

Abstract
Purpose
Primary central nervous system lymphoma (PCNSL) is an uncommon brain tumor accounting for 2%-5% of all primary brain tumors. Few population-based analyses of survival for patients with PCNSL have been conducted, particularly in Asian countries.
Materials and Methods
Using the Korea National Cancer Incidence Database, 1,062 cases of PCNSL newly diagnosed from 1999 to 2009 were analyzed. The crude rate, age-standardized rate (ASR), and annual percent change were calculated. To estimate the observed survival, we restricted the data to between 1999 and 2007 and followed the cases until December 2010. The overall survival was estimated using the Kaplan-Meier method, and piecewise Poisson regression model.
Results
The ASR for PCNSL between 1999 and 2009 was 0.17 per 100,000, and the annual percent change from 1999 to 2009 was 8.8% (p < 0.001). The ASR of males was higher than that of females, and the older groups (60s or over) showed the largest increase in incidence rates. For all ages, the five-year survival from PCNSL was 29.9% between 1999 and 2007. Survival from PCNSL is known to show strong association with age at diagnosis.
Conclusion
These results are similar to those of previous studies. Our findings may be helpful to clinicians and patients in determining long-term prognoses for PCNSL.
Keywords: Central nervous system, Lymphoma, Neoplasms, Registries, Incidence, Survival, Korea
Introduction
Primary central nervous system lymphoma (PCNSL) is an uncommon brain tumor accounting for 2%-5% of all primary brain tumors [1,2]. Between 1970 and 1990, the incidence of PCNSL increased significantly in both immunocompromised and immunocompetent individuals [3]. The age-adjusted incidence of PCNSL has increased substantially over the past 30 years [2,4]. These increases cannot be completely explained by changes in medical practice, or by changes in nosology and are independent of overall trends in the incidence of brain tumors and non-Hodgkin lymphoma (NHL). PCNSL comprises 2.0% of all brain tumors in Korea, with an increase from 1.2% in 1999 to 3.3% in 2009.
In 1980, the Korean Ministry of Health and Welfare started a nationwide, hospital-based cancer registry (the Korea Central Cancer Registry, KCCR). The Korea National Cancer Incidence Database was constructed by merging the KCCR database and all eight population-based regional cancer registry databases, data from an additional medical record review survey, and the cancer mortality database. Since 2005, the KCCR database has been especially useful for showing trends in cancer registration, including benign and borderline tumors of the central nervous system (CNS).
One study reported population-based survival data between 1999 and 2004 for primary brain tumors in Korea [5]. To predict the future incidence of PCNSL in Korea and to facilitate the implementation of efficient health care planning, we have performed a new analysis for nationwide population-based incidence and survival of PCNSL.
Materials and Methods
The KCCR had been collecting information on approximately 80%-90% of cancer cases from more than 150 training hospitals across the country. The KCCR then expanded cancer registration to cover the entire population under the population-based regional cancer registry program, and additional medical record surveys have been conducted since 2003. The national cancer incidence reports for cancer patients diagnosed since 1999 have been published since 2005. KCCR data from 1999 to 2002 and from 2003 to 2007 have been published in Cancer Incidence in Five Continents Vol. 9 [6] and Vol. 10 [7], which reflects the completeness of the incidence data.
The basic information available included demographic characteristics of the patients, date of diagnosis, primary site, and histological type of the tumor according to the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3).
A total of 1,062 cases of primary CNS lymphoma newly diagnosed from 1999 to 2009 were analyzed. For survival analysis, we restricted the data to patients diagnosed with histologically confirmed PCNSL from 1999 to 2007. We excluded cases that could not be followed up due to mismatched personal identification numbers and cases that were not first primary sites. As a result, 688 newly diagnosed cases of PCNSL from 1999 to 2007 were included. Passive follow-up was performed until December 31, 2010. The survival duration in each case was determined as the time difference (in months) from the date of initial diagnosis to the date of death, date of loss to follow-up, or the closing date for follow-up, whichever came first.
Crude rates (CRs) and age-standardized rates (ASRs) were calculated. The ASR was determined using Segi’s world population as a standard [8]. Annual percent changes (APC) for the incidence rates were calculated using a linear model according to the following formula: (exp(b)–1)×100, where b is the slope of the regression of the natural logarithm of the ASR in a calendar year [9]. Kaplan-Meier analysis was used to compare overall survival over sex, age group, and year of diagnosis using the log-rank test. We also applied piecewise Poisson regression model adjusting sex, age, and year of diagnosis. Two-tailed tests were used for all comparisons. All analyses were performed using SAS ver. 9.1 (SAS Institute Inc., Cary, NC) and Stata ver. 11.2 (StataCorp LP, College Station, TX).
Results
1. Epidemiological characteristics of registered primary CNS lymphoma
A total of 1,062 primary CNS lymphoma patients were registered between 1999 and 2009; 614 (57.8%) were males and 448 (42.2%) were females (Table 1). The ASR for CNS lymphoma was 0.17 per 100,000 between 1999 and 2009. The ASR for males was 0.22, and that for females was 0.14. The age group between 60 and 69 years old was the largest (n=303, 28.5%). The median age of primary CNS lymphoma patients was 58 years (range, 48 to 67 years) (data not shown). The ASR was 0.11 per 100,000 in 1999 and 0.25 in 2009 (APC; 8.8%; p < 0.001) (Table 2); these increases began in 2002 (Fig. 1). Increases in age-specific rates for those in their 60s and 70s or over were the largest in 1999-2001 and 2006-2009 (Fig. 2).
Table 1.
Demographic characteristics of primary central nervous system lymphoma, Korea, 1999-2009
| Characteristic | No. of cases (%) | Crude rate | Age-standardized rate |
|---|---|---|---|
| Total | 1,062 (100) | 0.20 | 0.17 |
| Gender | |||
| Male | 614 (57.8) | 0.23 | 0.22 |
| Female | 448 (42.2) | 0.17 | 0.14 |
| Age group (yr) | |||
| 0-14 | 18 (1.7) | 0.02 | - |
| 15-39 | 116 (10.9) | 0.05 | - |
| 40-49 | 171 (16.1) | 0.20 | - |
| 50-59 | 263 (24.8) | 0.47 | - |
| 60-69 | 303 (28.5) | 0.78 | - |
| ≥ 70 | 191 (18.0) | 0.70 | - |
Age-standardized rate per 100,000 was standardized using world standard population.
Table 2.
Trends in central nervous system lymphoma incidence, Korea, 1999-2009
| Year | No. of cases (%) | Crude rate Age-standardized rate | |
|---|---|---|---|
| 1999 | 55 (5.2) | 0.12 | 0.11 |
| 2000 | 58 (5.5) | 0.12 | 0.11 |
| 2001 | 55 (5.2) | 0.11 | 0.11 |
| 2002 | 72 (6.8) | 0.15 | 0.14 |
| 2003 | 84 (7.9) | 0.17 | 0.15 |
| 2004 | 97 (9.1) | 0.20 | 0.18 |
| 2005 | 101 (9.5) | 0.21 | 0.18 |
| 2006 | 114 (10.7) | 0.23 | 0.20 |
| 2007 | 130 (12.2) | 0.26 | 0.22 |
| 2008 | 134 (12.6) | 0.27 | 0.21 |
| 2009 | 162 (15.3) | 0.33 | 0.25 |
| 1999-2009 | 1,062 (100) | 0.20 | 0.17 |
| Annual percent change 8.8% (p < 0.001) | |||
Age-standardized rate per 100,000 was standardized using world standard population.
Fig. 1.
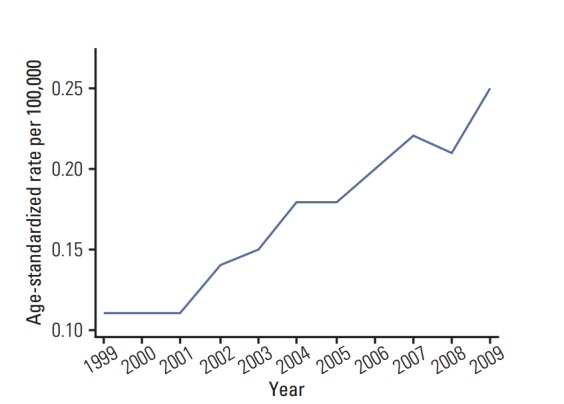
Incidence rate trends in central nervous system lymphoma, Korea, 1999-2009.
Fig. 2.
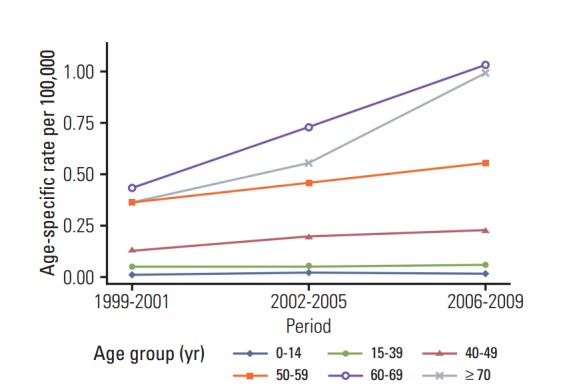
Trends in age-specific rates of central nervous system lymphoma by period of diagnosis, Korea, 1999-2009.
2. Survival from primary CNS lymphoma by gender and age
We analyzed survival data for 688 PCNSL patients diagnosed with histological verification between 1999 and 2007 by gender, year of diagnosis, and age group (Table 3, Figs. 3-5). The median survival for the 688 PCNSL patients was 21.0 months. The 1-year survival was 60.2%, 3-year survival was 39.1%, and 5-year survival was 29.9%. For males (n=416), the median survival was 19.0 months compared with 24.0 months for females (n=272, p=0.099). The 10-year survival of CNS lymphoma patients diagnosed from 1999 to 2000 was 17.6%; the survival of females was slightly higher than that of males, but the difference was statistically non-significant (Table 4, Fig. 5).
Table 3.
Survival of central nervous system lymphoma patients in Korea by gender, year of diagnosis (1999-2007), and age at diagnosis
| Characteristic | No. | Median survival (mo) | Kaplan-Meier survival (%) |
p-value | ||
|---|---|---|---|---|---|---|
| 1 yr | 3 yr | 5 yr | ||||
| Total | 688 | 21.0 | 60.2 | 39.1 | 29.9 | |
| Gender | 0.099 | |||||
| Male | 416 | 19.0 | 55.5 | 37.5 | 28.7 | |
| Female | 272 | 24.0 | 67.3 | 41.5 | 31.8 | |
| Year of diagnosis | 0.157 | |||||
| 1999-2001 | 161 | 18.0 | 57.1 | 34.8 | 23.0 | |
| 2002-2004 | 227 | 21.0 | 63.9 | 38.8 | 32.2 | |
| 2005-2007 | 300 | 22.5 | 59.0 | 41.7 | 31.3 | |
| Age group (yr) | < 0.001 | |||||
| 0-14 | 13 | NA | 69.2 | 69.2 | 61.5 | |
| 15-39 | 83 | NA | 71.1 | 62.7 | 58.4 | |
| 40-49 | 114 | 33.0 | 71.9 | 48.3 | 40.4 | |
| 50-59 | 188 | 28.0 | 66.5 | 44.7 | 28.5 | |
| 60-69 | 199 | 16.0 | 55.3 | 31.2 | 22.6 | |
| ≥ 70 | 91 | 6.0 | 31.9 | 7.7 | 3.7 | |
NA, not applicable.
Fig. 3.
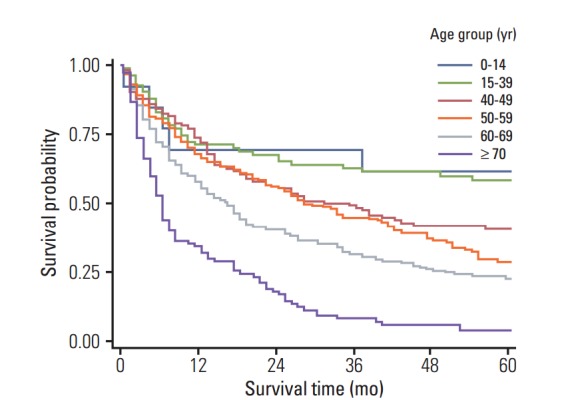
Survival curves by age of diagnosis (yr), 1999-2007.
Fig. 4.
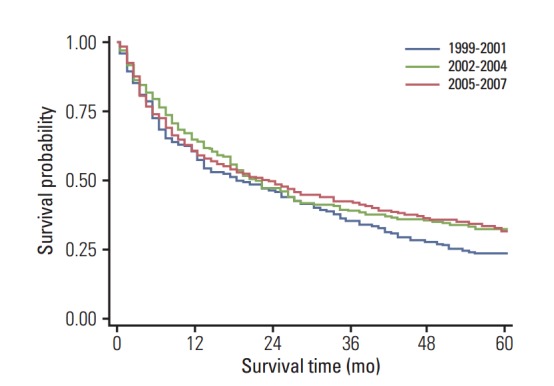
Survival curves by year of diagnosis, 1999-2007.
Fig. 5.
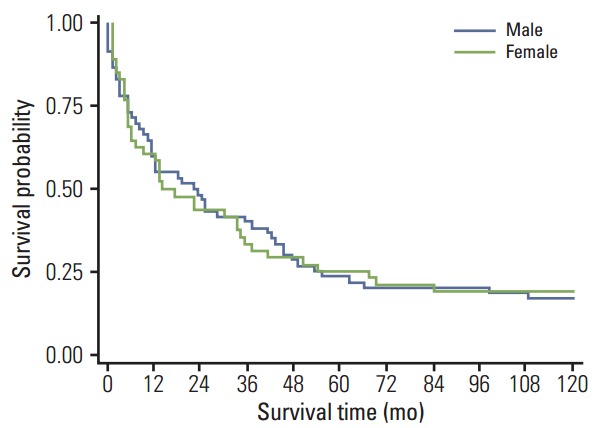
Survival curves by sex, 1999-2000.
Table 4.
Ten-year survival of central nervous system lymphoma patients diagnosed in 1999-2000 by gender and age at diagnosis
| Characteristic | No. | Kaplan-Meier survival (%) | p-value | |||
|---|---|---|---|---|---|---|
| 1 yr | 3 yr | 5 yr | 10 yr | |||
| Total | 108 | 57.4 | 37.0 | 24.1 | 17.6 | |
| Gender | 0.995 | |||||
| Male | 60 | 58.3 | 40.0 | 23.3 | 16.7 | |
| Female | 48 | 56.3 | 33.3 | 25.0 | 18.8 | |
| Age group (yr) | 0.001 | |||||
| 0-14 | 1 | 100.0 | 100.0 | 0.0 | 0.0 | |
| 15-39 | 22 | 59.1 | 54.6 | 50.0 | 40.9 | |
| 40-49 | 17 | 76.5 | 47.1 | 41.2 | 29.4 | |
| 50-59 | 32 | 59.4 | 43.8 | 15.6 | 9.4 | |
| 60-69 | 25 | 52.0 | 20.0 | 12.0 | 8.0 | |
| ≥ 70 | 11 | 27.3 | 0.0 | 0.0 | 0.0 | |
3. Multivariable survival analysis of primary CNS lymphoma patients
Poisson regression model estimated that the overall mortality rate for patients aged 60-69 and over 70 increased 3.16 folds, and 6.67 folds compared to patients aged 0-14, respectively. Female patients showed relatively good survival (23%) compared to males (Table 5).
Table 5.
Multivariable piecewise Poisson model of central nervous system lymphoma patients in Korea
| Characteristic | Rate ratio (95% confidence interval) |
|---|---|
| Gender | |
| Male | 1.00 |
| Female | 0.77 (0.64-0.93) |
| Year of diagnosis | |
| 1999-2001 | 1.00 |
| 2002-2004 | 0.75 (0.59-0.95) |
| 2005-2007 | 0.73 (0.59-0.92) |
| Age group (yr) | |
| 0-14 | 1.00 |
| 15-39 | 1.12 (0.44-2.86) |
| 40-49 | 1.86 (0.75-4.62) |
| 50-59 | 2.26 (0.92-5.53) |
| 60-69 | 3.16 (1.29-7.70) |
| ≥ 70 | 6.67 (2.69-16.50) |
Discussion
Comparison of survival between countries is difficult due to possible differences in pathological assessment of tumors and changes in the standard of care over time. However, the survival in Korea is as good as that reported in other studies [2,10,11].
PCNSL affects all age groups, with a peak incidence in the fifth to seventh decade in non-acquired immune deficiency syndrome (AIDS) patients. It has become the most common brain tumor in AIDS patients, although the introduction of highly active anti-retroviral therapy (HAART) in 1995 has resulted in dramatically reduced occurrence of all NHL [12], such that the incidence rates of primary and secondary brain lymphomas dropped from 2.8 per 1,000 patient-years in 1990 to 0.4 in 1998 [13]. Despite this reduction, there has been no concomitant decrease in the rates for immunocompetent individuals. A study based on the Surveillance, Epidemiology and End Results (SEER) programs, which included approximately 10% of the United States population, reported a threefold increase in the incidence of PCNSL [4]. In our study, PCNSL increased from 1.2% in 1999 to 3.3% in 2009. It is important to examine the question of whether the increase in PCNSL incidence is real or an artifact of the increasing age of the population, increased use of health screening tests, or improved diagnostic techniques.
Older age, Eastern Cooperative Oncology Group (ECOG) performance status > 2, multifocal or meningeal disease, and uncleaved histology have been associated with shorter survival among CNS lymphoma patients [11,14]. Among these factors, survival is known to show strong association with age at diagnosis. Our findings were similar to those of other papers regarding these characteristics.
Many studies have reported a further increase in PCNSL during the eighties and early nineties in immunocompetent patients [15,16]. In Korea, the age group between 60 and 69 years old was the largest (n=303, 28.5%). Our study is based on data from a nationwide, population-based cancer registry. Although many reports on PCNSL are based on hospital series, survival from population-based registry data has rarely been reported. Population-based survival reflects the average prognosis of unselected patients with a variety of natural histories and treatment patterns. Use of survival as a criterion reduced the likelihood of selection bias.
The data in the KCCR are of high quality, and completeness has been estimated as over 97% in recent years [17]. However, no information on chemotherapy method or radiation extent was available; therefore, we could not precisely analyze prognostic factors.
Conclusion
The ASR for PCNSL between 1999 and 2009 was 0.17 per 100,000. Males had higher incidence than that of females, and the older groups (60s or over) showed the largest increase in incidence rates. The 5-year survival from PCNSL was 29.9% between 1999 and 2007. Our findings may be helpful to clinicians and patients in determining long-term prognoses for PCNSL, and could be used as a master control data set for single-arm clinical trials, especially in Asian populations.
Acknowledgments
This work was supported by a research grant from the National Cancer Center (no. 1310220).
Footnotes
Conflict of interest relevant to this article was not reported.
References
- 1.Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer. 1972;29:252–60. doi: 10.1002/1097-0142(197201)29:1<252::aid-cncr2820290138>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 2.Olson JE, Janney CA, Rao RD, Cerhan JR, Kurtin PJ, Schiff D, et al. The continuing increase in the incidence of primary central nervous system non-Hodgkin lymphoma: a surveillance, epidemiology, and end results analysis. Cancer. 2002;95:1504–10. doi: 10.1002/cncr.10851. [DOI] [PubMed] [Google Scholar]
- 3.Schlegel U, Schmidt-Wolf IG, Deckert M. Primary CNS lymphoma: clinical presentation, pathological classification, molecular pathogenesis and treatment. J Neurol Sci. 2000;181:1–12. doi: 10.1016/s0022-510x(00)00385-3. [DOI] [PubMed] [Google Scholar]
- 4.Eby NL, Grufferman S, Flannelly CM, Schold SC, Jr, Vogel FS, Burger PC. Increasing incidence of primary brain lymphoma in the US. Cancer. 1988;62:2461–5. doi: 10.1002/1097-0142(19881201)62:11<2461::aid-cncr2820621135>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 5.Jung KW, Yoo H, Kong HJ, Won YJ, Park S, Lee SH. Population-based survival data for brain tumors in Korea. J Neurooncol. 2012;109:301–7. doi: 10.1007/s11060-012-0893-5. [DOI] [PubMed] [Google Scholar]
- 6.Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al. Cancer incidence in five continents, Vol. IX. IARC Scientific Publications, No. 160. Lyon: International Agency for Research on Cancer; 2007. [Google Scholar]
- 7.Forman D, Bray F, Brewster D, Gombe Mbalawa C, Kohler B, Pineros M, et al. Lyon: International Agency for Research on Cancer; 2014. Cancer incidence in five continents, Vol. X [Internet] [cited 2015 Feb 10]. Available from: http://ci5.iarc.fr. [DOI] [PubMed] [Google Scholar]
- 8.Segi M, Fujisaku S. Cancer mortality for selected sites in 24 countries (1950-1957) Sendai: Tohoku University School of Medicine; 1960. [Google Scholar]
- 9.Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, et al. SEER cancer statistics review, 1975-2007. Bethesda, MD: National Cancer Institute; 2010. [Google Scholar]
- 10.Ney DE, Reiner AS, Panageas KS, Brown HS, DeAngelis LM, Abrey LE. Characteristics and outcomes of elderly patients with primary central nervous system lymphoma: the Memorial Sloan-Kettering Cancer Center experience. Cancer. 2010;116:4605–12. doi: 10.1002/cncr.25363. [DOI] [PubMed] [Google Scholar]
- 11.Ferreri AJ, Blay JY, Reni M, Pasini F, Spina M, Ambrosetti A, et al. Prognostic scoring system for primary CNS lymphomas: the International Extranodal Lymphoma Study Group experience. J Clin Oncol. 2003;21:266–72. doi: 10.1200/JCO.2003.09.139. [DOI] [PubMed] [Google Scholar]
- 12.Mocroft A, Katlama C, Johnson AM, Pradier C, Antunes F, Mulcahy F, et al. AIDS across Europe, 1994-98: the EuroSIDA study. Lancet. 2000;356:291–6. doi: 10.1016/s0140-6736(00)02504-6. [DOI] [PubMed] [Google Scholar]
- 13.Sacktor N, Lyles RH, Skolasky R, Kleeberger C, Selnes OA, Miller EN, et al. HIV-associated neurologic disease incidence changes: Multicenter AIDS Cohort Study, 1990-1998. Neurology. 2001;56:257–60. doi: 10.1212/wnl.56.2.257. [DOI] [PubMed] [Google Scholar]
- 14.Schaller C, Kelly PJ. Primary central nervous system non-Hodgkin's lymphoma (PCNSL): does age and histology at presentation affect outcome? Zentralbl Neurochir. 1996;57:156–62. [PubMed] [Google Scholar]
- 15.Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg. 1988;68:835–53. doi: 10.3171/jns.1988.68.6.0835. [DOI] [PubMed] [Google Scholar]
- 16.O’Neill BP, Tomlinson FH, O’Fallon JR, Scheithauer BW, Kurtin PJ, O'Neill DB, et al. The continuing increase of primary central nervous system non-Hodgkin’s lymphoma. Ann Neurol. 1993;34:313. [Google Scholar]
- 17.Jung KW, Won YJ, Kong HJ, Oh CM, Seo HG, Lee JS. Cancer statistics in Korea: incidence, mortality, survival and prevalence in 2010. Cancer Res Treat. 2013;45:1–14. doi: 10.4143/crt.2013.45.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]