

Abstract
Patient: Female, 24
Final Diagnosis: Pinworms infection
Symptoms: Abdominal pain • bloating
Medication: —
Clinical Procedure: Colonoscopy and biopsy
Specialty: Gastroenterology and Hepatology
Objective:
Rare disease
Background:
Inflammatory bowel disease (IBD) is well recognized in developed countries and is generally among the differential diagnoses of young patients presenting with refractory diarrhea once other more common etiologies have been excluded. Pinworm infections, on the other hand, are not as common among adults in the United States.
Case Report:
Based on computed tomography features, a 24-year-old female patient with a history of multiple autoimmune disorders presented with abdominal pain and was diagnosed recently with Crohn’s disease. Colonoscopy was significant for pinworms seen throughout the colon. Colonic biopsy was negative for inflammatory bowel disease (IBD)-related changes.
Conclusions:
The diagnosis of IBD is a serious label that requires biopsy confirmation before committing to possibly lifelong treatment and possible adverse effects. Even in the most typical patient and when the presentation and imaging are classical, uncommon conditions (like Enterobius infection in this case) may preclude appropriate diagnosis and management.
MeSH Keywords: Colonoscopy, Crohn Disease, Enterobius, Inflammatory Bowel Diseases
Background
Inflammatory bowel disease (IBD) is well recognized in developed countries and is generally among the differential diagnoses of young patients presenting with refractory diarrhea once other more common etiologies have been excluded. IBD includes 2 entities: ulcerative colitis (UC) and Crohn’s disease (CD). CD has a prevalence of 201 per 100 000 population while UC has a prevalence of 238 per 100 000 population in the United States [1]. In contrast, Enterobius vermicularis infections are not commonly seen in everyday practice and are not considered in the differential of common gastrointestinal complaints. This diagnosis is only considered when travel to endemic areas is involved. However, Enterobiasis (also known as pinworm) is the most common helminthic infection in the US and Western Europe. The Center for Disease Control and Prevention (CDC) estimates that about 40 million persons are infected in the United States. While patients are commonly asymptomatic, gastrointestinal manifestations, such as abdominal pain and diarrhea, may occur. Diagnosis is usually made by microscopic visualization of Enterobius eggs and treatment consists of a course of an anti-helminthic agent, such as Albendazole [2,3]. We present the case of a patient with persistent diarrhea, who was presumed to have IBD without consideration of Enterobiasis, given the rarity of this diagnosis in everyday practice. CD was high on the differential because a previous CT abdomen showed inflammatory changes confined to the distal ileum. We wish to bring awareness to such an under-recognized but prevalent diagnosis here in the US.
Case Report
A 24-year-old white woman female was admitted for the evaluation of intolerable abdominal pain and bloating for the past 10 days prior to admission, associated with nausea, but no vomiting, fever, or diarrhea. She had a past medical history significant for juvenile rheumatoid arthritis A, chronic pericarditis, pulmonary arterial hypertension, and past surgical history of cholecystectomy. She had similar episodes before and was told she had Crohn’s disease at another facility, based on a computed tomography (CT) scan of the abdomen but she never had a colonoscopy. The patient denied sick contacts or history of recent travel.
A CT abdomen showed wall thickening with submucosal fat at the terminal ileum (Figure 1), which is nonspecific but can be seen with chronic inflammatory processes such as ulcerative colitis or Crohn’s disease. She underwent colonoscopy, which showed parasites in the transverse colon, the ascending colon, and in the cecum (Figure 2). Fluid aspiration was performed through the scope suction channel. Sample(s) were sent for ova and parasites and was positive for Enterobius vermicularis (pinworms). Ilial biopsy was negative for IBD-related changes.
Figure 1.
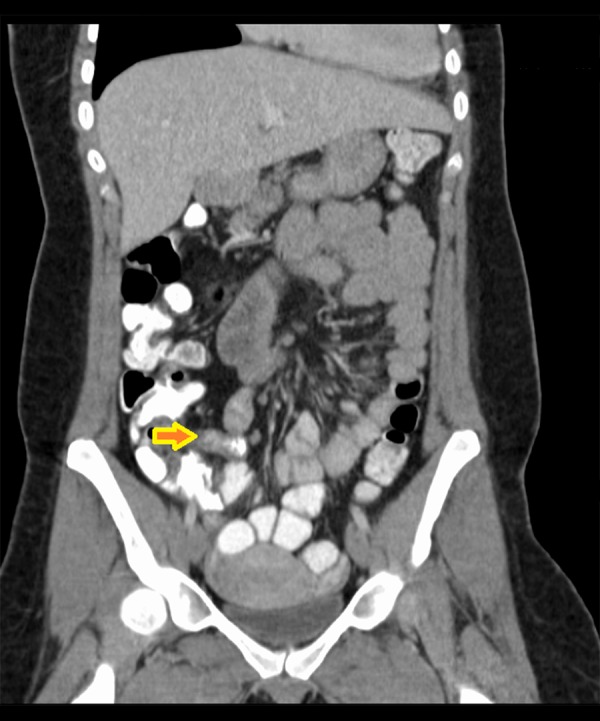
Computed tomography of the abdomen showing wall thickening with submucosal fat at the terminal ileum. The radiological features are suggestive of an inflammatory process.
Figure 2.

Colonoscopy images showing helminthic organisms throughout the colon. Those were sampled and histopathologically examined and confirmed as Enterobius vermicularis.
On subsequent questioning, she endorsed living in a wooded area where it had been rainy, with muddy grounds around her house. She also said she and her family usually consume private well water that occasionally dries out. This can be the route of infection (contaminated drinking water) given the lack of pertinent travel history or sick contacts to indicate the classic fecal-oral transmission.
The patient received 1 dose of Albendazole with subsequent improvement of her pain and she was discharged with a prescription for Albendazole to be taken for 2 weeks and instructions to have her children and partner treated.
Discussion
This is a case where a patient had a history of autoimmune disease, was not an immigrant/traveler from a helminthes-endemic area, and had radiological features of Crohn’s disease. In this case endoscopy and histopathology yielded a radically different diagnosis of colonic pinworm, with the subsequently appropriate treatment with anti-helminthic medications.
We seek to delineate that even in an apparently typical patient, inflammatory bowel disease should always be endoscopically confirmed and biopsy proven. While it was intuitive to proceed with the management of inflammatory bowel disease in our case, clinicians must keep in mind that colonoscopy is the cornerstone in such cases to exclude other causes of the patient’s presentation.
Conclusions
Inflammatory bowel diseases are serious diagnoses that require long-term treatment with immune-suppressive therapies. Colonic biopsies should always be performed before committing to these treatment modalities, and other etiologies, regardless how rare they may be, can also be ruled out this way.
References:
- 1.Kappelman MD, Rifas-shiman SL, Kleinman K, et al. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin Gastroenterol Hepatol. 2007;5(12):1424–29. doi: 10.1016/j.cgh.2007.07.012. [DOI] [PubMed] [Google Scholar]
- 2.Lormans JA, Wesel AJ, Vanparus OF. Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates. Chemotherapy. 1975;21(3–4):255–60. doi: 10.1159/000221866. [DOI] [PubMed] [Google Scholar]
- 3.Kucik CJ, Martin GL, Sortor BV. Common intestinal parasites. Am Fam Physician. 2004;69(5):1161–68. [PubMed] [Google Scholar]