

Abstract
We report a case of bilateral useless hand syndrome, a rare presenting manifestation of vitamin B12 deficiency. A 38-year-old man, a strict vegetarian and a teacher by occupation, presented with acute onset clumsiness of both hands while performing fine movements. Detailed history-taking, examination of the patient and relevant investigations (complete blood count, serum vitamin B12 and MRI of the cervical spinal cord) were carried out. Laboratory analysis was suggestive of vitamin B12 deficiency and MRI demonstrated a lesion involving the posterior columns of the cervical cord. The patient was diagnosed as a case of non-compressive cervical myelopathy predominantly involving the posterior column due to vitamin B12 deficiency. Acute bilateral useless hand syndrome can be a rare presenting feature of vitamin B12 deficiency.
Background
Useless hand syndrome is defined as difficulty in executing distal fine movements of the hands in the absence of any weakness (pyramidal) or extrapyramidal involvement. It is predominantly attributed to involvement of the posterior columns of the spinal cord. Patients with useless hand syndrome have difficulty using their fingers to manipulating objects. This phenomenon has been reported in patients with multiple sclerosis (MS)1–5 and may rarely be due to cervical compressive myelopathy.6
Common neurological manifestations of vitamin B12 deficiency are subacute combined degeneration of cord, behavioural abnormality, optic nerve involvement, peripheral neuropathy and myelopathy.7 8 Acute bilateral useless hand syndrome as a presenting feature of vitamin B12 deficiency has not been reported in the literature to date.
Case presentation
A 38-year-old man presented with difficulty in performing fine motor movements with his hands, such as buttoning and unbuttoning of shirts, tearing chapatis, writing and manipulating objects with his fingers, for the past 7 days. He had no history of weakness and/or stiffness in any of the limbs or tingling or numbness in the hands or feet. There was no history of exposure to toxins or drugs, and no high-risk behaviour. There was no history of similar episodes and no chronic illness in the past. He had no diabetes, no hypertension and was a strict vegetarian with no addictions.
The patient was thin-built, and his vitals and general examination were normal. On neurological examination, higher mental function, cranial nerves and fundus examination were normal. Nutrition, tone and power in all four limbs were normal. There was impairment of dexterity in both hands, loss of joint position and sense of vibration in both feet and hands, while pain and temperature sensations were intact. Astereognosis and pseudoathetosis were present in both hands. Deep tendon reflexes were normal in all four limbs except bilateral ankle jerks, which were absent with bilateral flexor plantar response. Romberg's test was positive. Gait was normal, and systemic examination including skull and spine was normal.
Investigations
On investigations, haemoglobin was 12.4 g/L, total leucocyte count (TLC) 8000/mm3, platelet count 50 000/mm3 and mean corpuscular volume (MCV) 107.6 (normal range 80–96 fL). Peripheral blood smear showed presence of macrocytes and reduced platelet counts. Renal and liver function tests, random blood sugar, serum electrolytes and thyroid function tests were normal. ELISA for HIV, HBsAg and hepatitis C virus was normal. Serum vitamin B12 was low (130 pg/mL). Routine cerebrospinal fluid (CSF) examination was normal and CSF virology study for herpes simplex virus,1 2 cytomegalovirus, Epstein-Barr virus and mumps was negative. Nerve conduction studies showed absent sural sensory nerve action potentials (SNAPs) and decreased amplitude of bilateral median and ulnar SNAPs. Pattern reversal visual-evoked potentials were normal.
On the basis of history, examination and laboratory features, a provisional diagnosis of pseudoathetosis due to non-compressive myelopathy (vitamin B12 deficiency) was made. The patient was subjected to cervical spine MRI, which showed abnormal hyperintensity on sagittal T2-weignted (T2W) images in the cervical spinal cord, which was localised to posterior columns from C3 to C7, not contrast enhancing and, on axial T2W MRI, there was a classical ‘inverted V sign’ in posterior columns (figure 1A, B). T2W and fluid-attenuated inversion recovery sequence on MRI of the brain did not show any white matter hyperintensity.
Figure 1.
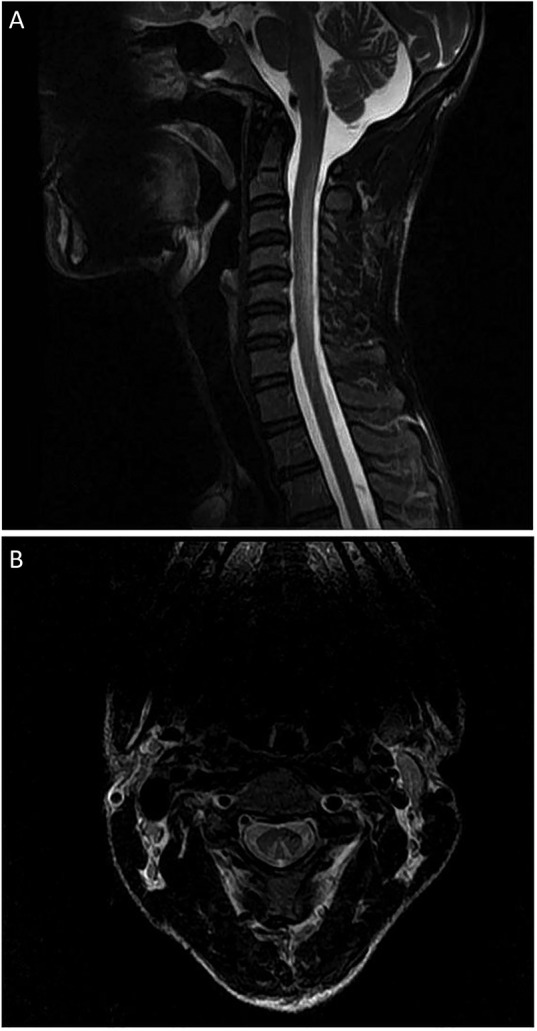
(A) T2-weighted (T2W) sagittal section MRI of the cervical spine showing hyperintensity involving the posterior columns from C2 to C7 level. (B) Axial T2W cervical spine MRI showing a typical inverted ‘V’-shaped hyperintensity.
After neuroimaging, a diagnosis of cervical non-compressive predominantly posterior myelopathy due to vitamin B12 deficiency was made.
Treatment
The patient received treatment with intramuscular injection of vitamin B12 (cyanocobalamine) 1000 µg daily for the first 7 days, then weekly for 4 weeks, followed by monthly for 12 months. Along with this, as he was strictly vegetarian, the patient was also advised to have vegetarian food products rich in vitamin B12, such as legumes, as well as milk and milk products.
Outcome and follow-up
The patient started showing significant improvement on follow-up at 4 weeks and, when examined at 8 weeks, he was completely relieved of his symptoms. When he was examined at 9 months he was doing well.
Discussion
Useless hand syndrome in patients with MS has been described by Oppenheim.9 It is a phenomenon in which the hand is functionally impaired due to posterior column deficits leading to clumsiness of complex finger movements and loss of manual dexterity. This phenomenon has been reported in patients with MS and cervical spondylosis. Unilateral involvement has been noted to be more common than bilateral involvement in patients with MS.1–5
The pathophysiology behind useless hand syndrome due to posterior cervical cord involvement remains unclear. It has been hypothesised that there is a centre for sensorimotor integration in the high cervical cord; this centre works to convey kinaesthetic and discriminative sensations necessary to guide fine finger movements. The propriospinal neurons in the cervical cord receive afferent signals from cutaneous forelimbs and efferent signals from the corticospinal tract, and integrate these signals, contributing to executing purposive forelimb movements at a premotoneuronal level.9 10
Neurological involvement is very common in vitamin B12 deficiency, reported in 40–70% of patients. The most commonly affected sites are the brain, optic nerve, spinal cord and peripheral nerves, in varying combinations; among these, the most common and important is involvement of the posterior and lateral columns of the cervical and thoracic spinal cord. These patients can have gradual or subacute onset paraesthesias in the feet, followed by the hands; later, patients may develop spastic weakness of both lower limbs and have significant ataxia. Behavioural and visual symptoms may also be present, along with myeloneuropathy. The mechanism behind myeloneuropathy is due to accumulation of methyl malonyl CoA and abnormal fatty acids that constitute the myelin sheath, leading to defective myelination of the neural sheath. Neuropathological study has demonstrated spongiform changes with foci of myelin and axonal destruction mainly in the posterior and lateral columns. The other features of vitamin B12 deficiency are macrocytic anaemia, skin pigmentation and atrophic glossitis, however, acute onset clumsiness of both hands due to involvement of the posterior column as the presenting symptom of vitamin B12 deficiency is not commonly seen.7 8 11 12
Vitamin B12 deficiency is quite common in pure vegetarians, as few vegetarian products are good sources of vitamin B12. So it is very important for vegetarians to have foods rich in vitamin B12, such as legumes and milk products. This measure can protect vegetarians from various clinical manifestations due to vitamin B12 deficiency.
In our patient, there was an acute history of clumsiness in both hands with significant deterioration on eye closure, without any pyramidal or extrapyramidal findings, and MRI findings were suggestive of abnormal T2W hyperintensity in the posterior and lateral cervical cord, without contrast enhancement. Axial T2W imaging showed a classical inverted ‘V’ sign.13 14 Our patient had a classic MRI picture of vitamin B12 deficiency, which was further corroborated by increased MCV and low vitamin B12 level. MRI of the brain was normal and the patient had significant improvement after supplementation of vitamin B12. Early recognition and treatment can reverse all symptoms of this condition affecting the nervous system, so timely diagnosis of vitamin B12 deficiency is very important.
Learning points.
Useless hand syndrome is defined as difficulty in executing distal fine movements of the hands in the absence of any weakness (pyramidal) or extrapyramidal involvement. It is predominantly attributed to involvement of the posterior columns of the spinal cord.
Common causes of this syndrome are multiple sclerosis and cervical spondylosis.
Vitamin B12 deficiency can present as acute onset useless hand syndrome due to involvement of the posterior cord early on in the disease course.
MRI of the spinal cord shows classic abnormalities in the posterolateral region suggestive of demyelination of the posterior and lateral columns.
Early diagnosis and treatment play an important role in the reversibility of neurological deficits; delayed treatment can result in irreversible disabling neurological impairment.
Footnotes
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hashimoto R, Kanho M, Fujimoto K et al. [Left hand clumsiness due to disturbance of kinaesthesia after damage to the dorsal column of the high cervical cord]. Rinsho Shinkeigaku 1997;37:319–25. [PubMed] [Google Scholar]
- 2.Pou Serradell A, Roquer Gonzalez J, Perich Alsina X. Acute posterior cord lesions in multiple sclerosis: an MRI study of the clinical course in 20 cases. Rev Neurol (Paris) 2000;156:1126–35. [PubMed] [Google Scholar]
- 3.Hamada E, Okamoto K, Okuda B. A case of multiple sclerosis with bilateral useless hand syndrome as a main clinical feature. Rinsho Shinkeigaku 2005;45:211–15. [PubMed] [Google Scholar]
- 4.Rae-Grant AD. Unusual symptoms and syndromes in multiple sclerosis. Continuum (Mimeep Minn) 2013;19(4 Multiple Sclerosis):992–1006. 10.1212/01.CON.0000433287.30715.07 [DOI] [PubMed] [Google Scholar]
- 5.Kamogawa K, Okuda B. Useless hand syndrome with astereognosis in multiple sclerosis. Mult Scler Relat Disord 2015;4:85–7. 10.1016/j.msard.2014.09.212 [DOI] [PubMed] [Google Scholar]
- 6.Nakajima M, Hirayama K. Midcervical central cord syndrome: numb and clumsy hands due to midline cervical disc protrusion at the C3–4 intervertebral level. J Neurol Neurosurg Psychiatry 1995;58:607–13. 10.1136/jnnp.58.5.607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Healton EB, Savege DG, Brust JC et al. Neurologic aspects of cobalamin deficiency. Medicine (Baltimore) 1991;70:229–45. 10.1097/00005792-199107000-00001 [DOI] [PubMed] [Google Scholar]
- 8.Savage DG, Lindenbaum J. Neurological complications of acquired cobalamin deficiency: clinical aspects. Baillieres Clin Haematol 1995;8:657–78. 10.1016/S0950-3536(05)80225-2 [DOI] [PubMed] [Google Scholar]
- 9.Oppenheim H. Discussion on the different types of multiple sclerosis. Br Med J 1911;2:729–33. [Google Scholar]
- 10.Alstermark B, Górska T, Johannisson T et al. Effect of dorsal column transection in the upper cervical segments on visually guided forelimb movements. Neurosci Res 1986;3:462–6. 10.1016/0168-0102(86)90039-8 [DOI] [PubMed] [Google Scholar]
- 11.Misra UK, Kalita J. Comparison of clinical and electrodiagnostic features in B12 deficiency neurological syndromes with and without antiparietal cell antibodies. Postgrad Med J 2007;83:124–7. 10.1136/pgmj.2006.048132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yuen TS. Simon RP, Deficiency diseases of the nervous system. In: Daroff RB, Fenichel GM, Jankovic J, eds. Bradley's neurology in clinical practice. Vol II 6th edn 2012:1343. [Google Scholar]
- 13.Ravina B, Loevner LA, Bank W. MR findings in subacute combined degeneration of the spinal cord: a case of reversible cervical myelopathy . AJR Am J Roentgenol 2000;174:863–5. 10.2214/ajr.174.3.1740863 [DOI] [PubMed] [Google Scholar]
- 14.Kumar A, Singh AK. Teaching NeuroImage: Inverted V sign in subacute combined degeneration of spinal cord. Neurology 2009;72:e4. 10.1212/01.wnl.0000338663.59433.9c [DOI] [PubMed] [Google Scholar]