

Abstract
Central venous access is a common procedure performed in many clinical settings for a variety of indications. Central lines are not without risk, and there are a multitude of complications that are associated with their placement. Complications can present in an immediate or delayed fashion and vary based on type of central venous access. Significant morbidity and mortality can result from complications related to central venous access. These complications can cause a significant healthcare burden in cost, hospital days, and patient quality of life. Advances in imaging, access technique, and medical devices have reduced and altered the types of complications encountered in clinical practice; but most complications still center around vascular injury, infection, and misplacement. Recognition and management of central line complications is important when caring for patients with vascular access, but prevention is the ultimate goal. This article discusses common and rare complications associated with central venous access, as well as techniques to recognize, manage, and prevent complications.
Keywords: Bleeding, central line, complications, infection, pneumothorax
INTRODUCTION
Central venous access is commonly performed in the care of the critically-ill patient, for a number of indications. However, this routine procedure has complications that every provider must recognize, consider, and be able to manage—either directly or with prompt specialty assistance. These complications can be immediate or delayed in nature. Immediate complications occur at the time of catheter insertion and include vascular, cardiac, pulmonary, and placement complications. Delayed complications include device dysfunction and infection. Peripherally inserted central venous catheters have an altered complication profile that clinicians should consider when deciding on central venous access, but are still associated with the same spectrum of complications as centrally placed catheter.
LITERATURE SEARCH
An extensive literature search was completed using both online and print resources. PubMed and Google Scholar were used to search for relevant articles with search phrases that included central line complications, central venous access complications, central venous catheter complications, subclavian line complications, internal jugular line complications, femoral line complications, and peripherally inserted central catheter (PICC) complications. Articles not published in English were excluded. Additional manual print literature search was conducted using various textbooks, manuals, and journals.
SIGNIFICANCE
Over 5 million central venous catheters are inserted every year in the United States alone, accounting for 15 million central venous catheter days.[1,2] However, this ubiquitous procedure has many associated complications that result in morbidity, mortality, and increased healthcare cost. Government organizations, such as Medicare, no longer reimburse for some preventable complications related to central line placement. Thus, it is imperative that both healthcare providers be aware of the prevention, incidence, and management of the immediate and delayed complications related to central venous access.
IMMEDIATE COMPLICATIONS
Immediate complications related to central venous access include vascular, cardiac, pulmonary, and placement complications. These immediate complications are related to technique at the time of procedure. Recognition and management of immediate complications is paramount as they can often quickly become life-threatening. Overall, number of unsuccessful insertion attempts is the biggest predictor of complications.[3] Ultrasound has significantly reduced the incidence of immediate complications from rates previously as high as 11.8 to 4 to 7%.[4,5]
VASCULAR COMPLICATIONS
Vascular injuries that can occur during catheter placement include arterial injury, venous injury, bleeding, and hematoma. The use of ultrasound and operator experience greatly influence the incidence of vascular complications.[3] Ultrasound guidance has been shown to decrease risk of complication at all access sites.[6,7,8]
Arterial injury occurs in less than 1% of catheter placements.[9] Arterial puncture occurs in 4.2–9.3% of line placements, and is often easily recognized secondary to pulsatile flow, but recognition may be difficult in a hypotensive and critically-ill patient.[9,10] Arterial injury occurs most commonly in femoral catheter placement and least commonly in subclavian placement.[1] Ultrasound is a widely available tool that can aid in proper catheter placement. Multiple studies have demonstrated the benefit of using ultrasound to reduce vascular complications.[11,12,13] Use of ultrasound does not eliminate the risk of arterial puncture, and catheters can still be inadvertently placed into the arterial system [Figure 1].[14,15,16] If there is uncertainty of the punctured vessel, a single lumen catheter can be placed over the guide wire and connected to a pressure transducer to assess for venous waveforms.[1,9]
Figure 1.

Chest X-ray demonstrating a pulmonary artery catheter inadvertently placed via the right carotid artery into the thoracic aorta. Despite pressure waveform monitoring, erroneous placement was not noticed until a post-procedure chest was obtained. The catheter was removed immediately. Follow-up carotid ultrasound was unremarkable for arteriovenous (AV) fistula or pseudoaneurysm. This patient had no residual complications as this complication was immediately recognized and managed
In the instance of an inadvertent arterial catheter placement, leaving the catheter in place and immediate removal with pressure, each carry separate risk. Prolonged arterial catheterization can result in thrombus, neurologic deficits, and stroke. Immediate removal of an accidental arterial catheter can result in uncontrolled hemorrhage, pseudoaneurysm, and arteriovenous (AV) fistula formation; especially in patients who are treated with anticoagulatants or antiplatelet agents.[9] Recent studies have demonstrated that leaving the arterial catheter in place with prompt repair carries less morbidity and mortality than catheter removal with pressure.[17,18] AV fistulas can be treated with image-guided coiling, and pseudoaneurysms can be treated with compression or image-guided thrombin or coil placement. However, fistulas between two large vessels (i.e., carotid artery and internal jugular vein) that are not promptly recognized and grow over time may require direct surgical repair as attempted coil placement, a technique that can be quite challenging in high-flow/high-pressure systems, may result in catastrophic coil embolization. Fortunately, surgery is rarely required for repair.[5] If inadvertent arterial insertion fails to be recognized, further complications can arise from infusion through malpositioned catheters. Rare cases of cerebrovascular events and neurologic deficits have been reported in the literature as a result of infusion through accidental arterial lines.[19,20,21]
While arterial injuries are more common, lacerations of the vena cava, mediastinal vessels, and right atrium have been reported. The proposed mechanism of these injuries is that the guide wire becomes trapped against a vessel wall, and subsequent insertion of dilator or catheter causes injury. The mechanism is such that as the catheter, or dilatator, is advanced; the wire starts to “bow” and push up against the vessel wall and potentially causing a linear laceration which can be much larger (and catastrophic) than a simple puncture. While catheter placement within the atria have higher flow rates and lower rates of thrombosis, the risk of atrial perforation has changed recommendations of catheter placement from within the atria to the atrial-caval junction. Catheter placement in the right atrium, or even, within the right ventricle can also cause local myocardial irritation that might result in supraventricular arrhythmias. Such arrhythmias, if left unrecognized, may result in significant hemodynamic compromise and be very difficult, if impossible, to control pharmacologically. The junction often lies 1.5–2 vertebrate below the carina.[22] Careful attention to resistance during guide wire insertion and direct visualization under fluoroscopy may minimize risk of vessel or atria injury.[9] If a central venous catheter rests against a vessel at an angle of greater than 40°, the risk of perforation increases.[3] If major venous vessel injury occurs, emergent surgical intervention is often needed, and literature related to this topic is largely limited to case reports [Figure 2].[9] Surgery can range from direct suture repair of a perforation to complete vascular reconstruction with autologous tissue or bovine pericardium. Prosthetic material in the venous system is highly thrombogenic, even with aggressive anticoagulation, and unlikely to remain patent for prolonged periods of time and should not be used. For surgical interventions in which the patient is in extremis from hemorrhage, proximal and distal ligation of the bleeding vessel—even if a major vein such as innominate (brachiocephalic) is an appropriate approach and potentially lifesaving technique. Time-consuming and extensive vascular reconstructions in unstable circumstances, in this author's experience, are rarely successful and only delay critical attempts at obtaining both hemostasis and physiologic stability. Major intrathoracic injuries may even require the use of cardiopulmonary bypass to achieve hemodynamic stability and to help define and manage complex injuries and should be available, if possible. This author's experience with management of such injuries suggests that collateral venous return will develop and head and/or limb swelling in the interim is well-tolerated. Delayed reconstruction after damage-control procedures, while theoretically appealing, has not been apparently reported and most likely is not required. For such injuries, the primary goal is to save the life of the patient.
Figure 2.
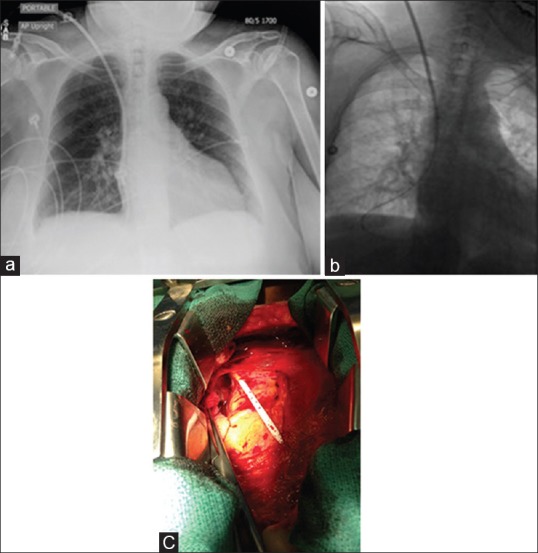
(a) Vascular injury following dialysis catheter placement. Initial chest X-ray after reported uneventful place of a tunneled right internal jugular dialysis line in a 67-year-old female with end-stage renal disease. (b) After initial attempts to access catheter demonstrated that fluid was easily flushed, but not aspirated out of the catheter, attempts to change the “malfunctioning” catheter over a wire suggested that the wire was in the pleural space, and hence the catheter tip was extravascular. (c) Due to concerns of a vascular injury, removal under direct visualization was recommended. Following median sternotomy, the intraoperative findings demonstrated the catheter had punctured the confluence of the right subclavian vein as it entered into the superior vena cava. The catheter was in the right pleural space. The pericardial space had not been violated. Under direct visualization the catheter was removed and the residual hole was repaired with a purse-string and pledgeted suture. Blood loss was minimal and the postoperative recovery was uneventful. Repeat line placement several days later, under fluoroscopic guidance, was uneventful
Hematoma formation has been reported in up to 4.7% of all catheter placements.[10] Hematoma formation is often not life-threatening, but the pleural space and mediastinum are both potential spaces where hematoma may occur. However, such fluid collections can be significant sources of infection in critically-ill patients and may progress to abscess formation. Accumulation of blood in these spaces results in hemothorax and hemomediastinum and may require surgical intervention for image-guided (i.e., computed tomography (CT)) drainage. Oozing related to catheter placement can occur in patients with coagulopathies, and can often be controlled with pressure at the insertion site.[10] Compressible access sites such as the internal jugular or femoral vein cannulation are favored if coagulopathy is a concern.[3]
Additional vascular complications can occur with abnormal anatomy. Congenital persistence of the left-sided vena cava, with or without a bridging innominate vein can occur in up to 0.3% of healthy patients and may be encountered during central line placement via the left subclavian or internal jugular veins.[23,24,25,26,27] This congenital abnormality does not preclude catheter placement; if this is the only reasonable option. However, recognition of this anomaly should prompt consideration of removal of the catheter and right-sided placement to avoid complications that can occur with persistent left-sided vena cava catheter placement. These complications include systemic emboli and cardiac arrhythmias when the left-sided vein drains into the left atrium (versus the more common drainage into the coronary sinus).[27]
Central venous catheter placement can also be complicated by existing central venous devices. Cases of line and wire entanglement with inferior vena cava (IVC) filters have been reported in the literature. Fluoroscopic visualization and interventional radiology are often needed to correct IVC filter entanglement.[28,29] Additionally, catheter entanglement can occur in patients with multiple catheters. Various techniques have been described to remove knotted catheters. Tightening the knot and removal through a dilated insertion site as well as manipulation under fluoroscopy has been described as minimally invasive techniques. However, surgical intervention may be required when multiple lines become entangled.[30,31,32] Additionally, lines can become entrapped by suture placement during cardiothoracic surgery.[33] To avoid this complication that requires reoperation for suture removal, free mobility of all lines should be tested at the conclusion of cardiovascular cases. In general, surgical removal in stable patients is often preferred in any type of catheter entrapment prior to the development of complications, especially if complications are the direct result of attempts at removal (such as catheter fragmentation, further distal embolization to harder to reach areas, such as the right ventricle or pulmonary arteries, or access site injuries). Understandably, there is little literature on the management of these primarily iatrogenic misadventures.
Complications can occur with guide wire placement alone. Cases of wire entrapment and “lost” wires have been reported.[34,35,36,37] Entangled wires may be removed with steady traction or require surgical intervention.[35] Lost wires are often amendable to snaring under fluoroscopic guidance by interventional radiology.[36,37]
PULMONARY COMPLICATIONS
Pulmonary complications that can occur during catheter placement include pneumothorax, pneumomediastinum, chylothorax, tracheal injury, injury to the recurrent laryngeal nerve, and air embolus. Injury to the parietal pleura during central line placement results in pneumothorax and pneumomediastinum. Pneumothorax and pneumomediastinum occur in up to 1% of cases and are most often related to subclavian catheter placement.[1,5,10] Risk factors for pneumothorax are larger catheter size and number of attempted insertions. Pneumothorax can be detected using bedside ultrasound at the time of insertion, but can also be detected on post-insertion upright chest X-ray or CT [Figures 3 and 4].[3] If the pneumothorax is less than <15% in size, it can be managed conservatively with high flow oxygen and close observation. Hemodynamic instability and hypoxia obviate the need for emergent chest tube placement.[10]
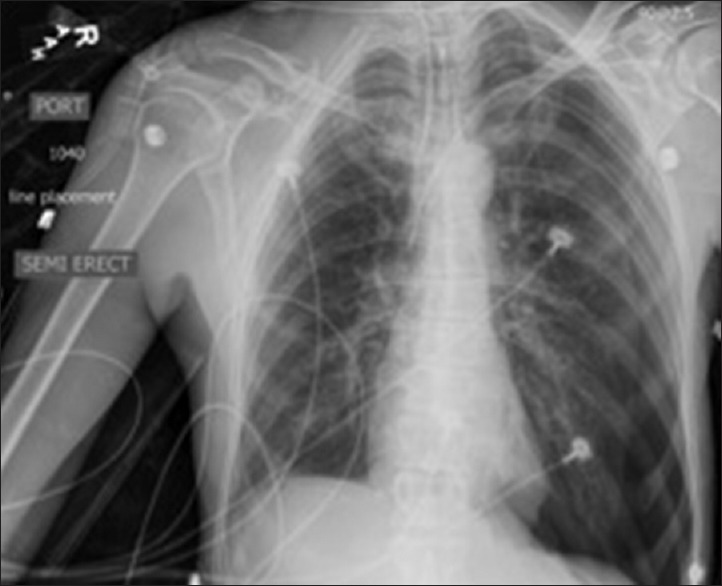
Figure 3.

Contralateral pneumothorax. Pneumothorax following failed chronic port placement on contralateral side
Figure 4.
Ipsilateral pneumothorax. Pneumothorax following left-sided subclavian line placement
Chylothorax and chylopericardium may have also been reported during central venous catheter insertion.[38] Venous congestion or injury to lymphatics can cause this rare complication. Left-sided internal jugular or subclavian access carries a higher risk of lymphatic injury due to the anatomic location of the thoracic duct, but lymphatic injury can still occur with right-sided access. Nitric oxide, thoracoscopic fibrin glue, and percutaneous coiling have all been used to treat lymphatic injury.[3] However, while fortunately exceedingly rare, significant lymphatic injuries, as with other iatrogenic lymphatic or thoracic duct injuries, should have an attempted trial of medical management with total parental nutrition or low-fat enteral nutrition prior to invasive repair attempts.
Nerve injury to the recurrent laryngeal nerve can result from accidental trauma or perineural hematoma. The sympathetic chain, brachial plexus, and phrenic nerve can also be injured in this way. Nerve injury can occur with an incidence of up to 1.6%.[19] Recovery from nerve injury sustained during central venous catheter placement can take up to 6–12 months.[3,19]
Tracheal injuries can be the direct result of inadvertent puncture of the trachea while trying to gain vascular access with either a “finder” needle or the larger bore needle used to advance the guide wire.[39,40] Such injuries are of little significance, unless the patient is mechanically ventilated. Needle punctures of a endotracheal or trachesostomy cuff may result in a clinically apparent air leak, and hence require tube change. For patients requiring mechanical ventilation with high airway pressures, punctures below an endotracheal tube cuff may result in progressively developing pneumomediastinum and/or subcutaneous emphysema. While this might be radiographically and clinically concerning; rarely is it a clinically relevant problem. Unless associated with a pneumothorax, therapy is rarely indicated and the air will reabsorb over time as airway pressures improve. Advancing the endotracheal tube, if possible, or replacing with a long trachesotomy tube might help control ongoing transtracheal airleaks.[41]
Air embolism can occur during catheter insertion or inadvertently when flushing the catheter. Negative intrathoracic pressure from inspiration can draw air into the vein while cannulized, and hypoxia can result from larger air emboli that reach the pulmonary arterial system. Patients with atrial or ventricular septal defects can transmit air emboli into the systemic circulation with potentially fatal complications. In order to avoid air embolism, the patient should be placed in the Trendelenburg position at all times during insertion to increase venous pressure. Additionally, all catheter hubs should be occluded at all times. If an air embolism is suspected, the patient should be placed on high flow oxygen and in the left lateral decubitus position. The left lateral decubitus position localizes air to the right atrium and right lung and prevents further air emboli from entering the pulmonary artery. This maneuver is not effective in patients with abnormal anatomy, such as patients with previous pneumonectomy or patent foramen ovale, and may worsen complications.[1,5] Small air embolisms, such as less than several cc's, are typically of little significant and should not distract from safely securing the line. Even with intracardiac shunts, small cerebral air embolisms can be self-resolving and can be managed with supplemental oxygen and increased systemic pressures to help “washout” the air bubble.[42] In extreme cases, hyperbaric oxygen therapy, if easily available, can be attempted to help reabsorb the air.[43]
CARDIAC COMPLICATIONS
Cardiac complications during catheter placement include arrhythmia and cardiac arrest. Arrhythmia results from guide wire contact with the right atrium. Most frequently, this results in premature atrial and ventricular contractions. However, if the AV node is contacted for a significant amount of time, supraventricular tachycardia can result and lead to fatal arrhythmia and arrest.[3,5,44] Awareness of guide wire depth and telemetry monitoring help in early recognition of arrhythmia. If arrhythmia does occur, prompt initiation of advanced cardiac life support (ACLS) is necessary. Although rare, deaths from cardiac arrest related to central venous catheter placement have been reported.[44] Probably underreported in the literature, direct valvular (particularly tricuspid) injuries would rarely require intervention as even severe tricuspid regurgitation can be managed medically. Likewise, right ventricular perforations with pulmonary artery catheters can occur and result in life-threatening tamponade. When suspected, emergent surface echocardiography may confirm the diagnosis and prompt immediate sternotomy for direct repair. Such injuries are rarely diagnosed preoperatively as immediate hemodynamic collapse from presumed hemorrhage may prompt emergent surgical exploration. Lifesaving cardiothoracic surgical intervention often requires a high index of suspicion as delaying surgery while awaiting diagnostic studies may be fatal.
DELAYED COMPLICATIONS
Delayed complications include device dysfunction and infection. These complications are more gradual in onset and can occur in the weeks to years after central venous catheter placement. Early recognition is important in reducing morbidity and mortality associated with these complications. As with any infection, appropriate culture-guided antibiotic therapy and prompt catheter removal, if possible, is indicated.
DEVICE DYSFUNCTION
Device dysfunction complications include fibrin sheath formation, fracture, thrombosis, central venous stenosis, and infection. Site of catheter placement, duration of catheterization, and underlying patient comorbidities all affect the rate of device dysfunction.
Fibrin sheath formation can occur within 1 week of catheter placement and can occlude the distal openings resulting in inability to withdraw blood. Fibrinolytics such as alteplase can be employed in order to dissolve the fibrin sheath.[5] Line stripping can be attempted in patients where fibrinolytics have failed.[19] Fibrin sheath formation does not correlate with future catheter thrombosis.[3] Unless there is a large thrombus associated with the sheath (>3 cm), simple line removal is appropriate. If there is a large thrombus at the end of the catheter, especially if there is concern that it is infected, direct surgical removal should be considered after attempted anticoagulation or thrombolytic therapy. In septic patients, intracardiac removal of infected lines may play an important role in infection source control and should be considered in appropriate patients.
Catheter fracture occurs most commonly in subclavian lines after a catheter has been in place for an extended period of time [Figures 5 and 6]. Fracture can lead to serious complications related to catheter embolization including sepsis, endocarditis, cardiac perforation, or arrhythmia.[19] Catheter fracture is preceded by pinch-off syndrome, which results in catheter malfunction from compression of the catheter by the subclavius-costoclavicular complex between the clavicle and first rib.[3] Catheter fracture can also occur during removal secondary to catheter entrapment. Catheter entrapment can occur due to the ingrowth of endothelium around the catheter and results in fracture upon attempted removal.
Figure 5.

Fractured catheters following chronic port removal. An elderly lady who underwent combined chemo and radiation therapy for breast cancer presented for elective removal of her chronic intravascular port (top image). Upon attempted removal of the port in the operating room, the distal half fractured (bottom image). As it appeared to be immobile and potentially adherent to the vascular wall, the initial recommendation was to follow it closely for signs of migration with serial chest X-rays. Patient concern for embolization prompted attempted extraction by interventional catheter-directed techniques by interventional radiology. Such attempts were unsuccessful as the catheter appeared, as suspected, to be adherent to the innominate vein. Due to patient frailty and concerns for causing a major injury, further attempts at removal were abandoned. The patient remains asymptomatic
Figure 6.

Chronic catheter fracture. Catheter fragment incidentally found on chest X-ray 4 years following chronic port removal. The patient was asymptomatic and opted for no intervention
Long-term catheters can also lead to venous thrombosis. Symptoms include ipsilateral extremity erythema, edema, and paresthesia. Additionally, thrombosis can lead to superior vena cava syndrome, which can present as head and neck swelling.[5] Incidence of superior vena cava syndrome is estimated to be 1 in 1,000 cases.[3] Subclavian central venous catheters have the lowest rate of thrombosis.[1,3] Femoral lines have the highest rate of thrombosis.[3] Cancer patients have a higher risk of central line thrombosis of up to 41%.[3] Primary thromboprophylaxis has no proven benefit in the oncologic or cancer-free population.[3]
Chronic central venous access can also lead to venous stenosis. Stenosis is often asymptomatic and has been reported to occur in up to 41% of cases.[19] Stenting may be required to treat symptomatic stenoses or occlusion.[19] Risk factors for stenosis include previous cannulation, infection, and increased in-dwelling catheter time.[3]
INFECTION
Infection is a serious delayed complication associated with central venous access that can lead to sepsis, shock, and death. Central line-associated bloodstream infections have a reported incidence between 80–189 episodes per 100,000 patient years, and the Centers for Disease Control and Prevention (CDC) estimates the additional cost per infection to be on average approximately $16,550.[45] Mortality related to central line infection can occur in up to 25% of cases.[29] Infections become established on the catheter through the production of biofilm. Staphylococcus aureus and Staphylococcus epidermidis are the two most common pathogens.[46]
Catheter infection sources include contamination from skin flora, contamination from infused substance, or from hematogenous spread from an unrelated site.[46] Femoral catheters have the highest rate of infection, and non-cuffed catheters have higher risk than cuffed catheters.[3] Catheters with greater number of lumens have been associated with a greater risk of infection.[47,48,49] Antimicrobial impregnated catheters can also aid in decreasing central line infection rates.[3]
If infection is suspected, two blood cultures should be drawn from separate sites before starting broad-spectrum antibiotics. The catheter tip should also be sent for culture. The type of catheter, virulence of pathogen, severity of illness, and the availability of additional venous access should be considered when evaluating central line infection. Antibiotics should be tailored to specific pathogens as cultures return.[50]
Guidelines for reducing infection address several key areas.[2] In order to prevent infection, it is recommended that upper extremity sites be used for catheter insertion and that any lower extremity site be changed as soon as possible. This recommendation is especially important if catheters were placed in emergent (and potentially less than sterile) situations such as during a cardiopulmonary arrest. A midline or peripherally inserted central venous catheter should be used if intravenous (IV) therapy is to exceed 6 days. Catheter sites should be inspected daily, and opaque dressings should not be removed unless necessary. Catheters should have the minimum number of ports necessary for the care of the patient, and any central line no longer needed should be removed. Maximal sterile barrier precautions should be used, an aseptic should be used to clean the skin, and transparent dressings should be changed every 7 days. Central line bundles incorporating these guidelines have been shown to significantly reduce the incidence of central line infection.[51,52]
PICC COMPLICATIONS
First described in 1975 by Hoshal, the PICC has become a popular method of central venous access.[53] Increased use of PICCs is multifactorial with one of the factors being a perception of an improved side effect profile. Immediate risks of peripherally inserted catheters include injury to local structures, phlebitis at insertion site, air embolism, hematoma, arrhythmia, and catheter malposition. Late complications include infection, thrombosis, and catheter malposition.
Early studies demonstrated that PICCs may have a decreased rate of bloodstream infection, but more recent studies have indicated that there may be no difference in the rate of bloodstream infection between traditional central venous catheters and PICCs.[54,55,56,57] Thrombosis of PICCs has been reported in the literature to be up to 5%.[58] Additional studies have suggested that the risk of thrombophlebitis is greater in PICCs.[57] However, there is lack of large randomized control trials comparing PICCs to central venous catheters.
As with centrally placed catheters, rare complications with PICCs have also been reported. Catheter fracture and embolization can occur and necessitate surgical intervention.[59,60] Life-threatening cardiovascular complications including cardiac perforation and tamponade, atrial arrhythmia, catheter-related right atrial thrombi, and pulmonary embolism have also been described.[61,62,63] PICC insertion can also lead to vascular complications such as AV fistula and venous injury. Cases of neurologic complications such as Horner's syndrome and injury to the interosseus nerve have been reported as well.[64,65] Pulmonary complications that have been described include hydromediastinum and pneumothorax.[66] These case reports demonstrate that PICCs can cause many of the same serious and life-threatening complications associated with traditional central venous catheters and should be considered when considering catheter type.
While perception remains that peripherally inserted catheters are less morbid than traditional catheters, recent data suggests that the complication profile may not be that altered. Physicians should be cautious and be aware of the risks that PICCs carry when deciding upon central venous access. The widely held perception that such catheters, because of peripheral placement, are associated with minimal risks is probably inappropriate.
FUTURE DIRECTIONS
Without a doubt as patients present with more comorbidities, as therapies become more aggressive and invasive, and the consequences of complications—both to the patient and potentially to the hospital and healthcare systems—become more significant (and potentially costly).[67] As such, the means in which therapies are delivered will come under greater scrutiny in terms of safety, efficacy, and costs. As mentioned, procedural related complications, more and more, are being considered as “never events” (implying they should never occur) with not only potential clinical and medical-legal implications, but reimbursement as well.[68] Payers, such as Medicare and Medicaid, are establishing reporting requirements and protocols that will no longer reimburse for costs incurred as a result of procedural-related complications. As such, greater emphasis is being placed on the development and adherence to protocols that emphasize proper technique, checklists to minimize complications, and technologies that improve patient safety. Previously routinely placed procedures performed by Junior residents; such as beside temporary dialysis catheters (which might not be billed nor charged for) are now routine procedures in Interventional Radiology suites, hybrid operating rooms, and/or specially designed and designated “procedure rooms”. The implications, in terms of costs and safety, not to mention patient convenience are poorly understood.[69] Nevertheless, as complications such as catheter line-associated blood stream infections (CLABSI), are now publically reported in the Institutional Quality Data, much emphasis will be placed improving this metric of safety. Clearly, tremendous resources and opportunities exist for the development of technologies and guidelines that minimize such risks.
PRACTICAL CONSIDERATIONS
Without a doubt, central venous access is one of the more commonly performed invasive vascular procedures in hospitalized patients. With increasing comorbidities and complexity of illness in hospitalized patients, the need for central IV access for medication administration, multiple lab testing, and central hemodynamic monitoring the risks of placement and spectrum of complications will only increase as well. While most of the complications outlined above are well-described, potentially preventable, and within the spectrum of acceptable procedural related risks, clearly unusual complications have been reported in isolated reports; all illustrating that the clinician must be aware that anything that can happen, will happen, and that awareness and a management plan are critical to the use of such lines. Complications from localized hematomas can cause vocal cord paralysis,[70] airway obstruction,[71] and phrenic nerve injuries.[72] Other rare, but reported complications, such as intracranial hypertension from AV malformation from inadvertent arterial puncture[73] and brain stem strokes from vertebral artery thrombosis[74] (again, from inadvertent arterial puncture); all illustrate that when unusual and rare problems develop shortly after central line placement, a procedural-related complication must be considered and a multidisciplinary team may be required for appropriate management.
CONCLUSION
While central venous access is routine in the critically-ill patient, it is not without risk. Physicians should be aware of the immediate and delayed complications related to central venous catheter placement. Recognizing and subsequent management of complications reduces morbidity and mortality and improves patient outcomes. Each type of access carries an altered likelihood of complication that physicians should consider. While the chance of complications can never be completely eliminated, their prevention should be a provider's ultimate goal.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348:1123–33. doi: 10.1056/NEJMra011883. [DOI] [PubMed] [Google Scholar]
- 2.O’Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, et al. Healthcare Infection Control Practices Advisory Committee (HICPAC) (Appendix 1). Summary of recommendations: Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52:1087–99. doi: 10.1093/cid/cir138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kusminsky RE. Complications of central venous catheterization. J Am Coll Surg. 2007;204:681–96. doi: 10.1016/j.jamcollsurg.2007.01.039. [DOI] [PubMed] [Google Scholar]
- 4.Sznajder JI, Zveibil FR, Bitterman H, Weiner P, Bursztein S. Central vein catheterization. Failure and complication rates by three percutaneous approaches. Arch Intern Med. 1986;146:259–61. doi: 10.1001/archinte.146.2.259. [DOI] [PubMed] [Google Scholar]
- 5.Bhutta ST, Culp WC. Evaluation and management of central venous access complications. Tech Vasc Interv Radiol. 2011;14:217–24. doi: 10.1053/j.tvir.2011.05.003. [DOI] [PubMed] [Google Scholar]
- 6.Powell JT, Mink JT, Nomura JT, Levine BJ, Jasani N, Nichols WL, et al. Ultrasound-guidance can reduce adverse events during femoral central venous cannulation. J Emerg Med. 2014;46:519–24. doi: 10.1016/j.jemermed.2013.08.023. [DOI] [PubMed] [Google Scholar]
- 7.Leung J, Duffy M, Finckh A. Real-time ultrasonographically-guided internal jugular vein catheterization in the emergency department increases success rates and reduces complications: A randomized, prospective study. Ann Emerg Med. 2006;48:540–7. doi: 10.1016/j.annemergmed.2006.01.011. [DOI] [PubMed] [Google Scholar]
- 8.Fragou M, Gravvanis A, Dimitriou V, Papalois A, Kouraklis G, Karabinis A, et al. Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: A prospective randomized study. Crit Care Med. 2011;39:1607–12. doi: 10.1097/CCM.0b013e318218a1ae. [DOI] [PubMed] [Google Scholar]
- 9.Bowdle A. Vascular complications of central venous catheter placement: Evidence-based methods for prevention and treatment. J Cardiothorac Vasc Anesth. 2014;28:358–68. doi: 10.1053/j.jvca.2013.02.027. [DOI] [PubMed] [Google Scholar]
- 10.Vats HS. Complications of catheters: Tunneled and nontunneled. Adv Chronic Kidney Dis. 2012;19:188–94. doi: 10.1053/j.ackd.2012.04.004. [DOI] [PubMed] [Google Scholar]
- 11.Troianos CA, Jobes DR, Ellison N. Ultrasound-guided cannulation of the internal jugular vein. A prospective, randomized study. Anesth Analg. 1991;72:823–6. doi: 10.1213/00000539-199106000-00020. [DOI] [PubMed] [Google Scholar]
- 12.Randolph AG, Cook DJ, Gonzales CA, Pribble CG. Ultrasound guidance for placement of central venous catheters: A meta-analysis of the literature. Crit Care Med. 1996;24:2053–8. doi: 10.1097/00003246-199612000-00020. [DOI] [PubMed] [Google Scholar]
- 13.Hind D, Calvert N, McWilliams R, Davidson A, Paisley S, Beverley C, et al. Ultrasonic locating devices for central venous cannulation: Meta analysis. BMJ. 2003;327:361. doi: 10.1136/bmj.327.7411.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pillai L, Zimmerman P, d’Audiffret A. Inadvertent great vessel arterial catheterization during ultrasound-guided central venous line placement: A potentially fatal event. J Vasc Surg. 2009;53:74. [Google Scholar]
- 15.Parsons AJ, Alfa J. Carotid dissection: A complication of internal jugular vein cannulation with the use of ultrasound. Anesth Analg. 2009;109:135–6. doi: 10.1213/ane.0b013e3181a7f5a4. [DOI] [PubMed] [Google Scholar]
- 16.Thompson C, Barrows T. Carotid arterial cannulation: Removing the risk with ultrasound? Can J Anaesth. 2009;56:471–2. doi: 10.1007/s12630-009-9082-1. [DOI] [PubMed] [Google Scholar]
- 17.Guilbert MC, Elkouri S, Bracco D, Corriveau MM, Beaudoin N, Dubois MJ, et al. Arterial trauma during central venous catheter insertion: Case series, review and proposed algorithm. J Vasc Surg. 2008;48:918–25. doi: 10.1016/j.jvs.2008.04.046. [DOI] [PubMed] [Google Scholar]
- 18.Shah PM, Babu SC, Goyal A, Mateo RB, Madden RE. Arterial misplacement of large-caliber cannulas during jugular vein catheterization: Case for surgical management. J Am Coll Surg. 2004;198:939–44. doi: 10.1016/j.jamcollsurg.2004.02.015. [DOI] [PubMed] [Google Scholar]
- 19.Khouzam RN, Soufi MK, Weatherly M. Heparin Infusion through through a central line misplaced in the carotid artery leading to hemorrhagic stroke. J Emerg Med. 2013;45:e87–9. doi: 10.1016/j.jemermed.2012.12.026. [DOI] [PubMed] [Google Scholar]
- 20.Wang RC, Katz SE, Lubow M. Visual loss and central venous catheterization: Cortical blindness and hemianopsia after inadvertent subclavian artery entry. J Neuroophthalmol. 2000;20:32–4. doi: 10.1097/00041327-200020010-00011. [DOI] [PubMed] [Google Scholar]
- 21.Shah PM, Leong B, Babu SC, Goyal AM, Mateo RB. Cerebrovascular events associated with infusion through arterially malpositioned triple-lumen catheter: Report of three cases and review of literature. Cardiol Rev. 2005;13:304–8. doi: 10.1097/01.crd.0000160307.89405.30. [DOI] [PubMed] [Google Scholar]
- 22.Nayeemuddin M, Pherwani AD, Asquith JR. Imaging and management of complications of central venous catheters. Clin Radiol. 2013;68:529–44. doi: 10.1016/j.crad.2012.10.013. [DOI] [PubMed] [Google Scholar]
- 23.Ratliff HL, Yousufuddin M, Lieving WR, Watson BE, Malas A, Rosencrance G, et al. Persistent left superior vena cava: Case reports and clinical implications. Int J Cardiol. 2006;113:242–6. doi: 10.1016/j.ijcard.2005.08.067. [DOI] [PubMed] [Google Scholar]
- 24.Higgs AG, Paris S, Potter F. Discovery of left-sided superior vena cava during central venous catheterization. Br J Anaesth. 1998;81:260–1. doi: 10.1093/bja/81.2.260. [DOI] [PubMed] [Google Scholar]
- 25.Leibowitz AB, Halpern NA, Lee MH, Iberti TJ. Left-sided superior vena cava: A not-so-unusual vascular anomaly discovered during central venous and pulmonary artery catheterization. Crit Care Med. 1992;20:1119–22. [PubMed] [Google Scholar]
- 26.Sweitzer BJ, Hoffman WJ, Allyn JW, Daggett WJ., Jr Diagnosis of a left-sided superior vena cava during placement of a pulmonary artery catheter. J Clin Anesth. 1993;5:500–4. doi: 10.1016/0952-8180(93)90070-u. [DOI] [PubMed] [Google Scholar]
- 27.Schelling G, Briegel J, Eichinger K, Raum W, Forst H. Pulmonary artery catheter placement and temporary cardiac pacing in a patient with a persistent left superior vena cava. Intensive Care Med. 1991;17:507–8. doi: 10.1007/BF01690781. [DOI] [PubMed] [Google Scholar]
- 28.Duong MH, Jensen WA, Kirsch CM, Wehner JH, Kagawa FT. An unusual complication during central venous catheter placement. J Clin Anesth. 2001;13:131–2. doi: 10.1016/s0952-8180(01)00229-x. [DOI] [PubMed] [Google Scholar]
- 29.Andrews RT, Geschwind JF, Savader SJ, Venbrux AC. Entrapment of J-tip guidewires by Venatech and stainless-steel Greenfield vena cava filters during central venous catheter placement: Percutaneous management in four patients. Cardiovasc Intervent Radiol. 1998;21:424–8. doi: 10.1007/s002709900292. [DOI] [PubMed] [Google Scholar]
- 30.Graff J, Gong R, Byron R, Hassett JM. Knotting and entanglement of multiple central venous catheters. JPEN J Parenter Enteral Nutr. 1986;10:319–21. doi: 10.1177/0148607186010003319. [DOI] [PubMed] [Google Scholar]
- 31.Bossert T, Gummert JF, Bittner HB, Barten M, Walther T, Falk V, et al. Swan-Ganz catheter-induced severe complications in cardiac surgery: Right ventricular perforation, knotting, and rupture of a pulmonary artery. J Card Surg. 2006;21:292–5. doi: 10.1111/j.1540-8191.2006.00235.x. [DOI] [PubMed] [Google Scholar]
- 32.Hida S, Ohashi S, Kinoshita H, Honda T, Yamamoto S, Kazama J, et al. Knotting of two central venous catheters: A rare complication of pulmonary artery catheterization. J Anesth. 2010;24:486–7. doi: 10.1007/s00540-010-0885-6. [DOI] [PubMed] [Google Scholar]
- 33.Yoho DJ, Firstenberg MS. The sequelae of silence: Catheter entrapment as a preventable morbidity resulting from communication failure. Heart Res Open J. 2015;2:82–4. [Google Scholar]
- 34.Wang HE, Sweeney TA. Subclavian central venous catheterization complicated by guidewire looping and entrapment. J Emerg Med. 1999;17:721–4. doi: 10.1016/s0736-4679(99)00067-0. [DOI] [PubMed] [Google Scholar]
- 35.Song Y, Messerlian AK, Matevosian R. A potentially hazardous complication during central venous catheterization: Lost guidewire retained in the patient. J Clin Anesth. 2012;24:221–6. doi: 10.1016/j.jclinane.2011.07.003. [DOI] [PubMed] [Google Scholar]
- 36.Jalwal GK, Rajagopalan V, Bindra A, Goyal K, Rath GP, Kumar A, et al. Percutaneous retrieval of malpositioned, kinked and unraveled guide wire under fluoroscopic guidance during central venous cannulation. J Anaesthesiol Clin Pharmacol. 2014;30:582. doi: 10.4103/0970-9185.142885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Vannucci A, Jeffcoat A, Ifune C, Salinas C, Duncan JR, Wall M. Special article: Retained guidewires after intraoperative placement of central venous catheters. Anesth Analg. 2013;117:102–8. doi: 10.1213/ANE.0b013e3182599179. [DOI] [PubMed] [Google Scholar]
- 38.Teichgraber UK, Nibbe L, Gebauer B, Wagner HJ. Inadvertent puncture of the thoracic duct during attempted central venous catheter placement. Cardiovasc Intervent Radiol. 2003;26:569–71. doi: 10.1007/s00270-003-0102-1. [DOI] [PubMed] [Google Scholar]
- 39.Konichezky S, Saguib S, Soroker D. Tracheal puncture. A complication of percutaneous internal jugular vein cannulation. Anaesthesia. 1983;38:572–4. doi: 10.1111/j.1365-2044.1983.tb12117.x. [DOI] [PubMed] [Google Scholar]
- 40.Malik IA, Adams RG. Tracheal cuff puncture: A complication of percutaneous internal jugular vein cannulation. Am J Med. 2003;115:590–1. doi: 10.1016/s0002-9343(03)00443-1. [DOI] [PubMed] [Google Scholar]
- 41.Lampl L. Tracheobronchial injuries. Conservative treatment. Interact Cardiovasc Thorac Surg. 2004;3:401–5. doi: 10.1016/j.icvts.2004.02.016. [DOI] [PubMed] [Google Scholar]
- 42.Hsu M, Trerotola SO. Air embolism during insertion and replacement of tunneled dialysis catheters: A retrospective investigation of the effect of aerostatic sheaths and over-the-wire exchange. J Vasc Interv Radiol. 2015;26:366–71. doi: 10.1016/j.jvir.2014.11.035. [DOI] [PubMed] [Google Scholar]
- 43.Huang YC, Huang JC, Chen SC, Chang JM, Chen HC. Lethal cardiac arrhythmia during central venous catheterization in a uremic patient: A case report and review of the literature. Hemodial Int. 2013;17:644–8. doi: 10.1111/hdi.12030. [DOI] [PubMed] [Google Scholar]
- 44.Centers for Disease Control and Prevention (CDC). Vital signs: Central line-associated blood stream infections--United States, 2001, 2008, and 2009. MMWR Morb Mortal Wkly Rep. 2011;60:243–8. [PubMed] [Google Scholar]
- 45.To KB, Napolitano LM. Common complications in the critically ill patient. Surg Clin North Am. 2012;92:1519–57. doi: 10.1016/j.suc.2012.08.018. [DOI] [PubMed] [Google Scholar]
- 46.Early TF, Gregory RT, Wheeler JR, Snyder SO, Jr, Gayle RG. Increased infection rate in double-lumen versus single-lumen Hickman catheters in cancer patients. South Med J. 1990;83:34–6. doi: 10.1097/00007611-199001000-00010. [DOI] [PubMed] [Google Scholar]
- 47.Hilton E, Haslett TM, Borenstein MT, Tucci V, Isenberg HD, Singer C. Central catheter infections: Single- versus triple-lumen catheters. Influence of guide wires on infection rates when used for replacement of catheters. Am J Med. 1988;84:667–72. doi: 10.1016/0002-9343(88)90102-7. [DOI] [PubMed] [Google Scholar]
- 48.Yeung C, May J, Hughes R. Infection rate for single lumen v triple lumen subclavian catheters. Infect Control Hosp Epidemiol. 1988;9:154–8. doi: 10.1086/645820. [DOI] [PubMed] [Google Scholar]
- 49.Watson CM, Al-Hasan MN. Bloodstream infections and central line-associated bloodstream infections. Surg Clin North Am. 2014;94:1233–44. doi: 10.1016/j.suc.2014.08.003. [DOI] [PubMed] [Google Scholar]
- 50.Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355:2725–32. doi: 10.1056/NEJMoa061115. [DOI] [PubMed] [Google Scholar]
- 51.Marsteller JA, Sexton JB, Hsu YJ, Hsiao CJ, Holzmueller CG, Pronovost PJ, et al. A multicenter, phased, cluster-randomized controlled trial to reduce central line-associated bloodstream infections in intensive care units*. Crit Care Med. 2012;40:2933–9. doi: 10.1097/CCM.0b013e31825fd4d8. [DOI] [PubMed] [Google Scholar]
- 52.Hoshal VL., Jr Total intravenous nutrition with peripherally inserted silicone elastomer central venous catheters. Arch Surg. 1975;110:644–6. doi: 10.1001/archsurg.1975.01360110190032. [DOI] [PubMed] [Google Scholar]
- 53.Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489–95. doi: 10.1378/chest.128.2.489. [DOI] [PubMed] [Google Scholar]
- 54.Shuman EK, Washer LL, Arndt JL, Zalewski CA, Hyzy RC, Napolitano LM, et al. Analysis of central line-associated bloodstream infections in the intensive care unit after implementation of central line bundles. Infect Control Hosp Epidemiol. 2010;31:551–3. doi: 10.1086/652157. [DOI] [PubMed] [Google Scholar]
- 55.Al Raiy B, Fakih MG, Bryan-Nomides N, Hopfner D, Riegel E, Nenninger T, et al. Peripherally inserted central venous catheters in the acute care setting: A safe alternative to high-risk short-term central venous catheters. Am J Infect Control. 2010;38:149–53. doi: 10.1016/j.ajic.2009.06.008. [DOI] [PubMed] [Google Scholar]
- 56.Pikwer A, Akeson J, Lindgren S. Complications associated with peripheral or central routes for central venous cannulation. Anaesthesia. 2012;67:65–71. doi: 10.1111/j.1365-2044.2011.06911.x. [DOI] [PubMed] [Google Scholar]
- 57.Chopra V, Anand S, Krein SL, Chenoweth C, Saint S. Bloodstream infection, venous thrombosis, and peripherally inserted central catheters: Reappraising the evidence. Am J Med. 2012;125:733–41. doi: 10.1016/j.amjmed.2012.04.010. [DOI] [PubMed] [Google Scholar]
- 58.Chow LM, Friedman JN, MacArthur C, Restrepo R, Temple M, Chait PG, et al. Peripherally inserted central catheter (PICC) fracture and embolozation in the pediatric population. J Pediatr. 2003;142:141–4. doi: 10.1067/mpd.2003.67. [DOI] [PubMed] [Google Scholar]
- 59.Ioachimescu OC, Stoller JK. An ectopic peripherally inserted central catheter (’ectoPICC’) Cleve Clin J Med. 2006;73:617–8. doi: 10.3949/ccjm.73.7.617. [DOI] [PubMed] [Google Scholar]
- 60.Orme RM, McSwiney MM, Chamberlain-Webber RF. Fatal cardiac tamponade as a result of a peripherally inserted central venous catheter: A case report and review of the literature. Br J Anaesth. 2007;99:384–8. doi: 10.1093/bja/aem181. [DOI] [PubMed] [Google Scholar]
- 61.Burns KE, McLaren A. Catheter-related right atrial thrombus and pulmonary embolism: A case report and systematic review of the literature. Can Respir J. 2009;16:163–5. doi: 10.1155/2009/751507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Elsharkawy H, Lewis BS, Steiger E, Farag E. Post placement positional atrial fibrillation and peripherally inserted central catheters. Minerva Anestesiol. 2009;75:471–4. [PubMed] [Google Scholar]
- 63.Links DJ, Crowe PJ. Horner's syndrome after placement of a peripherally inserted central catheter. JPEN Parenter Enteral Nutr. 2006;30:451–2. doi: 10.1177/0148607106030005451. [DOI] [PubMed] [Google Scholar]
- 64.Puhaindran ME, Wong HP. A case of anterior interosseous nerve syndrome after peripherally inserted central catheter (PICC) line insertion. Singapore Med J. 2003;44:653–5. [PubMed] [Google Scholar]
- 65.Maruyama K, Koizumi T. Hydromediastinum associated with a peripherally inserted central venous catheter in a newborn infant. J Clin Ultrasound. 2006;34:195–8. doi: 10.1002/jcu.20194. [DOI] [PubMed] [Google Scholar]
- 66.David G, Gunnarsson CL, Waters HC, Horblyuk R, Kaplan HS. Economic measurement of medical errors using a hospital claims database. Value Health. 2013;16:305–10. doi: 10.1016/j.jval.2012.11.010. [DOI] [PubMed] [Google Scholar]
- 67.Rosenthal MB. Nonpayment for performance? Medicare's new reimbursement rule. N Engl J Med. 2007;357:1573–5. doi: 10.1056/NEJMp078184. [DOI] [PubMed] [Google Scholar]
- 68.Waters TM, Daniels MJ, Bazzoli GJ, Perencevich E, Dunton N, Staggs VS, et al. Effect of Medicare's nonpayment for Hospital-Acquired Conditions: Lessons for future policy. JAMA Intern Med. 2015;175:347–54. doi: 10.1001/jamainternmed.2014.5486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Martin-Hirsch DP, Newbegin CJ. Right vocal fold paralysis as a result of central venous catheterization. J Laryngol Otol. 1995;109:1107–8. doi: 10.1017/s0022215100132153. [DOI] [PubMed] [Google Scholar]
- 70.Silva FS. Neck haematoma and airway obstruction in a patient with goitre: Complication of internal jugular vein cannulation. Acta Anaesthesiol Scand. 2003;47:626–9. doi: 10.1034/j.1399-6576.2003.00106.x. [DOI] [PubMed] [Google Scholar]
- 71.Drachler DH, Koepke GH, Weg JG. Phrenic nerve injury from subclavian vein catheterization. Diagnosis by electromyography. JAMA. 1976;236:2880–1. [PubMed] [Google Scholar]
- 72.Lal SM, Twardowski ZJ, Van Stone J, Keniston D, Scott WJ, Berg GG, et al. Benign intracranial hypertension: A complication of subclavian vein catheterization and arteriovenous fistula. Am J Kidney Dis. 1986;8:262–4. doi: 10.1016/s0272-6386(86)80037-3. [DOI] [PubMed] [Google Scholar]
- 73.Sloan MA, Mueller JD, Adelman LS, Caplan LR. Fatal brainstem stroke following internal jugular vein catheterization. Neurology. 1991;41:1092–2. doi: 10.1212/wnl.41.7.1092. [DOI] [PubMed] [Google Scholar]
- 74.Tek le WG, Adkinson CD, Chaudhry SA, Jadhav V, Hassan AE, Rodriguez GJ, et al. Factors associated with favorable response to hyperbaric oxygen therapy among patients presenting with iatrogenic cerebral arterial gas embolism. Neurocrit Care. 2013;18:228–33. doi: 10.1007/s12028-012-9683-3. [DOI] [PubMed] [Google Scholar]