

Key Clinical Message
While rare, Fahr's disease should be considered as a differential diagnosis for seizures, movement disorders, or cognitive impairment in tropical settings. Classically, bilateral calcification of the basal ganglia is seen on CT. Endemic infections, metabolic, and toxic causes should be excluded. Treatment using Levodopa is often beneficial.
Keywords: calcification, Fahr's disease, Nigeria, seizures
Introduction
Fahr's disease is a rare disorder of unknown prevalence, with a higher incidence reported among males and a typical age-of-onset in the 3rd-5th decade of life 1,2, although, it has been described in pediatric age groups. Children with Fahr's disease typically present with motor deficits though 40% have primarily cognitive and other psychiatric symptoms 3. First described by a German neurologist Fahr in 1930 4, it is also known as idiopathic basal ganglia calcification or bilateral steriopallidodentate calcinosis (BSPDC). Fahr's disease is a genetically dominant, inherited and progressive neurological disorder, which is sporadic and has a genetic locus on chromosome 14q48 5. Although Fahr's disease is associated with some underlying medical conditions, the exact etiology remains unknown 6. Movement disorders are the most common manifestation of Fahr's disease and Parkinsonism accounts for 57% 2. Other clinical features include disordered speech, cerebellar signs, chorea, dystonia, oro-facial dyskinesia, tremors, and seizure. Reports of cognitive impairment and neuropsychiatric features are common and often progressive. If left untreated, psychotic disorders and dementia can develop 1.
There are very limited reports on Fahr's disease from tropical African settings, where other differential diagnoses are more likely to be considered to explain the occurrence of seizures, movement disorders, or cognitive impairment. Therefore, we present a 58-year-old Nigerian man with seizures, movement disorders, and cognitive impairment, who was eventually diagnosed with Fahr's disease.
Case History/Examination
A local 58-year-old man presented to a regional Nigerian hospital with repeated seizures and a 3-week history of abnormal behaviour. He had been experiencing recurrent headaches, speech abnormalities, and worsening forgetfulness for a year. His past medical history included hypertension and diabetes, which were controlled on Amlodipine and Metformin, and reported no family history of seizure or movement disorders.
On examination he had a normal level of consciousness with disorientation to time, place, and person. There was mild neurocognitive impairment, which was reflected by mini-mental state assessment total score of 18/30. The breakdown of this score was as follows: orientation to time (3), orientation to place (3), registration (2), attention and calculation (3), recall (1), language (2), repetition (1), and complex commands (3). It was noted that he had spontaneous nystagmus, intention tremor, a mask-like expressionless face with reduced blink rate, and bradykinesia. He also demonstrated rigidity, stooped posture, and turned en-block, with dysarthria, dysmetria, and dysdiadochokinesia. However, no evidence of any spasticity was noted. The rest of the neurological and physical examination was unremarkable.
Differential Diagnosis, Investigations and Treatment
The initial differential diagnoses entertained were Parkinson's disease and an ischemic stroke involving the globus pallidus. Laboratory investigations revealed a normal hemoglobin, lipid profile, glucose, iron, ferritin, HbA1c, and electrocardiogram. His human immunodeficiency virus (HIV) and Mantoux (purified protein derivative) tests were negative. His serum calcium was normal at 2.3 mmol/L (2.2–2.7) while serum parathyroid hormone was at 10.8 pg/mL (10–55). Liver, kidney, and thyroid function tests were all normal. Noncontrast computed tomography (CT) of the brain showed bilateral, extensive, and dense calcifications involving the dentate nuclei and basal ganglia with preserved cerebral and cerebellar hemispheres (Fig.1).
Figure 1.
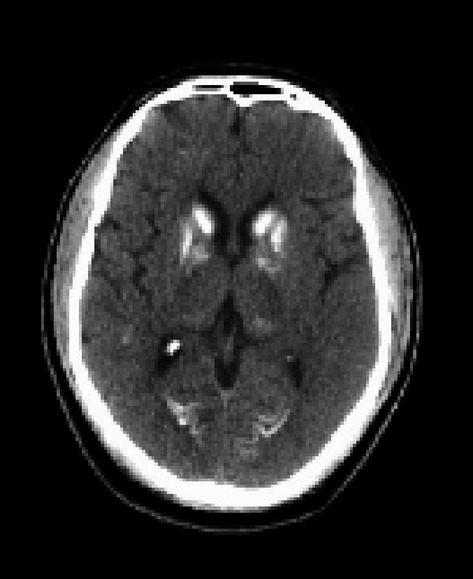
Noncontrast computer tomography of the brain showing bilateral, extensive, and dense calcifications involving the dentate nuclei and basal ganglia with preserved cerebral and cerebellar hemispheres.
Outcome and Follow-Up
The patient was started on Levodopa, Carbamazepine, and Clonazepam in addition to the routine antihypertensive and oral hypoglycemic drugs. Symptoms were gradually controlled over a period of 2 weeks and the patient is now being followed up on an out-patient basis.
Discussion
This patient presented with seizures, movement disorders, or cognitive impairment. Some other differential diagnoses that were entertained later included rare conditions such Creutzfeldt–Jakob disease that causes progressive dementia and focal neurologic signs, but tests for this was not available. We also considered neuroacanthocytosis – a genetic disorder which presents with chorea, oro-facial dyskinesia, seizures, and axonal neuropathy, but these were ruled out after laboratory testing.
The diagnosis of Fahr's disease is complex and requires both clinical and radiological evidence. The criteria include bilateral calcification of the basal ganglia with neuropsychiatric and/or extrapyramidal features associated with normal calcium and phosphate metabolism 7. These calcifications which are usually idiopathic occur most commonly at the basal ganglia, but other structures may also be affected 8. Patients exhibit progressive neurological symptoms such as seizures, rigidity, and dementia with classical bilateral basal ganglia calcification shown on CT imaging. CT imaging is said to be more sensitive in identifying the basal ganglia calcification in comparison to magnetic resonance imaging (MRI) 9. Exclusion of infective, metabolic, toxic, or traumatic causes is critical and a family history is commonly described 1. Our index patient had extensive symmetric calcifications of the basal ganglia, seizures, dementia, Parkinsonism, a speech disorder, and cerebellar signs. It is hypothesized that the calcium deposition in the basal ganglia typically begins in the third decade of life with the clinical manifestations occurring two decades later 9. This hypothesis seems to fit our index patient who developed the classic features at age 58.
The basal ganglia calcification may occur as a consequence of several other known genetic, infectious, and metabolic conditions 10. Endemic infectious agents such as cytomegalovirus (CMV), HIV, toxoplasmosis, and neurocysticercosis were eliminated as a cause, as were secondary hypoparathyroidism, hypothyroidism, neurofibromatosis, tuberculosis, tuberous sclerosis, cerebral hemorrhage, and vascular disease. Other potential causes to be considered include systemic lupus, hypervitaminosis D, lead poisoning, and radiotherapy. In limited resource settings, CT scans are becoming increasingly available and it remains a very useful modality for diagnosis of Fahr's disease. However, subarachnoid hemorrhage can easily be confused with Fahr's disease on the noncontrast brain CT scan in emergency departments.
Laboratory examinations in the suspected cases of Fahr's disease should include tests for blood calcium and parathyroid hormone. This will help differentiate idiopathic Fahr's disease (unremarkable laboratory test results) from secondary cases especially due to hypoparathyroidism. Some authors have used the term Fahr's syndrome to describe the basal ganglia calcification, which is secondary to some other disorders such as hypoparathyroidism 11,12.
The treatment for Fahr's disease targets symptomatic support and improvement in the quality of life 13.Treatment of the underlying disease process may lead to a marginal improvement in neuropsychiatric features. Prognosis is variable, unpredictable, and is unrelated to the extent of calcification 14. Use of haloperidol or lithium carbonate has been reported to help in patients with psychotic symptoms 15. Our patient responded well to Levodopa as seen in similar reports, and his seizures were controlled by a combination of Carbamazepine and Clonazepam. To the best of our knowledge, this is the only report of Fahr's disease in this region of Nigeria. We report this case to highlight its symptomatology and affirm its occurrence in Nigeria.
In conclusion, while rare, Fahr's disease should be considered as a differential diagnosis for seizures, movement disorders, or cognitive impairment in a tropical setting. The classical finding on CT is bilateral calcification of the basal ganglia, which may be confused with subarachnoid hemorrhage in an emergency setting. It is important to ensure that endemic infections, metabolic, or toxic causes are excluded early. Treatment using Levodopa and other medications can often be beneficial, and the aim of therapy is to provide symptomatic support and improve the quality of life.
Acknowledgments
None.
Conflict of Interest
None declared.
References
- Chiu HF, Lam LC, Shum PP. Li KW. Idiopathic calcification of the basal ganglia. Postgrad. Med. J. 1993;69:66–70. doi: 10.1136/pgmj.69.807.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manyam BV, Walters AS. Narla KR. Bilateral striopallido dentate calcinosis: clinical characteristics of patients seen in a registry. Mov. Disord. 2001;16:258–264. doi: 10.1002/mds.1049. [DOI] [PubMed] [Google Scholar]
- Benke T, Karner E, Seppi K, Delazer M, Marksteiner J. Donnemiller E. Subacute dementia and imaging correlates in a case of Fahr's disease. J. Neurol. Neurosurg. Psychiatry. 2004;75:1163–1165. doi: 10.1136/jnnp.2003.019547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fahr T. Idiopathische Verkalkung der Hirngefässe. Zentralbl. Allg. Pathol. 1931;50:129–133. [Google Scholar]
- Geschwind DH, Loginov M. Stern JM. Identification of a locus on chromosome 14q for idiopathic basal ganglia calcification (Fahr disease) Am. J. Hum. Genet. 1999;65:764–772. doi: 10.1086/302558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shigeyuki O. Imaging of bilateral striopallidodentate calcinosis. Clin. Nucl. Med. 2002;27:721–724. doi: 10.1097/00003072-200210000-00008. [DOI] [PubMed] [Google Scholar]
- Trautner RI, Cummings IL, Read SL. Benson DF. Idiopathic basal ganglia calcification and organic mood disorder. Am. J. Psychiatry. 1988;145:350–353. doi: 10.1176/ajp.145.3.350. [DOI] [PubMed] [Google Scholar]
- Taxer F, Halter R. Konig P. Clinical early symptoms and CT-Scan findings in Fahr syndrome. Nervenarzt. 1986;57:583–588. [PubMed] [Google Scholar]
- Manyam BV, Bhatt MH, Moore WD, Develschoward AB, Anderson DR. Caline DB. Bilateral striopallidodentate calcinosis: cerebrospinal fluid, imaging and electrophysiological studies. Ann. Neurol. 1992;31:379–384. doi: 10.1002/ana.410310406. [DOI] [PubMed] [Google Scholar]
- Niwa A, Naito Y. Kuzuhara S. Severe cerebral calcification in a case of LEOPARD syndrome. Intern. Med. 2008;47:1925–1929. doi: 10.2169/internalmedicine.47.1365. [DOI] [PubMed] [Google Scholar]
- Guerreiro MM. Scotoni AE. Calcificações dosgânglios da base nainfância. Arq. Neuropsiquiatr. 1992;50:513–518. doi: 10.1590/s0004-282x1992000400016. [DOI] [PubMed] [Google Scholar]
- Oliveira JR, Spiteri E, Sobrido MJ, Hopfer S, Klepper J, Voit T, et al. Genetic heterogeneity in familial idiopathic basal ganglia calcification (Fahr disease) Neurology. 2004;63:2165–2167. doi: 10.1212/01.wnl.0000145601.88274.88. [DOI] [PubMed] [Google Scholar]
- Senoglu M, Tuncel D, Orhan FO, Yuksel Z. Gokce M. Fahr's syndrome: a report of two cases. Firat Tip Dergisi. 2007;12:70–72. [Google Scholar]
- Rastogi R, Singh AK, Rastogi UC, Chander Mohan C. Vaibhav Rastogi V. Fahr's syndrome: a rare clinico-radiologic entity. Med. J. Armed Forces India. 2011;67:159–161. doi: 10.1016/S0377-1237(11)60020-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Munir KM. The treatment of psychotic symptoms in Fahr's disease with lithium carbonate. J. Clin. Psychopharmacol. 1986;6:36–38. [PubMed] [Google Scholar]