

Abstract
Terrible triad of the elbow is characterized as posterior dislocation of the elbow joint accompanied by the fractures of the radial head and coronoid process of the ulna, which is rarely seen in clinical practice, especially because the mild fracture is barely detected by imaging method In this study, we reported one case of serious complex bilateral elbow injury, presenting with unilateral typical terrible triad of the elbow and suspected terrible triad of the elbow complicated with olecranon fracture on the other side. Clinical experience was obtained during the diagnosis and treatment procedures.
Keywords: Coronoid process fracture, radial head fracture, terrible triad of the elbow
Case history
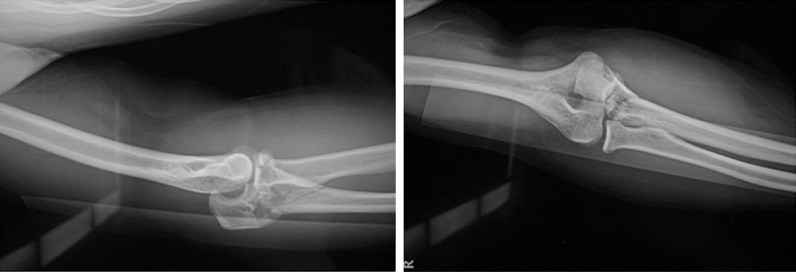
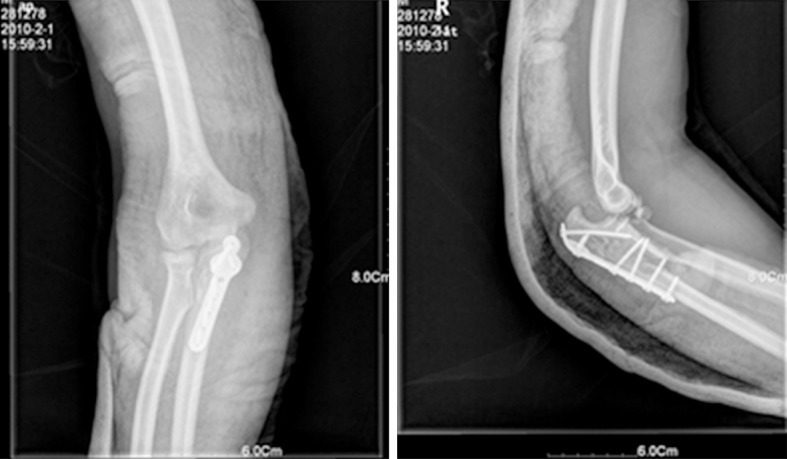
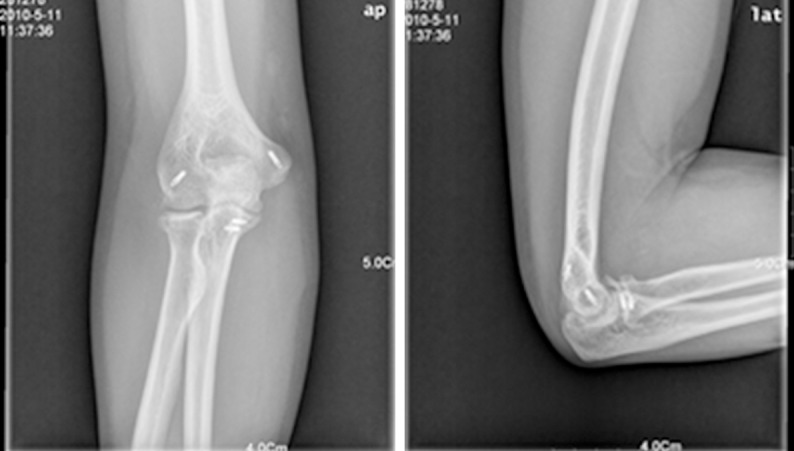
The male patient, aged 26 years, presented with significant swelling of bilateral elbows accompanied by acute pain and difficulty in elbow joint movement after he fell off the truck and touched the ground using his hands. No signs of neurological disorder or circulatory disturbance were noted in the bilateral upper limbs. Anterolateral X-ray examination in the emergency out-patient revealed dislocation of the left elbow joint, left radial head fracture, coronoid process fracture of the left ulna (Figure 1), subluxation of the right elbow joint and right olecranon fracture (Figure 2). Three dimensional CT reconstruction of the left elbow joint revealed dislocation of the left elbow joint, left radial head fracture and coronoid process fracture of the left ulna (Figure 3). He was treated with emergent surgery under general anesthesia at 6 h after injury. He underwent closure and reduction of dislocation of the left elbow joint via combined approach of medial and lateral incision. Lateral incision surgery (Kocher approach) found humeral lateral epicondyle avulsion of the lateral collateral ligaments. The reduction of type II radial head fracture was performed (Mason classification [2]) and fixed using 2 mm absorbable stick in diameter. The lateral collateral ligament injury was repaired using 2 mm rivet in diameter. Examination of distal medial incision stretching to anterior elbow revealed avulsion of the medial humeral epicondyle, ulnar coronoid process fracture complicated with avulsion fracture of the anterior joint capsule (type I according to Regan and Morrey classification [8]). The ulnar coronoid process fracture and anterior elbow joint capsule were repaired by two pieces of 2 mm rivets in diameter, and the medial collateral ligament injury was equally repaired using 2 mm rivet in diameter. Intraoperative examination found that the elbow joint was unstable and inclined to dislocation. Hence, the humeroulnar joint was fixed at 90° elbow bending using 2 pieces of 2 mm Kirschner wire and gypsum (Figure 4). The right elbow joint was subject to posterior incision of the proximal end of ulna, exposure of olecranon fracture, reduction and fixation using olecranon bone fracture plate, and the elbow joint was fixed when the elbow was bent at 90° using gypsum postoperatively. Dislocation of the right elbow joint was noted at 1 d after surgery (Figure 5). The patient underwent closure and reduction of the right elbow joint and fixed by 2 mm Kirschner wire under brachial plexus aneasthesia at emergent out-patient (Figure 6).
Figure 1.

Frontal and lateral view revealing typical triad of the left elbow.
Figure 2.
Lateral and Frontal view revealing atypical triad complicated with olecranon fracture of the right elbow.
Figure 3.
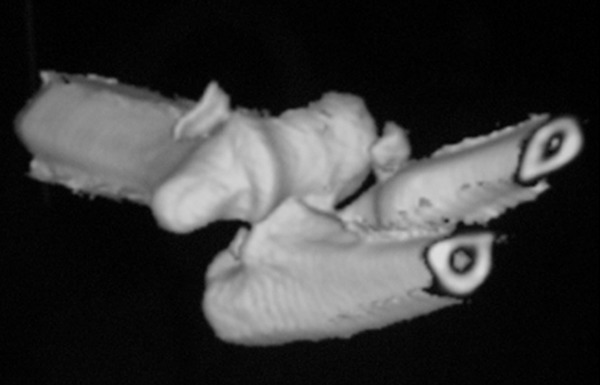
Three dimensional CT scan revealing typical triad of the left elbow.
Figure 4.

Frontal and Lateral view revealing the left elbow after surgery.
Figure 5.
Frontal and Lateral view revealing the dislocation of elbow joint of the right elbow at 1 day after surgery.
Figure 6.

Frontal and Lateral view revealing Kirschner wire fixation of elbow joint after closure and reduction of the right elbow.
Postoperative processing
The patients were orally administered with indomethacin 25 mg tid to prevent the incidence of heterotopic ossification. The patients were told to stretch their fingers and clench their fists to alleviate finger edema. At 4 weeks after surgery, the Kirschner wire fixed in bilateral elbow joints was removed. The patients were instructed to exercise the function of elbow joint guided by the rehabilitation therapists.
Results
No wound infection was noted in bilateral elbows. No vascular injury was observed. Stage I healing was obtained. At postoperative 10 months, fracture healing was seen in bilateral elbow joints (Figures 7, 8). The patients reported no severe pain in bilateral elbow joint, had a flexion-extension arc of the left elbow ranged from 5° to 140°, 75° pronation and 85° supination in the left forearm rotation (160° in total), 40°-120° for the flexion-extension arc of the right elbow, and 80° pronation and 80° supination for the right forearm rotation (160° in total). No apparent restriction of joint function was noted (Figure 9). Mayo elbow performance score (MEPS) [5] revealed that 95 points were obtained for the left elbow and 80 points for the right elbow. Repeated X-ray scan revealed that no heterotopic ossification could be noted during the fracture healing process of bilateral elbow joints.
Figure 7.
Fracture healing of the left elbow at 10 months after surgery.
Figure 8.

Fracture healing of the right elbow at 10 months after surgery.
Figure 9.

Joint function of bilateral elbows.
Discussion
The concept of “terrible triad of the elbow” was first proposed by Hotchkis in 1996 [3]. Armstrong re-defined and complemented the concept of “terrible triad of the elbow” after retrospectively analyzing the injury characteristics. He considered that it referred to posterior dislocation of humeroulnar joint accompanied by coronoid process fracture of the ulna, radial head fracture and lateral collateral ligamentous injuries. Besides, it probably occurs in the internal collateral ligaments, tendon origin, forearm flexor, pronator teres orgin or capitulum humeri and incisura trochlearis ulnae bone and soft bone injury. Terrible triad of the elbow is severe trauma caused by high energy, belonging to one of the complicated fracture dislocation of elbow joint. It is frequently noted in the young population. It mainly results from falling and traffic accident. As complex elbow joint injury, early surgical intervention is likely to yield relatively favorable clinical outcomes [1,6]. The operation aims to reconstruct the stability of elbow articular bone and repair internal and lateral collateral ligaments and joint capsule. In 2004, Pugh et al. [4,7,9] proposed the standard surgical protocol to treat terrible triad of the elbow: (1) The anatomical structure of humeroradial joint should be restored (The radial head should be retained as possible. Otherwise, prosthesis replacement may be considered); (2) Internal fixation should be conducted for coronoid process fracture; (3) The lateral collateral ligamentous and joint capsular injuries should be repaired; (4) The internal collateral ligaments should be repaired selectively; (5) Hinged external fixation using a stent should be supplemented; (6) Early functional exercise should be delivered to avert the incidence of anchylosis. Surgical approach should be determined based on the structure to be repaired. Elbow lateral and posterior approaches are mainly adopted. In recent years, the combination of elbow lateral and elbow frontomedial approaches has been more frequently chosen. elbow lateral approach acts to repair the fracture of radial head and lateral collateral ligaments, and frontomedial routes facilitates the repairing of coronal head and anterior joint capsular, and internal collateral ligamentous injuries. This combined technique yields mild injury, is convenient to expose the injury and lead to few surgical complications [10].
The patient in this study was diagnosed with typical terrible triad of the elbow. X-ray and three dimensional CT scans revealed the signs of dislocation of elbow joint, radial head fracture and coronoid process fracture of the ulna. The medial and lateral incision of the elbow joint was made, the radial head fracture, lateral collateral ligaments, coronoid process fracture of the ulna, anterior joint capsule and internal collateral ligamentous injuries were repaired in sequence. Nevertheless, elbow joint instability was still observed during intraoperative examination. Due to the lacking of external fixation stent, Kirschner wire was adopted to fix the humeroulnar joint and achieved favorable clinical efficacy. Since the injury of the elbow joint was misdiagnosed prior to surgery, simple fixation alone was conducted for olecranon fracture treatment. After the surgery, elbow joint instability was noted. Postoperative X-ray re-examination revealed the manifestations of coronoid process fracture of the ulna and slight fracture of radial head. Although Kirschner wire fixation was delivered additionally, the postoperative performance of right elbow joint was significantly worse compared with that of the left side. We concluded that CT scan should be performed for patients with complex elbow articular fracture to avoid missing the delicate fracture, especially type I fracture in the coronal process of the ulna and radial head. Otherwise, it tends to increase the difficulty of treatment and yield poor prognosis. In addition, Kirschner wire fixation of the humeroulnar joint is a feasible approach for managing postoperative elbow joint instability in patients with terrible triad of the elbow.
Conclusion
It is highly likely to cause missed diagnosis and misdiagnosis of terrible triad of the elbow due to the complex nature. Unsuitable therapy tends to lead to severe sequela to the patients. Three dimensional CT reconstruction should be used as conventional examination. Kirschner wire fixation of humeroulnar joint is an efficacious approach for resolving postoperative elbow joint instability.
Disclosure of conflict of interest
None.
References
- 1.Armstrong AD. The terrible triad injury of the elbow. Current Opinion in Orthopaedics. 2005;16:267–270. [Google Scholar]
- 2.Hotchkiss RN. Displaced fractures of the radial head: internal fixation or excision? J Am Acad Orthop Surg. 1997;5:1–10. doi: 10.5435/00124635-199701000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Hotchkiss RN. Fractures and dislocations of the elbow. In: Rockwood CA, Green DP, Bucholz RW, Heckman JD, editors. Rockwood and Green’s fractures in adults. 1, 4th edition. Philadelphia: Lippincott-Raven; 1996. pp. 929–1024. ISBN-10: 0397516029. [Google Scholar]
- 4.McKee MD, Pugh DM, Wild LM, Schemitsch EH, King GJ. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am. 2005;87(Suppl 1):22–32. doi: 10.2106/JBJS.D.02933. [DOI] [PubMed] [Google Scholar]
- 5.Morrey BF, Adams RA. Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Joint Surg Am. 1992;74:479–490. [PubMed] [Google Scholar]
- 6.O’Driscoll SW, Jupiter JB, King GJW. The Unstable Elbow*†. The Journal of Bone & Joint Surgery. 2000;82:724–724. [Google Scholar]
- 7.Pugh DM, Wild LM, Schemitsch EH, King GJ, McKee MD. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am. 2004;86:1122–1130. doi: 10.2106/00004623-200406000-00002. [DOI] [PubMed] [Google Scholar]
- 8.Regan W, Morrey BF. Classification and treatment of coronoid process fractures. Orthopedics. 1992;15:845–848. doi: 10.3928/0147-7447-19920701-09. [DOI] [PubMed] [Google Scholar]
- 9.Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg. 2002;84:547–551. doi: 10.2106/00004623-200204000-00006. [DOI] [PubMed] [Google Scholar]
- 10.Zhang C, Zhong B, Luo C. Treatment strategy of terrible triad of the elbow: Experience in Shanghai 6th People’s Hospital. Injury. 2014;45:942–948. doi: 10.1016/j.injury.2013.12.012. [DOI] [PubMed] [Google Scholar]