

Abstract
AIM: To clarify whether perimuscular connective tissue contains more lymphatic vessels than the shallower layers in human gallbladders.
METHODS: Lymphatic vessels were stained immunohistochemically with monoclonal antibody D2-40, which is a specific marker of lymphatic endothelium, in representative sections of 12 normal human gallbladders obtained at the time of resection for colorectal carcinoma liver metastases. In individual gallbladder specimens, nine high-power (× 200) fields with the highest lymphatic vessel density (LVD), termed “hot spots”, were identified for each layer (mucosa, muscle layer, and perimuscular connective tissue). In individual hot spots, the LVD and relative lymphatic vessel area (LVA) were measured microscopically using a computer-aided image analysis system. The mean LVD and LVA values for the nine hot spots in each layer were used for statistical analyses.
RESULTS: In the mucosa, muscle layer, and perimuscular connective tissue, the LVD was 16.1 ± 9.2, 35.4 ± 15.7, and 65.5 ± 12.2, respectively, and the LVA was 0.4 ± 0.4, 2.1 ± 1.1, and 9.4 ± 2.6, respectively. Thus, both the LVD and LVA differed significantly (P < 0.001 and P < 0.001, respectively; Kruskal-Wallis test) among the individual layers of the wall of the gallbladder, with the highest LVD and LVA values in the perimuscular connective tissue. Most (98 of 108) of the hot spots within the perimuscular connective tissue were located within 500 μm of the lower border of the muscle layer.
CONCLUSION: The perimuscular connective tissue contains more and larger lymphatic vessels than the shallower layers in the human gallbladder. This observation partly explains why the incidence of lymph node metastasis is high in T2 (tumor invading the perimuscular connective tissue) or more advanced gallbladder carcinoma.
Keywords: Gallbladder, Lymphatic vessels, Monoclonal antibody D2-40, Gallbladder neoplasms, Lymphatic metastasis
INTRODUCTION
Gallbladder carcinoma is a highly lethal disease[1,2]. Lymph node metastasis occurs early and is a major reason for the dismal prognosis for this disease[3-5]. The incidence of lymph node metastasis increases with the depth of penetration of the primary tumor; it ranges from 0% to 8%[5-9] for tumors that are limited to the mucosa or muscle layer (T1 disease according to the TNM staging system[10]), whereas it ranges from 33% to 62%[5-7,9,11,12] for tumors that have invaded the perimuscular connective tissue (T2 disease). This suggests that lymph node metastasis is frequent once the primary tumor has invaded the perimuscular connective tissue of the gallbladder.
The architecture of the lymphatic system of the gallbladder has been examined in various experimental animals, and a well-developed set of lymph channels has been described in the perimuscular connective tissue[13,14]. In 1989, Kambayashi reported similar findings for canine gallbladders[15]. The current study was conducted to clarify immunohistochemically whether the perimuscular connective tissue contains more lymphatic vessels than the mucosa or muscle layer of normal human gallbladders, using monoclonal antibody D2-40, which is a specific marker of the lymphatic endothelium[16-19], and a computer-aided image analysis system. The goal of the present study was to suggest the hypothesis that the presence of more and larger lymphatic vessels in the perimuscular connective tissue is linked to the reported high incidences of lymph node metastasis in T2 (tumor invading the perimuscular connective tissue) or more advanced gallbladder carcinoma[5-7,9,11].
MATERIALS AND METHODS
Twelve patients with colorectal carcinoma liver metastases underwent partial hepatectomy combined with cholecystectomy between January and December, 2005. The patient group included eight men and four women, with a median age of 68.5 years (range, 42-80 years). None of the patients had a history of biliary disease or chronic liver disease. The gallbladder specimens obtained from the patients, all of whom gave informed consent for histologically examining the specimens, were included in the present study.
Individual resected specimens were submitted to the Department of Surgical Pathology in our hospital for gross or histologic examination, which revealed that none of the liver tumors involved the gallbladders. The gallbladders (n = 12) were opened and examined grossly by experienced surgical pathologists, who found neither mucosal lesions nor gallstones in any of the viscera. The gallbladder specimens were then fixed in formalin. A single longitudinal representative section, which passed through both the tip of the fundus of the gallbladder and the cystic bile duct, was cut from each gallbladder specimen and embedded in paraffin. Routine histologic examination with hematoxylin and eosin staining detected no abnormalities in any of the representative sections.
Anatomy of the gallbladder
The gallbladder is divided into three equal parts: the fundus, body, and neck. Histologically, the wall of the viscus comprises three layers: the mucosa, muscle layer, and perimuscular connective tissue (subserosal layer)[10].
Lymphatic vessel parameters
Lymphatic vessel density (LVD) was defined as the number of lymphatic vessels per mm2; a high-power (× 200) field with the highest LVD in an area was referred to as a “hot spot”, in line with earlier studies[20,21]. Relative lymphatic vessel area (LVA) was defined as the percentage of positively stained lymphatic vessel area in a hot spot[20,21].
Immunohistochemistry
The paraffin-embedded blocks of the representative sections (n = 12) were used for immunohistochemistry. Three serial sections (3 μm thickness) were cut from each block: one for routine histologic examination using hematoxylin and eosin staining, one for immunohistochemical staining with monoclonal antibody D2-40, and one as a negative control.
The mouse monoclonal antibody D2-40 (Signet Laboratories, Inc., Dedham, MA) was used at a dilution of 1:200. The streptavidin-biotin immunoperoxidase method was used for detecting immune complexes. The sections were deparaffinized and rehydrated, then microwaved at 500 W for 7 cycles of 3 min each in 10 mmol/L citrate buffer (pH 6.0) to retrieve antigenic activity. After blocking of endogenous peroxidase, the sections were incubated overnight at 4°C with D2-40. The sections were then incubated at room temperature for 30 min with goat anti-mouse immunoglobulin conjugated to a peroxidase-labeled amino acid polymer, as provided in the SAB-PO (M) Kit (Nichirei Biosciences Inc., Tokyo, Japan). Diaminobenzidine was used as the chromogen, and the sections were counterstained with hematoxylin. Negative controls were treated in the same manner, except that incubation with the primary antibody was omitted. Sections of normal human tonsil were used as positive controls.
Computer-assisted morphometry of lymphatic vessels
The representative sections stained with the D2-40 antibody (n = 12) were examined for LVD and LVA using an Olympus FX 380 microscope (Olympus Co. Ltd., Tokyo, Japan). By scanning each representative section at low power (× 20), a total of nine hot spots, three for each part of the gallbladder (fundus, body, and neck), was identified per layer (mucosa, muscle layer, and perimuscular connective tissue) of the gallbladder. In individual hot spots, the outlines of individual immunohistochemically stained lymphatic vessels were identified and traced using a computer-aided image analysis system (FlvFs, ver 1.10; Flovel Co. Ltd., Tokyo, Japan) at × 200 magnification, to measure LVD and LVA.
Statistical analysis
The mean LVD and LVA for the nine hot spots per each layer (or per each part) of the gallbladder were subjected to statistical analyses. The Kruskal-Wallis test was used to compare the lymphatic vessel parameters (LVD and LVA) among individual layers (or individual parts). Statistical evaluations were performed using the SPSS 11.5J software package (SPSS Japan Inc., Tokyo, Japan). A P value < 0.05 was considered to be statistically significant.
RESULTS
D2-40 antibody-positive lymphatic vessels were found in all 12 gallbladder specimens (Figure 1). Computer-assisted morphometric analysis of the lymphatic vessels showed that both the LVD and LVA values differed significantly (P < 0.001 and P < 0.001, respectively) among the individual layers of the wall of the gallbladder, with the highest LVD and LVA values found in the perimuscular connective tissue (Table 1). Most (98 of 108) of the hot spots within the perimuscular connective tissue were located within 500 μm of the lower border of the muscle layer (Figure 1). The LVD and LVA values did not differ among the fundus, body, and neck (data not shown; P = 0.837 and P = 0.756, respectively).
Figure 1.
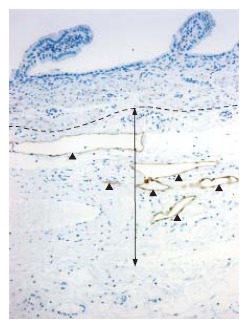
D2-40 antibody-positive lymphatic vessels in the wall of a human gallbladder. The perimuscular connective tissue contains more and larger lymphatic vessels (arrowheads), most of which are located within 500 μm (two-headed arrow) of the lower border of the muscle layer (broken line), than the mucosa or muscle layer (Original magnification, × 100).
Table 1.
LVD and LVA values for individual layers of the wall of the gallbladder (mean ± SD, n = 12)
| Layer of the wall of the gallbladder | LVD (per mm2) | P valuea | LVA (%) | P valuea |
| Mucosa | 16.1 ± 9.2 | < 0.001b | 0.4 ± 0.4 | < 0.001b |
| Muscle layer | 35.4 ± 15.7 | 2.1 ± 1.1 | ||
| Perimuscular connective tissue | 65.5 ± 12.2 | 9.4 ± 2.6 |
LVD: lymphatic vessel density; LVA: relative lymphatic vessel are;
Kruskal-Wallis test,
P < 0.001 between mucosa, muscle and perimuscular connective tissue of the gallbladder for both LVD and LVA.
DISCUSSION
The monoclonal antibody D2-40, which was generated against an oncofetal antigen that is expressed in fetal testes and in testicular germ cell tumors, is recognized as a highly specific lymphatic marker that does not react with the vascular endothelium[16-19]. Although it is difficult or sometimes impossible to distinguish morphologically lymphatic vessels from venules or capillaries on routine histologic examination, immunohistochemical staining using D2-40 enables easy identification of lymphatic vessels[16-19]. Using this method, we have clearly demonstrated that the LVD and LVA values are significantly higher in the perimuscular connective tissue than in the mucosa or muscle layer of normal human gallbladders.
A tumor that invades the deep layers of the gallbladder generally shows a higher histologic grade (less differentiation) than a superficial tumor[5,7]. It is very likely that a less-differentiated tumor that invades the perimuscular connective tissue (T2 disease) causes a higher incidence of nodal involvement than a differentiated tumor within the superficial layers (T1 disease). Another explanation for the high incidences of nodal disease in T2 gallbladder carcinoma is the higher abundance of vessels in the perimuscular connective tissue than in the shallower layers[15,22], as clearly demonstrated in the present study. The presence of more and larger lymphatic vessels in the perimuscular connective tissue (Figure 1) may increase the likelihood that the tumor will permeate the lymphatic vessels. The hot spots were prominent in the shallow (≤ 500 μm) zone of the perimuscular connective tissue of the gallbladder (Figure 1); this observation may partly explain why lymph node metastasis often occurs even in tumors with shallow (≤ 2 mm) subserosal invasion[12].
The results of the current study may provide a basis for the investigation of lymphangiogenesis in gallbladder carcinoma. Recent evidence suggests that lymphangiogenesis plays a key role in the development of nodal metastases from various human malignancies, including head and neck squamous cell carcinoma[21], cutaneous melanoma[20,23], breast carcinoma[24], and colorectal carcinoma[25]. However, to the best of the knowledge, no investigations of this type have been conducted on gallbladder carcinoma. Further investigations into the role of lymphangiogenesis in gallbladder carcinoma are warranted.
The limitations of the present study include the retrospective nature of the analysis, the low number of specimens examined, and the gallbladder specimens taken from patients with colorectal carcinoma liver metastases. Despite these limitations, the present work more clearly defines than earlier studies the abundance of lymphatic vessels in the perimuscular connective tissue of the human gallbladder.
In conclusion, the perimuscular connective tissue (subserosal layer) has more and larger lymphatic vessels than the shallower layers of the human gallbladder. This observation partly explains why the incidence of lymph node metastasis is high in T2 (tumor invading the perimuscular connective tissue) or more advanced gallbladder carcinoma.
ACKNOWLEDGMENTS
We thank Kazue Kobayashi, Ayako Sato and Naoyuki Yamaguchi for technical assistance.
Footnotes
S- Editor Zhu LH L- Editor Rippe RA E- Editor Li JL
References
- 1.Pitt HA, Dooley WC, Yeo CJ, Cameron JL. Malignancies of the biliary tree. Curr Probl Surg. 1995;32:1–90. doi: 10.1016/s0011-3840(05)80011-5. [DOI] [PubMed] [Google Scholar]
- 2.Misra S, Chaturvedi A, Misra NC, Sharma ID. Carcinoma of the gallbladder. Lancet Oncol. 2003;4:167–176. doi: 10.1016/s1470-2045(03)01021-0. [DOI] [PubMed] [Google Scholar]
- 3.Fahim RB, McDonald JR, Richards JC, Ferris DO. Carcinoma of the gallbladder: a study of its modes of spread. Ann Surg. 1962;156:114–124. doi: 10.1097/00000658-196207000-00021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shirai Y, Wakai T, Hatakeyama K. Radical lymph node dissection for gallbladder cancer: indications and limitations. Surg Oncol Clin N Am. 2007;16:221–232. doi: 10.1016/j.soc.2006.10.011. [DOI] [PubMed] [Google Scholar]
- 5.Tsukada K, Kurosaki I, Uchida K, Shirai Y, Oohashi Y, Yokoyama N, Watanabe H, Hatakeyama K. Lymph node spread from carcinoma of the gallbladder. Cancer. 1997;80:661–667. [PubMed] [Google Scholar]
- 6.Fong Y, Jarnagin W, Blumgart LH. Gallbladder cancer: comparison of patients presenting initially for definitive operation with those presenting after prior noncurative intervention. Ann Surg. 2000;232:557–569. doi: 10.1097/00000658-200010000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ogura Y, Mizumoto R, Isaji S, Kusuda T, Matsuda S, Tabata M. Radical operations for carcinoma of the gallbladder: present status in Japan. World J Surg. 1991;15:337–343. doi: 10.1007/BF01658725. [DOI] [PubMed] [Google Scholar]
- 8.Shirai Y, Yoshida K, Tsukada K, Muto T, Watanabe H. Early carcinoma of the gallbladder. Eur J Surg. 1992;158:545–548. [PubMed] [Google Scholar]
- 9.Shimada H, Endo I, Togo S, Nakano A, Izumi T, Nakagawara G. The role of lymph node dissection in the treatment of gallbladder carcinoma. Cancer. 1997;79:892–899. doi: 10.1002/(sici)1097-0142(19970301)79:5<892::aid-cncr4>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 10.Greene FL, Page DL, Fleming ID, Fritz A, Balch CM, Haller DG, Morrow M. AJCC Cancer Staging Manual. 6th ed. New York: Springer-Verlag; 2002. pp. 145–150. [Google Scholar]
- 11.Bartlett DL, Fong Y, Fortner JG, Brennan MF, Blumgart LH. Long-term results after resection for gallbladder cancer. Implications for staging and management. Ann Surg. 1996;224:639–646. doi: 10.1097/00000658-199611000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wakai T, Shirai Y, Yokoyama N, Ajioka Y, Watanabe H, Hatakeyama K. Depth of subserosal invasion predicts long-term survival after resection in patients with T2 gallbladder carcinoma. Ann Surg Oncol. 2003;10:447–454. doi: 10.1245/aso.2003.06.014. [DOI] [PubMed] [Google Scholar]
- 13.Sudler MT. The architecture of the gall-bladder. Bull Johns Hopkins Hosp. 1901;12:126. [Google Scholar]
- 14.Winkenwerder WL. A study of the lymphatics of the gall-bladder of the cat. Bull Johns Hopkins Hosp. 1927;41:226. [Google Scholar]
- 15.Kambayashi M. Lymphatic and vascular systems of the gallbladder--with special reference to carcinoma of the gallbladder. Hokkaido Igaku Zasshi. 1989;64:618–629. [PubMed] [Google Scholar]
- 16.Marks A, Sutherland DR, Bailey D, Iglesias J, Law J, Lei M, Yeger H, Banerjee D, Baumal R. Characterization and distribution of an oncofetal antigen (M2A antigen) expressed on testicular germ cell tumours. Br J Cancer. 1999;80:569–578. doi: 10.1038/sj.bjc.6690393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kahn HJ, Bailey D, Marks A. Monoclonal antibody D2-40, a new marker of lymphatic endothelium, reacts with Kaposi's sarcoma and a subset of angiosarcomas. Mod Pathol. 2002;15:434–440. doi: 10.1038/modpathol.3880543. [DOI] [PubMed] [Google Scholar]
- 18.Kahn HJ, Marks A. A new monoclonal antibody, D2-40, for detection of lymphatic invasion in primary tumors. Lab Invest. 2002;82:1255–1257. doi: 10.1097/01.lab.0000028824.03032.ab. [DOI] [PubMed] [Google Scholar]
- 19.Fogt F, Zimmerman RL, Daly T, Gausas RE. Observation of lymphatic vessels in orbital fat of patients with inflammatory conditions: a form fruste of lymphangiogenesis? Int J Mol Med. 2004;13:681–683. doi: 10.3892/ijmm.13.5.681. [DOI] [PubMed] [Google Scholar]
- 20.Dadras SS, Paul T, Bertoncini J, Brown LF, Muzikansky A, Jackson DG, Ellwanger U, Garbe C, Mihm MC, Detmar M. Tumor lymphangiogenesis: a novel prognostic indicator for cutaneous melanoma metastasis and survival. Am J Pathol. 2003;162:1951–1960. doi: 10.1016/S0002-9440(10)64328-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Franchi A, Gallo O, Massi D, Baroni G, Santucci M. Tumor lymphangiogenesis in head and neck squamous cell carcinoma: a morphometric study with clinical correlations. Cancer. 2004;101:973–978. doi: 10.1002/cncr.20454. [DOI] [PubMed] [Google Scholar]
- 22.Albores-Saavedra J, Henson DE, Klimstra D. Tumors of the Gallbladder and Extrahepatic Bile Ducts, and Ampulla of Vater. Atlas of Tumor Pathology, 3rd series. Washington, DC: Armed Forces Institute of Pathology; 2000. pp. 61–114. [Google Scholar]
- 23.Giorgadze TA, Zhang PJ, Pasha T, Coogan PS, Acs G, Elder DE, Xu X. Lymphatic vessel density is significantly increased in melanoma. J Cutan Pathol. 2004;31:672–677. doi: 10.1111/j.0303-6987.2004.00249.x. [DOI] [PubMed] [Google Scholar]
- 24.Skobe M, Hawighorst T, Jackson DG, Prevo R, Janes L, Velasco P, Riccardi L, Alitalo K, Claffey K, Detmar M. Induction of tumor lymphangiogenesis by VEGF-C promotes breast cancer metastasis. Nat Med. 2001;7:192–198. doi: 10.1038/84643. [DOI] [PubMed] [Google Scholar]
- 25.Jia YT, Li ZX, He YT, Liang W, Yang HC, Ma HJ. Expression of vascular endothelial growth factor-C and the relationship between lymphangiogenesis and lymphatic metastasis in colorectal cancer. World J Gastroenterol. 2004;10:3261–3263. doi: 10.3748/wjg.v10.i22.3261. [DOI] [PMC free article] [PubMed] [Google Scholar]