

Summary
Background
In the process of diagnosis and treatment of fractures, an X-ray study is typically performed. In modern medicine very important is the development of new diagnostic methods without adverse effects on the body. One of such techniques is ultrasound imaging. It has a high value in imaging most areas of the body, including the musculoskeletal system. Reports on the use of ultrasound in the evaluation of the callus are rare and this could be a method equivalent to or even better than standard radiographs. The aim of the study was to analyze the correlation of ultrasound with radiographs in imaging of callus formation after fractures of long bones in children and to analyze the correlation of vascular resistance index (RI) and the degree of vascularization of the callus with a subjective radiological assessment of the bone union quality.
Material/Methods
The prospective study was planned to qualify 50 children treated for long bones fractures of the arm, forearm, thigh and lower leg. Ultrasound diagnosis was carried out using a Philips iU22 camera equipped with a linear probe with 17-5-MHz resolution and MSK Superficial program. During ultrasound examination measurements of the callus were performed. Using the Power Doppler callus vascularity was visualized and vascular resistance index (RI) was measured. The same measurements were made within the corresponding area of the healthy limb. The results obtained by ultrasound were compared with radiograph measurements and with the subjective assessment of the callus quality.
Results
Preliminary results were developed on a group of 24 patients, where 28 fractured bones and 28 corresponding healthy bones were examined. Fifteen boys and 9 girls participated in the study. The average age at injury was, respectively, 11 and 9 years. In both groups fractures without displacement were the most frequent. A similar frequency was observed in fractures requiring reposition and subperiosteal fractures. In contrast, fractures with a slight displacement of the fragments, were 3 times more common in girls. Statistical analysis of the measurements of length and width of the callus demonstrated that the differences between results obtained in the ultrasound in comparison with X-rays were not statistically significant. Moreover, preliminary results showed a significantly higher degree of vascularization of the callus than of the healthy periosteum.
Conclusions
Preliminary results indicate the high efficacy of ultrasound in the evaluation of callus formation after fractures of long bones in children and the possibility of its alternative use to X-ray examinations.
MeSH Keywords: Child Care; Fracture Healing; Fractures, Bone; Radiography; Ultrasonography
Background
Fracture healing consists of restoring anatomical continuity of the bone by filling the fracture fissure with bone tissue and recovering the physiological activity of the limb. In the process of fracture healing it is very important to control the set of bone splinters and form a union. Clinical evaluation of bone healing is possible only after removing the plaster. Due to the translucency of plasters for X-rays, general availability and low cost of test execution, control radiographs were adopted as the standard in the monitoring of a fracture-healing process [1]. However, radiographs enable only quantitative assessment of periosteal reactions. Qualitative assessment of the degree of mineralization is subjective and depends on the radiologist’s abilities to describe a radiogram [2]. Therefore, other methods allowing assessment of bone union in terms of its mechanical properties, the strength or the degree of calcification have been sought. There has been much research about the use of computed tomography (CT) for this purpose as well as dual energy absorptiometry X-ray (DEXA) and quantitative computed tomography (QCT) [3]. It should be noted that all of these techniques expose the patient to ionizing radiation. According to the 13th U.S. Report on Carcinogens, X-rays have been officially recognized as a factor in the development of leukemia, lymphoma, cancer of the thyroid and lung [4]. Modern medicine is oriented to the development of new diagnostic methods without adverse effects on the patient’s body.
One of the imaging techniques, missing harmful effects on the body, is ultrasound. According to the WHO, ultrasound has been recognized as a safe, quick and effective method. It has a high value in imaging the majority of areas of the body, including the musculoskeletal system. Due to its general availability and low cost ultrasound examination has become widely used. The advantage of ultrasound is the possibility of frequent, even daily repetition of testing without subjecting the patient to harmful factors [5]. The aim of the study was to analyze the correlation of ultrasound with radiographs in imaging of callus formation after fractures of long bones in children and to analyze the correlation of vascular resistance index (RI) and the degree of vascularization of the callus with a subjective radiological assessment of the bone union quality.
Material and Methods
The prospective study was planned to qualify 50 children treated for fractures of the long bones in the Outpatient Clinic. To conduct research the consent of the Bioethics Committee was obtained (No. RNN/75/13/KE).
The study enclosed children aged 2 to 18 years, after fractures of the long bones of the arm, forearm, thigh and lower leg. Subperiosteal fractures, ones with periosteum interruption without displacement, fractures with fragments dislocation after closed or blunt reposition, as well as after internal fixation were analyzed. Patients with intra-articular fractures, with known metabolic bone disorders and children with an earlier fracture of the same bone or fracture of a corresponding bone of the other limb were excluded from the study.
According to the program, an ultrasound examination of the fracture area was performed within 3 days after the follow-up visit in the clinic, where radiograms in two projections (anterior-posterior and lateral) were taken and the plaster was removed. We do not recommend cutting out windows in the cast to perform ultrasound examination, because for children it is a stressful and painful procedure.
X-ray examinations were performed by radiographers experienced in examining children. The control kVp and mAs were adjusted depending on the age and physique. The average values for X-ray examinations of the lower limb in children were: kVp 40–50 and mAs 0.6–1.6. The average values for the upper limb were: kVp 35–50 and mAs 0.6–1.2. The X-ray system was not fitted with the Dose Area Product (DAP) meter and the accumulated DAP during examinations was not recorded. Radiograms were evaluated by a radiologist with a 30-year experience. Measurements and assessment of the callus quality were performed.
Ultrasound diagnosis was carried out using Philips iU22 camera equipped with a linear probe with 17-5-MHz resolution and MSK Superficial program. Studies were performed by one ultrasonographer experienced in imaging of the musculoskeletal system. During an ultrasound examination all surfaces of the fractured bone and the corresponding healthy bone were pictured. Measurements of the length and width of the callus were made on the front and lateral surfaces of the bone. Callus vascularity was visualized and the number of blood vessels with a diameter of 1 mm on the surface of 3 cm2 was measured. Vascular resistance index (RI), which is a measure of pulsatile blood flow that reflects the resistance to blood flow caused by a microvascular bed distal to the site of measurement, was measured with Power Doppler function. We used Pulsed Wave Doppler (PW) 40% with fixed Wave Frequency (WF) of 40 Hz and Sample Volume Lenght of 0.5 mm. The same measurements were performed within the corresponding area of the healthy limb. The results obtained by ultrasound were compared with radiographic measurements and with the subjective assessment of the callus quality. The patients’ clinical data, such as age, sex, location and type of fracture and the efficiency of the limb within two weeks after plaster removal were analyzed. The obtained results were analyzed statistically using arithmetic average, Wilcoxon test.
Results
Preliminary results were developed on a group of 24 patients, where 28 fractured bones and 28 corresponding healthy bones were examined. Fifteen boys and 9 girls participated in the study. The average age at injury was, respectively, 11 and 9 years.
In both groups fractures without displacement were the most frequent. A similar frequency was observed in fractures requiring reposition and in subperiosteal fractures. In contrast, fractures with a slight displacement of the fragments, were 3 times more common in girls (Table 1). In 2 boys there occurred limitation of movement of the limb after removing the plaster with the necessity of a referral to a physiotherapy center. The results obtained by ultrasound were compared with radiograph measurements and with the subjective assessment of the callus quality (Figures 1–3).
Table 1.
Description of the study.
| Subperiosteal fractures | Fractures without displacement | Fractures after reposition | Fractures with displacement | Row – Totals | |
|---|---|---|---|---|---|
| Male | 3 | 7 | 4 | 1 | 15 |
| Column% | 50.00% | 63.64% | 57.14% | 25.00% | |
| Row% | 20.00% | 46.67% | 26.67% | 6.67% | |
| Female | 3 | 4 | 3 | 3 | 13 |
| Column% | 50.00% | 36.36% | 42.86% | 75.00% | |
| Row% | 23.08% | 30.77% | 23.08% | 23.08% | |
| Totals | 6 | 11 | 7 | 4 | 28 |
Figure 1.

Measurements of callus length and width in AP projection in a 6-year-old girl. (A) X-ray; (B) USG – area medial; (C) USG – area lateral.
Figure 2.

Measurements of fracture gap width in an 11-year-old boy. (A) X-ray; (B) USG.
Figure 3.
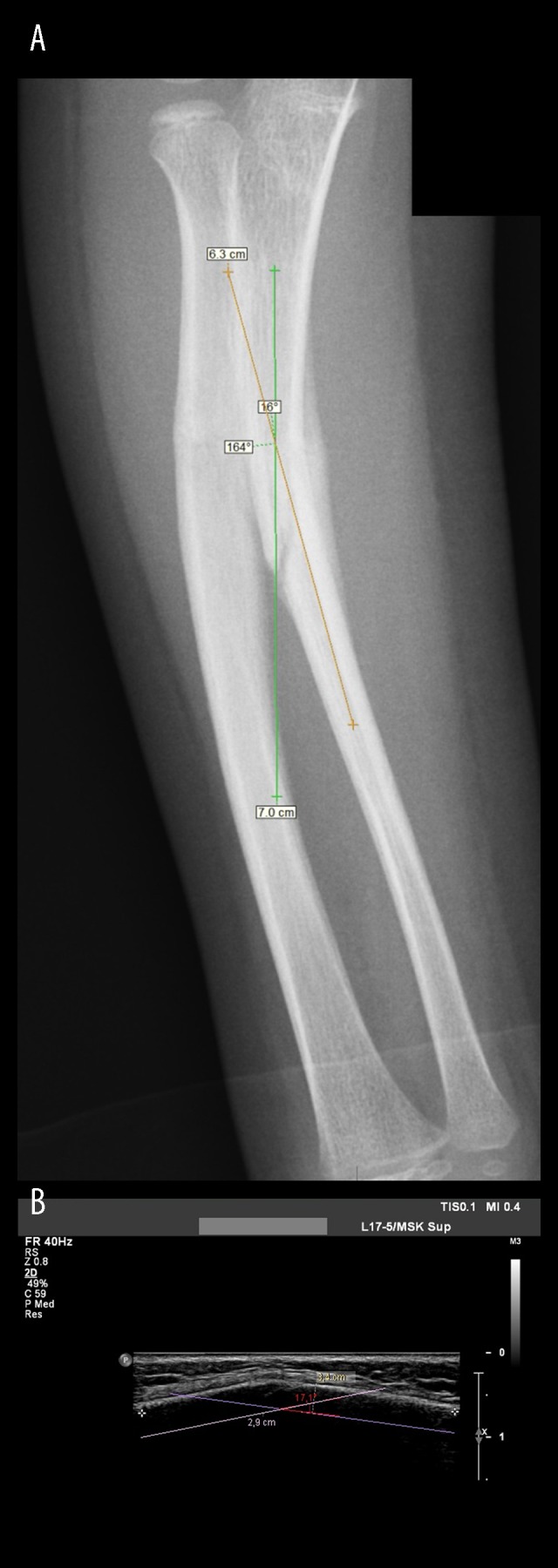
Measurements of bone splinter angle in a 6-year-old girl. (A) X-ray; (B) USG.
Measurements of the length and width of the callus were statistically analyzed using a Wilcoxon test. The differences in the results obtained in the ultrasound in comparison to X-ray were not statistically significant (Table 2).
Table 2.
Comparison of average callus measurements in X-ray and ultrasound.
| X-ray | Ultrasound | p | |
|---|---|---|---|
| Callus length AP I [cm] | 1.54±1.21 | 1.60±1.23 | 0.0355 |
| Callus width AP I [cm] | 0.16±0.11 | 0.14±0.10 | 0.1083 |
| Callus length AP II [cm] | 0.75±1.33 | 0.70±1.18 | 0.6744 |
| Callus width AP II [cm] | 0.08±0.11 | 0.06±0.10 | 0.1088 |
| Callus length L I [cm] | 1.45±1.14 | 1.40±1.05 | 0.1728 |
| Callus width L I [cm] | 0.16±0.12 | 0.15±0.10 | 0.5536 |
| Callus length L II [cm] | 0.35±0.84 | 0.35±0.82 | 0.8927 |
| Callus width L II [cm] | 0.04±0.10 | 0.03±0.07 | 0.1088 |
| Bone splinters angle AP | 2.75±6.14 | 2.74±6.11 | 0.7874 |
| Bone splinters angle L | 3.86±6.80 | 3.74±6.57 | 0.0929 |
| Fracture gap width [cm] | 0.09±0.10 | 0.09±0.11 | 1.0000 |
The level of vascularity in periosteal reactions was also examined and compared to healthy periosteum of the corresponding limb by assessing the number and size of blood vessels per 3 cm2. The results showed strong congestion of bone remodeling areas that can indirectly indicate the phase of the healing process (Figure 4).
Figure 4.

Comparison of the number of blood vessels with a diameter of 1 mm in the callus and in healthy periosteum on the surface of 3 cm2.
Vascular resistance index (RI) measurements in the callus were compared with subjective radiological assessment of the bone union quality. Bone union in our patients was described as fragile, good or complete. Based on this comparison, we found that vascular resistance index is an average of 0.2 lower in a fragile callus, when bone repair process is severe. The better is bone union, the higher are RI results. Vascular resistance index can be used for qualitative objective assessment of bone union (Figure 5).
Figure 5.

Comparison of callus vascular resistance index with subjective assessment of the callus quality (P<0.0001).
Disscusion
Usefulness of ultrasonography in the study of the motion system has been confirmed first in the diagnosis of musculoskeletal injuries. The first report on the use of ultrasound in the evaluation of rib fractures was published in 1990 by Smeets et al. and it was a proposal of a new sonographic sign to the radiological spectrum of child abuse [6]. Shortly afterwards, on the basis of numerous studies, ultrasound has proven to be more effective than the standard X-rays in the diagnosis of rib fractures [7–12]. According to Griffith et al. [12], X-rays revealed 12%, whereas ultrasound revealed 78% of ribs fractures.
In 1995 Rathfelder and Paar, in the first generous study, reported good results for using sonografic methods in diagnosing fractures in children. In that study, in 53.3% of examined children, an X-ray could have been replaced by an ultrasound. Authors proposed a term “Osteosonography” for an ultrasound examination in bone fractures [14].
The use of ultrasonography in bone evaluation raised and still raises a lot of controversies. Ultrasound allows to show only the outer surface of the bone, with no access to the trabecular bone. Moreover, not every area of the bone is available to ultrasound. Despite these major disadvantages the publications show a high correlation of ultrasonography with radiographs in the diagnosis of sternum and long bone fractures, as well as in the evaluation of fractures in children [13,14].
In the same period of time, research on the use of ultrasound in the evaluation of bone healing process after fracture was initiated. Authors showed a high correlation of ultrasonography with X-ray studies in the evaluation of periosteal reactions [15–18]. Maffulin et al. have also proven that ultrasound has a higher effectiveness in imaging of the callus in the early stages of the healing process. [15]. Moreover, the use of the Color or Power Doppler allows for evaluation of vascularization of periosteal reactions. Based on the research, it was found that vascular resistance and vessel density in the callus are greatest during the initial healing phase and gradually decrease from the 3–4 week after the fracture. Analysis of the results showed a high value of ultrasonographic evaluation of the vascularity of the callus in predicting normal or delayed healing [16,17]. Another method for qualitative assessment of periosteal reactions using ultrasonic waves trades on significant changes in the mineral composition of the callus, comparing it to the healthy bone. This study involves the assessment of changes in the speed of the reflected wave from the callus using transducers [18].
In our study high effectiveness of ultrasound examination in evaluation of bone healing was proved. There were many advantages as lack of ionizing radiation, possibility of muscle visualization and qualitative assessment of the callus based on vascularization. The procedure was painless and well tolerated. The examination was easy to perform. Unfortunately we can perform the examination after plaster removal due to opacity of ultrasonic waves.
Conclusions
Ultrasound gives more opportunities than we thought before. However, using US for evaluation of the callus after bone fractures needs practice and experience. We should consider all advantages of this examination. In certain cases we can reduce ionizing radiation and carry out qualitative assessment of the callus by replacing a standard X-ray with ultrasound. We should perform further studies and get more experience in ultrasound assessment in the bone healing process in children.
Preliminary results indicate the high efficacy of ultrasound in the evaluation of callus formation after fractures of long bones in children and a possibility of its alternative use to X-ray examinations.
Acknowledgements
The authors wish to express their gratitude to technicians and administrative personnel of the Radiology Department, and the patients whose participation made this study possible.
References
- 1.Grigoryan M, Lynch JA, Fierlinger AL, et al. Quantitative and qualitative assessment of closed fracture healing using computed tomography and conventional radiography. Academic Radiology. 2003;10(11):1267–73. doi: 10.1016/s1076-6332(03)00467-7. [DOI] [PubMed] [Google Scholar]
- 2.Webb J, Herling G, Gardner T, et al. Manual assessment of fracture stiffnes. Injury. 1996;27(5):319–20. doi: 10.1016/0020-1383(96)00009-5. [DOI] [PubMed] [Google Scholar]
- 3.Wong LC, Chiu WK, Russ M, Liew S. Review of techniques for monitoring the healing fracture of bones for implementation in an internally fixated pelvis. Med Eng Physics. 2012;34(2):140–52. doi: 10.1016/j.medengphy.2011.08.011. [DOI] [PubMed] [Google Scholar]
- 4.U.S Department of Health and Human Services. 13th Report on Carcinogenes. 2014. [Accessed 2 October 2014]. http://ntp.niehs.nih.gov/pubhealth/roc/roc13/index.html.
- 5.Williamson D, Watura R, Cobby M. Ultrasound imaging of forearm fractures in children: a viable alternative? J Accid Emerg. 2000;17:22–24. doi: 10.1136/emj.17.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Smeets AJ, Robben SG, Meradji M. Sonographically detected costochondral dislocation in an abused child: a new sonographic sign to the radiological spectrum of child abuse. Pediatr Radiol. 1990;20:566–67. doi: 10.1007/BF02011396. [DOI] [PubMed] [Google Scholar]
- 7.Battistelli JM, Anselem B. Echography in injuries of costal cartilages. J Radiol. 1993;74:409–12. [PubMed] [Google Scholar]
- 8.Bitschnau R, Gehmacher O, Kopf A, et al. Ultrasound diagnosis of rib and sternum fractures. Ultraschall Med. 1997;18:158–61. doi: 10.1055/s-2007-1000416. [DOI] [PubMed] [Google Scholar]
- 9.Mariacher-Gehler S, Michel BA. Sonography: a simple way to visualize rib fractures. Am J Roentgenol. 1994;163:1268. doi: 10.2214/ajr.163.5.7976923. [DOI] [PubMed] [Google Scholar]
- 10.Wischhöfer E, Fenkl R, Blum R. Ultrasound detection of rib fractures for verifying fracture diagnosis. A pilot project. Unfallchirurg. 1995;98:296–300. [PubMed] [Google Scholar]
- 11.Wüstner A, Gehmacher O, Hämmerle S, et al. Ultrasound diagnosis in blunt thoracic trauma. Ultraschall Med. 2005;26:285–90. doi: 10.1055/s-2005-858524. [DOI] [PubMed] [Google Scholar]
- 12.Griffith JF, Rainer TH, Ching AS, et al. Sonography compared with radiography in revealing acute rib fracture. Am J Roentgenol. 1999;173:1603–9. doi: 10.2214/ajr.173.6.10584808. [DOI] [PubMed] [Google Scholar]
- 13.Patten RM, Mack LA, Wang KY, Lingel J. Nondisplaced fractures of the greater tuberosity of the humerus: sonografic detection. Radiology. 1992;182:201–4. doi: 10.1148/radiology.182.1.1727282. [DOI] [PubMed] [Google Scholar]
- 14.Rathfelder FJ, Paar O. Possibilities for using sonography as a diagnostic procedure in fractures during the growth period. Unfallchirurg. 1995;98:645–49. [PubMed] [Google Scholar]
- 15.Maffulli N, Thornton A. Ultrasonographic appearance of external callus in long-bone fractures. Injury. 1995;26(1):5–12. doi: 10.1016/0020-1383(95)90544-8. [DOI] [PubMed] [Google Scholar]
- 16.Caruso G, Lagalla R, Derchi L, et al. Monitoring of fracture calluses with color Doppler sonography. J Clin Ultrasound. 2000;28(1):20–27. doi: 10.1002/(sici)1097-0096(200001)28:1<20::aid-jcu3>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 17.Risselada M, Kramer M, Saunders JH, et al. Power Doppler assessment of the neovascularization during uncomplicated fracture healing of long bones in dogs and cats. Vet Radiol Ultrasound. 2006;47(3):301–6. doi: 10.1111/j.1740-8261.2006.00144.x. [DOI] [PubMed] [Google Scholar]
- 18.Cunningham JL, Kenwright J, Kershaw CJ. Biomechanical measurement of fracture healing. J Med Eng Technol. 1990;14(3):92–101. doi: 10.3109/03091909009015420. [DOI] [PubMed] [Google Scholar]