

Description
A 56-year-old man presented with abdominal distention over a few months. He was otherwise well and routine blood tests were normal. Examination of the abdomen revealed a firm swelling. CT scan was performed for further evaluation.
A large, cystic, non-enhancing mass on the right side of the abdomen was observed on CT scan. This was closely related to the right psoas muscle with secondary compression of the right ureter and resultant right-sided hydronephrosis (figure 1).
Figure 1.
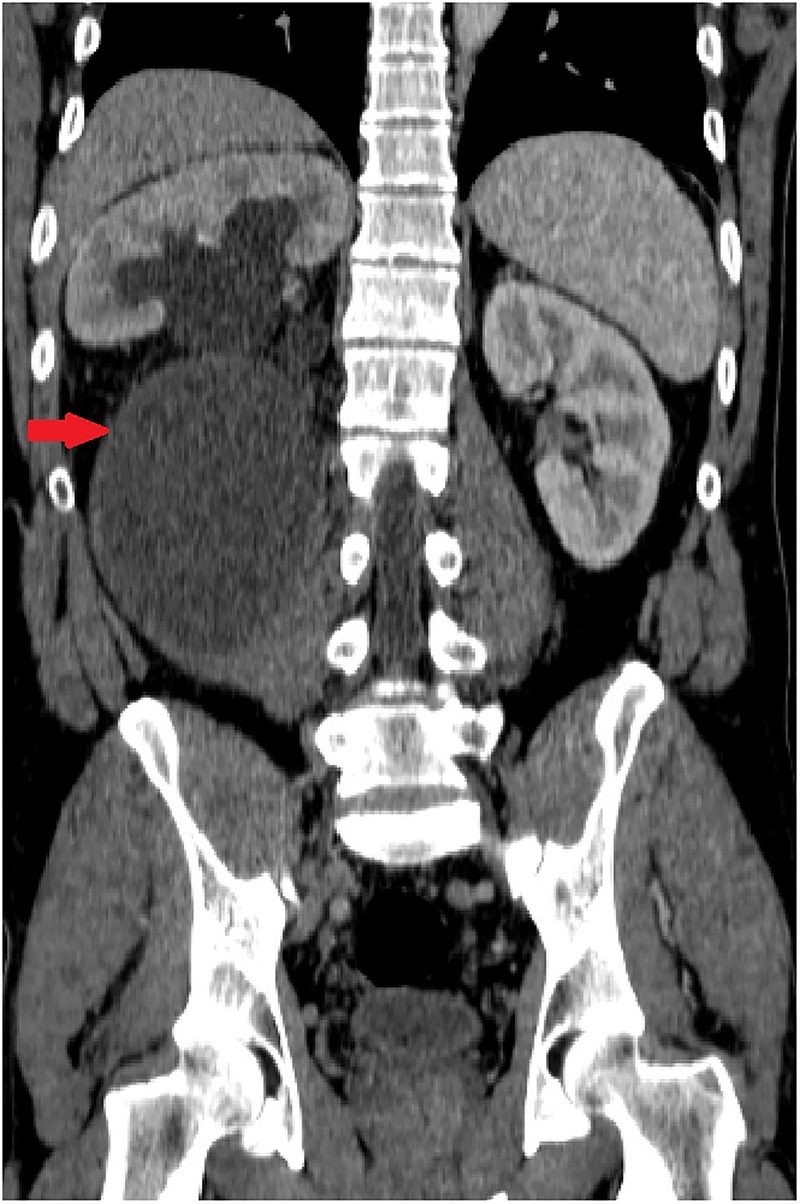
Coronal reformat demonstrating the mass in the right side of the abdomen causing secondary hydronephrosis (red arrow).
Subsequent MRI demonstrated a 19.5×17×21 cm, high T2 signal intensity lesion in the right retroperitoneum. On T1 fat saturated sequences, it appeared hypointense with thin internal mildly enhancing septations (figure 2). Right-sided hydronephrosis was observed (figure 3) together with compression of the distal common bile duct causing mild intra and extrahepatic biliary dilation (figure 4).
Figure 2.
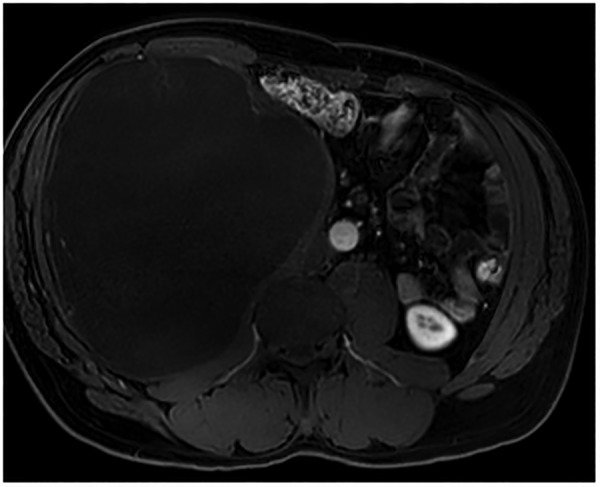
Axial contrast-enhanced T1 fat saturated image demonstrates a large hypointense mass arising from the right psoas muscle with mildly enhancing internal septations.
Figure 3.
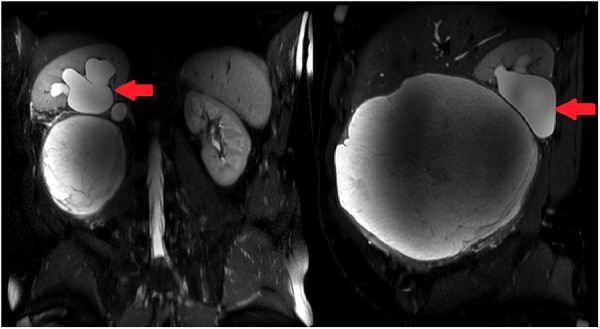
The mass is hyperintense on coronal and sagittal T2-weighted MR sequences. A hydronephrotic right kidney is shown (red arrow).
Figure 4.
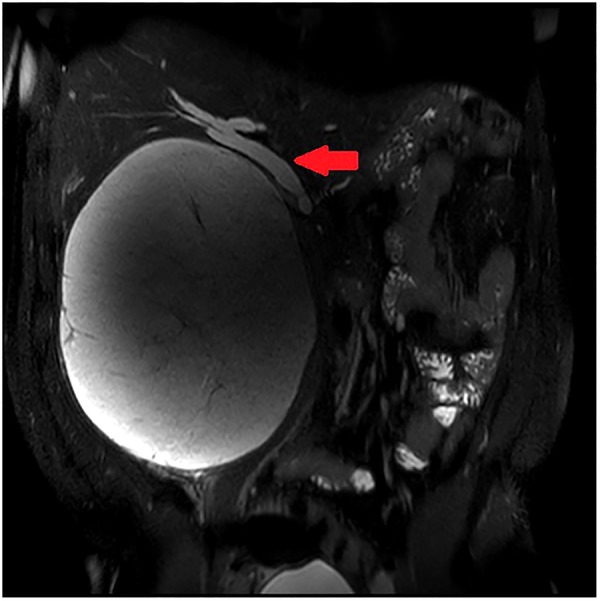
Coronal T2-weighted MR sequence showing a dilated common bile duct (red arrow), secondary to a large T2 hyperintense mass arising from the right psoas muscle.
The mass was removed surgically (figure 5). It was gelatinous in nature and was sent to the laboratory for histopathological diagnosis, which revealed that the mass was a myxoid liposarcoma.
Figure 5.

Surgical specimen.
Myxoid liposarcoma is the second most common adult soft tissue sarcoma after well-differentiated liposarcomas. It may be difficult to establish the diagnosis with MRI due to the lack of fat signal intensity and, without administration of contrast, the tumour may mimic cystic pathology, which includes benign lesions such as a hydatid cyst.1 Gadolinium-enhanced MRI is therefore an essential part of the management.2 Myxoid liposarcomas have a high risk of local recurrence (50%) and a 20% rate of metastasis.3
Learning points.
Myxoid liposarcoma is an indolent slow-growing malignant tumour of mesenchymal origin.
Myxoid liposarcoma may lead to diagnostic confusion on imaging—contrast-enhanced MRI is paramount in establishing the diagnosis.
Sarcomatous tumours should be included in the differential of retroperitoneal masses.
Footnotes
Contributors: CA and JA performed the literature review and drafted the article. KC made the radiological diagnosis and JEA performed the surgery.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Bermejo A, De Bustamante TD, Martinez A et al. MR imaging in the evaluation of cystic-appearing soft-tissue masses of the extremities. Radiographics 2013;33:833–56. doi:10.1148/rg.333115062 [DOI] [PubMed] [Google Scholar]
- 2.Sung MS, Kang HS, Suh JS et al. Myxoid liposarcoma: appearance at MR imaging with histologic correlation. Radiographics 2000; 20:1007–19. doi:10.1148/radiographics.20.4.g00jl021007 [DOI] [PubMed] [Google Scholar]
- 3.Loubignac F, Bourtoul C, Chapel F. Myxoid liposarcoma: a rare soft-tissue tumor with a misleading benign appearance. World J Surg Oncol 2009;7:42 http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2678127&tool=pmcentrez&rendertype=abstract [DOI] [PMC free article] [PubMed] [Google Scholar]