

Abstract
Objective
Evidence has linked economic hardship with increased intimate partner violence (IPV) perpetration among males. However, less is known about how economic debt or gender norms related to men's roles in relationships or the household, which often underlie IPV perpetration, intersect in or may explain these associations. We assessed the intersection of economic debt, attitudes toward gender norms, and IPV perpetration among married men in India.
Methods
Data were from the evaluation of a family planning intervention among young married couples (n=1,081) in rural Maharashtra, India. Crude and adjusted logistic regression models for dichotomous outcome variables and linear regression models for continuous outcomes were used to examine debt in relation to husbands' attitudes toward gender-based norms (i.e., beliefs supporting IPV and beliefs regarding male dominance in relationships and the household), as well as sexual and physical IPV perpetration.
Results
Twenty percent of husbands reported debt. In adjusted linear regression models, debt was associated with husbands' attitudes supportive of IPV (b=0.015, p=0.004) and norms supporting male dominance in relationships and the household (b=0.006, p=0.003). In logistic regression models adjusted for relevant demographics, debt was associated with perpetration of physical IPV (adjusted odds ratio [AOR] = 1.4, 95% confidence interval [CI] 1.1, 1.9) and sexual IPV (AOR=1.6, 95% CI 1.1, 2.1) from husbands. These findings related to debt and relation to IPV were slightly attenuated when further adjusted for men's attitudes toward gender norms.
Conclusion
Findings suggest the need for combined gender equity and economic promotion interventions to address high levels of debt and related IPV reported among married couples in rural India.
Intimate partner violence (IPV) perpetrated by male partners or husbands occurs in high proportions globally as well as in low- to middle-income countries such as India.1,2 One recent multi-country household study found that 37% of men in India reported having ever perpetrated physical violence against a female intimate partner in their lifetime. The health burden of IPV has been well demonstrated, with significant effects on women's sexual and reproductive health (e.g., increased sexually transmitted infections, unintended pregnancy, and poor pregnancy outcomes),3–5 mental health (e.g., anxiety, depression, and substance use),6,7 as well as a multitude of other poor health outcomes among women and their children (e.g., maternal and child malnutrition and infant death).8,9
Recent research among women has identified economic hardship (e.g., financial dependence on male partners and economic instability) as increasing women's vulnerability to IPV.10,11 Although studies have found an association between economic stressors and reports of male IPV perpetration,12–16 no research has examined debt in relation to these outcomes.
Debt and other economic decisions in the context of marriage, particularly in rural India, are largely under the control of husbands. Taking on debt may be associated with economic hardship, heightening stress levels among men, and, in turn, IPV. Also, previous work documenting the association between economic hardship and increased IPV perpetration by males12–15 has largely been explained by perceptions related to men's roles financially within the family (e.g., men who do not feel that they are providing financially for their families may perceive that they are not fulfilling their roles as husbands/males, and this perception related to lack of role fulfillment may escalate into violence). Given that a decision to take on debt appears to be largely controlled by men in this context and likely tied to their perceived role of providing financially for the family, a man's decision to take out loans may be determined, in part, by their support of masculine gender norms (e.g., a man's role in the family and male dominance and control in the household). In addition, given previous work highlighting the association between masculine gender norms and a number of risk behaviors among boys and men (e.g., substance and tobacco use and behaviors resulting in unintentional injury),17–21 such gender norms may also be linked to taking on risks associated with debt, as well as debt-acquiring behaviors (e.g., spending money on nonessential goods such as alcohol).
Gender norms pertaining to IPV, relationships, and the household are also important driving factors in terms of understanding men's behaviors related to IPV. Cross-cultural research has shown that societies with greater gender inequities in social norms and policies have a higher prevalence of IPV.21 In the context of India and elsewhere, women's low status in families and high levels of societal tolerance and acceptance of IPV promote IPV.22
More research is needed to understand economic hardship, and debt specifically, in relation to attitudes toward gender norms and IPV perpetration. Many studies have hypothesized that stress related to economic hardship and debts increases IPV perpetration;12–15 however, less research has sought to understand the role of attitudes supportive of men's more traditional gender norms in relationships or households in contributing to decisions to take on debt as well as in terms of explaining its association with increased IPV perpetration. Increased understanding of the mechanisms that explain associations between economic hardship/debt and IPV is needed to inform prevention approaches, particularly given the increasing number of economic promotion interventions being implemented globally and throughout India.
Thus, the primary objective of the current study was to assess household debt in relation to husbands' support of gender-inequitable norms and norms promoting IPV as well as husbands' use of IPV against wives. The secondary objective of this study was to assess whether or not gender-based attitudes are important factors in debt and IPV, as well as in explaining an association between debt and increased risk for IPV perpetration among husbands.
METHODS
This cross-sectional study involved analyses of data (n=1,081 married men) from baseline surveys of a male-centered family planning intervention for young couples in rural Maharashtra, Counseling Husbands to Achieve Reproductive Health and Marital Equity (CHARM).
Sample and study procedures
Participants were recruited from the rural Thane District of Maharashtra. Geographic clusters (n=50) were selected via community mapping based on geographic boundaries (e.g., hills, roads, and streams), population density (each cluster had at least 300 households), and presence of a private health-care provider. From March to December 2012, trained research staff members approached households to identify young married men aged 18–30 years within selected clusters. Research staff provided informed consent in a private space in the house. Eligibility criteria included being 18–30 years of age, being fluent in Marathi, residing with their wife for the past three months, having plans to stay in the same location for another two years, and not having been sterilized (for either the man or his wife). Research staff members provided details regarding the CHARM intervention and evaluation to interested couples who met these criteria. Research staff members screened 1,881 couples from March to December 2012. Of those couples screened, 1,143 (61%) were eligible to participate in the study and 1,081 (95%) eligible couples chose to participate in the study. Clusters were randomized to intervention and control conditions. The present analyses were based on data from the baseline survey assessment of wives and their husbands (n=1,081).
Eligible and interested participants completed a 60-minute paper survey (with distinct surveys for husbands and wives). Survey items covered a broad range of topics including demographics, contraception knowledge and use, marital communication, substance use, sexual history, and gender equity attitudes. No monetary incentive was provided for study or intervention program participation.
Survey measures
Sample characteristics.
Age was measured continuously and grouped into three categories (≤20, 21–25, and 26–30 years). Education was measured by whether or not the participant attended any school (yes/no). Age at marriage was measured continuously and categorized as having been married when <18 years of age (yes/no). Number of children was measured continuously and categorized based on the sample distribution as having none, one, or ≥2 children. Alcohol use was measured by asking male participants if they drank alcohol and how frequently (every day, once a week, or less than once per week).
Debt.
Household debt was measured by asking, “Do you have any debt?” Those responding “yes” were categorized as having debt. Husbands' and wives' reports of debt were each measured separately. For the purpose of this study, husbands' reports of debt were used.
IPV.
Male IPV perpetration was based on data reported by wives regarding their husbands' perpetration of IPV. In the survey among the wives, a series of questions were asked regarding whether or not women had ever experienced physical and/or sexual IPV. Physical IPV was categorized based on respondents' report of any of the following: “husband slapped you”; “husband twisted your arm or pulled your hair”; “husband pushed you, shook you, or threw something at you”; “husband kicked you, dragged you, or beat you up”; “husband choked you or tried to burn you on purpose”; or “husband threatened to attack you with a knife, gun, or any other weapon.” Sexual IPV was categorized based on respondents' report of any of the following: “husband physically forced you to have sexual intercourse with him even when you did not want to” and “husband forced you to perform any sexual acts when you did not want to.”
Gender attitudes related to men's roles in relationships and the household were measured using 25 items from the Gender Equitable Men (GEM) scale,23 related to husbands' perceptions of men's roles and expectations. Examples included: “A man should have the final word about decisions in his home”; “It is important that a father is present in the lives of his children, even if he is no longer with the mother”; “A man needs other women, even if things with his wife are fine”; “Men are always ready to have sex”; and “I would be outraged if my wife asked me to use a condom.” Responses included a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Cronbach's alpha was 0.72 for these 25 items, indicating moderate reliability. A summary score was used for these 25 items, reversing items as appropriate, so that a higher score indicated greater support of gender-inequitable norms.
Attitudes supportive of IPV were measured using seven items related to husbands' perceptions of men's justification for using violence against wives.24 Respondents were asked, “In your opinion, is a husband justified in hitting or beating his wife in the following situations …” Examples included: “If she goes out without telling him,” “If she neglects the house or the children,” “If she argues with him,” and “If she refuses to have sex with him.” Responses used a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Cronbach's alpha was 0.77 for these seven items, indicating strong reliability. A summary score was used for these seven items, with a higher score indicating higher levels of attitudes supportive of IPV.
Data analysis
Frequencies and means were calculated for categorical and continuous variables, respectively. Chi-squared tests were used to assess sample characteristics by reports of household debt. Crude and adjusted logistic regression models for dichotomous outcome variables and linear regression models for continuous outcomes were used to examine household debt reported by husbands in relation to husbands' attitudes supportive of IPV, beliefs supportive of male dominance in relationships and the household, and reports of sexual or physical IPV by wives. To understand whether or not attitudes toward gender-based norms were an important factor in explaining any significant findings related to the relationship between debt and IPV, fully adjusted models were also used to further adjust for attitudes toward gender norms. All demographic variables associated with debt (p<0.10) were included in adjusted models. Findings from logistic regression models were calculated as odds ratios with associated 95% confidence intervals (CIs), and significance of individual variables was evaluated using Wald chi-squared tests. Linear regression findings were calculated as parameter estimates (b), 95% CIs, and associated p-values. All analyses were conducted using SAS® version 9.1.25
RESULTS
Sample characteristics
The mean age of husbands in the survey was 26.2 years (standard deviation [SD] = 2.7). Only 3% of husbands reported being married at ≤18 years of age (Table 1). Couples reported being married on average for four years (SD=2.6, range: 0–14 years). About three-quarters (77%) of the sample reported having children; 47% had one child and 30% had ≥2 children. About half (49%) of husbands reported no alcohol use, 13% reported once-weekly alcohol use, 36% reported less than weekly alcohol use, and 3% reported daily alcohol use. Those who reported debt were significantly more likely than those reporting no debt to have fewer children (chi-squared = 9.50, p=0.009) (Table 1).
Table 1.
Sample characteristics of husbands participating in the CHARM study in rural Maharashtra, India (total and by reported debt), 2012
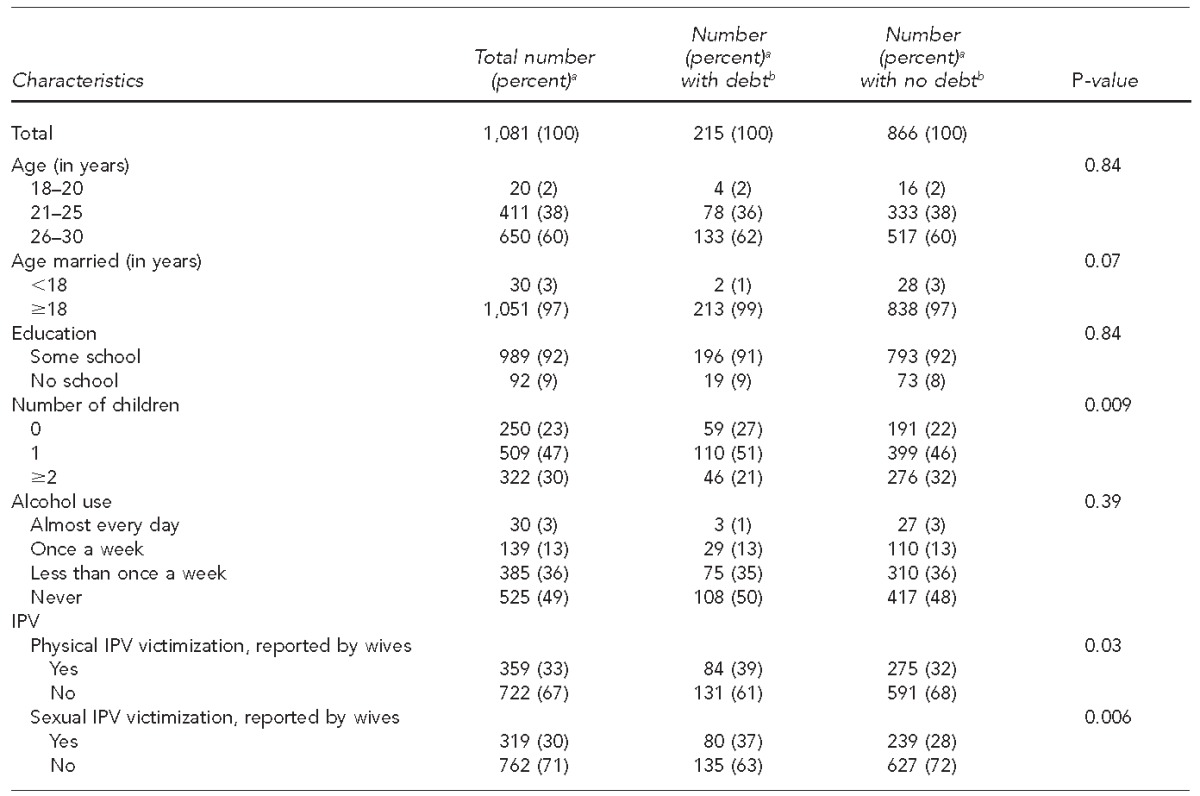
aPercentages may not total to 100 due to rounding and missing data (e.g., two respondents were missing data on alcohol use).
bRefers to husbands' report of household debt (yes/no)
cUsing the Wald chi-squared test
CHARM = Counseling Husbands to Achieve Reproductive Health and Marital Equity
IPV = intimate partner violence
Twenty percent (n=215/1,081) of the sample reported debt (Table 1). In exploratory analyses, only 15% of the wives reported having debt. Thus, a significant number of wives did not report debt that husbands reported. About one-third of wives reported physical IPV (33%) or sexual IPV (30%).
Household debt, attitudes toward gender-based norms, and IPV perpetration
In linear regression analyses adjusted for age, husbands' report of debt was associated with greater support of IPV (b=0.015, p=0.004) as well as greater support of male dominance in relationships and the household by husbands (b=0.006, p=0.003) (Table 2).
Table 2.
Findings from crude and adjusted linear regression models: household debta and relation to gender-based attitudes among husbands (n=1,081) participating in the CHARM study in rural Maharashtra, India, 2012
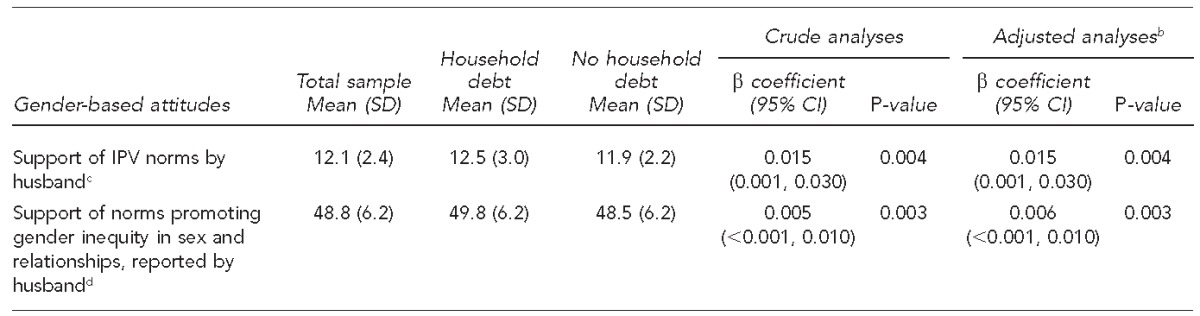
Debt refers to husbands' reports of household debt (yes/no).
bAdjusted for age of marriage and number of children
cHusbands' support of IPV norms was measured using seven items. Responses ranged from 1 (strongly disagree) to 5 (strongly agree), with higher values representing greater levels of support. A summary score was calculated for each participant. The mean of these summary scores is presented in the table.
dSupport of norms promoting gender equity in sex and relationships was measured using 25 items. Responses ranged from 1 (strongly disagree) to 5 (strongly agree), with higher values representing greater levels of support. A summary score was calculated for each participant. The mean of these summary scores is presented in the table.
CHARM = Counseling Husbands to Achieve Reproductive Health and Marital Equity
SD = standard deviation
CI = confidence interval
IPV = intimate partner violence
In logistic regression models adjusted for age of marriage and number of children, husbands who reported having economic debt were more likely to perpetrate physical IPV (adjusted odds ratio [AOR] = 1.4, 95% CI 1.1, 1.9) and sexual IPV (AOR=1.6, 95% CI 1.1, 2.1). When models were further adjusted for attitudes supportive of IPV and male dominance in relationships and the household, debt was still significantly associated with sexual IPV (AOR=1.5, 95% CI 1.1, 2.0) (Table 3).
Table 3.
Findings from crude and adjusted logistic regression models: household debta and relation to physical and sexual IPV among husbands (n=1,081) participating in the CHARM study in rural Maharashtra, India, 2012
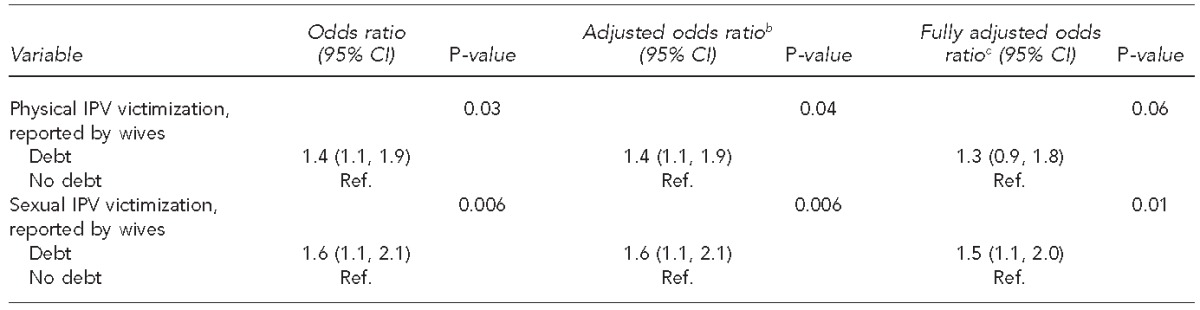
Debt refers to husbands' reports of household debt (yes/no).
bAdjusted for age of marriage and number of children
cModels assessing debt in relation to physical/sexual IPV are adjusted for demographic variables, other violence, as well as gender-based attitudes. For example, models assessing the relationship between debt and physical IPV victimization are adjusted for demographic variables, sexual IPV, and gender-based attitudes.
IPV = intimate partner violence
CHARM = Counseling Husbands to Achieve Reproductive Health and Marital Equity
CI = confidence interval
Ref. = reference group
DISCUSSION
This study is among the first to document the association between household economic debt and relationship to husbands' risk for IPV perpetration. This study also provides evidence of a link between debt and attitudes supportive of norms promoting IPV and gender inequity in relationships and the household. Furthermore, findings suggest that the relationship between debt and IPV perpetration may be partly explained by these gender-based attitudes (i.e., those supportive of IPV or male dominance in relationships and the household). Although not a primary aim of the study, study findings highlighted a discrepancy between debts reported by husbands and those reported by their wives, suggesting that wives may not have been aware of debts in the household. Although more research is needed to understand the temporal order and mechanisms involved in these associations, this study highlights the gender-based nature of economic debt in this context, both in terms of gender-based factors that may be involved in decisions to take on debt as well as in the relationship of debt to IPV.
To our knowledge, this study is the first to find that reports of debt are associated with attitudes supportive of IPV as well as more traditional gender roles for men in relationships and the household among a sample of men. Previous studies have shown that husbands are more likely than their wives to spend money on alcohol or other non-fundamental household items, which may promote household debt. However, when women have control over how finances are spent in the -household, they tend to spend money on children and basic household needs (e.g., food and shelter).10,11,26 Notably, we did not find a significant association between debt and alcohol use among men. However, findings related to gender-based attitudes are supported by previous -studies among men that have linked gender-inequitable attitudes to other risky behaviors, such as men's violence, other activities promoting physical injuries (e.g., car accidents and suicide attempts), and substance use.17–20 The link between debt and these gender-based attitudes may also be explained by men's perceptions of their role as husbands, particularly if men perceive that they are not fulfilling their financial breadwinning role, and this perception regarding lack of role fulfillment may escalate into violence or extramarital sexual relationships. Future research is needed that includes more specific measures on debt to better understand men's decision-making process, behaviors related to debt, as well as the types of debt.
Our study findings suggest that attitudes supportive of IPV and men's more traditional gender norms in relationships/households appear to be associated with taking on debt (e.g., as part of men's desire to provide financially for the household, or as part of a broader set of risky behaviors associated with traditional gender norms and beliefs) as well as in terms of explaining the association between debt and IPV perpetration (e.g., beliefs supportive of IPV coupled with economic stressors may lead to violence and men's perceptions that they are not fulfilling gendered expectations to provide financially for their families, escalating to violence). However, because we found strong associations between debt and risk for sexual IPV, independent of men's support of gender-inequitable norms, more work may be needed to examine other mechanisms that may also contribute to these associations (e.g., other factors within one's environment or family). Thus, although our findings suggest that attitudes supportive of IPV or traditional gender roles appear to be important, other factors may also be important contributors explaining the relationship between debt and IPV. In the context of rural India among young married couples, such stressors could include the influence of or need to financially support other family members in the household, as well as other types of community influences or norms. More work is needed to better identify the contributing factors explaining the relationship between debt and IPV.
Limitations
This study was subject to several limitations. The cross-sectional design does not establish the temporality of these associations; thus, future longitudinal studies are needed. Additionally, the items used for analyses relied on self-reported responses. Stigma can often result in underreporting of sensitive issues or socially undesirable outcomes, such as IPV.27–29 However, such underreporting would decrease the power to detect an association between debt and IPV. The current study found multiple strong links among these factors. Furthermore, future studies are needed to understand the types of debt reported, given that some forms of debt may be indicative of financial well-being rather than economic hardship (e.g., purchasing a home). However, in this relatively homogenous sample of young, poor, rural married couples, debt was most likely indicative of economic hardship. Finally, the findings of this study are most applicable to populations of young, rural, married couples in the state of Maharashtra and may not be generalizable to other populations from this state, other Indian states, or elsewhere.
CONCLUSION
This study highlights the link between IPV and debt, attitudes supportive of IPV, and more traditional gender roles for men in relationships or the household. This study is among the first to also suggest that husbands' reports of debt may not be aligned with debt reported or known by wives. Study findings suggest that decisions related to debt may be predominantly male controlled but also that debt appears to be associated with men's gender-based attitudes. These findings are especially important given that many of the promising economic interventions, particularly in India, have overwhelmingly targeted poor populations of women rather than men. In the current study, given that debt was strongly associated with the support of gender-based attitudes as well as a discrepancy in the reporting of debt between husbands and wives, economic-based programs may also need to consider the gender-based nature of debt, as well as the inclusion of men in such programming. Given that women may be less aware of economic debts taken on by their husbands, findings suggest that debt-reduction interventions may be needed that include a focus on men but that also incorporate aspects to address and challenge men's attitudes supportive of more traditional gender norms and roles. Although longitudinal studies are needed to better understand the temporal order of these associations, findings suggest that approaches that combine aspects of gender equity and economic promotion may be effective to address debt and other forms of economic hardship, and may also help alleviate high levels of IPV reported among married couples in rural India.
Footnotes
The authors thank the participants of the Counseling Husbands to Achieve Reproductive Health and Marital Equity (CHARM) study as well as all research staff members who supported data collection for this project; Drs. Sudan Ramaji Suryawanshi and Gajanan Velhal of Bai Yamunabai Laxman Nair Hospital and Topiwala National Medical College Mumbai; the Primary Health Centers and private health-care providers of project areas for supporting CHARM intervention delivery; and the project officer at Eunice Kennedy Shriver National Institute of Child Health and Human Development, Susan Newcomer, for her consistent support of this Indo-U.S. research study.
The study was funded by grants from the David and Lucile Packard Foundation (grant #2011-37366), the National Institutes of Health Indo-U.S. Joint Working Group on Contraception and Reproductive Health Research (grant #R01HD061115), and the Department of Biotechnology, India. Elizabeth Reed was also supported by grant #K01MH099969 from the National Institute of Mental Health.
All research study procedures were approved by the institutional review boards at the University of California, San Diego, and the National Institute for Research in Reproductive Health (Indian Council of Medical Research), Mumbai, India.
REFERENCES
- 1.Rocca CH, Rathod S, Falle T, Pande RP, Krishnan S. Challenging assumptions about women's empowerment: social and economic resources and domestic violence among young married women in urban South India. Int J Epidemiol. 2009;38:577–85. doi: 10.1093/ije/dyn226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fleming PJ, McCleary-Sills J, Morton M, Levtov R, Heilman B, Barker G. Risk factors for men's lifetime perpetration of physical violence against intimate partners: results from the International Men and Gender Equality Survey (IMAGES) in eight countries. PLoS One. 2015;10:e0118639. doi: 10.1371/journal.pone.0118639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Silverman JG, Decker MR, Saggurti N, Balaiah D, Raj A. Intimate partner violence and HIV infection among married Indian women. JAMA. 2008;300:703–10. doi: 10.1001/jama.300.6.703. [DOI] [PubMed] [Google Scholar]
- 4.Barua A, Kurz K. Reproductive health-seeking by married adolescent girls in Maharashtra, India. Reprod Health Matters. 2001;9:53–62. doi: 10.1016/s0968-8080(01)90008-4. [DOI] [PubMed] [Google Scholar]
- 5.Silverman JG, Decker MR, Cheng DM, Wirth K, Saggurti N, McCauley HL, et al. Gender-based disparities in infant and child mortality based on maternal exposure to spousal violence: the heavy burden borne by Indian girls. Arch Pediatr Adolesc Med. 2011;165:22–7. doi: 10.1001/archpediatrics.2010.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sarkar NN. The impact of intimate partner violence on women's reproductive health and pregnancy outcome. J Obstet Gynaecol. 2008;28:266–71. doi: 10.1080/01443610802042415. [DOI] [PubMed] [Google Scholar]
- 7.Chandran M, Tharyan P, Muliyil J, Abraham S. Post-partum depression in a cohort of women from a rural area of Tamil Nadu, India. Incidence and risk factors. Br J Psychiatry. 2002;181:499–504. doi: 10.1192/bjp.181.6.499. [DOI] [PubMed] [Google Scholar]
- 8.Ackerson LK, Subramanian SV. Domestic violence and chronic malnutrition among women and children in India. Am J Epidemiol. 2008;167:1188–96. doi: 10.1093/aje/kwn049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jejeebhoy SJ. Associations between wife-beating and fetal and infant death: impressions from a survey in rural India. Stud Fam Plan. 1998;29:300–8. [PubMed] [Google Scholar]
- 10.Reed E, Gupta J, Biradavolu M, Devireddy V, Blankenship KM. The context of economic insecurity and its relation to violence and risk factors for HIV among female sex workers in Andhra Pradesh, India. Public Health Rep. 2010;125(Suppl 4):81–9. doi: 10.1177/00333549101250S412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Reed E, Emanuel AN, Myers B, Johnson K, Wechsberg WM. The relevance of social contexts and social action to reducing substance use and victimization among women participating in an HIV prevention intervention in Cape Town, South Africa. Subst Abuse Rehabili. 2013;4:55–64. doi: 10.2147/SAR.S45961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sambisa W, Angeles G, Lance PM, Naved RT, Thornton J. Prevalence and correlates of physical spousal violence against women in slum and nonslum areas of urban Bangladesh. J Interpers Violence. 2011;26:2592–618. doi: 10.1177/0886260510388282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Selic P, Svab I, Gucek NK. A cross-sectional study identifying the pattern of factors related to psychological intimate partner violence exposure in Slovenian family practice attendees: what hurt them the most. BMC Public Health. 2014;14:223. doi: 10.1186/1471-2458-14-223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Malcoe LH, Duran BM, Montgomery JM. Socioeconomic disparities in intimate partner violence against Native American women: a cross-sectional study. BMC Med. 2004;2:20. doi: 10.1186/1741-7015-2-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rodgers KB, McGuire JK. Adolescent sexual risk and multiple contexts: interpersonal violence, parenting, and poverty. J Interpers Violence. 2012;27:2091–107. doi: 10.1177/0886260511432148. [DOI] [PubMed] [Google Scholar]
- 16.Ford JL, Browning CR. Neighborhood social disorganization and the acquisition of trichomoniasis among young adults in the United States. Am J Public Health. 2011;101:1696–703. doi: 10.2105/AJPH.2011.300213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Feingold A, Kerr DC, Capaldi DM. Associations of substance use problems with intimate partner violence for at-risk men in long-term relationships. J Fam Psychol. 2008;22:429–38. doi: 10.1037/0893-3200.22.3.429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Decker MR, Seage GR, 3rd, Hemenway D, Raj A, Saggurti N, Balaiah D, et al. Intimate partner violence functions as both a risk marker and risk factor for women's HIV infection: findings from Indian husband-wife dyads. J Acquir Immune Defic Syndr. 2009;51:593–600. doi: 10.1097/QAI.0b013e3181a255d6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Patel N, Webb K, White D, Barker L, Rosby A, DeBerry M, et al. Homicides and suicides—National Violent Death Reporting System, United States, 2003–2004[published erratum appears in MMWR Morb Mortal Wkly Rep 2006;55(39):1074-5] MMWR Morb Mortal Wkly Rep. 2006;55(26):721–4. [PubMed] [Google Scholar]
- 20.Peden M, McGee K, Krug E, editors. Injury: a leading cause of the global burden of disease, 2000. Geneva: World Health Organization; 2002. [Google Scholar]
- 21.Palma-Solis M, Vives-Cases C, Alvarez-Dardet C. Gender progress and government expenditure as determinants of femicide. Ann Epidemiol. 2008;18:322–9. doi: 10.1016/j.annepidem.2007.11.007. [DOI] [PubMed] [Google Scholar]
- 22.Burton B, Duvvury N, Varia N. Washington: International Center for Research on Women; 2000. Domestic violence in India, part 3: a summary report of a multi-site household survey. [Google Scholar]
- 23.Pulerwitz J, Barker G. Measuring attitudes toward gender norms among young men in Brazil: development and psychometric evaluation of the GEM Scale. Men Masculin. 2008;10:322–38. [Google Scholar]
- 24.Demographic and Health Surveys. India: standard DHS, 2005–2006 [cited 2012 Mar 27] Available from: URL: http://www.measuredhs.com/what-we-do/survey/survey-display-264.cfm.
- 25.SAS Institute, Inc. SAS®: Version 9.1. Cary (NC): SAS Institute, Inc.; 2003. [Google Scholar]
- 26.Wechsberg WM, Myers B, Reed E, Carney T, Emanuel AN, Browne FA. Substance use, gender inequity, violence and sexual risk among couples in Cape Town. Cult Health Sex. 2013;15:1221–36. doi: 10.1080/13691058.2013.815366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hanck SE, Blankenship KM, Irwin KS, West BS, Kershaw T. Assessment of self-reported sexual behavior and condom use among female sex workers in India using a polling box approach: a preliminary report. Sex Transm Dis. 2008;35:489–94. doi: 10.1097/OLQ.0b013e3181653433. [DOI] [PubMed] [Google Scholar]
- 28.Botta RA, Pingree S. Interpersonal communication and rape: women acknowledge their assaults. J Health Commun. 1997;2:197–212. doi: 10.1080/108107397127752. [DOI] [PubMed] [Google Scholar]
- 29.Fisher BS, Daigle LE, Cullen FT, Turner MG. Acknowledging sexual victimization as a rape: results from a national-level study. Justice Q. 2003;20:535–74. [Google Scholar]