

Abstract
We reported a case of 79-year old woman with known large bowel diverticulosis presenting with small bowel obstruction due to stone impaction - found on plain abdominal X-ray. Contrast studies demonstrated small bowel diverticulosis. At laparotomy, the gall bladder was normal with no stones and no abnormal communication with small bowel - excluding the possibility of a gallstone ileus. Analysis of the stone revealed a composition of bile pigments and calcium oxalate. This was a rare case of small bowel obstruction due to enterolith formation - made distinctive by calcification (previously unreported in the proximal small bowel).
INTRODUCTION
Diverticulosis of the small bowel (excluding Meckel’s) is uncommon - being found in less than 5% of post-mortem examinations, although the prevalence increases with age[1]. The condition can be complicated by diverticulitis, haemorrhage or perforation[2,3]. Small bowel obstruction due to an enterolith formed and extruded from a diverticulum is a rare complication[4-6].
Enteroliths form in small bowel diverticula either de novo or around a central nidus such as a fruit stone or undigested vegetable matter (the latter is termed a bezoar). The usual composition of true enteroliths is choleic acid[7] - an end product of bile salt metabolism - postulated to form as a result of acidic pH shift within a small bowel diverticulum. Radiological diagnosis of such stones is rare, unless calcified (which usually occurs only in the more alkaline ileum)[7]. Diagnosis is therefore made at laparotomy with the presence of the stone, diverticula and the finding of a normal gall bladder (excluding a gallstone ileus). It is unclear how stones are extruded from small bowel diverticula lacking a muscular coat, but larger stones will be extruded and pass distally to cause obstruction - an enterolith ileus.
CASE REPORT
A 79-year-old lady presented with a two-day history of vomiting and central, colicky abdominal pain. She had been constipated prior to this episode and had taken senna with only a little effect on the previous day. She had a known history of sigmoid diverticular disease and had been admitted only once previously for suspected diverticulitis. She appeared dehydrated with fever of 37.6 degrees. Her abdomen was distended but soft with some central and left-sided tenderness. Bowel sounds were heard and digital rectal examination was unremarkable. Blood tests revealed a white cell count of 21.6 × 109/L without other abnormality. A plain abdominal film demonstrated opacity on the left side (Figure 1) and a gastrografin study revealed numerous small bowel diverticula of varying sizes. The opacity now was presumed to be a stone, was noted within the small bowel (Figure 2).
Figure 1.

Radio-opaque stone was clearly seen in the plain abdominal radiograph (arrow).
Figure 2.
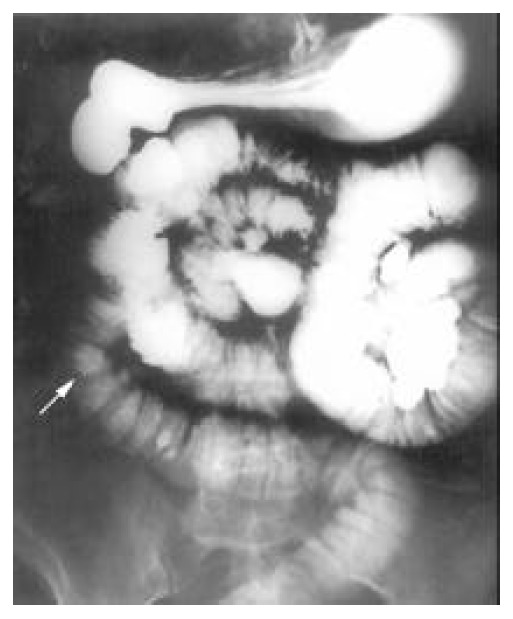
Contrast study (105 mins) demonstrated multiple jejunal diverticula and minimal passage of barium beyond the mid-jejunum. Stone was still visible (arrow).
At laparotomy, the presence of large jejunal diverticula was confirmed and the stone was found impacted in the mid-jejunum. The gall bladder appeared normal without stones. The stone approximately 3 × 4 cm and weighing 10.60 g appeared greyish and hard which was removed via a small enterotomy close to it. The patient made a good recovery from operation, delayed only by post-operative nausea. Analysis of the stone revealed a composition of bile pigments and calcium oxalate.
DISCUSSION
We reported the first case of proximal small bowel obstruction due to a calcified enterolith. It is postulated that diverticulas provide the more acidic environment necessary for choleic acid precipitation and stone formation[7]. However calcification cannot occur without an alkaline pH shift, which normally occurs in the ileum. Our case confirmed calcification occurring in the proximal small bowel which made this theory less definitive but facilitated the diagnosis.
The consensus management of enterolith ileus at laparotomy is to first attempt manual lysis of the stone without enterotomy and to milk the smaller parts into the colon where they are passed through rectum[8]. If this is proved to be impossible or inappropriate, the stone is removed through an enterotomy which is made in a less edematous segment of proximal small bowel.
The rarity of enterolith small bowel obstruction is well recognised with the condition occurring in conjunction with cases of diverticulosis. However the diagnosis should be considered in patients presenting with clinical features of small bowel obstruction without evidence of previous abdominal surgery or incarcerated hernia.
Footnotes
Edited by Xu XQ
References
- 1.NOER T. Non-Meckelian diverticula of the small bowel. The incidence in an autopsy material. Acta Chir Scand. 1960;120:175–179. [PubMed] [Google Scholar]
- 2.Longo WE, Vernava AM. Clinical implications of jejunoileal diverticular disease. Dis Colon Rectum. 1992;35:381–388. doi: 10.1007/BF02048119. [DOI] [PubMed] [Google Scholar]
- 3.Sibille A, Willocx R. Jejunal diverticulitis. Am J Gastroenterol. 1992;87:655–658. [PubMed] [Google Scholar]
- 4.Yang HK, Fondacaro PF. Enterolith ileus: a rare complication of duodenal diverticula. Am J Gastroenterol. 1992;87:1846–1848. [PubMed] [Google Scholar]
- 5.Ishizuka D, Shirai Y, Hatakeyama K. Duodenal obstruction caused by gallstone impaction into an intraluminal duodenal diverticulum. Am J Gastroenterol. 1997;92:182–183. [PubMed] [Google Scholar]
- 6.Klingler PJ, Seelig MH, Floch NR, Branton SA, Metzger PP. Small-intestinal enteroliths--unusual cause of small-intestinal obstruction: report of three cases. Dis Colon Rectum. 1999;42:676–679. doi: 10.1007/BF02234149. [DOI] [PubMed] [Google Scholar]
- 7.Shocket E, Simon SA. Small bowel obstruction due to enterolith (bezoar) formed in a duodenal diverticulum: a case report and review of the literature. Am J Gastroenterol. 1982;77:621–624. [PubMed] [Google Scholar]
- 8.Yang HK, Fondacaro PF. Enterolith ileus: a rare complication of duodenal diverticula. Am J Gastroenterol. 1992;87:1846–1848. [PubMed] [Google Scholar]