

Abstract
AIM: Transcystic biliary decompression (TCBD) has been proposed as an alternative to T-tube placement after laparoscopic choledochotomy (LCD). This permits safe primary closure of the choledochotomy and eliminates the complications associated with T-tubes. TCBD tube has been secured by Roeder knots and transfixation, and removed later than 3 wk after surgery. We presented a modified TCBD (mTCBD) method after LCD using the ureteral catheter and the Lapro-Clip (David and Geck, Danbury, Connecticut, USA), and compared it with T-tube drainage.
METHODS: Between October 2002 and June 2003, patients with choledocholithiasis undergoing LCD with mTCBD (mTCBD Group, n = 30) were retrospectively compared to those undergoing LCD with T-tube drainage (T-tube Group, n = 52) at a single institution.
RESULTS: There were no significant differences in operative time and retained stones between the two groups. Patients in mTCBD group had a significantly decreased average output of bile compared with those in T-tube group (306 ± 141 vs 409 ± 243 mL/24 h, P = 0.000). Removal of drain tubes in mTCBD group was done significantly earlier than that in T-tube group (median, 5 vs 29 d, P = 0.000). No complication related to drain tubes was found in mTCBD group, and morbidity rate with the T-tube was significantly higher (11.5%), and bile leakage following T-tube removal was 5.8%.
CONCLUSION: A modified TCBD after LCD is safe, effective and easy to perform. It may reduce postoperative complications, especially bile leakage.
INTRODUCTION
Laparoscopic choledochotomy (LCD) has been proposed as an efficacious, safe, and cost-effective method for the treatment of choledocholithiasis[1-6]. However, it is associated with a relatively higher morbidity rate, mainly related to T-tube insertion[7,8]. To eliminate the complications related to T-tubes, some authors have proposed transcystic biliary decompression (TCBD) after LCD, but the TCBD tube is still removed later than 3 wk after surgery[9,10], limiting the value of the procedure. We presented a modified TCBD (mTCBD) method using ureteral catheter and Lapro-Clip, and compared it with T-tube drainage.
MATERIALS AND METHODS
Patients
Eighty-two patients with choledocholithiasis undergoing LC plus laparoscopic choledochotomy were retrospectively reviewed at a single institution, between October 2002 and June 2003. mTCBD was performed for 30 patients (mTCBD group) and T-tube drainage for 52 patients (T-tube group). The clinical and demographic details are shown in Table 1. There were no significant differences between the groups. Preoperative investigations included liver function tests and external ultrasound. Six patients had ERCP or MRCP in the mTCBD group, and three in the T-tube group. The criteria for preoperative suspicion of CBD stones were serum alkaline phosphatase or bilirubin levels twice the upper normal limit, and an ultrasonic diameter of the CBD equal to or larger than 9 mm. Patients with acute cholecystitis underwent an operation within 48 h admission. Those with choledocholithiasis associated with acute pancreatitis were operated on after the acute bout of pancreatitis was subsided. The patients were restricted to the American Society of Anesthesiology class I and class II (ASA I and II). Cases were excluded if preoperative and intraoperative endoscopic sphincterotomy (ES) were performed. Two patients had previous biliary surgery in the mTCBD group, and three in the T-tube group.
Table 1.
Clinical and demographic details of the patients
| mTCBD1 | T-tube | |
| n | 30 | 52 |
| Age range(yr) | 28-77 | 26-82 |
| Male:female | 12: 18 | 17: 35 |
| Jaundice | 12 | 16 |
| Acute cholecystitis | 9 | 13 |
| Acute pancreatitis | 3 | 5 |
| Known CBD stone (s) | 16 | 37 |
| Suspected CBD stone (s) | 11 | 13 |
| Dilated CBD (≥ 9 mm) | 18 | 35 |
| Biliary surgery | 2 | 3 |
1Modified transcystic biliary decompression.
Operative techniques
Laparoscopic cholecystectomy was performed by a standardized technique. One 10 mm port was inserted into the left upper quadrant. Intraoperative cholangiography (IOC) was mandatory. Choledochotomy was performed by a vertical incision. CBD stones were retrieved by instrumental exploration with forceps, flushing of CBD with saline, and use of a Dormia basket with a 5 mm chledochoscopy.
Modified transcystic biliary decompression (mTCBD) After complete clearance of the CBD, which was primarily closed with a running suture (3-0 vicryl). A 5Fr ureteral catheter was advanced into the CBD lumen 2 cm to 4 cm and a saline syringe was attached to the three-way stopcock external fitting of the catheter. If the position of the terminal segment of the ureteral catheter inside CBD was correct, the catheter was fixed to the cystic duct by a 12 mm absorbable Lapro-Clip (Figure 1). Saline irrigation through the catheter was maintained during application of the Lapro-Clip to prevent overtightening the catheter. A loose loop of the catheter was left. A completion IOC was performed to confirm the correct position of the ureteral catheter, also to ensure the adequate closure of the CBD and free flow of contrast into the duodenal lumen. A postoperative cholangiogram was performed on d 3 to 7 after surgery. Under fluoroscopy, the catheter was removed.
Figure 1.
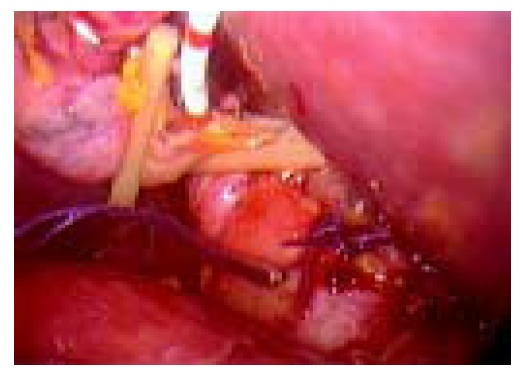
A 5 Fr ureteral catheter was placed for biliary decom-pression and secured with a 12 mm absorbable Lapro-Clip.
T-tube drainage A latex rubber T-tube of appropriate size (12-16 Fr) was inserted completely into the abdomen. The T limbs were advanced with grasping forceps into the choledochotomy. After proper positioning, the choledochotomy was closed using interrupted sutures (3-0 vicryl). T-tube clamping was carried out 7-10 d postoperatively. A postoperative cholangiogram was performed 3 to 4 wk after surgery. If the examination was normal, the T-tube was removed. If retained stones were shown, the T-tube was left for another 3 to 4 wk. A No.10 Jackson-Pratt drain was placed in the subhepatic space for all patients. The subhepatic drain tube was removed on the 3rd d for most of patients.
Five surgeons performed the 82 laparoscopic choledochotomies. In the mTCBD group, one senior author performed 25 of 30 procedures, whereas the remaining 5 procedures by one junior staff member. In the T-tube group, three senior staff performed 47 of 52 procedures, whereas 7 procedures by two junior members.
The output of bile was measured only during the hospital stay. The data recorded were insufficient in the case notes to compare the number and size of CBD stones, and postoperative liver function test.
A “drain complication” was defined as an event causing morbidity, requiring medical intervention, or resulting in a prolonged admission or requiring readmission. The complication had to be clearly related to the presence or removal of the drain.
Statistical analysis
Statistical analyses were performed using Student’s t test, chi square test for likelihood ratio, and Mann-Whitney test for nonparametric data. Significance was set at the 5% level.
RESULTS
Outcome of mTCBD group
The average operative time was 178 ± 34 min (Table 2). There were two conversions to open surgery (6.5%). One patient had large impacted stones, and the other had multiple stones. The modified transcystic biliary decompression (mTCBD) was also used in those patients. The average output of bile via the ureteral catheter was 306 ± 141 mL/24 h. The median postoperative time of drain removal was 5 (range 4 to 5) d. Under fluoroscopy, the catheter could be pulled out easily from the cystic duct without any bile leakage or slippage of the Lapro-Clip (Figure 2). No patients developed complications from ureteral catheter occlusion. The median postoperative hospital stay was 5 (range 4 to 6) d.
Table 2.
Comparison of clinical outcome between two groups
| mTCBD | T-tube | t or χ2 (z) | P | |
| Operative time (min) | 178 | 173 | -0.469 | 0.6402 |
| Output of bile (mL/24 h) | 306 | 409 | 2.118 | 0.0372 |
| Postoperative stay(d) | 5.4-61 | 4.4-61 | (-2.060) | 0.0394 |
| Drain removal (d) | 5.4-51 | 29.22-321 | (-7.560) | 0.0004 |
| Complications (%) | 0 | 11.5 | 5.736 | 0.0173 |
| Retained stones (%) | 3.3 | 13.5 | 2.574 | 0.1093 |
| Convert to open (%) | 6.5 | 3.8 | 0.315 | 0.5753 |
Median, 25%-75% quartile rang;
t-test;
χ2 test with Likelihood Ratio;
Mann-Whitney test.
Figure 2.
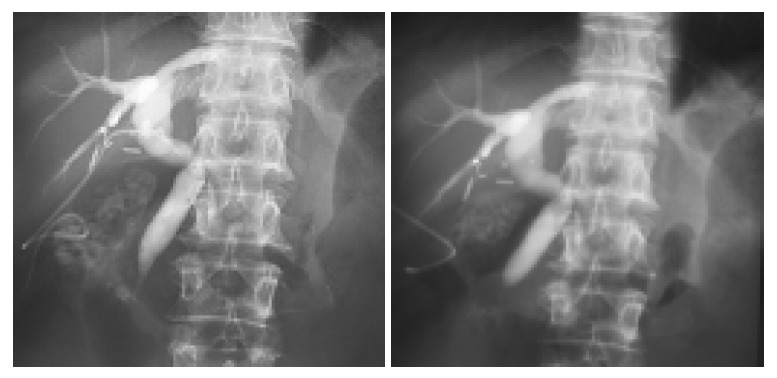
A ureteral catheter was pulled out without bile leakage. The cystic duct was closed with the Lapro-Clip.
One patient (3.3%) had unexpected retained stones, requiring endoscopic sphincterotomy (ES). Two patients had problems. The ureteral catheter was dislocated with the biliary tree not shown in the postoperative cholangiogram, but there was no bile leakage.
Outcome of T-tube group
The average operative time was 173 ± 45 min (Table 2). There were two conversions to open surgery (6.5%). Two patients had large impacted stones. The average output of bile via T-tube was 409 ± 243 mL/24 h. The median drain removal time was 29 (range 22 to 32) d. The median postoperative hospital stay was 4 (range 4 to 6) d.
Seven (13.5%) had retained stones (Table 3). There were intentionally retained stones in 5 patients (9.6%), 2 with intrahepatic duct stones, 1 with multiple common duct stones because of difficulty in removing them laparoscopically, and another 2 patients with temporary unavailability of the choledochoscope. There were unexpected residual stones in 2 patients (3.8%). All of the stones were successfully removed, 5 patients through the T-tube tract, using a choledochoscope, and a stone basket. The T-tube was taken out in two patients prior to planed removal, thereby requiring ES.
Table 3.
Retained stones in T-tube group
| n(%) | |
| Known stones | 5 (9.6) |
| Instrument problems | 2 |
| Intrahepatic stones | 2 |
| Multiple stones | 1 |
| Unexpected stones | 2 (3.8) |
| Total | 7 (13.5) |
Postoperative complications occurred in 6 patients (11.5%) (Table 4). Following T-tube removal, three patients had significant bile leakage (5.8%). Two patients developed severe abdominal pain, sweating and tachycardia and were diagnosed as localized bile collection. They were treated with antibiotics, parental fluids, analgesia, and the drain tube was reinserted through T-tube sinus tract. Recovery was achieved with this management. The third patient developed biliary peritonitis and required open drainage.
Table 4.
Complications and problems of biliary drainage
| T-tube | mTCBD | |
| Complications | ||
| n | 6 (11.5%) | 0 |
| Drain in situ | ||
| Leak around drain | 1 | 0 |
| Stricture | 1 | 0 |
| Drain pulled out | 1 | 0 |
| Drain removed | 3 (5.8%) | |
| Bile collection | 2 | 0 |
| Bile peritonitis | 1 | 0 |
| Problems | ||
| n | 3 (5.8%) | 2 (6.7%) |
| Drain out | 2 | 2 |
| Dislocation | 1 | 0 |
One patient had a CBD stricture and T-tube stenting was necessary for 3 mo. In the other patient the T-tube was pulled out on the second day after surgery and the subhepatic suction drain provided biliary drainage for two weeks postoperatively.
Other related morbidity was found in one patient with a bile leak around the T-tube. In addition, the tip of the T-tube in one patient was dislocated from the bile duct, but caused no problem.
Comparison of clinical outcome between two groups
The statistical analyses comparing the mTCBD group with the T-tube group are presented in Table 2. There were no significant differences in operative time and retained stones. Patients in mTCBD group had a significantly decreased average output of bile compared with those in T-tube group (P = 0.000). The biliary drainage tube in the mTCBD group was removed significantly earlier than that in the T-tube group (P = 0.000). No morbidity was directly related to drain tube in the mTCBD group, and the morbidity rate in the T-tube group was significantly higher (11.5%, P = 0.017). However, the postoperative hospital stay in the mTCBD group was significantly longer compared with that in the T-tube group (P = 0.039).
There was no postoperative mortality or recurrence of choledocholithiasis in this study. The length of follow-up was 4 to 30 wk.
DISCUSSION
Previous studies have documented a temporary obstruction at the lower end of the CBD due to sludge, fibrin debris, or edema following manipulations to extract duct calculi or retained stones in the first few days after surgery[9,11-16], thus temporary decompression is advisable in the prevention of postoperative bile leakage. A transcystic biliary decompression (TCBD) tube, like a T-tube, could achieve biliary decompression and has the advantage of avoiding the well-known complications of T-tubes. A TCBD tube was secured to the cystic duct with two Roeder knots or a transfixing suture. The biliary drainage tube must be kept in place for 2-4 wk[9,10]. This might not be easy to manipulate, and could reduce the benefits of the minimal access approach.
In October 2002, a modified TCBD (mTCBD) was placed followed by primary closure of the CBD. The ureteral catheter was inserted down into the CBD and once in the correct position, the cystic duct was clipped by a 12 mm Lapro-Clip. The Lapro-Clip has a two-part compression closure mechanism, the inner flexible track piece could close around the cystic duct, and rigid outer body could was then slide over the track piece to secure the cystic duct[17]. The ureteral catheter was pulled out easily with no bile leakage and the cystic duct was closed automatically with the Lapro-Clip even if drain displacement occurred.
In mTCBD group, no bile leakage was related to drain tube removal, and median time for ureteral catheter removal was 5 (range 4 to 5) d. The ureteral catheter in two patients was dislocated, this also caused no bile leakage.
Complications related to T-tubes were reported to occur between 5%-15.3%[7,18,19]. Biliary leakage following removal was the most serious. Incidence of bile leak was 4.12%-6.9%[19,20]. There was no difference when laparoscopic cases were compared to open and converted cases for overall complications (13.8% vs 15.5%) or for bile leakage after planned tube removal (6.9% vs 6.9%)[19].
In our study, postoperative complications in the T-tube group occurred in 6 patients (11.5%) (Table 4). Following T-tube removal, 3 patients developed bile leakage (5.8%). The T-tube was left in the three patients for three weeks postoperatively. Sinus tract formation of the T-tube might need a longer time because of the less reaction of laparoscopic approach[21-23]. Bile leakage was inevitable with accidental T-tube dislocation[7,18-20]. The median time for T-tube removed was 29 (range 22 to 32) d, even if cases of retained stones were excluded. The data suggest that placement of T-tube may require a longer time than 4 wk.
Biliary drainage with a TCBD tube and primary closure of the choledochotomy were indicated only for patients whose stones were completely extracted at the time of surgery. Routine intraoperative cholangiogram and chledochoscopy were used in the laparoscopic approach, and the occurrence of retained stones was decreased to accepted levels[7,24,25]. Endoscopic sphincterotomy could be a back up procedure for retained stones[25,26]. In the mTCBD group, one patient (3.3%) had unexpected retained stones retrieved by ES.
If there was any possibility of residual stones, T-tube placement was mandatory for postoperative choledochoscopy. Five patients (9.6%) in the T-tube group had intentionally retained stones (Table 3). T-tube placement may be needed for another 3-4 wk[21-23], in order to form a mature tract. It was worthwhile without any injury to the sphincter of Oddi, and complete removal could be expected.
Although patients in the mTCBD group had a significantly decreased average output of bile compared with those in the T-tube group (306 ± 141 vs 409 ± 243 mL/24 h, P = 0.000), it was shown that enough output of bile led to a decrease in the biliary pressure. Consequently, this finding suggested that the output of bile from mTCBD was sufficient to decompress the biliary tract as T-tube. On the other hand, the T-tube drain mostly was clamped on d 7 to 10, which means that many patients were discharged with an open drain.
The postoperative hospital stay in mTCBD group was significantly longer compared with that in T-tube group (median, 5 vs 4 d, P = 0.039). It may relate to the drain removal during hospitalization because of our initial trial for the mTCBD.
A modified TCBD is not suitable for patients with abnormal anatomy of cystic duct, intrahepatic duct stones and stricture of duodenal papillary.
The chief concern of the Lapro-Clip is the occlusion of the catheter. Maintaining saline irrigation through the ureteral catheter prevents occluding. We also feel that the diameter of the ureteral catheter is an important factor for avoiding occlusion or dislocation, so a 5Fr ureteral catheter is most suitable. We used a 5Fr ureteral catheter in all mTCBD cases.
A 12 mm Lapro-Clip holds the cystic duct tightly to a 5Fr ureteral catheter while the spring of the Lapro-Clip closes the cystic duct when the ureteral catheter is removed. In this study, no slippage of the clip occurred. The short period of TCBD could reduce the risk of ureteral catheter occlusion. No patients in the present study developed catheter occlusion.
Our results were similar to the use of exclusive C-tube and elastic thread described by some authors[27-30]. Our initial experiences demonstrated that the modified transcystic biliary decompression (mTCBD) after laparoscopic choledochotomy (LCD) was useful for decreasing postoperative complications, especially bile leakage, and easy to perform. The patients were discharged without any drainage tube within a wk. If biliary drainage was used carefully with selected indications, patients with laparoscopic choledochotomy for CBD stones could achieve a better postoperative quality of life. We propose mTCBD as an option for patients with CBD stones.
ACKNOWLEDGMENTS
We thank Dr. C.Welch for editorial assistance and helpful suggestions.
Footnotes
Edited by Zhang JZ and Wang XL Proofread by Xu FM
References
- 1.Cuschieri A, Lezoche E, Morino M, Croce E, Lacy A, Toouli J, Faggioni A, Ribeiro VM, Jakimowicz J, Visa J, et al. E.A.E.S. multicenter prospective randomized trial comparing two-stage vs single-stage management of patients with gallstone disease and ductal calculi. Surg Endosc. 1999;13:952–957. doi: 10.1007/s004649901145. [DOI] [PubMed] [Google Scholar]
- 2.Heili MJ, Wintz NK, Fowler DL. Choledocholithiasis: endoscopic versus laparoscopic management. Am Surg. 1999;65:135–138. [PubMed] [Google Scholar]
- 3.Wei Q, Wang JG, Li LB, Li JD. Management of choledocholithiasis: comparison between laparoscopic common bile duct exploration and intraoperative endoscopic sphincterotomy. World J Gastroenterol. 2003;9:2856–2858. doi: 10.3748/wjg.v9.i12.2856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Memon MA, Hassaballa H, Memon MI. Laparoscopic common bile duct exploration: the past, the present, and the future. Am J Surg. 2000;179:309–315. doi: 10.1016/s0002-9610(00)00346-9. [DOI] [PubMed] [Google Scholar]
- 5.Patel AP, Lokey JS, Harris JB, Sticca RP, McGill ES, Arrillaga A, Miller RS, Kopelman TR. Current management of common bile duct stones in a teaching community hospital. Am Surg. 2003;69:555–560; discussion 560-561. [PubMed] [Google Scholar]
- 6.Petelin JB. Laparoscopic common bile duct exploration. Surg Endosc. 2003;17:1705–1715. doi: 10.1007/s00464-002-8917-4. [DOI] [PubMed] [Google Scholar]
- 7.Martin IJ, Bailey IS, Rhodes M, O'Rourke N, Nathanson L, Fielding G. Towards T-tube free laparoscopic bile duct exploration: a methodologic evolution during 300 consecutive procedures. Ann Surg. 1998;228:29–34. doi: 10.1097/00000658-199807000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thompson MH, Tranter SE. All-comers policy for laparoscopic exploration of the common bile duct. Br J Surg. 2002;89:1608–1612. doi: 10.1046/j.1365-2168.2002.02298.x. [DOI] [PubMed] [Google Scholar]
- 9.Hensman C, Crosthwaite G, Cuschieri A. Transcystic biliary decompression after direct laparoscopic exploration of the common bile duct. Surg Endosc. 1997;11:1106–1110. doi: 10.1007/s004649900541. [DOI] [PubMed] [Google Scholar]
- 10.Paganini AM, Feliciotti F, Guerrieri M, Tamburini A, De Sanctis A, Campagnacci R, Lezoche E. Laparoscopic common bile duct exploration. J Laparoendosc Adv Surg Tech A. 2001;11:391–400. doi: 10.1089/10926420152761923. [DOI] [PubMed] [Google Scholar]
- 11.Holdsworth RJ, Sadek SA, Ambikar S, Cuschieri A. Dynamics of bile flow through the human choledochal sphincter following exploration of the common bile duct. World J Surg. 1989;13:300–304; discussion 305-306;. doi: 10.1007/BF01659038. [DOI] [PubMed] [Google Scholar]
- 12.DePaula AL, Hashiba K, Bafutto M, Machado C, Ferrari A, Machado MM. Results of the routine use of a modified endoprosthesis to drain the common bile duct after laparoscopic choledochotomy. Surg Endosc. 1998;12:933–935. doi: 10.1007/s004649900750. [DOI] [PubMed] [Google Scholar]
- 13.Gersin KS, Fanelli RD. Laparoscopic endobiliary stenting as an adjunct to common bile duct exploration. Surg Endosc. 1998;12:301–304. doi: 10.1007/s004649900658. [DOI] [PubMed] [Google Scholar]
- 14.Isla AM, Griniatsos J, Wan A. A technique for safe placement of a biliary endoprosthesis after laparoscopic choledochotomy. J Laparoendosc Adv Surg Tech A. 2002;12:207–211. doi: 10.1089/10926420260188128. [DOI] [PubMed] [Google Scholar]
- 15.Chen XP, Peng SY, Peng CH, Liu YB, Shi LB, Jiang XC, Shen HW, Xu YL, Fang SB, Rui J, et al. A ten-year study on non-surgical treatment of postoperative bile leakage. World J Gastroenterol. 2002;8:937–942. doi: 10.3748/wjg.v8.i5.937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yamaner S, Bilsel Y, Bulut T, Bugra D, Buyukuncu Y, Akyuz A, Sokucu N. Endoscopic diagnosis and management of complications following surgery for gallstones. Surg Endosc. 2002;16:1685–1690. doi: 10.1007/s00464-002-9048-7. [DOI] [PubMed] [Google Scholar]
- 17.Darzi A, Soin B, Coleman J, Lirici NM, Angelini L. Initial experience with an absorbable laparoscopic ligation clip. Br J Surg. 1997;84:974–976. doi: 10.1002/bjs.1800840718. [DOI] [PubMed] [Google Scholar]
- 18.Moreaux J. Traditional surgical management of common bile duct stones: a prospective study during a 20-year experience. Am J Surg. 1995;169:220–226. doi: 10.1016/S0002-9610(99)80141-X. [DOI] [PubMed] [Google Scholar]
- 19.Wills VL, Gibson K, Karihaloot C, Jorgensen JO. Complications of biliary T-tubes after choledochotomy. ANZ J Surg. 2002;72:177–180. doi: 10.1046/j.1445-2197.2002.02308.x. [DOI] [PubMed] [Google Scholar]
- 20.Gharaibeh KI, Heiss HA. Biliary leakage following T-tube removal. Int Surg. 2000;85:57–63. [PubMed] [Google Scholar]
- 21.Schippers E, Tittel A, Ottinger A, Schumpelick V. Laparoscopy versus laparotomy: comparison of adhesion-formation after bowel resection in a canine model. Dig Surg. 1998;15:145–147. doi: 10.1159/000018608. [DOI] [PubMed] [Google Scholar]
- 22.Tittel A, Treutner KH, Titkova S, Ottinger A, Schumpelick V. Comparison of adhesion reformation after laparoscopic and conventional adhesiolysis in an animal model. Langenbecks Arch Surg. 2001;386:141–145. doi: 10.1007/s004230000190. [DOI] [PubMed] [Google Scholar]
- 23.Polymeneas G, Theodosopoulos T, Stamatiadis A, Kourias E. A comparative study of postoperative adhesion formation after laparoscopic vs open cholecystectomy. Surg Endosc. 2001;15:41–43. doi: 10.1007/s004640000269. [DOI] [PubMed] [Google Scholar]
- 24.Riciardi R, Islam S, Canete JJ, Arcand PL, Stoker ME. Effectiveness and long-term results of laparoscopic common bile duct exploration. Surg Endosc. 2003;17:19–22. doi: 10.1007/s00464-002-8925-4. [DOI] [PubMed] [Google Scholar]
- 25.Hawasli A, Lloyd L, Cacucci B. Management of choledocholithiasis in the era of laparoscopic surgery. Am Surg. 2000;66:425–430; discussion 430-431. [PubMed] [Google Scholar]
- 26.Yamakawa T, Sakai S, Mu ZB, Pineres G. Laparoscopic management of common bile duct stones. J Hepatobiliary Pancreat Surg. 2000;7:9–14. doi: 10.1007/s005340050147. [DOI] [PubMed] [Google Scholar]
- 27.Fujimura M, Hirano M, Sato I, Kinoshita T, Yamamoto I, Nishimura K, Takahara H, Yamamoto A. [The C tube in biliary surgery--its development and clinical application] Nihon Geka Hokan. 2000;68:85–122. [PubMed] [Google Scholar]
- 28.Shimizu S, Yokohata K, Mizumoto K, Yamaguchi K, Chijiiwa K, Tanaka M. Laparoscopic choledochotomy for bile duct stones. J Hepatobiliary Pancreat Surg. 2002;9:201–205. doi: 10.1007/s005340200019. [DOI] [PubMed] [Google Scholar]
- 29.Tokumura H, Umezawa A, Cao H, Sakamoto N, Imaoka Y, Ouchi A, Yamamoto K. Laparoscopic management of common bile duct stones: transcystic approach and choledochotomy. J Hepatobiliary Pancreat Surg. 2002;9:206–212. doi: 10.1007/s005340200020. [DOI] [PubMed] [Google Scholar]
- 30.Hotta T, Taniguchi K, Kobayashi Y, Johata K, Sahara M, Naka T, Maeda T, Tanimura H. Biliary drainage tube evaluation after common bile duct exploration for choledocholithiasis. Hepatogastroenterology. 2003;50:315–321. [PubMed] [Google Scholar]