of the cases[276]. Extrinsic compression of the external iliac and femoral veins by the mass can be observed by venography. Venography is also useful if deep vein thrombosis is suspected and needs to be excluded. A cystic lesion of the hip joint should be taken into consideration in the differential diagnosis of deep vein thrombosis.
Urinary symptoms
When a cyst compresses the ureter or bladder, the patient may complain of dysuria, frequency, and nocturia, or have no symptoms[18,83,182,226]. Intravenous pyelography can reveal obstruction of the ureter, which results in hydronephrosis of the kidney[212]. Watson and Ochsner reported a case with high urinary frequency and dribbling caused by compression of the lateral walls of the bladder due to a distended iliopsoas bursa[182].
TREATMENT
Although variable therapeutic strategies have been used for cystic lesions of the hip, treatment of the cysts depends on their size, the severity of symptoms, the nature of the underlying disease or associated condition, and the presence or absence of local compression. When cysts of the hip are asymptomatic, they can be treated by observation[22,54,253]. When an enlarged and painful cyst is suspected to be a synovial cyst or bursitis, rest, nonsteroidal anti-inflammatory medications, application of local heat, and physical therapy may provide symptomatic relief[7,21,96,98,100]. If the cyst is a synovial cyst caused by rheumatoid arthritis, prednisone and methotrexate may be effective for decreasing the symptoms[40,114,136,152]. In addition, injection of local anesthetic and/or corticosteroids following needle aspiration may be considered as a treatment option[7,23,83,98,100,112,175,185,258]. When patients have compression neuropathy or obstruction of an artery, vein, or ureter due to a cyst, they are often treated by aspiration of the cyst or surgical excision. Colasanti et al[276] reviewed 27 cases with vessel compression due to cysts. Needle aspiration was initially performed in 8 of the patients, and the other 19 patients were treated by surgical removal of the cysts associated with synovectomy or capsulectomy[12,21,23,51,68,83,101-103,110,125,131,176,188,254,273,275-280,282-284,286]. Lower limb swelling recurred in 3 of 8 patients (37%) initially treated with needle aspiration, whereas recurrence was noted in only 1 surgically treated patient (5%). This result indicated that surgical excision is a more reliable technique for prevention of recurrence[107,130,134,147,148,189,260,290,291]. However, we still believe that needle aspiration/puncture should be the first treatment choice because simple needle aspiration/puncture has been shown to decrease the cyst size and symptoms in some cases involving vein or nerve compression[21,83,125,131,286], it is easier to perform and less invasive than surgery, and the contents of a cyst can aid diagnosis[34,195,286]. When a cystic lesion associated with osteoarthritis, rheumatoid arthritis, and THA is excised, primary or revision THA surgery may be necessary to relieve the pain and improve hip functions[9,38,119,127,180].
CONCLUSION
Almost all cystic lesions around the hip joint will be asymptomatic, but recently, they are frequently discovered by CT or MRI examinations. Enlargement of a cyst, including the bursa, might cause unexplained hip pain. Furthermore, when cysts compress their surrounding structures, such as nerves or vessels, various symptoms will appear depending on the compressed tissue. In orthopaedics, leg pain, intermittent claudication, or leg edema are common symptoms in lumbar spine or vascular disorders. In such cases, cysts around the hip should be considered as the differential diagnosis.
Footnotes
P- Reviewer: Musumeci G, Ohishi T S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Conflict-of-interest statement: All authors state that they have no conflicts of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: April 24, 2015
First decision: June 9, 2015
Article in press: September 8, 2015
References
- 1.Cook TD. Ganglion of the hip; case report. Surgery. 1952;32:129–131. [PubMed] [Google Scholar]
- 2.Chandler S. The iliopsoas bursa in man. Anat Rec. 1934;58:235–240. [Google Scholar]
- 3.Soren A. Pathogenesis and treatment of ganglion. Clin Orthop Relat Res. 1966;48:173–179. [PubMed] [Google Scholar]
- 4.Steiner E, Steinbach LS, Schnarkowski P, Tirman PF, Genant HK. Ganglia and cysts around joints. Radiol Clin North Am. 1996;34:395–425, xi-xii. [PubMed] [Google Scholar]
- 5.Haller J, Resnick D, Greenway G, Chevrot A, Murray W, Haghighi P, Sartoris DJ, Chen CK. Juxtaacetabular ganglionic (or synovial) cysts: CT and MR features. J Comput Assist Tomogr. 1989;13:976–983. doi: 10.1097/00004728-198911000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Schnarkowski P, Steinbach LS, Tirman PF, Peterfy CG, Genant HK. Magnetic resonance imaging of labral cysts of the hip. Skeletal Radiol. 1996;25:733–737. doi: 10.1007/s002560050170. [DOI] [PubMed] [Google Scholar]
- 7.Coventry MB, Polley HF, Weiner AD. Rheumatoid synovial cyst of the hip; report of three cases. J Bone Joint Surg Am. 1959;41-A:721–730 passim. [PubMed] [Google Scholar]
- 8.Fokter SK, Repse-Fokter A, Takac I. Case report: femoral neuropathy secondary to total hip arthroplasty wear debris. Clin Orthop Relat Res. 2009;467:3032–3035. doi: 10.1007/s11999-009-0894-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kataoka M, Torisu T, Nakamura M, Uchida K. Iliopsoas bursa of the rheumatoid hip joint. A case report and review of the literature. Clin Rheumatol. 1995;14:358–364. doi: 10.1007/BF02208355. [DOI] [PubMed] [Google Scholar]
- 10.Lin YK, Tien YC, Lin SY. Hip ganglion cyst associated with developmental dysplasia of hip in a child-a case report. Acta Orthop Scand. 2002;73:109–110. doi: 10.1080/000164702317281512. [DOI] [PubMed] [Google Scholar]
- 11.Pritchard RS, Shah HR, Nelson CL, FitzRandolph RL. MR and CT appearance of iliopsoas bursal distention secondary to diseased hips. J Comput Assist Tomogr. 1990;14:797–800. doi: 10.1097/00004728-199009000-00024. [DOI] [PubMed] [Google Scholar]
- 12.Sartoris DJ, Danzig L, Gilula L, Greenway G, Resnick D. Synovial cysts of the hip joint and iliopsoas bursitis: a spectrum of imaging abnormalities. Skeletal Radiol. 1985;14:85–94. doi: 10.1007/BF00349741. [DOI] [PubMed] [Google Scholar]
- 13.Torisu T, Chosa H, Kitano M. Rheumatoid synovial cyst of the hip joint: a case report. Clin Orthop Relat Res. 1978;(137):191–194. [PubMed] [Google Scholar]
- 14.Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57:413–415. [PubMed] [Google Scholar]
- 15.Flanagan FL, Sant S, Coughlan RJ, O’Connell D. Symptomatic enlarged iliopsoas bursae in the presence of a normal plain hip radiograph. Br J Rheumatol. 1995;34:365–369. doi: 10.1093/rheumatology/34.4.365. [DOI] [PubMed] [Google Scholar]
- 16.Wunderbaldinger P, Bremer C, Schellenberger E, Cejna M, Turetschek K, Kainberger F. Imaging features of iliopsoas bursitis. Eur Radiol. 2002;12:409–415. doi: 10.1007/s003300101041. [DOI] [PubMed] [Google Scholar]
- 17.Gong E, Jia B, Shi Z, Zhou L, Xu G, Tian Z. [CT/MRI image characteristics of iliopsoas bursitis in avascular necrosis of femoral head] Zhongguo Xiufu Chongjian Waike Zazhi. 2008;22:295–298. [PubMed] [Google Scholar]
- 18.Hattrup SJ, Bryan RS, Gaffey TA, Stanhope CR. Pelvic mass causing vesical compression after total hip arthroplasty. Case report. Clin Orthop Relat Res. 1988;227:184–189. [PubMed] [Google Scholar]
- 19.Fischer SR, Christ DJ, Roehr BA. Sciatic neuropathy secondary to total hip arthroplasty wear debris. J Arthroplasty. 1999;14:771–774. doi: 10.1016/s0883-5403(99)90237-1. [DOI] [PubMed] [Google Scholar]
- 20.Nazarian DG, Zeni JA. Management of a pelvic mass following a worn uncemented total hip arthroplasty. J Arthroplasty. 2012;27:323.e17–323.e20. doi: 10.1016/j.arth.2011.03.023. [DOI] [PubMed] [Google Scholar]
- 21.Ford MJ, Martynoga AG, Nuki G. Iliopsoas bursitis in rheumatoid arthritis: an unusual cause of leg oedema. Br Med J (Clin Res Ed) 1981;282:947–948. doi: 10.1136/bmj.282.6268.947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Staple TW. Arthrographic demonstration of lliopsoas bursa extension of the hip joint. Radiology. 1972;102:515–516. doi: 10.1148/102.3.515. [DOI] [PubMed] [Google Scholar]
- 23.Armstrong P, Saxton H. Ilio-psoas bursa. Br J Radiol. 1972;45:493–495. doi: 10.1259/0007-1285-45-535-493. [DOI] [PubMed] [Google Scholar]
- 24.Harper MC, Schaberg JE, Allen WC. Primary iliopsoas bursography in the diagnosis of disorders of the hip. Clin Orthop Relat Res. 1987;(221):238–241. [PubMed] [Google Scholar]
- 25.Kolmert L, Persson BM, Herrlin K, Ekelund L. Ileopectineal bursitis following total hip replacement. Acta Orthop Scand. 1984;55:63–65. doi: 10.3109/17453678408992314. [DOI] [PubMed] [Google Scholar]
- 26.Loneragan R, Anderson J, Taylor J. Distended iliopsoas bursa: case reports and anatomical dissection. Australas Radiol. 1994;38:331–335. doi: 10.1111/j.1440-1673.1994.tb00212.x. [DOI] [PubMed] [Google Scholar]
- 27.Yoon TR, Song EK, Chung JY, Park CH. Femoral neuropathy caused by enlarged iliopsoas bursa associated with osteonecrosis of femoral head--a case report. Acta Orthop Scand. 2000;71:322–324. doi: 10.1080/000164700317411960. [DOI] [PubMed] [Google Scholar]
- 28.Morita M, Yamada H, Terahata S, Tamai S, Shinmei M. Pseudo-synovial cyst arising at the pubic bone region and forming a large femoral-inguinal mass. J Rheumatol. 1997;24:396–399. [PubMed] [Google Scholar]
- 29.Vaccaro JP, Sauser DD, Beals RK. Iliopsoas bursa imaging: efficacy in depicting abnormal iliopsoas tendon motion in patients with internal snapping hip syndrome. Radiology. 1995;197:853–856. doi: 10.1148/radiology.197.3.7480768. [DOI] [PubMed] [Google Scholar]
- 30.Fritz P, Mariette X, Clerc D, Glon Y, Bennet P, Bisson M. Rectus femoris sheath: a new localization of hip synovial cyst. J Rheumatol. 1989;16:1575–1578. [PubMed] [Google Scholar]
- 31.Matsumoto K, Hukuda S, Nishioka J, Fujita T. Iliopsoas bursal distension caused by acetabular loosening after total hip arthroplasty. A rare complication of total hip arthroplasty. Clin Orthop Relat Res. 1992;(279):144–148. [PubMed] [Google Scholar]
- 32.Mau H, Niethard FU. [Cause of pain in early dysplasia coxarthrosis. A case report] Z Orthop Ihre Grenzgeb. 1995;133:364–366. doi: 10.1055/s-2008-1039809. [DOI] [PubMed] [Google Scholar]
- 33.Steinbach LS, Schneider R, Goldman AB, Kazam E, Ranawat CS, Ghelman B. Bursae and abscess cavities communicating with the hip. Diagnosis using arthrography and CT. Radiology. 1985;156:303–307. doi: 10.1148/radiology.156.2.4011891. [DOI] [PubMed] [Google Scholar]
- 34.Yukata K, Arai K, Yoshizumi Y, Tamano K, Imada K, Nakaima N. Obturator neuropathy caused by an acetabular labral cyst: MRI findings. AJR Am J Roentgenol. 2005;184:S112–S114. doi: 10.2214/ajr.184.3_supplement.0184s112. [DOI] [PubMed] [Google Scholar]
- 35.Lavyne MH, Voorhies RM, Coll RH. Femoral neuropathy caused by an iliopsoas bursal cyst. Case report. J Neurosurg. 1982;56:584–586. doi: 10.3171/jns.1982.56.4.0584. [DOI] [PubMed] [Google Scholar]
- 36.Kim SM, Shin MJ, Kim KS, Ahn JM, Cho KH, Chang JS, Lee SH, Chhem RK. Imaging features of ischial bursitis with an emphasis on ultrasonography. Skeletal Radiol. 2002;31:631–636. doi: 10.1007/s00256-002-0573-1. [DOI] [PubMed] [Google Scholar]
- 37.Bianchi S, Martinoli C, Keller A, Bianchi-Zamorani MP. Giant iliopsoas bursitis: sonographic findings with magnetic resonance correlations. J Clin Ultrasound. 2002;30:437–441. doi: 10.1002/jcu.10093. [DOI] [PubMed] [Google Scholar]
- 38.Di Sante L, Paoloni M, De Benedittis S, Tognolo L, Santilli V. Groin pain and iliopsoas bursitis: always a cause-effect relationship? J Back Musculoskelet Rehabil. 2014;27:103–106. doi: 10.3233/BMR-130412. [DOI] [PubMed] [Google Scholar]
- 39.Forstner R, Forstner K, Grethen C, Kainberger P. [Ultrasound diagnosis of iliopectineal bursitis--contribution to differential diagnosis of leg swelling] Rofo. 1998;169:408–411. doi: 10.1055/s-2007-1015308. [DOI] [PubMed] [Google Scholar]
- 40.Ginesty E, Dromer C, Galy-Fourcade D, Bénazet JF, Marc V, Zabraniecki L, Railhac JJ, Fournié B. Iliopsoas bursopathies. A review of twelve cases. Rev Rhum Engl Ed. 1998;65:181–186. [PubMed] [Google Scholar]
- 41.Iversen JK, Nelleman H, Buus A, Stengaard-Pedersen K, Lucht U, Myhre Jensen O, Jurik AG. Synovial cysts of the hips in seronegative arthritis. Skeletal Radiol. 1996;25:396–399. doi: 10.1007/s002560050103. [DOI] [PubMed] [Google Scholar]
- 42.Lerais JM, Baudrillard JC, Durot JF, Segal P, Tellart MO, Wallays C, Auquier F, Toubas O, Petit J. [Synovial cysts of unusual localization. 2 cases and review of the literature] J Radiol. 1986;67:201–207. [PubMed] [Google Scholar]
- 43.Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45:161–168. doi: 10.1016/s0009-9260(05)80632-4. [DOI] [PubMed] [Google Scholar]
- 44.Nestorova R, Vlad V, Petranova T, Porta F, Radunovic G, Micu MC, Iagnocco A. Ultrasonography of the hip. Med Ultrason. 2012;14:217–224. [PubMed] [Google Scholar]
- 45.Pellman E, Kumari S, Greenwald R. Rheumatoid iliopsoas bursitis presenting as unilateral leg edema. J Rheumatol. 1986;13:197–200. [PubMed] [Google Scholar]
- 46.Roth J, Scheer I, Kraft S, Keitzer R, Riebel T. Uncommon synovial cysts in children. Eur J Pediatr. 2006;165:178–181. doi: 10.1007/s00431-005-0028-5. [DOI] [PubMed] [Google Scholar]
- 47.Wilhelm E. [Sonographic detection of a cystic tumor originating in the hip joint (bursitis iliopectinea). Contribution to the differential diagnosis of tumors of the hip] Ultraschall Med. 1987;8:40. doi: 10.1055/s-2007-1011656. [DOI] [PubMed] [Google Scholar]
- 48.Blankenbaker DG, De Smet AA, Keene JS. Sonography of the iliopsoas tendon and injection of the iliopsoas bursa for diagnosis and management of the painful snapping hip. Skeletal Radiol. 2006;35:565–571. doi: 10.1007/s00256-006-0084-6. [DOI] [PubMed] [Google Scholar]
- 49.Flanum ME, Keene JS, Blankenbaker DG, Desmet AA. Arthroscopic treatment of the painful “internal” snapping hip: results of a new endoscopic technique and imaging protocol. Am J Sports Med. 2007;35:770–779. doi: 10.1177/0363546506298580. [DOI] [PubMed] [Google Scholar]
- 50.Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124:720–723. doi: 10.1007/s00402-004-0751-9. [DOI] [PubMed] [Google Scholar]
- 51.Byström S, Adalberth G, Milbrink J. Giant synovial cyst of the hip: an unusual presentation with compression of the femoral vessels. Can J Surg. 1995;38:368–370. [PubMed] [Google Scholar]
- 52.Kalacı A, Dogramaci Y, Sevinç TT, Yanat AN. Femoral nerve compression secondary to a ganglion cyst arising from a hip joint: a case report and review of the literature. J Med Case Rep. 2009;3:33. doi: 10.1186/1752-1947-3-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Liman J, von Gottberg P, Bähr M, Kermer P. Femoral nerve palsy caused by ileopectineal bursitis after total hip replacement: a case report. J Med Case Rep. 2011;5:190. doi: 10.1186/1752-1947-5-190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.O’Riordan CO, Ahmed W, Grace P, Burke T. Synovial cyst of the hip joint: an unusual cause of a pulsating groin mass. Ir Med J. 2002;95:24–25. [PubMed] [Google Scholar]
- 55.Penkava RR. Iliopsoas bursitis demonstrated by computed tomography. AJR Am J Roentgenol. 1980;135:175–176. doi: 10.2214/ajr.135.1.175. [DOI] [PubMed] [Google Scholar]
- 56.Toohey AK, LaSalle TL, Martinez S, Polisson RP. Iliopsoas bursitis: clinical features, radiographic findings, and disease associations. Semin Arthritis Rheum. 1990;20:41–47. doi: 10.1016/0049-0172(90)90093-u. [DOI] [PubMed] [Google Scholar]
- 57.Zack JR, Greben C, Simon DW, Naidich JB. Iliac artery thrombosis secondary to a giant synovial cyst. Orthopedics. 2003;26:1153–1154. doi: 10.3928/0147-7447-20031101-19. [DOI] [PubMed] [Google Scholar]
- 58.Peters A, Tillmann B. [Bursa iliopectinea--size and morphology] Anat Anz. 1988;167:403–407. [PubMed] [Google Scholar]
- 59.Peters JC, Coleman BG, Turner ML, Arger PH, Mulhern CB, Dalinka MK, Allan DA, Schumacher HR. CT evaluation of enlarged lliopsoas bursa. AJR Am J Roentgenol. 1980;135:392–394. doi: 10.2214/ajr.135.2.392. [DOI] [PubMed] [Google Scholar]
- 60.Manueddu CA, Hoogewoud HM, Balague F, Waldeburger M. Infective iliopsoas bursitis. A case report. Int Orthop. 1991;15:135–137. doi: 10.1007/BF00179712. [DOI] [PubMed] [Google Scholar]
- 61.Skiadas V, Koutoulidis V, Plotas A. An atypical case of noninfected iliopsoas bursitis - MRI findings. J Radiol Case Rep. 2009;3:15–18. doi: 10.3941/jrcr.v3i10.326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Cohen JM, Hodges SC, Weinreb JC, Muschler G. MR imaging of iliopsoas bursitis and concurrent avascular necrosis of the femoral head. J Comput Assist Tomogr. 1985;9:969–971. doi: 10.1097/00004728-198509000-00028. [DOI] [PubMed] [Google Scholar]
- 63.Lee KH, Park YS, Lim SJ. Arthroscopic treatment of symptomatic paralabral cysts in the hip. Orthopedics. 2013;36:e373–e376. doi: 10.3928/01477447-20130222-29. [DOI] [PubMed] [Google Scholar]
- 64.Mert M, Oztürkmen Y, Unkar EA, Erdoğan S, Uzümcügil O. Sciatic nerve compression by an extrapelvic cyst secondary to wear debris after a cementless total hip arthroplasty: A case report and literature review. Int J Surg Case Rep. 2013;4:805–808. doi: 10.1016/j.ijscr.2013.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Patkar D, Shah J, Prasad S, Patankar T, Gokhale S, Krishnan A, Limdi J. Giant rheumatoid synovial cyst of the hip joint: diagnosed by MRI. J Postgrad Med. 1999;45:118–119. [PubMed] [Google Scholar]
- 66.Robinson KP, Carroll FA, Bull MJ, McClelland M, Stockley I. Transient femoral nerve palsy associated with a synovial cyst of the hip in a patient with spinal cord injury. J Bone Joint Surg Br. 2007;89:107–108. doi: 10.1302/0301-620X.89B1.18273. [DOI] [PubMed] [Google Scholar]
- 67.Sherman PM, Matchette MW, Sanders TG, Parsons TW. Acetabular paralabral cyst: an uncommon cause of sciatica. Skeletal Radiol. 2003;32:90–94. doi: 10.1007/s00256-002-0543-7. [DOI] [PubMed] [Google Scholar]
- 68.Stuplich M, Hottinger AF, Stoupis C, Sturzenegger M. Combined femoral and obturator neuropathy caused by synovial cyst of the hip. Muscle Nerve. 2005;32:552–554. doi: 10.1002/mus.20364. [DOI] [PubMed] [Google Scholar]
- 69.Wu KW, Hu MH, Huang SC, Kuo KN, Yang SH. Giant ganglionic cyst of the hip as a rare cause of sciatica. J Neurosurg Spine. 2011;14:484–487. doi: 10.3171/2010.12.SPINE10498. [DOI] [PubMed] [Google Scholar]
- 70.Amrar-Vennier F, Lerais JM, Dibiane A, Guy F, Blavoux M, Couaillier JF, Cercueil JP, Krause D. [Subcutaneous trochanteric bursitis: an unrecognized cause of peritrochanteric pain revealed by imaging] J Radiol. 1998;79:557–562. [PubMed] [Google Scholar]
- 71.Genez BM. MR diagnosis of a prosthesis pseudobursa. AJR Am J Roentgenol. 1988;151:837. doi: 10.2214/ajr.151.4.837-a. [DOI] [PubMed] [Google Scholar]
- 72.Lupetin AR, Daffner RH. Rheumatoid iliopsoas bursitis: MR findings. J Comput Assist Tomogr. 1990;14:1035–1036. doi: 10.1097/00004728-199011000-00040. [DOI] [PubMed] [Google Scholar]
- 73.Murphy CL, Meaney JF, Rana H, McCarthy EM, Howard D, Cunnane G. Giant iliopsoas bursitis: a complication of chronic arthritis. J Clin Rheumatol. 2010;16:83–85. doi: 10.1097/RHU.0b013e3181d072bb. [DOI] [PubMed] [Google Scholar]
- 74.Scherger B, Hinkenjann B, Klein M, Ostermann PA. [Extensive hip joint ganglion as a rare cause of chronic pain in the groin] Orthopade. 2007;36:868–870. doi: 10.1007/s00132-007-1123-2. [DOI] [PubMed] [Google Scholar]
- 75.Varma DG, Richli WR, Charnsangavej C, Samuels BI, Kim EE, Wallace S. MR appearance of the distended iliopsoas bursa. AJR Am J Roentgenol. 1991;156:1025–1028. doi: 10.2214/ajr.156.5.2017926. [DOI] [PubMed] [Google Scholar]
- 76.Pettersson H, Eliasson J, Egund N, Rööser B, Willén H, Rydholm A, Berg NO, Holtås S. Gadolinium-DTPA enhancement of soft tissue tumors in magnetic resonance imaging--preliminary clinical experience in five patients. Skeletal Radiol. 1988;17:319–323. doi: 10.1007/BF00367175. [DOI] [PubMed] [Google Scholar]
- 77.Magerkurth O, Jacobson JA, Girish G, Brigido MK, Bedi A, Fessell D. Paralabral cysts in the hip joint: findings at MR arthrography. Skeletal Radiol. 2012;41:1279–1285. doi: 10.1007/s00256-012-1395-4. [DOI] [PubMed] [Google Scholar]
- 78.O’Cooner DS. Early recognition of iliopectineal bursitis. Surg Gynec Obstet. 1933;57:576–579. [Google Scholar]
- 79.Cotten A, Boutry N, Demondion X, Paret C, Dewatre F, Liesse A, Chastanet P, Fontaine C. Acetabular labrum: MRI in asymptomatic volunteers. J Comput Assist Tomogr. 1998;22:1–7. doi: 10.1097/00004728-199801000-00001. [DOI] [PubMed] [Google Scholar]
- 80.Schmitz MR, Campbell SE, Fajardo RS, Kadrmas WR. Identification of acetabular labral pathological changes in asymptomatic volunteers using optimized, noncontrast 1.5-T magnetic resonance imaging. Am J Sports Med. 2012;40:1337–1341. doi: 10.1177/0363546512439991. [DOI] [PubMed] [Google Scholar]
- 81.Register B, Pennock AT, Ho CP, Strickland CD, Lawand A, Philippon MJ. Prevalence of abnormal hip findings in asymptomatic participants: a prospective, blinded study. Am J Sports Med. 2012;40:2720–2724. doi: 10.1177/0363546512462124. [DOI] [PubMed] [Google Scholar]
- 82.Botchu R, Esler CN, Lloyd DM, Rennie WJ. Ganglia arising from the transverse acetabular ligament: a report of two cases. J Orthop Surg (Hong Kong) 2013;21:380–382. doi: 10.1177/230949901302100324. [DOI] [PubMed] [Google Scholar]
- 83.Binek R, Levinsohn EM. Enlarged iliopsoas bursa. An unusual cause of thigh mass and hip pain. Clin Orthop Relat Res. 1987;(224):158–163. [PubMed] [Google Scholar]
- 84.Helfgott SM. Unusual features of iliopsoas bursitis. Arthritis Rheum. 1988;31:1331–1333. doi: 10.1002/art.1780311021. [DOI] [PubMed] [Google Scholar]
- 85.Robinson P, White LM, Agur A, Wunder J, Bell RS. Obturator externus bursa: anatomic origin and MR imaging features of pathologic involvement. Radiology. 2003;228:230–234. doi: 10.1148/radiol.2281020819. [DOI] [PubMed] [Google Scholar]
- 86.Dunn T, Heller CA, McCarthy SW, Dos Remedios C. Anatomical study of the “trochanteric bursa”. Clin Anat. 2003;16:233–240. doi: 10.1002/ca.10084. [DOI] [PubMed] [Google Scholar]
- 87.Heller A. Anatomy of the trochanteric bursae. Radiology. 2003;226:921; author reply 921–922. doi: 10.1148/radiol.2263020857. [DOI] [PubMed] [Google Scholar]
- 88.Pfirrmann CW, Chung CB, Theumann NH, Trudell DJ, Resnick D. Greater trochanter of the hip: attachment of the abductor mechanism and a complex of three bursae--MR imaging and MR bursography in cadavers and MR imaging in asymptomatic volunteers. Radiology. 2001;221:469–477. doi: 10.1148/radiol.2211001634. [DOI] [PubMed] [Google Scholar]
- 89.Woodley SJ, Mercer SR, Nicholson HD. Morphology of the bursae associated with the greater trochanter of the femur. J Bone Joint Surg Am. 2008;90:284–294. doi: 10.2106/JBJS.G.00257. [DOI] [PubMed] [Google Scholar]
- 90.Hwang JY, Lee SW, Kim JO. MR imaging features of obturator internus bursa of the hip. Korean J Radiol. 2008;9:375–378. doi: 10.3348/kjr.2008.9.4.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Kassarjian A, Llopis E, Schwartz RB, Bencardino JT. Obturator externus bursa: prevalence of communication with the hip joint and associated intra-articular findings in 200 consecutive hip MR arthrograms. Eur Radiol. 2009;19:2779–2782. doi: 10.1007/s00330-009-1476-5. [DOI] [PubMed] [Google Scholar]
- 92.Le Floch P. [Serous ischial bursa] Bull Assoc Anat (Nancy) 1982;66:89–94. [PubMed] [Google Scholar]
- 93.Pope TL, Keats TE, de Lange EE, Fechner RE, Harvey JW. Idiopathic synovial chondromatosis in two unusual sites: inferior radioulnar joint and ischial bursa. Skeletal Radiol. 1987;16:205–208. doi: 10.1007/BF00356954. [DOI] [PubMed] [Google Scholar]
- 94.Gatch WD, Green WT. Cysts of the ilio-psoas bursa. Ann Surg. 1925;82:277–285. doi: 10.1097/00000658-192508000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Finder JG. Iliopectinealbursitis. Arch Surg. 1938;36:519–530. [Google Scholar]
- 96.Hucherson DC, Denman FR. Non-infectious iliopectineal bursitis. Am J Surg. 1946;72:576–579. doi: 10.1016/0002-9610(46)90394-7. [DOI] [PubMed] [Google Scholar]
- 97.Sumanovac Z. Traumatic cyst in the hip joint; a case report. J Bone Joint Surg Am. 1959;41-A:175–178. [PubMed] [Google Scholar]
- 98.Hucherson DC, Freeman GE. Iliopectineal bursitis. A cause of hip pain frequently unrecognized. Am J Orthop. 1962;4:220–221. [PubMed] [Google Scholar]
- 99.Jeremy R. Acute psoas bursitis and unusual joint cysts in rheumatoid arthritis. Med J Aust. 1969;2:1106–1107. [PubMed] [Google Scholar]
- 100.Samuelson C, Ward JR, Albo D. Rheumatoid synovial cyst of the hip. A case report. Arthritis Rheum. 1971;14:105–108. doi: 10.1002/art.1780140113. [DOI] [PubMed] [Google Scholar]
- 101.Chilton CP, Darke SG. External iliac venous compression by a giant iliopsoas rheumatoid bursa. Br J Surg. 1980;67:641. doi: 10.1002/bjs.1800670911. [DOI] [PubMed] [Google Scholar]
- 102.Grindulis KA, McConkey B, Norcross K. Iliopsoas bursitis--a surgically correctable cause of lower limb oedema. Practitioner. 1982;226:1336–1337. [PubMed] [Google Scholar]
- 103.Janus C, Hermann G. Enlargement of the iliopsoas bursa: unusual cause of cystic mass on pelvic sonogram. J Clin Ultrasound. 1982;10:133–135. doi: 10.1002/jcu.1870100310. [DOI] [PubMed] [Google Scholar]
- 104.Dyon JF, Ben Salah S, Baudain P, De Marliave H, Delannoy P. [An abdominal tumor of unusual nature. Synovial cyst in the iliopsoas bursa] Chir Pediatr. 1987;28:115–119. [PubMed] [Google Scholar]
- 105.Dihlmann W, Peters A, Tillmann B. [The bursa iliopectinea--a morphologic-computed tomographic study] Rofo. 1989;150:274–279. doi: 10.1055/s-2008-1047022. [DOI] [PubMed] [Google Scholar]
- 106.Mainard D, Reynier A, Delagoutte JP. [Value of the scanner for diagnosing synovial cysts of the hip. Apropos of 2 cases. Review of the literature] Rev Chir Orthop Reparatrice Appar Mot. 1989;75:271–277. [PubMed] [Google Scholar]
- 107.Diel R, Tuschick B, Hamborg V, Krüger C. [Enlarged iliopsoas bursa. Possible significance and place of computed tomography and sonography] Radiologe. 1990;30:547–549. [PubMed] [Google Scholar]
- 108.Ginai AZ. Case report 607: Synovial (osteo) chondromatosis of left hip joint and ileopsoas bursa. Skeletal Radiol. 1990;19:227–231. doi: 10.1007/BF00204106. [DOI] [PubMed] [Google Scholar]
- 109.Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29–32. doi: 10.1302/0301-620X.73B1.1991769. [DOI] [PubMed] [Google Scholar]
- 110.Savarese RP, Kaplan SM, Calligaro KD, DeLaurentis DA. Iliopectineal bursitis: an unusual cause of iliofemoral vein compression. J Vasc Surg. 1991;13:725–727. [PubMed] [Google Scholar]
- 111.Gresser J, Bitz K, Binswanger R, Hegglin J. [Bursitis iliopectinea--a rare differential diagnosis of painful inguinal swelling] Helv Chir Acta. 1992;59:383–388. [PubMed] [Google Scholar]
- 112.Stadelmann A, Waldis M, von Hochstetter A, Schreiber A. [Nerve compression syndrome caused by synovial cyst of the hip joint] Z Orthop Ihre Grenzgeb. 1992;130:125–128. doi: 10.1055/s-2008-1040125. [DOI] [PubMed] [Google Scholar]
- 113.Wössmann W, Verhage CC. [Enlarged iliopsoas bursa. A rare cause of inguinal mass] Tidsskr Nor Laegeforen. 1992;112:202–203. [PubMed] [Google Scholar]
- 114.Generini S, Matucci-Cerinic M. Iliopsoas bursitis in rheumatoid arthritis. Clin Exp Rheumatol. 1993;11:549–551. [PubMed] [Google Scholar]
- 115.Jones PB, Economou G, Adams JE, Bernstein RM. Iliopsoas bursa presenting as deep vein thrombosis in rheumatoid arthritis. Br J Rheumatol. 1993;32:832–834. doi: 10.1093/rheumatology/32.9.832. [DOI] [PubMed] [Google Scholar]
- 116.Bakx PA, Wiggers RH. Iliopsoas bursa: a rare type of swelling in the groin. Eur J Surg. 1996;162:249–250. [PubMed] [Google Scholar]
- 117.Byrne PA, Rees JI, Williams BD. Iliopsoas bursitis-an unusual presentation of metastatic bone disease. Br J Rheumatol. 1996;35:285–288. doi: 10.1093/rheumatology/35.3.285. [DOI] [PubMed] [Google Scholar]
- 118.van Riet YE, van Vroonhoven TJ, van der Werken C, Berkhoudt AN. Bursae communicating with the hip joint. A report on 2 cases. Acta Orthop Belg. 1996;62:120–122. [PubMed] [Google Scholar]
- 119.Emery D, Griffiths W. Ileopectineal bursitis: orthopaedic cause for a lump in the groin. J R Soc Med. 1997;90:158–159. doi: 10.1177/014107689709000312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Moran KM, Finkbeiner AA. Iliopsoas abscess following catheterization of the femoral artery: diagnostic and treatment strategies. Am J Orthop (Belle Mead NJ) 1997;26:446–448. [PubMed] [Google Scholar]
- 121.Johnston CA, Wiley JP, Lindsay DM, Wiseman DA. Iliopsoas bursitis and tendinitis. A review. Sports Med. 1998;25:271–283. doi: 10.2165/00007256-199825040-00005. [DOI] [PubMed] [Google Scholar]
- 122.Mallant MP, Mastboom WJ, de Backer GP. [Inguinal pain caused by iliopsoas bursitis] Ned Tijdschr Geneeskd. 1998;142:1328–1331. [PubMed] [Google Scholar]
- 123.Nihal A, Drabu KJ. A lump in the groin: an unusual presentation of loose hip prosthesis. J R Coll Surg Edinb. 1998;43:59–60. [PubMed] [Google Scholar]
- 124.Salmerón I, Cárdenas JL, Ramirez-Escobas MA, Bermejo C. Idiopathic iliopsoas bursitis. Eur Radiol. 1999;9:175. doi: 10.1007/s003300050652. [DOI] [PubMed] [Google Scholar]
- 125.Vohra HA, Jones B. Femoral vein obstruction with an arthritic hip. J R Soc Med. 2000;93:594–595. doi: 10.1177/014107680009301112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Lin YM, Ho TF, Lee TS. Iliopectineal bursitis complicating hemiarthroplasty: a case report. Clin Orthop Relat Res. 2001;(392):366–371. doi: 10.1097/00003086-200111000-00047. [DOI] [PubMed] [Google Scholar]
- 127.Shiga T, Watanabe N, Sugita M, Kamada Y, Inoue S, Kubo T. Two cases of osteochondromatosis which developed in the iliopectineal bursa of an osteoarthritic hip. Mod Rheumatol. 2001;11:360–362. doi: 10.3109/s10165-001-8072-0. [DOI] [PubMed] [Google Scholar]
- 128.Tani Y, Nishimura I, Mimura T, Ushiyama T, Inoue K, Murakami M. Enlargement of iliopsoas bursa in a patient with polymyalgia rheumatica. J Rheumatol. 2001;28:1198–1199. [PubMed] [Google Scholar]
- 129.Luning HA, Koster MN, Coene LN. [Rapidly destructive hip disease with resultant iliopectineal bursitis] Ned Tijdschr Geneeskd. 2003;147:1282–1286. [PubMed] [Google Scholar]
- 130.Mori S, Tamura T, Komatsubara S, Kawaguchi Y, Todo S, Inoo M, Kurata N, Norimatsu H. A case of femoral nerve palsy caused by iliopectineal bursitis associated with rheumatoid arthritis. Mod Rheumatol. 2004;14:274–278. doi: 10.1007/s10165-004-0308-3. [DOI] [PubMed] [Google Scholar]
- 131.Rodriguez-Gomez M, Willisch A, Fernandez L, Lopez-Barros G, Abel V, Monton E. Bilateral giant iliopsoas bursitis presenting as refractory edema of lower limbs. J Rheumatol. 2004;31:1452–1454. [PubMed] [Google Scholar]
- 132.Grosclaude S, Adam P, Besse JL, Fessy MH. [Iliopsoas bursal distension revealing complication of total hip arthroplasty: five cases] Rev Chir Orthop Reparatrice Appar Mot. 2006;92:351–357. doi: 10.1016/s0035-1040(06)75765-8. [DOI] [PubMed] [Google Scholar]
- 133.Beksaç B, Tözün R, Baktiroglu S, Sener N, Gonzalez Della Valle A. Extravascular compression of the femoral vein due to wear debris-induced iliopsoas bursitis: a rare cause of leg swelling after total hip arthroplasty. J Arthroplasty. 2007;22:453–456. doi: 10.1016/j.arth.2006.04.002. [DOI] [PubMed] [Google Scholar]
- 134.Tokita A, Ikari K, Tsukahara S, Toki H, Miyawaki M, Mochizuki T, Kawamura K, Tomatsu T, Momohara S. Iliopsoas bursitis-associated femoral neuropathy exacerbated after internal fixation of an intertrochanteric hip fracture in rheumatoid arthritis: a case report. Mod Rheumatol. 2008;18:394–398. doi: 10.1007/s10165-008-0060-1. [DOI] [PubMed] [Google Scholar]
- 135.Yoshioka T, Tachihara A, Koyama T, Iwakawa K, Sakane M, Nakamura H. Rapid destruction of the hip joint associated with enlarged iliopsoas bursa in a patient with refractory rheumatoid arthritis. J Nippon Med Sch. 2008;75:233–238. doi: 10.1272/jnms.75.233. [DOI] [PubMed] [Google Scholar]
- 136.Nunley RM, Wilson JM, Gilula L, Clohisy JC, Barrack RL, Maloney WJ. Iliopsoas bursa injections can be beneficial for pain after total hip arthroplasty. Clin Orthop Relat Res. 2010;468:519–526. doi: 10.1007/s11999-009-1141-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Algarni AD, Huk OL, Pelmus M. Metallosis-induced iliopsoas bursal cyst causing venous obstruction and lower-limb swelling after metal-on-metal THA. Orthopedics. 2012;35:e1811–e1814. doi: 10.3928/01477447-20121120-30. [DOI] [PubMed] [Google Scholar]
- 138.Iwata T, Nozawa S, Ohashi M, Sakai H, Shimizu K. Giant iliopectineal bursitis presenting as neuropathy and severe edema of the lower limb: case illustration and review of the literature. Clin Rheumatol. 2013;32:721–725. doi: 10.1007/s10067-013-2223-5. [DOI] [PubMed] [Google Scholar]
- 139.Rothschild B. Trochanteric area pain, the result of a quartet of bursal inflammation. World J Orthop. 2013;4:100–102. doi: 10.5312/wjo.v4.i3.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Farr J. Tuberculosis of Bursa in the Region of the Hip Joint. Can Med Assoc J. 1944;50:60–62. [PMC free article] [PubMed] [Google Scholar]
- 141.Swezey RL. Pseudo-radiculopathy in subacute trochanteric bursitis of the subgluteus maximus bursa. Arch Phys Med Rehabil. 1976;57:387–390. [PubMed] [Google Scholar]
- 142.Rehm-Graves S, Weinstein AJ, Calabrese LH, Cook SA, Boumphrey FR. Tuberculosis of the greater trochanteric bursa. Arthritis Rheum. 1983;26:77–81. doi: 10.1002/art.1780260112. [DOI] [PubMed] [Google Scholar]
- 143.Zoltan DJ, Clancy WG, Keene JS. A new operative approach to snapping hip and refractory trochanteric bursitis in athletes. Am J Sports Med. 1986;14:201–204. doi: 10.1177/036354658601400304. [DOI] [PubMed] [Google Scholar]
- 144.Haller CC, Coleman PA, Estes NC, Grisolia A. Traumatic trochanteric bursitis. Kans Med. 1989;90:17–18, 22. [PubMed] [Google Scholar]
- 145.Franceschi JP, Chapuis J, Curvale G, Roux H, Aquaviva P, Groulier P. [Bacillary trochanteritis. Apropos of 30 cases] Rev Rhum Mal Osteoartic. 1991;58:433–439. [PubMed] [Google Scholar]
- 146.Varma DG, Parihar A, Richli WR. CT appearance of the distended trochanteric bursa. J Comput Assist Tomogr. 1993;17:141–143. doi: 10.1097/00004728-199301000-00027. [DOI] [PubMed] [Google Scholar]
- 147.Slawski DP, Howard RF. Surgical management of refractory trochanteric bursitis. Am J Sports Med. 1997;25:86–89. doi: 10.1177/036354659702500117. [DOI] [PubMed] [Google Scholar]
- 148.Fox JL. The role of arthroscopic bursectomy in the treatment of trochanteric bursitis. Arthroscopy. 2002;18:E34. doi: 10.1053/jars.2002.35143. [DOI] [PubMed] [Google Scholar]
- 149.Yamamoto T, Iwasaki Y, Kurosaka M. Tuberculosis of the greater trochanteric bursa occurring 51 years after tuberculous nephritis. Clin Rheumatol. 2002;21:397–400. doi: 10.1007/s100670200105. [DOI] [PubMed] [Google Scholar]
- 150.Govaert LH, van der Vis HM, Marti RK, Albers GH. Trochanteric reduction osteotomy as a treatment for refractory trochanteric bursitis. J Bone Joint Surg Br. 2003;85:199–203. doi: 10.1302/0301-620x.85b2.13474. [DOI] [PubMed] [Google Scholar]
- 151.Haritides J, Christodoulou P, Tsakonas A. Tuberculous trochanteric bursitis. Chir Organi Mov. 2004;89:177–180. [PubMed] [Google Scholar]
- 152.Cohen SP, Narvaez JC, Lebovits AH, Stojanovic MP. Corticosteroid injections for trochanteric bursitis: is fluoroscopy necessary? A pilot study. Br J Anaesth. 2005;94:100–106. doi: 10.1093/bja/aei012. [DOI] [PubMed] [Google Scholar]
- 153.Abdelwahab IF, Bianchi S, Martinoli C, Klein M, Hermann G. Atypical extraspinal musculoskeletal tuberculosis in immunocompetent patients: part II, tuberculous myositis, tuberculous bursitis, and tuberculous tenosynovites. Can Assoc Radiol J. 2006;57:278–286. [PubMed] [Google Scholar]
- 154.Kawamura E, Kawabe J, Tsumoto C, Hayashi T, Oe A, Kurooka H, Kotani J, Higashiyama S, Tsushima H, Habu D, et al. Gallium scintigraphy in a case of tuberculous trochanteric bursitis. Ann Nucl Med. 2007;21:229–233. doi: 10.1007/s12149-007-0014-2. [DOI] [PubMed] [Google Scholar]
- 155.Silva F, Adams T, Feinstein J, Arroyo RA. Trochanteric bursitis: refuting the myth of inflammation. J Clin Rheumatol. 2008;14:82–86. doi: 10.1097/RHU.0b013e31816b4471. [DOI] [PubMed] [Google Scholar]
- 156.Makki D, Watson AJ. Septic trochanteric bursitis in an adolescent. Am J Orthop (Belle Mead NJ) 2010;39:E1–E3. [PubMed] [Google Scholar]
- 157.Viradia NK, Berger AA, Dahners LE. Relationship between width of greater trochanters and width of iliac wings in tronchanteric bursitis. Am J Orthop (Belle Mead NJ) 2011;40:E159–E162. [PubMed] [Google Scholar]
- 158.Soro Marín S, Sánchez Trenado MA, Mínguez Sánchez MD, Paulino Huertas M, García Morales PV, Salas Manzanedo V. [Trochanteric bursitis due to tuberculosis in an immunocompetent young woman] Reumatol Clin. 2012;8:34–35. doi: 10.1016/j.reuma.2011.01.007. [DOI] [PubMed] [Google Scholar]
- 159.Klauser AS, Martinoli C, Tagliafico A, Bellmann-Weiler R, Feuchtner GM, Wick M, Jaschke WR. Greater trochanteric pain syndrome. Semin Musculoskelet Radiol. 2013;17:43–48. doi: 10.1055/s-0033-1333913. [DOI] [PubMed] [Google Scholar]
- 160.Koudela K, Koudelová J, Koudela K, Kunesová M. [Bursitis iliopectinea] Acta Chir Orthop Traumatol Cech. 2008;75:347–354. [PubMed] [Google Scholar]
- 161.Schvingt E, Katzner M, Steinmetz A. [Inguinal tumor due to synovial cysts of the hip] Rev Chir Orthop Reparatrice Appar Mot. 1975;61:147–152. [PubMed] [Google Scholar]
- 162.Pope TL, Fechner RE, Keats TE. Intra-osseous ganglion. Report of four cases and review of the literature. Skeletal Radiol. 1989;18:185–187. doi: 10.1007/BF00360966. [DOI] [PubMed] [Google Scholar]
- 163.DiMaio FR, Santore RF. A large ganglion cyst in a patient with hip dysplasia. Orthopedics. 1997;20:650–652. doi: 10.3928/0147-7447-19970701-16. [DOI] [PubMed] [Google Scholar]
- 164.Bech B, Dirksen KL, Jørgensen U, Jacobsen B. [Synovial femoral cyst caused by trauma to the hip verified by MR arthrography] Ugeskr Laeger. 2004;166:495–496. [PubMed] [Google Scholar]
- 165.Lamyman MJ, Baden JM, Reid CD. The diagnosis and management of an expanding post-traumatic soft tissue cyst of the hip and groin. J Plast Reconstr Aesthet Surg. 2009;62:e394–e397. doi: 10.1016/j.bjps.2008.01.027. [DOI] [PubMed] [Google Scholar]
- 166.Magee T, Hinson G. Association of paralabral cysts with acetabular disorders. AJR Am J Roentgenol. 2000;174:1381–1384. doi: 10.2214/ajr.174.5.1741381. [DOI] [PubMed] [Google Scholar]
- 167.Mervak BM, Morag Y, Marcantonio D, Jacobson J, Brandon C, Fessell D. Paralabral cysts of the hip: sonographic evaluation with magnetic resonance arthrographic correlation. J Ultrasound Med. 2012;31:495–500. doi: 10.7863/jum.2012.31.3.495. [DOI] [PubMed] [Google Scholar]
- 168.Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG. Association of glenoid labral cysts with labral tears and glenohumeral instability: radiologic findings and clinical significance. Radiology. 1994;190:653–658. doi: 10.1148/radiology.190.3.8115605. [DOI] [PubMed] [Google Scholar]
- 169.Ikeda T, Awaya G, Suzuki S, Okada Y, Tada H. Torn acetabular labrum in young patients. Arthroscopic diagnosis and management. J Bone Joint Surg Br. 1988;70:13–16. doi: 10.1302/0301-620X.70B1.3339044. [DOI] [PubMed] [Google Scholar]
- 170.Czerny C, Hofmann S, Neuhold A, Tschauner C, Engel A, Recht MP, Kramer J. Lesions of the acetabular labrum: accuracy of MR imaging and MR arthrography in detection and staging. Radiology. 1996;200:225–230. doi: 10.1148/radiology.200.1.8657916. [DOI] [PubMed] [Google Scholar]
- 171.Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R. Acetabular labral tears: evaluation with MR arthrography. Radiology. 1996;200:231–235. doi: 10.1148/radiology.200.1.8657917. [DOI] [PubMed] [Google Scholar]
- 172.Tey M, Alvarez S, Ríos JL. Hip labral cyst caused by psoas impingement. Arthroscopy. 2012;28:1184–1186. doi: 10.1016/j.arthro.2012.03.028. [DOI] [PubMed] [Google Scholar]
- 173.Kanauchi T, Suganuma J, Mochizuki R, Uchikawa S. Arthroscopic treatment of femoral nerve paresthesia caused by an acetabular paralabral cyst. Orthopedics. 2014;37:e496–e499. doi: 10.3928/01477447-20140430-62. [DOI] [PubMed] [Google Scholar]
- 174.Bergenudd H, Bengnér U, Telhag H, Hjelmqvist B. Ganglion of the hip--an unusual cause of soft tissue swelling of the groin. Arch Orthop Trauma Surg. 1987;106:274–275. doi: 10.1007/BF00454332. [DOI] [PubMed] [Google Scholar]
- 175.Jaffray DC, Nade S. Painless groin swelling associated with osteoarthritis of the hip. J R Coll Surg Edinb. 1986;31:185–186. [PubMed] [Google Scholar]
- 176.Melamed A, Bauer CA, Johnson JH. Iliopsoas bursal extension of arthritic disease of the hip. Radiology. 1967;89:54–58. doi: 10.1148/89.1.54. [DOI] [PubMed] [Google Scholar]
- 177.McBeath AA, Neidhart DA. Acetabular cyst with communicating ganglion. A case report. J Bone Joint Surg Am. 1976;58:267–269. [PubMed] [Google Scholar]
- 178.Garcia J, Chevalley P. [Synovial cysts of the hip. Diagnosis by x-ray computed tomography] J Radiol. 1985;66:425–432. [PubMed] [Google Scholar]
- 179.Delplace J, Arnaout A, Beya K, Khatib H, Lecestre P. [Synovial cyst of the hip. An unusual pathology for the orthopedic surgeon. Apropos of 2 cases] Ann Chir. 1990;44:302–305. [PubMed] [Google Scholar]
- 180.Kosuge DD, Park DH, Cannon SR, Briggs TW, Pollock RC, Skinner JA. Large osteoarthritic cyst presenting as soft tissue tumour - a case report. Ann R Coll Surg Engl. 2007;89:4–6. doi: 10.1308/147870807X1834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Keller C, Leden I, Lidgren L, Stenberg T. Anaerobic bacterial coxitis and pseudocystic tumour in rheumatoid arthritis. A case report. Scand J Rheumatol. 1980;9:216–220. doi: 10.3109/03009748009112350. [DOI] [PubMed] [Google Scholar]
- 182.Watson JD, Ochsner SF. Compression of bladder due to “rheumatoid” cysts of hip joint. Am J Roentgenol Radium Ther Nucl Med. 1967;99:695–696. doi: 10.2214/ajr.99.3.695. [DOI] [PubMed] [Google Scholar]
- 183.White TK, Incavo SJ, Moreland MS. Giant synovial cyst of the hip joint. Orthop Rev. 1988;17:609–612. [PubMed] [Google Scholar]
- 184.Feldman C. A case of rheumatoid arthritis with generalized lymphadenopathy and synovial cyst of the hip-joint. Ann Phys Med. 1961;6:23–27. doi: 10.1093/rheumatology/6.1.23. [DOI] [PubMed] [Google Scholar]
- 185.Levy RN, Hermann G, Haimov M, Sherry HS, Train JS, Davison S. Rheumatoid synovial cyst of the hip. Arthritis Rheum. 1982;25:1382–1384. doi: 10.1002/art.1780251118. [DOI] [PubMed] [Google Scholar]
- 186.Wendling D, Raguin JM, Guidet M. [Rheumatoid synovial cyst of the hip. Apropos of a case] Rev Rhum Mal Osteoartic. 1987;54:69–71. [PubMed] [Google Scholar]
- 187.Kawasaki M, Inoue H, Sabanai K, Sawai T, Sato K. Synovial cyst of the hip in a patient with rheumatoid arthritis. Mod Rheumatol. 2013;23:587–592. doi: 10.1007/s10165-012-0697-7. [DOI] [PubMed] [Google Scholar]
- 188.Benichou M, Joyeux A, Mary H, Thevenet A. [Synovial cyst of the hip. 2 cases presenting with vascular symptomatology] J Mal Vasc. 1985;10:209–211. [PubMed] [Google Scholar]
- 189.Tatsumura M, Mishima H, Shiina I, Hara Y, Nishiura Y, Ishii T, Ochiai N, Ishii W, Sumida T. Femoral nerve palsy caused by a huge iliopectineal synovitis extending to the iliac fossa in a rheumatoid arthritis case. Mod Rheumatol. 2008;18:81–85. doi: 10.1007/s10165-007-0009-9. [DOI] [PubMed] [Google Scholar]
- 190.Chalmers J, Chalmers N. Leg oedema due to a rheumatoid cyst in the pelvis. J Bone Joint Surg Br. 1992;74:390–392. doi: 10.1302/0301-620X.74B3.1587884. [DOI] [PubMed] [Google Scholar]
- 191.Griffiths HJ, Burke J, Bonfiglio TA. Granulomatous pseudotumors in total joint replacement. Skeletal Radiol. 1987;16:146–152. doi: 10.1007/BF00367764. [DOI] [PubMed] [Google Scholar]
- 192.Van Mourik JB, Josaputra HA, Axler A. Giant synovial cyst causing deep venous thrombosis: brief report. J Bone Joint Surg Br. 1988;70:841. doi: 10.1302/0301-620X.70B5.3192594. [DOI] [PubMed] [Google Scholar]
- 193.McGraw RW, Morton KS, Duncan CP. Massive intrapelvic synovial cyst as a complication of total hip replacement arthroplasty: a case report. Can J Surg. 1991;34:267–269. [PubMed] [Google Scholar]
- 194.Reigstad A, Røkkum M. An intrapelvic granuloma induced by acetabular cup loosening. Acta Orthop Scand. 1992;63:465–466. doi: 10.3109/17453679209154770. [DOI] [PubMed] [Google Scholar]
- 195.Yang SS, Bronson MJ. Cystic enlargement of the iliopsoas bursa causing venous obstruction as a complication of total hip arthroplasty. A case report. J Arthroplasty. 1993;8:657–661. doi: 10.1016/0883-5403(93)90015-v. [DOI] [PubMed] [Google Scholar]
- 196.DeFrang RD, Guyer WD, Porter JM, Duwelius PJ. Synovial cyst formation complicating total hip arthroplasty: a case report. Clin Orthop Relat Res. 1996;(325):163–167. doi: 10.1097/00003086-199604000-00018. [DOI] [PubMed] [Google Scholar]
- 197.Wang JW, Lin CC. Pelvic mass caused by polyethylene wear after uncemented total hip arthroplasty. J Arthroplasty. 1996;11:626–628. doi: 10.1016/s0883-5403(96)80121-5. [DOI] [PubMed] [Google Scholar]
- 198.Morrison KM, Apelgren KN, Mahany BD. Back pain, femoral vein thrombosis, and an iliopsoas cyst: unusual presentation of a loose total hip arthroplasty. Orthopedics. 1997;20:347–348. doi: 10.3928/0147-7447-19970401-14. [DOI] [PubMed] [Google Scholar]
- 199.Shilt JS, Rozencwaig R, Wilson MR. Pelvic mass secondary to polyethylene and titanium alloy wear debris resulting in recurrent deep vein thrombosis. J Arthroplasty. 1997;12:946–949. doi: 10.1016/s0883-5403(97)90165-0. [DOI] [PubMed] [Google Scholar]
- 200.Adelman SC, Urquhart AG, Sondak V, Biermann JS, Freiberg AA. Polyethylene wear debris presenting as a retroperitoneal tumor. Surgery. 1998;123:111–112. [PubMed] [Google Scholar]
- 201.Korkala O, Syrjänen KJ. Intrapelvic cyst formation after hip arthroplasty with a carbon fibre-reinforced polyethylene socket. Arch Orthop Trauma Surg. 1998;118:113–115. doi: 10.1007/s004020050327. [DOI] [PubMed] [Google Scholar]
- 202.Jeanrot C, Ouaknine M, Anract P, Forest M, Tomeno B. Massive pelvic and femoral pseudotumoral osteolysis secondary to an uncemented total hip arthroplasty. Int Orthop. 1999;23:37–40. doi: 10.1007/s002640050300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 203.Madan S, Jowett RL, Goodwin MI. Recurrent intrapelvic cyst complicating metal-on-metal cemented total hip arthroplasty. Arch Orthop Trauma Surg. 2000;120:508–510. doi: 10.1007/s004020000171. [DOI] [PubMed] [Google Scholar]
- 204.Mak KH, Wong TK, Poddar NC. Wear debris from total hip arthroplasty presenting as an intrapelvic mass. J Arthroplasty. 2001;16:674–676. doi: 10.1054/arth.2001.23726. [DOI] [PubMed] [Google Scholar]
- 205.Olesen Schaarup S, Varmarken JE. Intrapelvic mass in a young woman with an uncemented hip arthroplasty. Acta Orthop Belg. 2002;68:546–550. [PubMed] [Google Scholar]
- 206.Crawford JR, Van Rensburg L, Marx C. Compression of the sciatic nerve by wear debris following total hip replacement: a report of three cases. J Bone Joint Surg Br. 2003;85:1178–1180. doi: 10.1302/0301-620x.85b8.13638. [DOI] [PubMed] [Google Scholar]
- 207.Hisatome T, Yasunaga Y, Ikuta Y, Takahashi K. Hidden intrapelvic granulomatous lesions associated with total hip arthroplasty: a report of two cases. J Bone Joint Surg Am. 2003;85-A:708–710. doi: 10.2106/00004623-200304000-00019. [DOI] [PubMed] [Google Scholar]
- 208.Thienpont E, Vernaeve H. Reactive pelvic cyst following total hip arthroplasty. A case report. Acta Orthop Belg. 2003;69:292–294. [PubMed] [Google Scholar]
- 209.Butler RA, Barrack RL. Total hip wear debris presenting as lower extremity swelling. A report of two cases. J Bone Joint Surg Am. 2004;86-A:142–145. doi: 10.2106/00004623-200401000-00022. [DOI] [PubMed] [Google Scholar]
- 210.Schuh A, Werber S, Zeiler G, Craiovan B. [Femoral nerve palsy due to excessive granuloma in aseptic cup loosening in cementless total hip arthroplasty] Zentralbl Chir. 2004;129:421–423. doi: 10.1055/s-2004-820360. [DOI] [PubMed] [Google Scholar]
- 211.Davies AP, Willert HG, Campbell PA, Learmonth ID, Case CP. An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J Bone Joint Surg Am. 2005;87:18–27. doi: 10.2106/JBJS.C.00949. [DOI] [PubMed] [Google Scholar]
- 212.Hananouchi T, Saito M, Nakamura N, Yamamoto T, Yonenobu K. Huge pelvic mass secondary to wear debris causing ureteral obstruction. J Arthroplasty. 2005;20:946–949. doi: 10.1016/j.arth.2004.11.005. [DOI] [PubMed] [Google Scholar]
- 213.Nehme A, Oakes DA, Marcheix B, Gomez-Brouchet A, Puget J. Compressive intrapelvic synovial cysts: an early complication of an HA-coated cup. Clin Orthop Relat Res. 2005;(430):232–236. [PubMed] [Google Scholar]
- 214.Willert HG, Buchhorn GH, Fayyazi A, Flury R, Windler M, Köster G, Lohmann CH. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. A clinical and histomorphological study. J Bone Joint Surg Am. 2005;87:28–36. doi: 10.2106/JBJS.A.02039pp. [DOI] [PubMed] [Google Scholar]
- 215.Kohn D, Pape D. Extensive intrapelvic granuloma formation caused by ceramic fragments after revision total hip arthroplasty. J Arthroplasty. 2007;22:293–296. doi: 10.1016/j.arth.2006.01.030. [DOI] [PubMed] [Google Scholar]
- 216.Clayton RA, Beggs I, Salter DM, Grant MH, Patton JT, Porter DE. Inflammatory pseudotumor associated with femoral nerve palsy following metal-on-metal resurfacing of the hip. A case report. J Bone Joint Surg Am. 2008;90:1988–1993. doi: 10.2106/JBJS.G.00879. [DOI] [PubMed] [Google Scholar]
- 217.Harvie P, Giele H, Fang C, Ansorge O, Ostlere S, Gibbons M, Whitwell D. The treatment of femoral neuropathy due to pseudotumour caused by metal-on-metal resurfacing arthroplasty. Hip Int. 2008;18:313–320. doi: 10.1177/112070000801800408. [DOI] [PubMed] [Google Scholar]
- 218.Leigh W, O’Grady P, Lawson EM, Hung NA, Theis JC, Matheson J. Pelvic pseudotumor: an unusual presentation of an extra-articular granuloma in a well-fixed total hip arthroplasty. J Arthroplasty. 2008;23:934–938. doi: 10.1016/j.arth.2007.08.003. [DOI] [PubMed] [Google Scholar]
- 219.Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, Gibbons CL, Ostlere S, Athanasou N, Gill HS, Murray DW. Pseudotumours associated with metal-on-metal hip resurfacings. J Bone Joint Surg Br. 2008;90:847–851. doi: 10.1302/0301-620X.90B7.20213. [DOI] [PubMed] [Google Scholar]
- 220.Regis D, Sandri A, Costa A, Bartolozzi P, Mazzilli G. Recurrent femoral deep vein thrombosis: rare complication of a pelvic mass induced by polyethylene wear debris following total hip arthroplasty. A case report. Thromb Res. 2008;121:593–595. doi: 10.1016/j.thromres.2007.05.024. [DOI] [PubMed] [Google Scholar]
- 221.Lin KH, Lo NN. Failure of polyethylene in total hip arthroplasty presenting as a pelvic mass. J Arthroplasty. 2009;24:1144.e13–1144.e15. doi: 10.1016/j.arth.2008.06.029. [DOI] [PubMed] [Google Scholar]
- 222.Lax-Pérez R, Salinas-Gilabert JE, Lajara-Marco F, Lax-Pérez A, Corraliza-Zamorano A, García-Gálvez A, Izquierdo-Plazas L. [Thrombosis of the superficial femoral vein due to psoas bursitis secondary to particle disease in total hip arthroplasty] Acta Ortop Mex. 2011;25:180–183. [PubMed] [Google Scholar]
- 223.Picardo NE, Al-Khateeb H, Pollock RC. Atypical pseudotumour after metal-on-polyethylene total hip arthroplasty causing deep venous thrombosis. Hip Int. 2011;21:762–765. doi: 10.5301/HIP.2011.8839. [DOI] [PubMed] [Google Scholar]
- 224.Mann BS, Whittingham-Jones PM, Shaerf DA, Nawaz ZS, Harvie P, Hart AJ, Skinner JA. Metal-on-metal bearings, inflammatory pseudotumours and their neurological manifestations. Hip Int. 2012;22:129–136. doi: 10.5301/HIP.2012.9185. [DOI] [PubMed] [Google Scholar]
- 225.Hernández-Vaquero D, Suárez-Vazquez A. [Asymptomatic intrapelvic cyst associated to total hip arthroplasty] Med Clin (Barc) 2007;128:598–599. doi: 10.1157/13101621. [DOI] [PubMed] [Google Scholar]
- 226.Chiang CM, Tarng YW, Yao ZK, Hsu CJ, Wong CY, Huang JK. Voiding dysfunction caused by an intrapelvic synovial cyst that resulted from a screw misplaced when fixing the metal cup during total hip arthroplasty. J Orthop Sci. 2010;15:682–685. doi: 10.1007/s00776-010-1503-z. [DOI] [PubMed] [Google Scholar]
- 227.Issack PS. Formation of a large rice body-containing cyst following total hip arthroplasty. BMC Res Notes. 2012;5:294. doi: 10.1186/1756-0500-5-294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 228.Berquist TH, Bender CE, Maus TP, Ward EM, Rand JA. Pseudobursae: a useful finding in patients with painful hip arthroplasty. AJR Am J Roentgenol. 1987;148:103–106. doi: 10.2214/ajr.148.1.103. [DOI] [PubMed] [Google Scholar]
- 229.Buttaro M, González Della Valle A, Piccaluga F. Psoas abscess associated with infected total hip arthroplasty. J Arthroplasty. 2002;17:230–234. doi: 10.1054/arth.2002.28734. [DOI] [PubMed] [Google Scholar]
- 230.Legaye J, Lenfant P, Delos M. [Arthrosynovial cyst of the hip after total hip arthroplasty with a ceramic-on-ceramic interface] Rev Chir Orthop Reparatrice Appar Mot. 2004;90:475–478. doi: 10.1016/s0035-1040(04)70176-2. [DOI] [PubMed] [Google Scholar]
- 231.Howell GE. Pelvic synovial cyst formation secondary to perforation of the quadrilateral plate: a case report. J R Nav Med Serv. 1999;85:172–173. [PubMed] [Google Scholar]
- 232.Kuiken DS, ten Have BL, van Raay JJ. [A swollen leg after total hip arthroplasty] Ned Tijdschr Geneeskd. 2008;152:1634–1639. [PubMed] [Google Scholar]
- 233.Gruber FW, Böck A, Trattnig S, Lintner F, Ritschl P. Cystic lesion of the groin due to metallosis: a rare long-term complication of metal-on-metal total hip arthroplasty. J Arthroplasty. 2007;22:923–927. doi: 10.1016/j.arth.2006.10.002. [DOI] [PubMed] [Google Scholar]
- 234.Hart AJ, Satchithananda K, Liddle AD, Sabah SA, McRobbie D, Henckel J, Cobb JP, Skinner JA, Mitchell AW. Pseudotumors in association with well-functioning metal-on-metal hip prostheses: a case-control study using three-dimensional computed tomography and magnetic resonance imaging. J Bone Joint Surg Am. 2012;94:317–325. doi: 10.2106/JBJS.J.01508. [DOI] [PubMed] [Google Scholar]
- 235.Hauptfleisch J, Pandit H, Grammatopoulos G, Gill HS, Murray DW, Ostlere S. A MRI classification of periprosthetic soft tissue masses (pseudotumours) associated with metal-on-metal resurfacing hip arthroplasty. Skeletal Radiol. 2012;41:149–155. doi: 10.1007/s00256-011-1329-6. [DOI] [PubMed] [Google Scholar]
- 236.Malviya A, Holland JP. Pseudotumours associated with metal-on-metal hip resurfacing: 10-year Newcastle experience. Acta Orthop Belg. 2009;75:477–483. [PubMed] [Google Scholar]
- 237.Williams DH, Greidanus NV, Masri BA, Duncan CP, Garbuz DS. Prevalence of pseudotumor in asymptomatic patients after metal-on-metal hip arthroplasty. J Bone Joint Surg Am. 2011;93:2164–2171. doi: 10.2106/JBJS.J.01884. [DOI] [PubMed] [Google Scholar]
- 238.Lohmann CH, Singh G, Willert HG, Buchhorn GH. Metallic debris from metal-on-metal total hip arthroplasty regulates periprosthetic tissues. World J Orthop. 2014;5:660–666. doi: 10.5312/wjo.v5.i5.660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 239.Silver DA, Cassar-Pullicino VN, Morrissey BM, Etherington RJ, McCall IW. Gas-containing ganglia of the hip. Clin Radiol. 1992;46:257–260. doi: 10.1016/s0009-9260(05)80166-7. [DOI] [PubMed] [Google Scholar]
- 240.Coulier B, Cloots V. Atypical retroperitoneal extension of iliopsoas bursitis. Skeletal Radiol. 2003;32:298–301. doi: 10.1007/s00256-002-0601-1. [DOI] [PubMed] [Google Scholar]
- 241.Atkins HJ, Key JA. A case of myxomatous tumour arising in the adventitia of the left external iliac artery; case report. Br J Surg. 1947;34:426. doi: 10.1002/bjs.18003413618. [DOI] [PubMed] [Google Scholar]
- 242.Paty PS, Kaufman JL, Koslow AR, Chang BB, Leather RP, Shah DM. Adventitial cystic disease of the femoral vein: a case report and review of the literature. J Vasc Surg. 1992;15:214–217. doi: 10.1067/mva.1992.30555. [DOI] [PubMed] [Google Scholar]
- 243.Oi K, Yoshida T, Shinohara N. Rapid recurrence of cystic adventitial disease in femoral artery and an etiologic consideration for the cyst. J Vasc Surg. 2011;53:1702–1706. doi: 10.1016/j.jvs.2011.02.021. [DOI] [PubMed] [Google Scholar]
- 244.Michaelides M, Papas S, Pantziara M, Ioannidis K. High spatial resolution MRI of cystic adventitial disease of the iliofemoral vein communicating with the hip joint. Cardiovasc Intervent Radiol. 2014;37:271–274. doi: 10.1007/s00270-013-0645-8. [DOI] [PubMed] [Google Scholar]
- 245.Carr CR, Berley FV, Davis WC. Pigmented villonodular synovitis of the hip joint; a case report. J Bone Joint Surg Am. 1954;36-A:1007–1013. [PubMed] [Google Scholar]
- 246.Weisser JR, Robinson DW. Pigmented villonodular synovitis of iliopectineal bursa; a case report. J Bone Joint Surg Am. 1951;33-A:988–992. [PubMed] [Google Scholar]
- 247.Eisenberg KS, Johnston JO. Synovial chondromatosis of the hip joint presenting as an intrapelvic mass: a case report. J Bone Joint Surg Am. 1972;54:176–178. [PubMed] [Google Scholar]
- 248.Schagemann JC, Hunold P, Russlies M, Mittelstaedt H. Synovial chondromatosis of the hip with atypical MRI morphology and mistakable clinical symptoms--a case report. Acta Orthop. 2011;82:246–249. doi: 10.3109/17453674.2011.570679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 249.McCredie JA. Ganglia presenting as an irreducible femoral hernia. J R Coll Surg Edinb. 1979;24:231–233. [PubMed] [Google Scholar]
- 250.Wu CC, Liu TJ. An unusual ganglion communicating with hip joint resembling a femoral hernia. Case report. Acta Chir Scand. 1986;152:705–706. [PubMed] [Google Scholar]
- 251.Wuenschel M, Kunze B. Iliopsoas cyst causing persistent pain after total hip arthroplasty. Orthopedics. 2011;34:396. doi: 10.3928/01477447-20110317-25. [DOI] [PubMed] [Google Scholar]
- 252.Akman S, Gür B, Sülün T, Aksoy B. [A case of a ganglion cyst originating from the hip joint and surgical outcome] Acta Orthop Traumatol Turc. 2002;36:76–78. [PubMed] [Google Scholar]
- 253.Lim IG, Berger M, Bertouch J. An unusual cause of pain in both hips. Ann Rheum Dis. 2003;62:510–511. doi: 10.1136/ard.62.6.510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 254.Tebib JG, Dumontet C, Carret JP, Colson F, Bouvier M. Synovial cyst of the hip causing iliac vein and femoral nerve compression. Clin Exp Rheumatol. 1987;5:92–93. [PubMed] [Google Scholar]
- 255.Mährlein R, Weiand G, Schmelzeisen H. Ganglion of the hip: report of five cases. J South Orthop Assoc. 2001;10:1–5; discussion 5. [PubMed] [Google Scholar]
- 256.Cassina PC, Hauser M, Kossmann T, Brunner U. Juxtaacetabular ganglion as a differential diagnosis in pulsating groin masses. Vasa. 2000;29:75–76. doi: 10.1024/0301-1526.29.1.75. [DOI] [PubMed] [Google Scholar]
- 257.Tamai O, Mamadi T, Muto Y, Toda T. Large synovial cyst of the pelvis containing rice bodies. A case report. Int Orthop. 1998;22:325–327. doi: 10.1007/s002640050270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 258.Al-Khodairy AT, Gobelet C, Nançoz R, De Preux J. Iliopsoas bursitis and pseudogout of the knee mimicking L2-L3 radiculopathy: case report and review of the literature. Eur Spine J. 1997;6:336–341. doi: 10.1007/BF01142682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 259.Kim DH, Murovic JA, Tiel RL, Kline DG. Intrapelvic and thigh-level femoral nerve lesions: management and outcomes in 119 surgically treated cases. J Neurosurg. 2004;100:989–996. doi: 10.3171/jns.2004.100.6.0989. [DOI] [PubMed] [Google Scholar]
- 260.Kim DH, Kline DG. Surgical outcome for intra- and extrapelvic femoral nerve lesions. J Neurosurg. 1995;83:783–790. doi: 10.3171/jns.1995.83.5.0783. [DOI] [PubMed] [Google Scholar]
- 261.Leinung S, Schönfelder M, Würl P. [Inflammatory pseudotumor of the ileopsoas muscle with femoral paralysis caused by massive metal abrasion of a hip endoprosthesis] Chirurg. 2002;73:725–728. doi: 10.1007/s00104-002-0444-2. [DOI] [PubMed] [Google Scholar]
- 262.Campeas S, Rafii M. Pelvic presentation of a hip joint ganglion: a case report. Bull Hosp Jt Dis 2002- 2003;61:89–92. [PubMed] [Google Scholar]
- 263.Kim SH, Seok H, Lee SY, Park SW. Acetabular paralabral cyst as a rare cause of obturator neuropathy: a case report. Ann Rehabil Med. 2014;38:427–432. doi: 10.5535/arm.2014.38.3.427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 264.Juglard G, Le Nen D, Lefevre C, Leroy JP, Le Henaff B. [Synovial cyst of the hip with revealing neurologic symptoms] J Chir (Paris) 1991;128:424–427. [PubMed] [Google Scholar]
- 265.Salunke AA, Panchal R. A paralabral cyst of the hip joint causing sciatica: case report and review of literature. Malays J Med Sci. 2014;21:57–60. [PMC free article] [PubMed] [Google Scholar]
- 266.Yang G, Wen X, Gong Y, Yang C. Sciatica and claudication caused by ganglion cyst. Spine (Phila Pa 1976) 2013;38:E1701–E1703. doi: 10.1097/BRS.0000000000000024. [DOI] [PubMed] [Google Scholar]
- 267.Jones HG, Sarasin SM, Jones SA, Mullaney P. Acetabular paralabral cyst as a rare cause of sciatica. A case report. J Bone Joint Surg Am. 2009;91:2696–2699. doi: 10.2106/JBJS.H.01318. [DOI] [PubMed] [Google Scholar]
- 268.Spinner RJ, Hébert-Blouin MN, Trousdale RT, Midha R, Russell SM, Yamauchi T, Sasaki S, Amrami KK. Intraneural ganglia in the hip and pelvic region. Clinical article. J Neurosurg. 2009;111:317–325. doi: 10.3171/2009.2.JNS081720. [DOI] [PubMed] [Google Scholar]
- 269.Jiang Y, Song HW, Wang D, Yang ML. [Treatment of lumbar intervertebral disc herniation and sciatica with percutaneous transforaminal endoscopic technique] Zhongguo Gushang. 2013;26:800–804. [PubMed] [Google Scholar]
- 270.Gupta R, Stafford S, Cox N. Unusual cause of meralgia paraesthetica. Rheumatology (Oxford) 2003;42:1005. doi: 10.1093/rheumatology/keg241. [DOI] [PubMed] [Google Scholar]
- 271.Beardsmore D, Spark JI, MacAdam R, Macdonald D, Scott DJ. A psoas ganglion causing obstruction of the iliofemoral arteries. Eur J Vasc Endovasc Surg. 2000;19:554–555. doi: 10.1053/ejvs.1999.1065. [DOI] [PubMed] [Google Scholar]
- 272.Stanek F, Ouhrabkova R, Hejdova H, Zubkovsky O, Ott Z, Kvasnicka J, Janousek M. Intermittent claudication caused by a hip joint ganglion. Vasa. 2007;36:217–219. doi: 10.1024/0301-1526.36.3.217. [DOI] [PubMed] [Google Scholar]
- 273.Atkinson MH. Rheumatoid synovial cyst of the hip: an unusual cause of leg swelling. J Rheumatol. 1986;13:986–988. [PubMed] [Google Scholar]
- 274.Bhan C, Corfield L. A case of unilateral lower limb swelling secondary to a ganglion cyst. Eur J Vasc Endovasc Surg. 2007;33:371–372. doi: 10.1016/j.ejvs.2006.10.027. [DOI] [PubMed] [Google Scholar]
- 275.Bolhuis HW, Van der Werf TS, Tjabbes T, Ponsen RJ, Van de Loo RA. Giant synovial cyst of the hip joint presenting with femoral vein compression. Neth J Surg. 1990;42:88–91. [PubMed] [Google Scholar]
- 276.Colasanti M, Sapienza P, Moroni E, Mosiello G, Postacchini F, di Marzo L. An unusual case of synovial cyst of the hip joint presenting as femoral vein compression and severe lower limb edema. Eur J Vasc Endovasc Surg. 2006;32:468–470. doi: 10.1016/j.ejvs.2006.05.012. [DOI] [PubMed] [Google Scholar]
- 277.De Smedt M, Lechien P. [Synovial cyst of the hip: a rare cause of iliac vein compression] Acta Orthop Belg. 1996;62:238–240. [PubMed] [Google Scholar]
- 278.Duato Jané A, Azcona Elizalde JM, Lorente Navarro MC, Ortiz de Solórzano J. [Compression of the femoral vein caused by a synovial cyst of the hip] Angiologia. 1989;41:156–160. [PubMed] [Google Scholar]
- 279.Endo M, Sato H, Murakami S, Kidani M, Noto T. A case of pseudothrombophlebitis due to inguinal synovial cyst. Am Surg. 1990;56:533–534. [PubMed] [Google Scholar]
- 280.Gale SS, Fine M, Dosick SM, Whalen RC. Deep vein obstruction and leg swelling caused by femoral ganglion. J Vasc Surg. 1990;12:594–595. [PubMed] [Google Scholar]
- 281.Gong W, Ge F, Chen L. A giant ganglion cyst of hip joint causing lower limb edema. Saudi Med J. 2010;31:569–571. [PubMed] [Google Scholar]
- 282.Harris RW, Andros G, Dulawa LB, Oblath RW, Horowitz R. Iliofemoral venous obstruction without thrombosis. J Vasc Surg. 1987;6:594–599. doi: 10.2196/39512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 283.Julien Y, Favoulet P, Mistrih R, de Dompsure R, Trouilloud P, Cougard P. [Synovial cyst of the hip: a misleading strangulated crural hernia diagnosis] Ann Chir. 2003;128:554–556. doi: 10.1016/s0003-3944(03)00222-0. [DOI] [PubMed] [Google Scholar]
- 284.Legaye J, Redier S. [Synovial cyst of the hip. Apropos of a case manifested by venous compression] Acta Orthop Belg. 1995;61:140–143. [PubMed] [Google Scholar]
- 285.Matsumoto H, Yamamoto E, Kamiya C, Miura E, Kitaoka T, Suzuki J, Deguchi J, Yamada H, Matsumoto R, Kuroda T, et al. Femoral vein compression resulting from a ganglion of the hip joint: a case report. Ann Vasc Dis. 2012;5:233–236. doi: 10.3400/avd.cr.12.00025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286.Sugiura M, Komiyama T, Akagi D, Miyata T, Shigematsu H. Compression of the iliac vein by a synovial cyst. Ann Vasc Surg. 2004;18:369–371. doi: 10.1007/s10016-004-0025-6. [DOI] [PubMed] [Google Scholar]
- 287.Kummer E, De Senarclens P. Un cas d’hygroma chronique de la bourse du psoas-iliaque ou iliopectinee. Revue Medicale de la Suisse Romande. 1917;37:574–580. [Google Scholar]
- 288.Forster BB, Connell DG, Scudamore CH. Synovial cyst of the hip: an unusual cause of an inguinal mass. Can J Surg. 1989;32:133–134. [PubMed] [Google Scholar]
- 289.Bousquet JC, Ravaux S, Durand A. [Synovial cyst of the hip with venous compression. Diagnosis using x-ray computed tomography. A case report] J Radiol. 1990;71:623–627. [PubMed] [Google Scholar]
- 290.Clarke MD, Edwards DP, Barker P. Ganglion of the hip joint--we present a logical approach to the exploration of a mass in the femoral triangle. J R Army Med Corps. 1999;145:145–146. doi: 10.1136/jramc-145-03-09. [DOI] [PubMed] [Google Scholar]
- 291.Margreiter R, Steiner E, Mikuz G. [Synovial cysts of the hip joint] Chirurg. 1978;49:620–624. [PubMed] [Google Scholar]