

Abstract
The zebra guidewire is widely used in endoscopic surgery. Because of its central mental core, it is not easy to break or shear off within the urinary tract. We report a case about the breakage of zebra guidewire in ureteroscopy (URS) with Holmium: YAG laser lithotripsy. It is easily to be managed by percutaneous access or open surgery. For the purpose of minimal invasiveness and risk, we performed a retrograde flexible ureteroscopy and extracted it successfully without any complication. To our knowledge, this is the first case report on flexible ureteroscopy to remove the residual tip of damaged guidewire in renal.
Keywords: Zebra guidewire, Holmium: YAG laser, flexible ureteroscopy, management
Introduction
Zebra guidewire is frequently used in endoscopic surgery. The zebra guidewire is made of central nitinol core and hydrophilic coating, which has a favorable flexibility. We report a case about the zebra guidewire broke and sheared off within the kidney in ureteroscopy (URS) with Holmium: YAG (Ho: YAG) laser lithotripsy, which was managed by successive retrograde ureteroscopic procedures without usually antegrade percutaneous access or open surgery.
Case report
A previously healthy 46 years old man was admitted to hospital with right constant flank pain for the last three days. The plain X-ray of the kidneys, ureters, and bladder (KUB) and intravenous urography (IVU) revealed a right proximal ureteral stone with mild hydronephrosis and ureteric dilation. An URS with Ho: YAG laser lithotripsy was performed. Briefly, a zebra guidewire was first inserted into the renal pelvis as the safety guidewire, then an 8/9.8F rigid ureteroscope was placed into the level where the stone was located. A 360-µm holmium laser fiber with an energy level of 0.5 to 0.8 J and a rate of 10 to 20 Hz was used for the stone fragmentation. After the stone was completely fragmented, over this guidewire a 5F D-J stent was inserted. On postoperative day 3, the KUB revealed the position of D-J stent was properly positioned, however, a high density ancistrous foreign body was found near the D-J stent (Figure 1). The urologist checked the zebra guidewire used in previous operation, and found the tip of guidewire was missing. Thus the patient was transferred to our hospital. The urinalysis showed red blood cell +++, white blood cell 0-2/HP and no pus cell presented. Computed tomography (CT) revealed a high density foreign body located in the right renal pelvis and upper calices (Figure 2). Considering usually retrograde rigid-ureteroscopic management could be difficult because of the feature of the collecting system anatomy in this situation and minimizing the operation invasiveness and risk, a flexible ureteroscopy (FURS) was conducted to remove the residual tip of the guidewire (Figures 3, 4). Briefly, a routine real-time on-table image was performed to confirm the location of residual tip and D-J stent followed by a retrograde ureteroscopy to remove the D-J stent. For protecting the ureteric mucosa, a flexible ureteroscope (URF-P5, Olympus, Japan) was placed through a ureteral access sheath (AQ Fus-120045 12/14 Fr; Cook Medical, America) under a direct visualization. Through the working channel of the flexible ureteroscope, a forceps was inserted and deployed to coaxially grasp the residual tip of guidewire. Whether a forceps could grasp and extract a residual tip depended on the angle between the tip axis and the extraction device. Once grasping the tip coaxially, the forceps was gently retrieved together with the flexible ureteroscope, and the grip strength of the forceps was sufficient to provide enough force to reposition the residual tip outside the access sheath. All the procedures were carried out under general anesthesia. Patient was discharged on the same day as his procedure without any complication.
Figure 1.

KUB showed the tip of zebra guidewire (A) and D-J stent (B) before operation.
Figure 2.
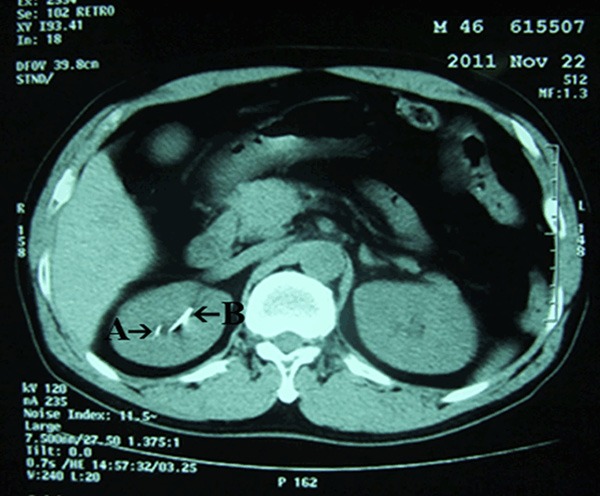
CT scan of the abdomen showed the tip of zebra guidewire in the right renal pelvis and upper calices (A) and D-J stent in right ureter (B).
Figure 3.
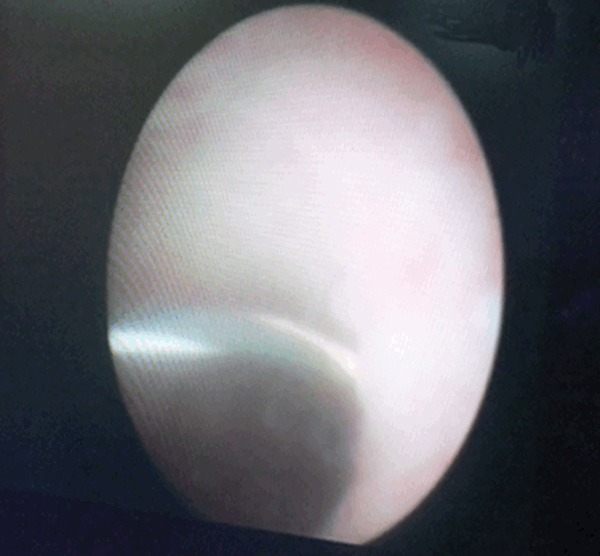
Direct visualization of residual tip by FURS intraoperatively.
Figure 4.
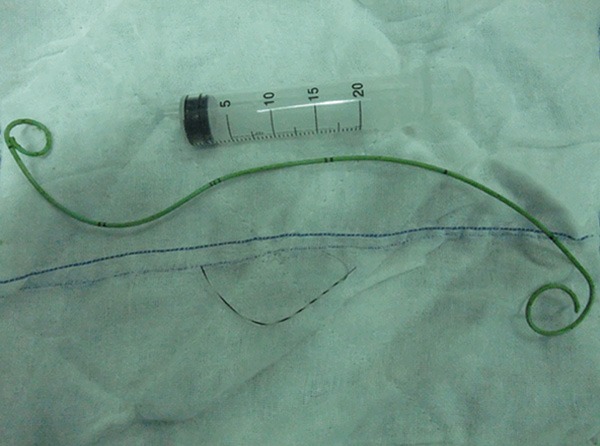
The removed complete tip of zebra guidewire and D-J stent after operation.
Discussion
Guidewires, zebra guidewire especially, is a frequently-used tool of many urinary tract procedures. During endoscopic treatment, guidewires are routinely used to provide access or act as a safety guidewire over which stents can later be passed. The central core of the zebra guidewire is mental string, so it is not easy to break or shear off within the urinary tract. Similar incidents involving zebra guidewire breakage have been rarely reported.
Foreign bodies of the upper urinary tract are silent only exceptionally. Infection is generally associated with this condition. General malaise, fever and flank pain are the most common presenting symptoms. The urinalysis may be completely negative for blood and/or pus if the foreign body does not penetrate the pelvis or ureter [1]. Retained foreign bodies can be a nidus for stone formation and as a continued irritant in collecting system [2]. The using of KUB, ultrasound and CT is the key for the diagnosis, but sometimes excretory or retrograde urography may provide additional information and show surprising findings and unexpected radiolucent object [3].
Removal of all retained foreign bodies in a single operation should be the optimal goal during a surgery [4]. The suitable treatment depends on factors such as the size and position of the object, parenchymal injury, the extent of local inflammation, and the stone formation should also be considered as well. URS is generally recognized as an effective procedure both for the diagnostic and therapeutic purpose. Direct visualization of the object is achieved, followed by its prompt removal using suitable extraction tools [5]. But in some situations, retrograde ureteroscopic approach may be difficult, so percutaneous access is preferred. If the situation can’t be managed by minimal invasive surgical technology based methods, open surgeries such as pyelotomy can also be taken into consideration [4].
In endourologic stone treatment, the Ho: YAG laser is considered as the gold standard lithotripsy because of its ability to effectively fragment urinary calculi of all compositions [6]. Energy from a Ho: YAG laser is absorbed remarkably by water resulting in less tissue penetration (≤0.5 mm) [7]. However, accidental damage to guidewire may occur when the laser fiber tip is directly onto or even closed to the guidewire during the laser-firing period. Beeves et al [8] reported that the damage caused by Ho: YAG laser was dependent on pulse energy, cumulative energy and distance. Freiha et al [9] demonstrated that at the greater distance or incident angle between the laser fiber tip and guidewire the less likely the damage occur. Their experiments showed the reasonable safe distance between the laser fiber and guidewire or mucosa during ureterscopic procedure was ≥1 mm. The tip of zebra guidewire is potential faulty in construction so that it can be manipulated readily at the time of access. So any extra-damage to the metal core could weaken it and induce breakage during removal, especially in violent manipulation or tortuous ureters. During the Ho: YAG lithotripsy, the guidewire is usually parallel to the Ho: YAG laser fiber, so it is important to keep an adequate distance between the guidewire and the laser fiber. Meanwhile, careful inspection of the integrity of the guidewire before and after operation is necessary to avoid fractured guidewire retaining and delayed diagnosis. When necessary, imaging of the patient or even repeat URS under the same anesthesia before terminating operation should also be considered.
Disclosure of conflict of interest
None.
References
- 1.Campbell EW. Foreign bodies in the urinary tract. In: Campbell MF, editor. Urology. 2nd edition. Philadelphia: W. B. Saunders; 1963. pp. 775–795. [Google Scholar]
- 2.Ahn J, Trost DW, Topham SL, Sos TA. Retained nephrostomy thread providing a nidus for atypical renal calcification. Br J Radiol. 1997;70:309–310. doi: 10.1259/bjr.70.831.9166059. [DOI] [PubMed] [Google Scholar]
- 3.Arndt van O, Jean BK. Clinical management of foreign bodies of the genitourinary tract. J Urol. 2000;164:274–287. doi: 10.1097/00005392-200008000-00003. [DOI] [PubMed] [Google Scholar]
- 4.Michael LE, Keith LL, Marshall LS. Endoscopic management of retained renal foreign bodies. Urology. 2009;73:1189–1194. doi: 10.1016/j.urology.2008.09.010. [DOI] [PubMed] [Google Scholar]
- 5.Gideon L, Mordechai D, Ofper NG. Transected guidewire tip simulating ureteral stone. J Endourol. 2008;22:661–662. doi: 10.1089/end.2007.0348. [DOI] [PubMed] [Google Scholar]
- 6.Honeck P, Wendt-Nordahl G, Häcker A, Alken P, Knoll T. Risk of collateral damage to endourologic tools by Holmium: YAG laser energy. J Endourol. 2006;20:495–497. doi: 10.1089/end.2006.20.495. [DOI] [PubMed] [Google Scholar]
- 7.Vassar G, Chan K, Teichman JM, Glickman RD, Weintraub ST, Pfefer TJ, Welch AJ. Holmium: YAG lithotripsy: photothermal mechanism. J Endourol. 1999;13:181–190. doi: 10.1089/end.1999.13.181. [DOI] [PubMed] [Google Scholar]
- 8.Reeves J, El Husseiny T, Papatsoris A, Masood J, Buchholz N, Birch M. Ureteric guidewire damage by Holmium: YAG laser: preliminary result. Urol Res. 2009;37:7–10. doi: 10.1007/s00240-008-0168-y. [DOI] [PubMed] [Google Scholar]
- 9.Freiha GS, Glickman RD, Teichman JM. Holmium: YAG Laser-induced damage to guidewires: experimental study. J Endourol. 1997;11:331–336. doi: 10.1089/end.1997.11.331. [DOI] [PubMed] [Google Scholar]