

Abstract
Purpose
We conducted a nationwide study to assess the incidence and treatment patterns of extremity soft tissue sarcoma (STS) in South Korea.
Materials and Methods
The nationwide incidence and treatment patterns of extremity STS were assessed using two nationwide databases, the Korea National Cancer Incidence (KNCI) database and the Health Insurance Review and Assessment Service (HIRA) database.
Results
A total of 1,236 patients were newly diagnosed with extremity STS during the 3-year study period, from 2009 to 2011. The annual incidence of extremity STS in the Korean population was approximately 0.9 per 100,000 people with a male bias that increased with age and was especially pronounced amongst individuals aged > 80 years. Approximately 7% of patients did not receive any treatment, and surgical excision was performed for 85% of those who were treated.
Conclusion
This is the first nationwide study of the incidence and treatment patterns of extremity STS in Korea using two national databases (KNCI and HIRA), which include the entire Korean population. The results of this study may be useful for future planning and management of STS, at the national level.
Keywords: Sarcoma, Incidence, Registries, Korea, Therapy
Introduction
Soft tissue sarcoma (STS) is a heterogeneous group of malignant tumors of mesodermal origin that constitute < 1% of all malignant tumors [1]. STS is deadly, which accounts for more deaths than testicular cancer, Hodgkin’s disease, and thyroid cancer combined [2,3]. A better understanding of the incidence and treatment patterns of STS is necessary to assess the impact of STS on public health. Due to its rarity, even specialized sarcoma centers only see a relatively small number of patients with STS. Thus, a large population-based study would be helpful to assess its incidence and treatment pattern.
A few population-based studies on STS have been published, reporting the incidences <to be> between 1.8 and 5.0 cases per 100,000 people per year [4-9]. However, these studies were based on Western populations and focused on the incidence of STS. Moreover, these studies typically included STS of all anatomical sites, whereas the treatment and prognoses of STS differ according to the anatomical location (e.g., head and neck, viscera, retroperitoneum, and extremity) [10]. Thus, a large population-based study on the incidence and treatment patterns of extremity STS in Korea is needed.
South Korea operates two mandatory nationwide databases for medical records that cover <almost> the entire population. These are the Korea National Cancer Incidence (KNCI) database from the Korean Central Cancer Registry (KCCR) and the Korean Health Insurance Review and Assessment Service (HIRA) database from HIRA. The KNCI database has covered the whole population under the Population-based Regional Cancer Registry Program since 1999, and it has high diagnostic accuracy but lacks treatment information [11]. Conversely, the HIRA database includes the health insurance claim records under the Korean National Health Insurance Program, and thus provides detailed information on patient treatment, but has less diagnostic accuracy [12,13].
In this study, we combined and utilized the KNCI and HIRA databases to estimate the nationwide incidence and treatment pattern of extremity STS in the Korean population.
Materials and Methods
1. Data sources
KCCR, initiated as a nationwide hospital-based cancer registry by the Ministry of Health and Welfare in 1980, was expanded in 1999 to cover the entire population under the Population-based Regional Cancer Registry Program. Since 2002, KCCR has constructed KNCI, a nationwide cancer registry database, and presented the annual incidence of cancer based on the whole Korean population [11]. Cancer cases were classified in accordance to the International Classification of Disease for Oncology (ICD-O) third edition [14,15], and subsequently re-classified according to the 10th revised version of the International Classification of Disease (ICD-10) [16].
The Korean National Health Insurance Program covers the entire Korean population (97% of the population have health insurance, and 3% are covered by medical aid). HIRA, operated under the Korean National Health Insurance Program, contains the adjusted medical and pharmacy claims for all Koreans [12,13], and its database has been used for many epidemiological studies [17]. All clinics and hospitals submit claims data for inpatient and outpatient care, including diagnoses, procedures, prescription records, demographic information, and direct medical costs, to HIRA to obtain reimbursement of medical costs from the government. The HIRA database was established based on the sixth edition of the Korean Classification of Disease (KCD-6), which is a modified version of the ICD-10 for the Korean health care system.
For patients with serious diseases or cancer, the Korean government covers most of their medical costs [12]. If patients are confirmed to have a malignant disease, they are registered by KCCR and paid only 5% of their total medical costs. The remaining 95% of costs are paid by the National Health Insurance Corporation, and the associated review data are saved in the HIRA database. Thus, virtually all patients with malignant disease are registered by both KCCR and HIRA.
All Korean residents receive a unique identification number (Korean Resident Registration Number, KRRN) at birth, allowing easy identification of every citizen. This is widely used in government-operated databases, including the KNCI and HIRA databases. These databases can therefore be used to obtain the health care records and demographic characteristics of specific patients without any duplications or omissions. Public access to both databases is not allowed; however, access can be granted with permission from the Deliberative Committee if they believe that the requested study will ultimately be for the greater good. After receiving approval for the study from the Deliberative Committee of HIRA and permission to access the requested data from KCCR, the de-identified individual information from the HIRA database were accessed and the total annual incident cases of extremity STS from the KNCI database were obtained. The access to the data was allowed on September 2013 and February 2014 from HIRA and KCCR, respectively. The HIRA provided the data after it had been de-identified. Each de-identified individual’s (1) diagnostic code and claim date, and referral level of the hospital where the first confirmed diagnosis of STS was registered and regional distribution of those hospitals; and (2) the procedure code and its claim date. Although each database uses KRRN for data processing, the authors are prohibited to access the identified information. Therefore, informed consent from each patient was not acquired, and the study was exempted by the Seoul National University Hospital Institutional Review Board (IRB No. 1311-054-533) because the authors could access only de-identified data.
2. Study population
To identify patients with newly diagnosed extremity STS from the KNCI database, the following ICD-10 diagnostic codes were searched: “malignant neoplasm of the peripheral nerves and autonomic nervous system” (ICD-10 diagnostic code: C47.1 for upper extremity and C47.2 for lower extremity) or “malignant neoplasm of other connective and soft tissues” (C49.1 for upper extremity and C49.2 for lower extremity). As a result, Kaposi sarcoma and malignant neoplasms of the skin, such as malignant melanoma, were excluded from this study [7]. The most recent data available are for 2011, and thus, we obtained data for cases between 2009 and 2011 from the KNCI database.
To identify patients who were newly diagnosed and treated for extremity STS from the HIRA database, with the following ICD-10 diagnostic codes were searched: C47.1, C47.2, C49.1, and C49.2. Because HIRA only provides data from the previous 5 years―for example if the data were requested in 2013, HIRA would provide data for 2008-2012― we assessed patients with extremity STS in the entire Korean population between 2008 and 2011 from the HIRA database (to match the KNCI database search period). All claims records of outpatient visits or hospital admissions of patients containing “diagnosis of STS” between January 1, 2008 and December 31, 2011 were identified in the database. For cases involving more than one claim record that satisfied the inclusion criteria, only the claim record with the earliest date was counted. There were 3,155 patients, who were initially diagnosed with STS between 2008 and 2011: 1,132 in 2008, 671 in 2009, 685 in 2010, and 667 in 2011.
Orthopedic oncologists in Korea are advised to treat patients in adherence to the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines) [18]. The NCCN Guidelines for STS recommended that stage I tumors are routinely followed up every 3-6 months for 2-3 years and then annually <thereafter>; and stage II, III, or IV disease is followed up every 3-6 months for 2-3 years, then every 6 months for the next 2 years, and then annually <thereafter>. Actually, in our clinical experience, most of the follow-up intervals for STS are < 6-12 months until 5 years of no-evidence-of-disease (NED) status has been achieved, and annually thereafter. Therefore, when we additionally consider that local or distant disease recurrence is very rare after 5 years of NED, it can be assumed that absence of any claims record for the diagnosis or treatment of STS in the previous 12 months represents a new case. We therefore set a 1-year period (i.e., January 1 to December 31, 2008) as a “window period,” and patients with the first claim record in 2008 (n=1,132), which might include patients diagnosed before 2008, were excluded from our study.
In the HIRA database, a reimbursement claim for STS diagnosis is also made when an examination has been performed because STS is suspected, and not definitely diagnosed. The remaining 2,023 cases must involve these patients. Therefore, to determine whether these cases actually involved STS, we additionally investigated whether these patients had undergone any procedure for the treatment of this malignancy. The “procedure for STS” included STS-related surgery (removal of malignant soft tissue tumor [ICD-10 procedure code: N0232], limb-salvage procedure for malignant tumor removal [NA282 for thigh, scapula, and upper arm; NA283 for forearm and lower leg; and NA284 for hand and foot], and removal of a malignant neurogenic tumor [S4616]), a radiotherapy-related procedure (teletherapy [HD051-056], rotational irradiation [HD057-059], three-dimensional conformal therapy [HD061], body stereotactic radiosurgery [HD111, 112]), and/or a chemotherapy-related procedure (chemotherapy administration [KK151-156, 158, KK059]). Additionally, cases with both a diagnostic code for STS and a procedure code for the removal of a benign soft tissue tumor (N0233, N0234, and S4615), and with a claim date that preceded the earliest claim date for STS diagnosis by < 6 months and at the same anatomical site, were regarded as involving an unplanned excision, and were included in the analysis. Among the 2,023 patients, who were initially diagnosed with STS between 2009 and 2011, 879 patients had not undergone any treatment for STS, and were also excluded from this study. These 879 patients might include those who were initially suspected to have STS and were subsequently found to not have this malignancy, as well as patients newly diagnosed but not treated. Finally, 1,144 patients with a claims record for both “diagnosis of STS” and “procedure for STS” were included and analyzed. The diagnosis and procedure codes for STS were confirmed by a panel of oncologists specialized in extremity STS (2 orthopedic oncologists, 1 radiation oncologist, and 1 medical oncologist) working in a tertiary hospital in Korea.
3. Data analysis
The standard population was defined as the entire population of Korea, based on the 2010 Population and Housing Census (PHC) available from the Korean Statistical Information Service (http://kosis.kr) [19]. The Korean Statistical Information Service of the Korean central government conducts PHC every 5 years to obtain the following information: size, distribution, and structure of the Korean population and housing stock. Most recent PHC was conducted in 2010. A detailed age distribution of the Korean population is shown in Fig. 1.
Fig. 1.
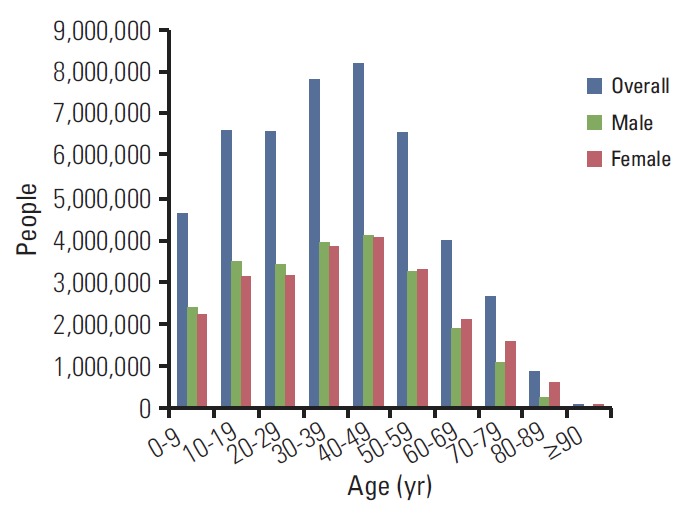
The age distribution of the Korean population based on the 2010 census from the Korean Statistical Information Service [19]. Notably, there were relatively few individuals aged ≥ 50 years.
For cases that occurred between 2009 and 2011, we presented the annual incidence rates per 100,000 people for each year. The incidence rates were calculated as the number of cases who had developed extremity STS divided by the whole population based on the 2010 census. The age at the earliest claim date of STS diagnosis was adopted as the patient’s age. The age and sex-specific incidence rates per 100,000 inhabitants were estimated. A 95% confidence interval (CI) of the incidence rate was estimated based on the Poisson distribution. The incidence rate according to sex was also estimated. Statistical analyses were performed using the SPSS ver. 21 (IBM Co., Armonk, NY). We also presented the distribution according to the anatomical site, the referral level of the hospital where the first diagnosis of STS was claimed, and the region of the hospital.
We divided the treatments into surgical and non-surgical categories, and then further subdivided these cases dependent on the administration of radiotherapy or chemotherapy.
Results
From the KNCI database, a total of 1,236 patients newly diagnosed with extremity STS during the 3-year study period (January 2009 to December 2011) were identified. The mean incidence rate was 0.86 per 100,000 people per year (95% CI, 0.68 to 1.03). The mean incidence and incidence rates of extremity STS per 100,000 people by sex and age group are listed in Table 1 and Fig. 2. The annual incidence rates of age ≥ 80 were 4.51 (95% CI, 3.160 to 5.863) for male and 2.01 (95% CI, 1.449 to 2.563) for female (p < 0.01).
Table 1.
The incidence and incidence rate of extremity STS per 100,000 people by sex and age group in South Korea (2009-2011)
| Age (yr) | No. of patients (2009-2011) |
Population (2010)a) |
Annual incidence ratesb) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | Male | Female | Overall | Male | Female | Overall | Male | Female | |
| 0-9 | 20 | 9 | 11 | 4,613,747 | 2,385,514 | 2,228,233 | 0.14 | 0.13 | 0.16 |
| 10-19 | 67 | 40 | 27 | 6,611,640 | 3,481,143 | 3,130,497 | 0.34 | 0.38 | 0.29 |
| 20-29 | 100 | 62 | 38 | 6,594,369 | 3,428,176 | 3,166,193 | 0.51 | 0.60 | 0.40 |
| 30-39 | 138 | 77 | 61 | 7,794,495 | 3,926,630 | 3,867,865 | 0.59 | 0.65 | 0.53 |
| 40-49 | 195 | 94 | 101 | 8,204,781 | 4,116,072 | 4,088,709 | 0.79 | 0.76 | 0.82 |
| 50-59 | 239 | 135 | 104 | 6,564,826 | 3,248,720 | 3,316,106 | 1.21 | 1.39 | 1.05 |
| 60-69 | 218 | 120 | 98 | 3,994,404 | 1,890,277 | 2,104,127 | 1.82 | 2.12 | 1.55 |
| 70-79 | 180 | 88 | 92 | 2,650,381 | 1,083,620 | 1,566,761 | 2.26 | 2.71 | 1.96 |
| 80-89 | 74 | 34 | 40 | 866,675 | 260,126 | 606,549 | 2.85 | 4.36 | 2.2 |
| ≥ 90 | 5 | 4 | 1 | 95,443 | 20,618 | 74,825 | 1.75 | 6.47 | 0.45 |
| Total | 1,236 | 663 | 573 | 47,990,761 | 23,840,896 | 24,149,865 | 0.86 | 0.93 | 0.79 |
Population of Korea was based on the 2010 census from the Korean Statistical Information Service [19],
Incidence of extremity soft tissue sarcoma (STS) per 100,000 people per year.
Fig. 2.
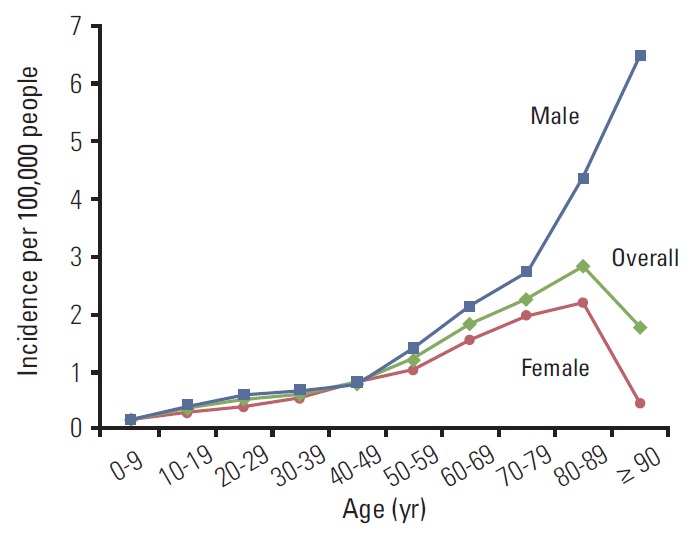
The mean incidence and incidence rates of extremity soft tissue sarcoma per 100,000 people by sex and age group.
Of the 1,236 patients who were newly diagnosed with extremity STS during the study period, 1,144 (92.6%) underwent at least one of the 3 treatment modalities: surgery, radiotherapy, or chemotherapy. The distribution of patients who underwent treatment according to year, sex, age, and anatomical site is presented in Table 2 and Fig. 3.
Table 2.
The proportions of patients who were treated according to the year, sex, age, and anatomical site
| Variable | Total | Patients who underwent treatment | Patients who underwent treatment (%) |
|---|---|---|---|
| Incidence (No. of patients) | |||
| 2009 | 392 | 376 | 95.9 |
| 2010 | 393 | 393 | 100 |
| 2011 | 451 | 375 | 83.1 |
| 2009-2011 | 1,236 (average, 412.0) | 1,144 (average, 381.3) | 92.6 |
| Sex | |||
| Male | 663 (53.6) | 624 (54.5) | 94.1 |
| Female | 573 (46.4) | 520 (45.5) | 90.8 |
| Age (yr) | |||
| 0-9 | 20 | 20 | 100 |
| 10-19 | 67 | 67 | 100 |
| 20-29 | 100 | 88 | 88.0 |
| 30-39 | 138 | 129 | 93.5 |
| 40-49 | 195 | 180 | 92.3 |
| 50-59 | 239 | 235 | 98.3 |
| 60-69 | 218 | 198 | 90.8 |
| 70-79 | 180 | 158 | 87.8 |
| 80-89 | 74 | 64 | 86.5 |
| ≥90 | 5 | 5 | 100 |
| Anatomical site | |||
| Upper extremity | 319 (25.8) | 309 (27.0) | 96.9 |
| Lower extremity | 917 (74.2) | 835 (73.0) | 91.1 |
Values are presented as number (%) unless otherwise indicated.
Fig. 3.
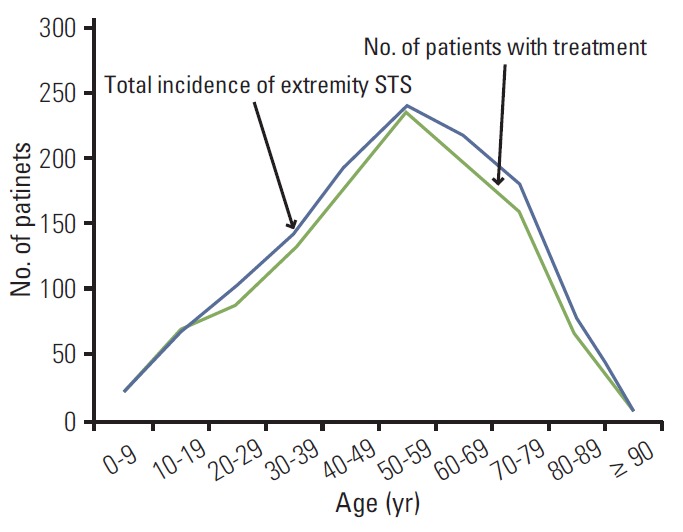
Total incidence of extremity soft tissue sarcoma (STS) (blue line) and the number of patients who underwent treatment (green line).
The treatment patterns, including treatment modality, the distribution of hospitals (where the first diagnostic code of extremity STS was claimed), and the regional distribution of those hospitals, are listed in Table 3. Overall, approximately 85% of patients underwent surgical excision.
Table 3.
Treatment patterns for patients with extremity soft tissue sarcoma in 2009-2012
| Characteristic | No. of patients (%) |
|---|---|
| Treatment modality | |
| With surgery | 969 (84.7) |
| Surgery alone | 664 (58.0) |
| Surgery and RT | 126 (11.0) |
| Surgery and CTx | 85 (7.4) |
| Surgery, RT, and CTx | 94 (8.2) |
| Without surgery | 175 (15.3) |
| RT only | 59 (5.2) |
| CTx only | 76 (6.4) |
| RT and CTx | 43 (3.8) |
| Hospital distribution | |
| Tertiary hospital | 776 (67.8) |
| General hospital | 306 (26.7) |
| Hospital | 18 (1.6) |
| Clinic | 44 (3.8) |
| Regional distribution | |
| Seoul | 563 (49.2) |
| Busan | 143 (12.5) |
| Gyeonggi-do | 112 (9.8) |
| Daegu | 89 (7.8) |
| Gwangju | 50 (4.4) |
| Jeollabuk-do | 43 (3.8) |
| Others | 144 (12.6) |
RT, radiation therapy; CTx, chemotherapy.
Discussion
Because of its rarity and heterogeneity, a large population-based database is needed to estimate the nationwide incidence of STS [4-9]. There have been several previous epidemiological studies on the incidence of STS, but most of them were conducted in Western countries and targeted STS of the whole body. This is the first nationwide study of the incidence and treatment pattern of extremity STS in Korea using two national databases, which together include the entire Korean population. This study could serve as the backbone for future clinical trials and nationwide strategy planning for STS.
Most previous studies used either cancer registries [4] or databases covering some portion of the whole population [5]. We used two nationwide databases that include the whole Korean population, but were based on different systems, one of which was a registry-based system and the other a claim-based system. Each system has its associated advantages and disadvantages. The KNCI database, based on a cancer registry system, contains only patients with a confirmed diagnosis of STS, and thus has a high diagnostic accuracy, but it cannot provide detailed information regarding the treatment because only the diagnostic codes and basic demographics are registered. In comparison, the HIRA database may lack diagnostic accuracy because it is based on the claim system for insurance from each physician; the diagnosis of a specific disease is also claimed if an examination has been performed due to disease suspicion without diagnosis. However, this claim system can provide detailed treatment information when the treatment is highly specific for a disease, such as cancer. Furthermore, as all Korean residents receive a unique identification number that is used in both databases, each database can be used to obtain specific patient data without duplications or omissions.
There are some considerations when interpreting the results of this study. First, we obtained the total number of newly diagnosed extremity STS cases from the KNCI database and the treatment patterns from the HIRA database. This separate acquisition of data from the two independent databases warrants caution when interpreting the results of this study. Therefore, there could be differences in patients included for any given year between the databases; some patients who underwent diagnostic tests because STS was suspected close to the end of year had their claims entered to HIRA in that year but entered to KNCI in the following year if confirmative biopsies were performed then. However, such difference would not affect the main result because it is likely to represent a relatively small number of cases, and we analyzed combined patient data over a 3-year period. Second, amputation is not included as a procedure for STS. This is because most orthopedic oncologists do not perform limb amputation as the initial surgical treatment. Even in cases where amputation was the only surgical procedure for STS, the reimbursement claim usually combines it under the category of “removal of malignant soft tissue tumor (N0232).” Furthermore, categorizing amputation as a procedure for STS could result in overestimation of the number of cases, as patients with late complications, such as infection or trauma several years after treatment, could be included as new cases. Third, we could not assess specific information, such as the presence of metastasis, histological grade of the tumor, or specific diagnosis of each patient, and any of these factors may have affected the treatment modality. Therefore, we only present the current treatment patterns without an explanation or even speculation on the exact reasons for such patterns. Fourth, the results of this study may not represent the official national data of Korea, as the study was performed based on the data requested by researchers from a single institution.
In our study, the mean incidence rate of extremity STS in the Korean population was found to be approximately 0.9 per 100,000 people annually. As many as 1.85 new cases of extremity STS of the trunk wall per 100,000 people per year were previously reported in Finland [20]. Furthermore, although not specifically for extremity STS, many previous studies reported an incidence of 1.8-5.0 per 100,000 people per year of whole body STS [4-9]. Given that extremity STS occurs in approximately 50%-60% of whole body STSs [10,21,22], its incidence in the Korean population is one of the lowest reported. This may be explained by different inclusion criteria adopted by different studies. For example, the incidence of STS between 1984 and 2004 in Austria was 2.4 per 100,000 persons per year, with a total of 5,333 cases [9]. However, when the same criteria used for diagnostic code C45-C49 (mesothelial and soft tissue) in our study were applied, there were only 3,312 cases of whole body STS, and the incidence rate was reduced to approximately 1.5 per 100,000 persons per year. Given that it still included cases of STS in other parts of the body, it can be inferred that the incidence rate of extremity STS would be 0.8-0.9 cases per 100,000 persons per year, which is almost the same as that observed in our study. Furthermore, unlike our study, many other studies included Kaposi’s sarcoma as a target disease [5,6]. The increasing incidence of immunodeficiency-related Kaposi’s sarcoma could also partly explain the differences in the rates of STS. Additionally, the ethnic differences between the populations of different countries may also contribute to the observed differences in the incidence of STS. Finally, the different age distributions of populations could additionally contribute to the differences in the incidence of this malignancy. As shown in Fig. 1, relatively few Koreans are aged > 50 years. As the incidence of STS tends to increase with age (Fig. 2), the relatively young population in Korea might contribute to the low incidence of STS. However, the proportion of elders in Korea is expected to increase rapidly [23]. If this is true, as the population grows older, the incidence of STS is likely to increase in the future due to its higher incidence rate in older people. Although its incidence is lower than that of other cancer types, the changes in the incidence of extremity STS should be carefully monitored because of the high mortality associated with this disease [2,3].
Of the extremity STS patients, approximately 93% underwent treatments. There was a minor tendency for older people to not receive treatment, with patients aged 70-89 years least likely to receive treatment (Table 3). Among patients who were treated for extremity STS, this usually involved surgical excision in approximately 85% of cases. According to one hospital-based study, only 6% of STS patients did not undergo surgery [24], but a greater proportion of patients (15%) did not undergo surgical excision in our study; overall 26% and 28% of patients in our study received chemotherapy and radiotherapy, respectively. This is rather higher than the results reported in a previous study [24], and it is unclear whether these differences reflect the fact that the previous study was hospital-based, while ours was population-based, or whether it actually reflects the differences in treatment patterns between countries.
Some demographic characteristics, such as sex, also varied among different countries and studies [4,6,7]. On contrary to many other studies [4,5,9], our study, together with many previous studies, found that STS was more common in men [7,8]. Most previous studies in Korea regarding STS also found that men had STS more frequently, although none of these were population-based [25]. Overall, no clear tendency with respect to sex bias in STS development can be discerned.
Approximately 75%-85% of STSs are reported in adults [5]. In our study, only 7.0% (87 of 1,236) of cases involved patients aged < 20 years. We noted a continuously increasing incidence of STS with age, especially among men (Fig. 2). The highest incidence was found in both sexes between aged 80 and 89 years, but the incidence increased consistently with increasing age among men. The overall incidence in older people mainly depends on the incidence in female patients because there are many more women than men in this age group.
Conclusion
The annual incidence rate of extremity STS in the Korean population is approximately 0.9 per 100,000 people, with relatively more men affected than women, and this rate could increase as the population continues to age. The differences between sexes increased with age, and were especially apparent in patients aged > 80 years. Approximately 93% of STS patients received treatment, of whom 85% underwent surgical excision. This is the first nationwide study of the incidence and treatment patterns of extremity STS in Korea using two national databases that include the whole population (KNCI and HIRA). The results of this study might be useful for planning future national STS management.
Acknowledgments
Supported by Korean Human Technology Research Foundation, Grant No. KOHTERF-2014-02. The contents of this study do not represent the official views of the Korea Central Cancer Registry.
Footnotes
Conflict of interest relevant to this article was not reported.
References
- 1.Boring CC, Squires TS, Tong T. Cancer statistics, 1993. CA Cancer J Clin. 1993;43:7–26. doi: 10.3322/canjclin.43.1.7. [DOI] [PubMed] [Google Scholar]
- 2.Sondak VK. Sarcomas of bone and soft tissue. In: Greenfield LJ, Mulholland MW, Oldham KT, editors. Surgery: scientific principles and practice. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2000. pp. 2258–80. [Google Scholar]
- 3.Parsons HM, Habermann EB, Tuttle TM, Al-Refaie WB. Conditional survival of extremity soft-tissue sarcoma: results beyond the staging system. Cancer. 2011;117:1055–60. doi: 10.1002/cncr.25564. [DOI] [PubMed] [Google Scholar]
- 4.Levi F, La Vecchia C, Randimbison L, Te VC. Descriptive epidemiology of soft tissue sarcomas in Vaud, Switzerland. Eur J Cancer. 1999;35:1711–6. doi: 10.1016/s0959-8049(99)00179-3. [DOI] [PubMed] [Google Scholar]
- 5.Ross JA, Severson RK, Davis S, Brooks JJ. Trends in the incidence of soft tissue sarcomas in the United States from 1973 through 1987. Cancer. 1993;72:486–90. doi: 10.1002/1097-0142(19930715)72:2<486::aid-cncr2820720226>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 6.Schuurman B, Meyer S, Cuesta MA, Nauta JJ. Increasing frequency of soft tissue sarcomas in The Netherlands. Ned Tijdschr Geneeskd. 1992;136:1556–60. [PubMed] [Google Scholar]
- 7.Storm HH. Cancers of the soft tissues. Cancer Surv. 1994;19-20:197–217. [PubMed] [Google Scholar]
- 8.Toro JR, Travis LB, Wu HJ, Zhu K, Fletcher CD, Devesa SS. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the surveillance, epidemiology and end results program, 1978-2001: an analysis of 26,758 cases. Int J Cancer. 2006;119:2922–30. doi: 10.1002/ijc.22239. [DOI] [PubMed] [Google Scholar]
- 9.Wibmer C, Leithner A, Zielonke N, Sperl M, Windhager R. Increasing incidence rates of soft tissue sarcomas? A population-based epidemiologic study and literature review. Ann Oncol. 2010;21:1106–11. doi: 10.1093/annonc/mdp415. [DOI] [PubMed] [Google Scholar]
- 10.Lewis JJ, Brennan MF. Soft tissue sarcomas. Curr Probl Surg. 1996;33:817–72. [PubMed] [Google Scholar]
- 11.Shin HR, Won YJ, Jung KW, Kong HJ, Yim SH, Lee JK, et al. Nationwide cancer incidence in Korea, 1999~2001; first result using the national cancer incidence database. Cancer Res Treat. 2005;37:325–31. doi: 10.4143/crt.2005.37.6.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Health Insurance Review and Assessment Service . Seoul: National Health Insurance Service; c2013. Health insurance statistics yearbook: 9th annual publication [Internet] [cited 2013 Sep 1]. Available from: http://www.hira.or.kr. [Google Scholar]
- 13.Park YT, Yoon JS, Speedie SM, Yoon H, Lee J. Health insurance claim review using information technologies. Healthc Inform Res. 2012;18:215–24. doi: 10.4258/hir.2012.18.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin DM. International Classification of Disease for Oncology. 3rd ed. Geneva: World Health Organization; 2000. [Google Scholar]
- 15.Korea Central Cancer Registry. International Classification of Diseases for Oncology. 3rd ed. (Korean version) Goyang: National Cancer Center; 2003. [Google Scholar]
- 16.World Health Organization . Manual of the international statistical classification of diseases, injuries, and causes of death. 10th revision. Geneva: World Health Organization; 1992. [Google Scholar]
- 17.Gong HS, Oh WS, Chung MS, Oh JH, Lee YH, Baek GH. Patients with wrist fractures are less likely to be evaluated and managed for osteoporosis. J Bone Joint Surg Am. 2009;91:2376–80. doi: 10.2106/JBJS.H.01871. [DOI] [PubMed] [Google Scholar]
- 18.Demetri GD, Antonia S, Benjamin RS, Bui MM, Casper ES, Conrad EU, 3rd, et al. Soft tissue sarcoma. J Natl Compr Canc Netw. 2010;8:630–74. doi: 10.6004/jnccn.2010.0049. [DOI] [PubMed] [Google Scholar]
- 19.Statistics Korea . Daejeon: Statistics Korea; Estimates of future population 2010-2060 [Internet] c2012 [cited 2012 Sep 15]. Available from: http://kosis.kr. 2010. [Google Scholar]
- 20.Sampo MM, Ronty M, Tarkkanen M, Tukiainen EJ, Bohling TO, Blomqvist CP. Soft tissue sarcoma: a population-based, nationwide study with special emphasis on local control. Acta Oncol. 2012;51:706–12. doi: 10.3109/0284186X.2011.643821. [DOI] [PubMed] [Google Scholar]
- 21.Brennan MF. Management of extremity soft-tissue sarcoma. Am J Surg. 1989;158:71–8. doi: 10.1016/0002-9610(89)90319-x. [DOI] [PubMed] [Google Scholar]
- 22.Lawrence W Jr, Donegan WL, Natarajan N, Mettlin C, Beart R, Winchester D. Adult soft tissue sarcomas: a pattern of care survey of the American College of Surgeons. Ann Surg. 1987;205:349–59. doi: 10.1097/00000658-198704000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kang YP, Cho MH. Elderly population distribution and it's evolution in Korea: 1980, 1990, 2000. J Korean Cartogr Assoc. 2005;5:1–5. [Google Scholar]
- 24.Bauer HC, Trovik CS, Alvegard TA, Berlin O, Erlanson M, Gustafson P, et al. Monitoring referral and treatment in soft tissue sarcoma: study based on 1,851 patients from the Scandinavian Sarcoma Group Register. Acta Orthop Scand. 2001;72:150–9. doi: 10.1080/000164701317323408. [DOI] [PubMed] [Google Scholar]
- 25.Kang S, Han I, Lee S, Kim W, Kim H. Clinicopathological characteristics and prognostic factors of T1 (≤ 5 cm) soft tissue sarcoma: a comparative study with T2 (> 5 cm) soft tissue sarcoma. Eur J Surg Oncol. 2014;40:406–11. doi: 10.1016/j.ejso.2013.12.010. [DOI] [PubMed] [Google Scholar]