

Abstract
Cardiac lipomas are extremely rare in the heart diseases and only few present with a wide spectrum of clinical signs, including life-threatening arrhythmias and sudden death. We report a 48-year-old woman who with a 2-year history of recurrent dyspnea with mild anemia was admitted to our hospital as a huge mass was found in her mediastinum. After complete surgical tumor resection, she was recurred at the fifth year. This case underlines the giant cardiac lipomas had a slightly higher risk of recurrence over the next five years.
Keywords: Cardiac, lipoma, recurrence, surgery
Introduction
Cardiac lipoma is an extremely rare disease, which majority is benign and only few cause symptoms. Recurrence cardiac lipoma is even rarer. Here the investigators present a big impressive cardiac lipoma which was been made surgical resection and relapsed just short of five years.
Case presentation
In 2009, a 48-year-old woman with a 2-year history of recurrent dyspnea with mild anemia was referred to our hospital with a huge mass (The diameter of the mass was about 15 cm and the CT value arranged from -85 to -114 similar to that of fat. Histology confirmed the diagnosis of a benign, cardiac lipoma after the operation) was found in the right ventricular wall, and the heart was jostled to right [1]. She had any family history of heart tumor problems, going backfour generations. The operation was performed on extracorporeal circulation, and excised most of the tumor (It was impossible to remove the entire tumor because of its integration with and partly immersed into left and right ventricular wall). She was asymptomatic at routine medical follow-up after 4 years with no recurrence of the tumor.
In 2014, this patient appears dyspnea once again at five years after initial excision, and the suspicion of a new tumor was raised. Transthoracic echocardiography study revealed two new denticulate slightly dense-echo masses, however this time the location was on the left atrium and the right atrium (Figure 1A and 1B). The dense-echo masses findings were confirmed recurrent giant cardiac lipoma by 16-slice computed tomography angiography (CTA) and 320-slice CTA (Figure 2A and 2B). Secondary surgical removal of the masses was not recommended, and she has been suggested undergone cardiac transplantation.
Figure 1.
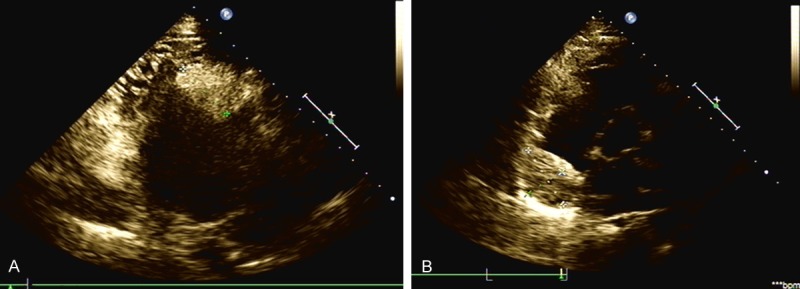
Transthoracic echocardiograms showing two new denticulate slightly dense-echo masses on the left atrium (A) and the right atrium (B).
Figure 2.
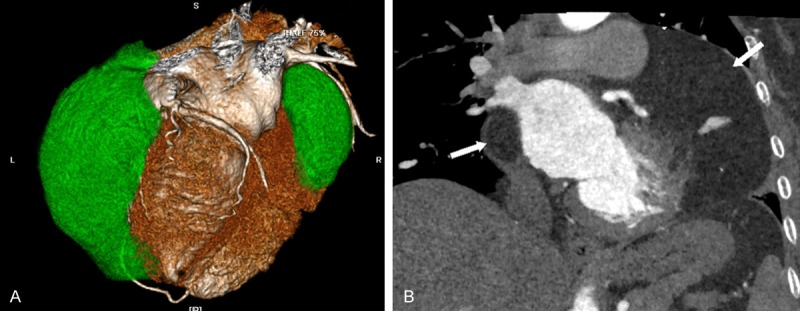
320-slice computed tomographic angiography scan confirmed recurrent giant cardiac lipoma on the left atrium (104 mm×93 mm×71 mm) and the right atrium(67 mm×54 mm×35 mm), heart tumors located at the green areas on volume rendering of three-dimensions (A) and the white arrow on frontal plane scan (B).
Comments
Primary tumors of the heart are rare, and the incidence varies between 0.0017 and 0.19% in unselected autopsy studies. Like other organs, the heart can be affected by tumor and its relapses [2]. Three quarters of primary heart tumors are benign and half of them are atrial myxomas. Other benign tumors are lipoma, papillary fibroelastoma, rhabdomyoma and fibroma [3]. Giant cardiac lipoma, especially recurrent giant cardiac lipoma is extremely rare in the heart diseases. Cardiac lipoma is well-encapsulated tumors typically composed of mature fat cells and it can occur in almost any location of the heart [1,4]. The risk of a cardiac lipoma relapse was not documented in the reported literature. Reasons for relapses may: inadequate resections, intraoperative implantation of parts of the tumor and multi-located tumor origin. Other heart tumors suggest that, natural history of recurrent giant cardiac lipoma required long-term echocardiography follow-up of patients and their relatives. High incidence of recurrence is observed in the younger age group, with familial predisposition [3], though this patient with no family history of heart tumor problems. As with sporadically occurring giant cardiac lipoma a resection of the cardiac tumor and its relapses should be performed cardiac transplantation. Our report highlights the importance of a comprehensive cardiac 320-CTA approach that can provide the clinician not with only an accurate description of the imaging findings, and the giant cardiac lipoma had a slightly higher risk of recurrence over the next five years.
Disclosure of conflict of interest
None.
References
- 1.Zhu SB, Zhu J, Liu Y, Wang RP. Surgical treatment of a giant symptomatic cardiac lipoma. J Thorac Oncol. 2013;8:1341–1342. doi: 10.1097/JTO.0b013e3182a12a6a. [DOI] [PubMed] [Google Scholar]
- 2.Andersen RE, Kristensen BW, Gill S. Cardiac leiomyosarcoma, a case report. Int J Clin Exp Pathol. 2013;6:1197–1199. [PMC free article] [PubMed] [Google Scholar]
- 3.Marina K, Vasiliki KE, George S, Vasiliki V, Androniki T, Abraham G, Loukas K, Andreas K, Alkiviadis M. Recurrent cardiac myxoma in a 25 year old male: a DNA study. World J Surg Oncol. 2013;11:95. doi: 10.1186/1477-7819-11-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ganame J, Wright J, Bogaert J. Cardiac lipoma diagnosed by cardiac magnetic resonance imaging. Eur Heart J. 2008;29:697. doi: 10.1093/eurheartj/ehm476. [DOI] [PubMed] [Google Scholar]