

Abstract
Patients with inflammatory bowel disease have normal life expectancy and, due to modern immunosuppressive therapies, also a normal quality of life. Since mostly young people are affected, their social behaviour suits this environment. Alcohol binging is an increasingly disturbing factor among young people. We describe a patient with Crohn’s disease, treated with azathioprine, who developed peliosis hepatis after three epsiodes of alcohol binging. Liver toxicity was not observed previously during the course of the treatment. Azathioprine-induced peliosis hepatis is thought to be idiosyncratic in humans. From animal studies, however, it is clear that hepatic depletion of glutathione leads to azathioprine toxicity to the sinusoidal endothelial cells. Damage of these cells causes peliosis hepatis. Since alcohol binging leads to hepatic glutathione depletion, we conclude that in our patient the episodes of binging have reduced liver gluathione content and therefore this has increased azathioprine toxicity causing peliosis hepatis. The problem of alcohol binging has not yet been addressed in IBD patients undertaking immunosuppressive therapy. This should be reviewed in future considerations regarding patients advice.
Keywords: Inflammatory bowel disease, Treatment, Side effects, Alcohol, Liver
INTRODUCTION
Patients with inflammatory bowel disease (IBD) have normal life expectancy and, due to modern immunosuppressive therapies, also a normal quality of life[1,2]. Since young people are often affected, their social behaviour suits this environment[3]. Alcohol binging is an increasingly disturbing factor among young people[4] and also occurs in treated IBD patients. However, there is little information about the toxicity of drugs used in IBD patients during alcohol binging. Azathioprine is frequently used as immunosuppressant in IBD. Adverse effects occur in 15% to 30% of patients[5]. Hepatotoxicity is a rare but important complication of this drug. In the liver, three syndromes can be grouped: hypersensitivity, idiosyncratic cholestatic reaction, and endothelial cell injury. Liver endothelial cell injury presents with portal hypertension caused by venoocclusive disease or peliosis hepatis[6]. Here we describe a patient with IBD who developed peliosis hepatis during azathioprine therapy most likely due to concomitant alcohol binging.
CASE REPORT
In 1996, the diagnosis of Crohn’s disease was made in a 37-year-old male after a right hemicolectomy with resection of the terminal ileum. He was treated with mesalazine. In September 2005, the patient presented us with an incomplete intestinal cutaneous fistula originating from the anastomosis. He was treated with metronidazole and immunosuppression was begun with steroids (prednisolon 60 mg/d) and azathioprine (2.5 mg/kg body weight per day), mesalazine was stopped. The fistula disappeared and steroids were tapered to zero in the course of the following weeks. In April 2006, liver enzymes were within normal limits, as were white and red blood counts under azathioprine medication. At the end of July, the patient experienced an episode of ethanol binging at a local festival with intake of 800 g alcohol (11 g/kg body weight) over 3 d. The consumption of comparable amounts of alcohol had been uneventful in the former years. In August, he had two episodes of binging with intake of 20 g per day (0.3 g/kg body weight). At the end of October, he developed progressive fatigue, abdominal discomfort and pruritus. Laboratory values showed pancytopenia [WBC 2.1 × 103/μL (normal range 3.6-9.6 × 103/μL), platelets 66 × 103/μL (normal range 150-400 × 103/μL), erythrocytes 2.53 × 106/μL (normal range 4.5-5.9 × 106/μL)] and elevated gammaglutamytransferase (121 U/L, normal value < 66 U/L), alkaline phosphatase (220 U/L, normal value < 129 U/L) and total bilirubin (4.03 mg/dL, normal value < 1.10 mg/dL). Transaminases were normal. Thiopurine-methyl-transferase (TMA) activity was 44 nmol/g Hb × h (normal value > 20 nmol/g Hb × h). Hyaluronic acid levels were 166 ng/mL (normal value < 100 ng/mL). Ultrasound showed an enlarged liver with a macronodular surface (Figure 1) and an enlarged spleen. The diagnosis of cholestatic hepatitis with portal hypertension and related pancytopenia was made. Viral, autoimmune and hereditary causes of liver disease were serologically excluded, chronic alcohol intake was negated. Simultaneously the patient developed signs of small bowel obstruction with the presence of dilated jejunal loops. Steroid pulse therapy was administered and azathioprine was stopped. A liver biopsy was performed, which showed a sinusoidal ectasia in zone II and III without venous obliterations, minimal portal tract fibrosis without bile duct alterations (Figure 2). No cirrhotic change was noted. Thus, a diagnosis of peliosis hepatis was made. After withdrawal of azathioprine, the patient’s condition improved, pancytopenia disappeared and bilirubin values returned to normal. A liver biopsy to document histological resolution was not performed.
Figure 1.
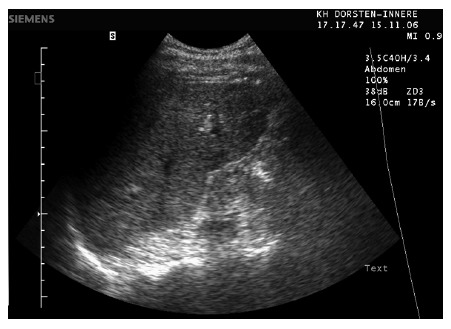
Ultrasonography of the liver.
Figure 2.

Peliosis hepatis with sinusoidal ectasia in Zone II and III (Elastica von Gieson stain, x 80).
DISCUSSION
Azathioprine-induced peliosis hepatis is thought to be idiosyncratic in humans. Possible risk factors are male gender, renal transplantation and intake of steoids[7,8]. From our observation, we conclude that alcohol binging is an additional risk factor. Peliosis hepatis is a consequence of sinusoidal endothelial cell damage[9]. This damage is demonstrated in our patient by the elevation of serum hyaluronic acid levels[10]. In vitro studies with murine sinusoidal endothelial cells and hepatocytes exposed to azathioprine have suggested that the mechanism of hepatotoxicity is sinusoidal endothelial damage associated with glutathione depletion. In this model, azathioprine toxicity was selective to sinusoidal endothelial cells and hepatocellular damage was likely due to subsequent ischemia rather than direct toxicity to hepatocytes. Reducing intracellular glutathione levels in sinusoidal endothelial cells increased azathioprine toxicity. Glutathione levels in sinusoidal endothelial cells play an essential role in azathioprine detoxification[9]. Since ethanol binging depletes hepatic glutathione by 60% and therewith increases the toxicity of paracetamol to sinusoidal endothelial cells[11], we hypothesize from our observation that the alcohol binges of the patient led to glutathione depletion in endothelial cells, thereby increasing the susceptibility to azathioprine toxicity and leading to peliosis hepatis with portal hypertension.
The observed pancytopenia was a consequence of the hypertension rather than a direct myelotoxic effect since TMA activity was normal in our patient. High TMA activity has been associated with hepatotoxicity and refractoriness on therapy[12], while a diminished activity increases the risk of developing myelotoxicity (e.g. leucopenia or thrombocytopenia)[13].
Of interest is also the appearance of the liver during sonography. Peliosis hepatis can be a focal, segmental or diffuse dilatation of hepatic sinusoids. According to this, imaging findings are quite variable[14]. Cirrhotic appearance as in our patient without histological signs of fibrosis or cirrhosis has not been described so far.
The problem of alcohol binging has not yet been addressed in IBD patients undertaking immunosuppressive therapy. This should be reviewed in future considerations regarding patients advice.
ACKNOWLEDGMENTS
We thank L Browning for careful reading the manuscript.
Footnotes
S- Editor Zhu LH L- Editor Kumar M E- Editor Lu W
References
- 1.Winther KV, Jess T, Langholz E, Munkholm P, Binder V. Survival and cause-specific mortality in ulcerative colitis: follow-up of a population-based cohort in Copenhagen County. Gastroenterology. 2003;125:1576–1582. doi: 10.1053/j.gastro.2003.09.036. [DOI] [PubMed] [Google Scholar]
- 2.Card T, Hubbard R, Logan RF. Mortality in inflammatory bowel disease: a population-based cohort study. Gastroenterology. 2003;125:1583–1590. doi: 10.1053/j.gastro.2003.09.029. [DOI] [PubMed] [Google Scholar]
- 3.Sainsbury A, Heatley RV. Review article: psychosocial factors in the quality of life of patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2005;21:499–508. doi: 10.1111/j.1365-2036.2005.02380.x. [DOI] [PubMed] [Google Scholar]
- 4.Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge drinking among US adults. JAMA. 2003;289:70–75. doi: 10.1001/jama.289.1.70. [DOI] [PubMed] [Google Scholar]
- 5.Pearson DC, May GR, Fick GH, Sutherland LR. Azathioprine and 6-mercaptopurine in Crohn disease. A meta-analysis. Ann Intern Med. 1995;123:132–142. doi: 10.7326/0003-4819-123-2-199507150-00009. [DOI] [PubMed] [Google Scholar]
- 6.Romagnuolo J, Sadowski DC, Lalor E, Jewell L, Thomson AB. Cholestatic hepatocellular injury with azathioprine: a case report and review of the mechanisms of hepatotoxicity. Can J Gastroenterol. 1998;12:479–483. doi: 10.1155/1998/294752. [DOI] [PubMed] [Google Scholar]
- 7.Russmann S, Zimmermann A, Krähenbühl S, Kern B, Reichen J. Veno-occlusive disease, nodular regenerative hyperplasia and hepatocellular carcinoma after azathioprine treatment in a patient with ulcerative colitis. Eur J Gastroenterol Hepatol. 2001;13:287–290. doi: 10.1097/00042737-200103000-00013. [DOI] [PubMed] [Google Scholar]
- 8.Bastida G, Nos P, Aguas M, Beltrán B, Rubín A, Dasí F, Ponce J. Incidence, risk factors and clinical course of thiopurine-induced liver injury in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2005;22:775–782. doi: 10.1111/j.1365-2036.2005.02636.x. [DOI] [PubMed] [Google Scholar]
- 9.DeLeve LD, Wang X, Kuhlenkamp JF, Kaplowitz N. Toxicity of azathioprine and monocrotaline in murine sinusoidal endothelial cells and hepatocytes: the role of glutathione and relevance to hepatic venoocclusive disease. Hepatology. 1996;23:589–599. doi: 10.1002/hep.510230326. [DOI] [PubMed] [Google Scholar]
- 10.Williams AM, Langley PG, Osei-Hwediah J, Wendon JA, Hughes RD. Hyaluronic acid and endothelial damage due to paracetamol-induced hepatotoxicity. Liver Int. 2003;23:110–115. doi: 10.1034/j.1600-0676.2003.00808.x. [DOI] [PubMed] [Google Scholar]
- 11.McCuskey RS, Bethea NW, Wong J, McCuskey MK, Abril ER, Wang X, Ito Y, DeLeve LD. Ethanol binging exacerbates sinusoidal endothelial and parenchymal injury elicited by acetaminophen. J Hepatol. 2005;42:371–377. doi: 10.1016/j.jhep.2004.11.033. [DOI] [PubMed] [Google Scholar]
- 12.Dubinsky MC, Lamothe S, Yang HY, Targan SR, Sinnett D, Théorêt Y, Seidman EG. Pharmacogenomics and metabolite measurement for 6-mercaptopurine therapy in inflammatory bowel disease. Gastroenterology. 2000;118:705–713. doi: 10.1016/s0016-5085(00)70140-5. [DOI] [PubMed] [Google Scholar]
- 13.Schütz E, Gummert J, Mohr FW, Armstrong VW, Oellerich M. Azathioprine myelotoxicity related to elevated 6-thioguanine nucleotides in heart transplantation. Transplant Proc. 1995;27:1298–1300. [PubMed] [Google Scholar]
- 14.Iannaccone R, Federle MP, Brancatelli G, Matsui O, Fishman EK, Narra VR, Grazioli L, McCarthy SM, Piacentini F, Maruzzelli L, et al. Peliosis hepatis: spectrum of imaging findings. AJR Am J Roentgenol. 2006;187:W43–W52. doi: 10.2214/AJR.05.0167. [DOI] [PubMed] [Google Scholar]